
Data Mining for ICD-10 Admission Diagnoses Preceding Tuberculosis within 1 Year among Non-HIV and Non-Diabetes Patients


Abstract
:1. Introduction
2. Materials and Methods
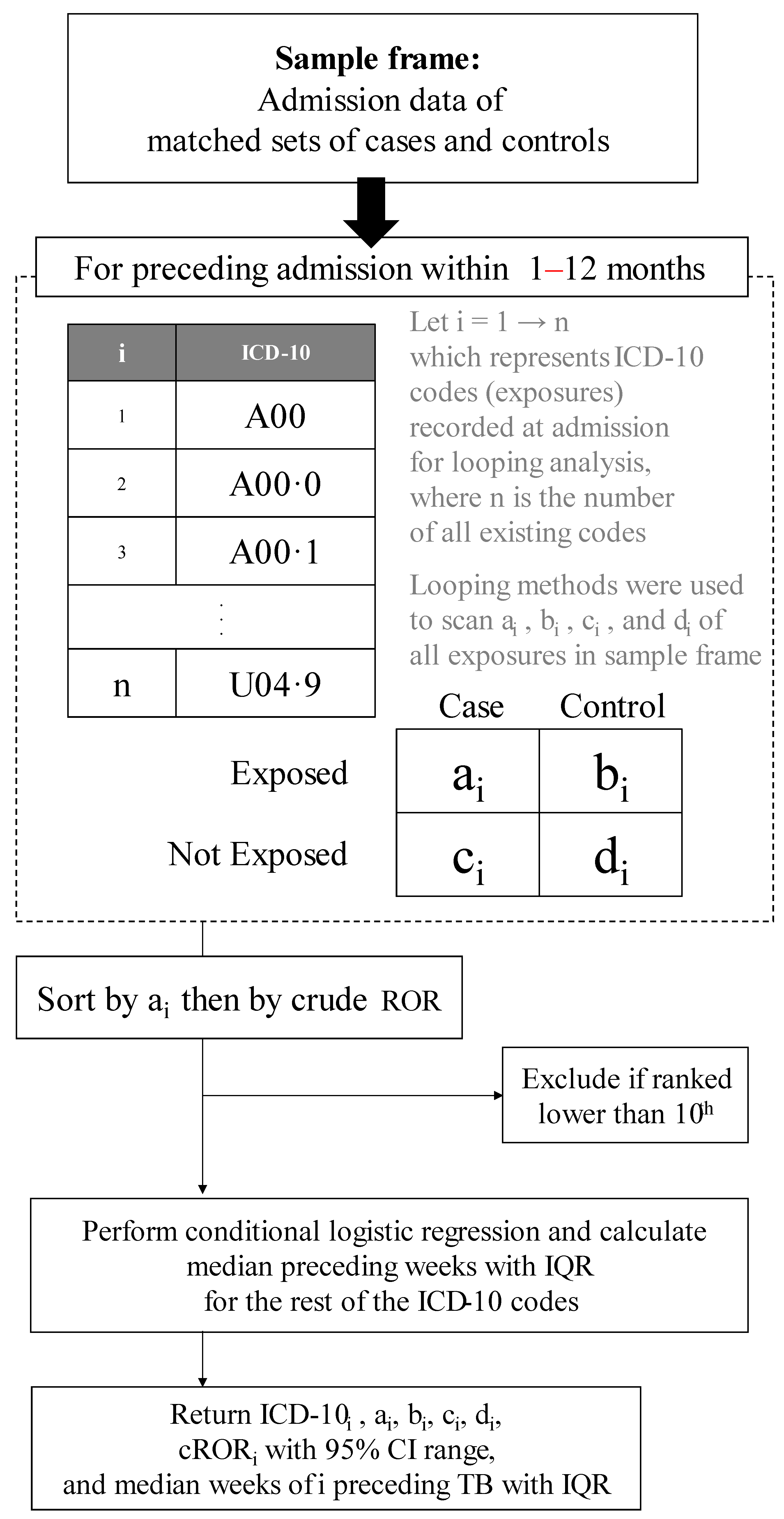
2.1. Concept and Study Design
2.2. Data Collection and Retrieval
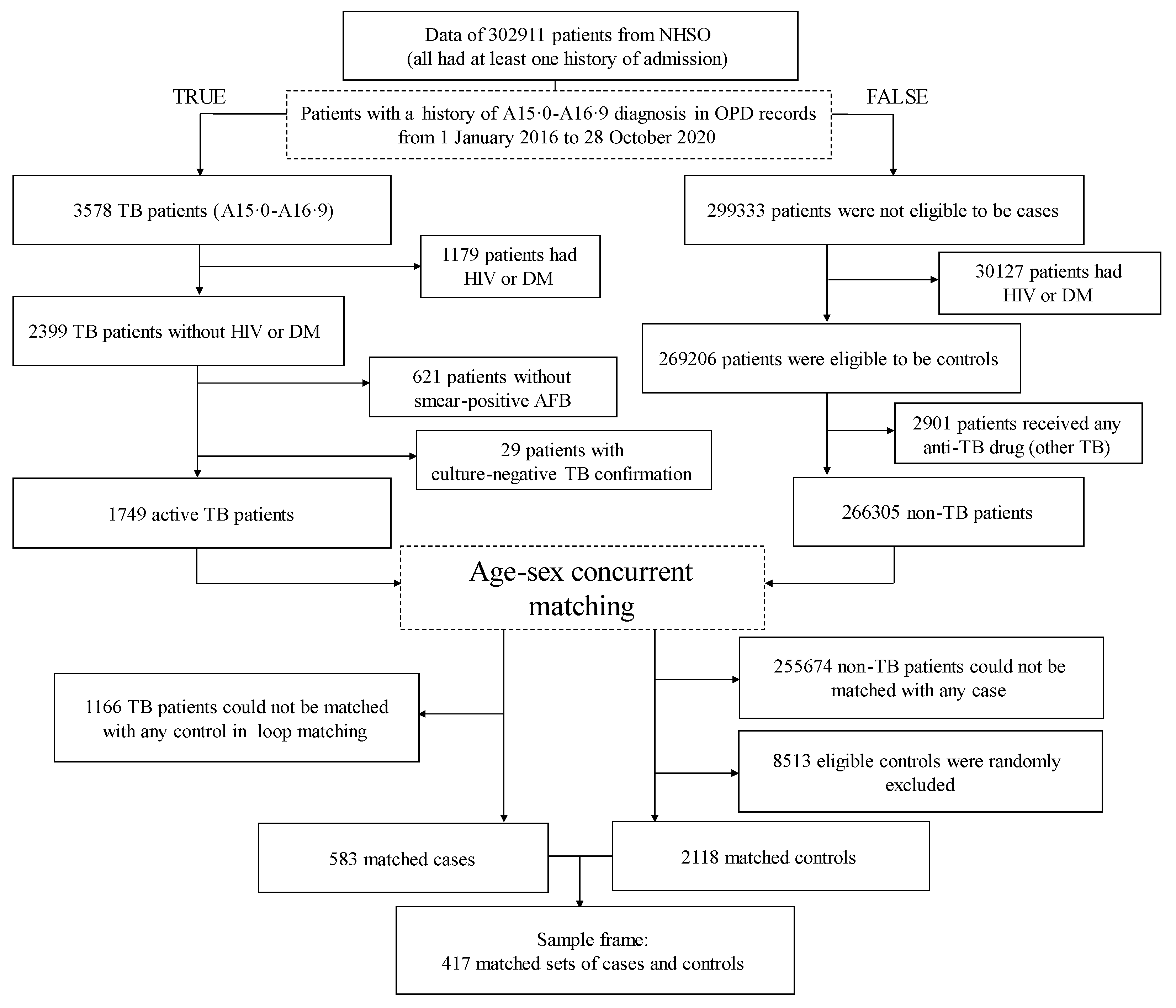
2.3. Case Ascertainment
2.4. Control Selection
2.5. Matching Ratio and Matching Process
2.6. Outcome
2.7. Exposures
2.8. Statistical Analysis
2.9. Further Exploration for Hospitalized Comorbidities Preceding
3. Results
3.1. Matching Results and Their Characteristics
3.2. Preceding Admitted Diseases Returned from the Looping Analysis
3.3. Bacteriological Evidence for TB
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 29 March 2022).
- World Health Organization. Global Tuberculosis Report 2020; World Health Organization: Geneva, Switzerland, 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/336069/9789240013131-eng.pdf (accessed on 31 March 2022).
- Getahun, H.; Matteelli, A.; Chaisson, R.E.; Raviglione, M. Latent Mycobacterium tuberculosis infection. N. Engl. J. Med. 2015, 372, 2127–2135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiazyk, S.; Ball, T. Latent tuberculosis infection: An overview. Can. Commun. Dis. Rep. 2017, 43, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Behr, M.A.; Edelstein, P.H.; Ramakrishnan, L. Revisiting the timetable of tuberculosis. BMJ 2018, 362, k2738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, C.; Jarvis, W.R. Administrative, Engineering, and Personal Protective Measures for Controlling Mycobacterium tuberculosis. In Multidrug-Resistant Tuberculosis; Bastian, I., Portaels, F., Eds.; Springer: Dordrecht, The Netherlands, 2000; pp. 269–284. [Google Scholar]
- Thailand Department of Disease Control, Tuberculosis Division. Tuberculosis Case Management Dashboard. Available online: http://tbcmthailand.ddc.moph.go.th/UIForm/Tableau/TEST_tbcm.php (accessed on 31 March 2022).
- Getnet, F.; Demissie, M.; Assefa, N.; Mengistie, B.; Worku, A. Delay in diagnosis of pulmonary tuberculosis in low-and middle-income settings: Systematic review and meta-analysis. BMC Pulm. Med. 2017, 17, 202. [Google Scholar] [CrossRef] [PubMed]
- Bhalla, A.S.; Goyal, A.; Guleria, R.; Gupta, A.K. Chest tuberculosis: Radiological review and imaging recommendations. Indian J. Radiol. Imaging 2015, 25, 213–225. [Google Scholar] [CrossRef]
- Török, M.E. Tuberculous meningitis: Advances in diagnosis and treatment. Br. Med. Bull. 2015, 113, 117–131. [Google Scholar] [CrossRef] [Green Version]
- Ladumor, H.; Al-Mohannadi, S.; Ameerudeen, F.S.; Ladumor, S.; Fadl, S. TB or not TB: A comprehensive review of imaging manifestations of abdominal tuberculosis and its mimics. Clin. Imaging 2021, 76, 130–143. [Google Scholar] [CrossRef]
- Bhuket, J.R.N.; Pungrassami, P.; Chongsuvivatwong, V. Hospital tuberculosis control activities and treatment success in Thailand during the implementation year of the admission policy for new smear positive pulmonary tuberculosis patients. J. Med. Assoc. Thai. 2013, 96, 782–785. [Google Scholar]
- Silva, D.R.; Muñoz-Torrico, M.; Duarte, R.; Galvão, T.; Bonini, E.H.; Arbex, F.F.; Arbex, M.A.; Augusto, V.M.; Rabahi, M.F.; de Mello, F.C.Q. Risk factors for tuberculosis: Diabetes, smoking, alcohol use, and the use of other drugs. J. Bras. Pneumol. 2018, 44, 145–152. [Google Scholar] [CrossRef] [Green Version]
- Melsew, Y.A.; Doan, T.N.; Gambhir, M.; Cheng, A.C.; McBryde, E.; Trauer, J.M. Risk Factors for infectiousness of patients with tuberculosis: A systematic review and meta-analysis. Epidemiol. Infect. 2018, 146, 345–353. [Google Scholar] [CrossRef] [Green Version]
- Ai, J.W.; Ruan, Q.L.; Liu, Q.H.; Zhang, W.H. Updates on the risk factors for latent tuberculosis reactivation and their managements. Emerg. Microbes Infect. 2016, 5, e10. [Google Scholar] [CrossRef] [PubMed]
- Wagnew, F.; Eshetie, S.; Alebel, A.; Dessie, G.; Tesema, C.; Abajobir, A.A. Meta-analysis of the prevalence of tuberculosis in diabetic patients and its association with cigarette smoking in African and Asian countries. BMC Res. Notes 2018, 11, 298. [Google Scholar] [CrossRef] [PubMed]
- Gelaw, Y.; Getaneh, Z.; Melku, M. Anemia as a risk factor for tuberculosis: A systematic review and meta-analysis. Environ. Health Prev. Med. 2021, 26, 13. [Google Scholar] [CrossRef]
- Rees, D.; Murray, J. Silica, silicosis and tuberculosis. Int. J. Tuberc. Lung Dis. 2007, 11, 474–484. [Google Scholar] [PubMed]
- Simou, E.; Britton, J.; Leonardi-Bee, J. Alcohol consumption and risk of tuberculosis: A systematic review and meta-analysis. Int. J. Tuberc. Lung. Dis. 2018, 22, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Byrne, A.L.; Marais, B.J.; Mitnick, C.D.; Lecca, L.; Marks, G.B. Tuberculosis and chronic respiratory disease: A systematic review. Int. J. Infect. Dis. 2015, 32, 138–146. [Google Scholar] [CrossRef] [Green Version]
- Tavares, A.M.; Fronteira, I.; Couto, I.; Machado, D.; Viveiros, M.; Abecasis, A.B.; Dias, S. HIV and tuberculosis co-infection among migrants in Europe: A systematic review on the prevalence, incidence and mortality. PLoS ONE 2017, 12, e0185526. [Google Scholar] [CrossRef] [Green Version]
- Imsanguan, W.; Bupachat, S.; Wanchaithanawong, V.; Luangjina, S.; Thawtheong, S.; Nedsuwan, S.; Pungrassami, P.; Mahasirimongkol, S.; Wiriyaprasobchok, A.; Kaewmamuang, K.; et al. Contact tracing for tuberculosis, Thailand. Bull. World Health Organ. 2020, 98, 212–218. [Google Scholar] [CrossRef]
- Oo, M.M.; Tassanakijpanich, N.; Phyu, M.H.; Safira, N.; Kandel, S.; Chumchuen, K.; Zhang, L.M.; Kyu, H.A.; Sriwannawit, P.; Bilmumad, B.; et al. Coverage of tuberculosis and diabetes mellitus screening among household contacts of tuberculosis patients: A household-based cross-sectional survey from Southern Thailand. BMC Public Health 2020, 20, 957. [Google Scholar] [CrossRef]
- Bureau of Tuberculosis, Department of Disease Control, Thailand. National Tuberculosis Control Program Guideline, Thailand. 2020. Available online: https://www.thainapci.org/2021/2021/11/30/ (accessed on 31 March 2022).
- Wei, M.; Zhao, Y.; Qian, Z.; Yang, B.; Xi, J.; Wei, J.; Tang, B. Pneumonia caused by Mycobacterium tuberculosis. Microbes Infect. 2020, 22, 278–284. [Google Scholar] [CrossRef]
- Gengenbacher, M.; Kaufmann, S.H.E. Mycobacterium tuberculosis: Success through dormancy. FEMS Microbiol. Rev. 2012, 36, 514–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gopi, A.; Madhavan, S.M.; Sharma, S.K.; Sahn, S.A. Diagnosis and treatment of tuberculous pleural effusion in 2006. Chest 2007, 131, 880–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huo, Z.; Peng, L. Is Xpert MTB/RIF Appropriate for diagnosing tuberculous pleurisy with pleural fluid samples? A systematic review. BMC Infect. Dis. 2018, 18, 284. [Google Scholar] [CrossRef] [Green Version]
- Castro, D.J.; Nuevo, G.D.; Pérez-Rodríguez, E.; Light, R.W. Diagnostic value of adenosine deaminase in nontuberculous lymphocytic pleural effusions. Eur. Respir. J. 2003, 21, 220–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allan, W.G.; Girling, D.J.; Fayers, P.M.; Fox, W. The symptoms of newly diagnosed pulmonary tuberculosis and patients’ attitudes to the disease and to its treatment in Hong Kong. Tubercle 1979, 60, 211–223. [Google Scholar] [CrossRef]
- Fidan, A.; Ozdoğan, S.; Oruç, O.; Salepçi, B.; Ocal, Z.; Cağlayan, B. Hemoptysis: A retrospective analysis of 108 cases. Respir. Med. 2002, 96, 677–680. [Google Scholar] [CrossRef] [Green Version]
- Jonaidi Jafari, N.; Izadi, M.; Sarrafzadeh, F.; Heidari, A.; Ranjbar, R.; Saburi, A. Hyponatremia due to pulmonary tuberculosis: Review of 200 Cases. Nephrourol. Mon. 2013, 5, 687–691. [Google Scholar] [CrossRef] [Green Version]
- Shalhoub, R.J.; Antoniou, L.D. The mechanism of hyponatremia in pulmonary tuberculosis. Ann. Intern. Med. 1969, 70, 943–962. [Google Scholar] [CrossRef]
- Mupere, E.; Parraga, I.M.; Tisch, D.J.; Mayanja, H.K.; Whalen, C.C. Low nutrient intake among adult women and patients with severe tuberculosis disease in Uganda: A cross-sectional study. BMC Public Health 2012, 12, 1050. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Category | Decode | Reasons |
|---|---|---|
| F | Mental, behavioral, and neurodevelopmental disorders | The cases are usually passed to a specific department or psychiatric hospital; thus, the patients are not proper controls. |
| O, P, Q | Pregnancy, childbirth, and puerperium Certain conditions originating in the perinatal period | The diseases/conditions in these categories are rarely related to TB. |
| S, T, V, W, X, Y | External causes of morbidity and mortality | Almost all cases belong to the emergency department, but ED data are also recorded in the OPD database |
| Z | Factors influencing health status and contact with health services | These are not codes for hospitalized comorbidities |
| Characteristics | TB Case | Concurrent Matched Controls | Concurrent Matched Sets |
|---|---|---|---|
| Age group, n (%) | |||
| Male | |||
| 1–10 | 30 (5.1) | 119 (5.6) | 26 (6.2) |
| 11–20 | 16 (2.7) | 64 (3.0) | 13 (3.1) |
| 21–30 | 77 (13.2) | 291 (13.7) | 51 (12.2) |
| 31–40 | 74 (12.7) | 281 (13.3) | 47 (11.3) |
| 41–50 | 75 (12.9) | 251 (11.9) | 53 (12.7) |
| 51–60 | 67 (11.5) | 219 (10.3) | 49 (11.8) |
| 61–70 | 43 (7.4) | 141 (6.7) | 28 (6.7) |
| 71–80 | 36 (6.2) | 126 (6.0) | 22 (5.3) |
| Female | |||
| 1–10 | 34 (5.8) | 136 (6.4) | 26 (6.2) |
| 11–20 | 14 (2.4) | 51 (2.4) | 13 (3.1) |
| 21–30 | 29 (5.0) | 112 (5.3) | 23 (5.5) |
| 31–40 | 32 (5.5) | 121 (5.7) | 26 (6.2) |
| 41–50 | 16 (2.7) | 58 (2.7) | 12 (3.0) |
| 51–60 | 15 (2.6) | 57 (2.7) | 11 (2.6) |
| 61–70 | 11 (1.9) | 40 (1.9) | 8 (1.9) |
| 71–80 | 14 (2.4) | 51 (2.4) | 9 (2.2) |
| ICD-10 | Diagnosis | Case | Control | Median Preceding Weeks (IQR) | Conditional ROR (95% CI) | |||
|---|---|---|---|---|---|---|---|---|
| Exposed (a) | Not Exposed (b) | Exposed (c) | Not Exposed (d) | p-Value | ||||
| J18.9 | Unspecified pneumonia | 33 | 550 | 39 | 2079 | 31 (19, 42) | 3.10 (1.91, 4.98) | <0.001 |
| E87.6 | Hypokalemia | 30 | 553 | 99 | 2019 | 30 (17, 40) | 1.04 (0.68, 1.61) | 0.854 |
| J15.9 | Unspecified bacterial pneumonia | 21 | 562 | 35 | 2083 | 23 (14, 33) | 2.13 (1.21, 3.74) | 0.008 |
| E87.1 | hypo-osmolality and hyponatremia 1 | 20 | 563 | 33 | 2085 | 25 (18, 37) | 2.14 (1.18, 3.87) | 0.012 |
| J90 | Unclassified pleural effusion | 17 | 566 | 9 | 2109 | 30 (21, 46) | 6.15 (2.68, 14.14) | <0.001 * |
| R04.2 | Hemoptysis | 10 | 573 | 1 | 2117 | 30 (13, 36) | 34.69 (4.40, 273.39) | <0.001 * |
| J44.1 | Unspecified COPD with acute exacerbation | 10 | 573 | 21 | 2097 | 27 (17, 39) | 1.63 (0.75, 3.55) | 0.215 |
| J18.1 | Unspecified lobar pneumonia | 9 | 574 | 6 | 2112 | 24 (20, 34) | 6.19 (2.05, 18.77) | 0.001 |
| A09.9 | Unspecified gastroenteritis and colitis | 9 | 574 | 50 | 2068 | 29 (21, 41) | 0.63 (0.31, 1.30) | 0.212 |
| R50.9 | Unspecified fever | 8 | 575 | 35 | 2083 | 33 (15, 42) | 0.85 (0.39, 1.86) | 0.690 |
| ICD-10 | Principal Diagnosis of the Cases Admitted with E87.1 | Frequency n (%) |
|---|---|---|
| J18.9 | Unspecified pneumonia | 12 (60) |
| R50.9 | Unspecified fever | 3 (15) |
| J15.9 | Unspecified bacterial pneumonia | 2 (10) |
| C34.9 | Malignant neoplasm of bronchus or lung | 2 (10) |
| J18.1 | Unspecified lobar pneumonia | 1 (5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumwichar, P.; Chongsuvivatwong, V. Data Mining for ICD-10 Admission Diagnoses Preceding Tuberculosis within 1 Year among Non-HIV and Non-Diabetes Patients. Trop. Med. Infect. Dis. 2022, 7, 61. https://doi.org/10.3390/tropicalmed7040061
Kumwichar P, Chongsuvivatwong V. Data Mining for ICD-10 Admission Diagnoses Preceding Tuberculosis within 1 Year among Non-HIV and Non-Diabetes Patients. Tropical Medicine and Infectious Disease. 2022; 7(4):61. https://doi.org/10.3390/tropicalmed7040061
Chicago/Turabian StyleKumwichar, Ponlagrit, and Virasakdi Chongsuvivatwong. 2022. "Data Mining for ICD-10 Admission Diagnoses Preceding Tuberculosis within 1 Year among Non-HIV and Non-Diabetes Patients" Tropical Medicine and Infectious Disease 7, no. 4: 61. https://doi.org/10.3390/tropicalmed7040061
APA StyleKumwichar, P., & Chongsuvivatwong, V. (2022). Data Mining for ICD-10 Admission Diagnoses Preceding Tuberculosis within 1 Year among Non-HIV and Non-Diabetes Patients. Tropical Medicine and Infectious Disease, 7(4), 61. https://doi.org/10.3390/tropicalmed7040061