
C-Reactive Protein-to-Albumin Ratio and Clinical Outcomes in COVID-19 Patients: A Systematic Review and Meta-Analysis

 , , and
, , and 
Abstract
:1. Introduction
2. Methods
2.1. Study Design, Register, and Report
2.2. Search Strategy and Data Sources
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Data Extraction
2.6. Quality Assessment
2.7. Data Synthesis and Statistical Analysis
2.8. Publication Bias
3. Results
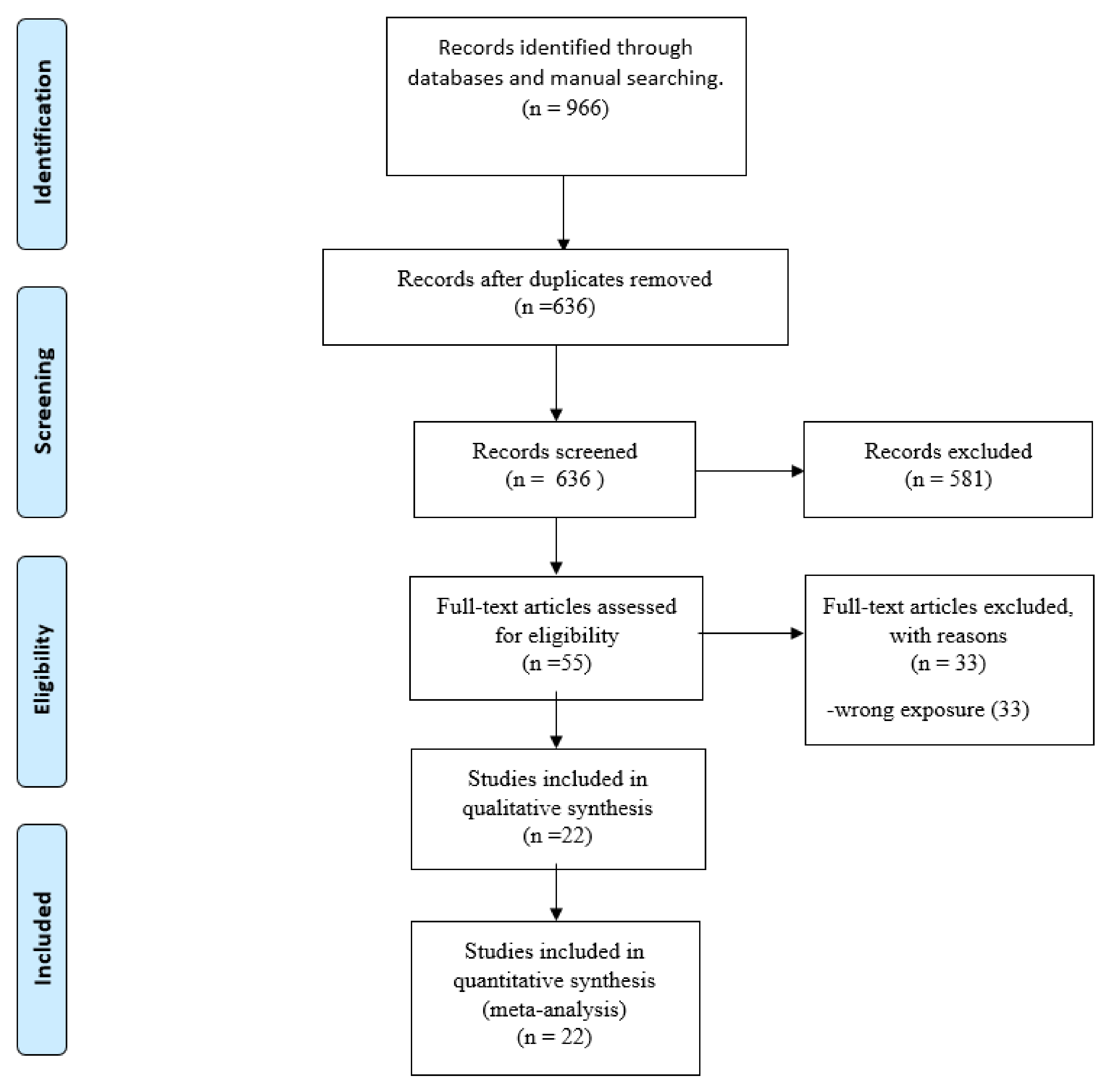
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment
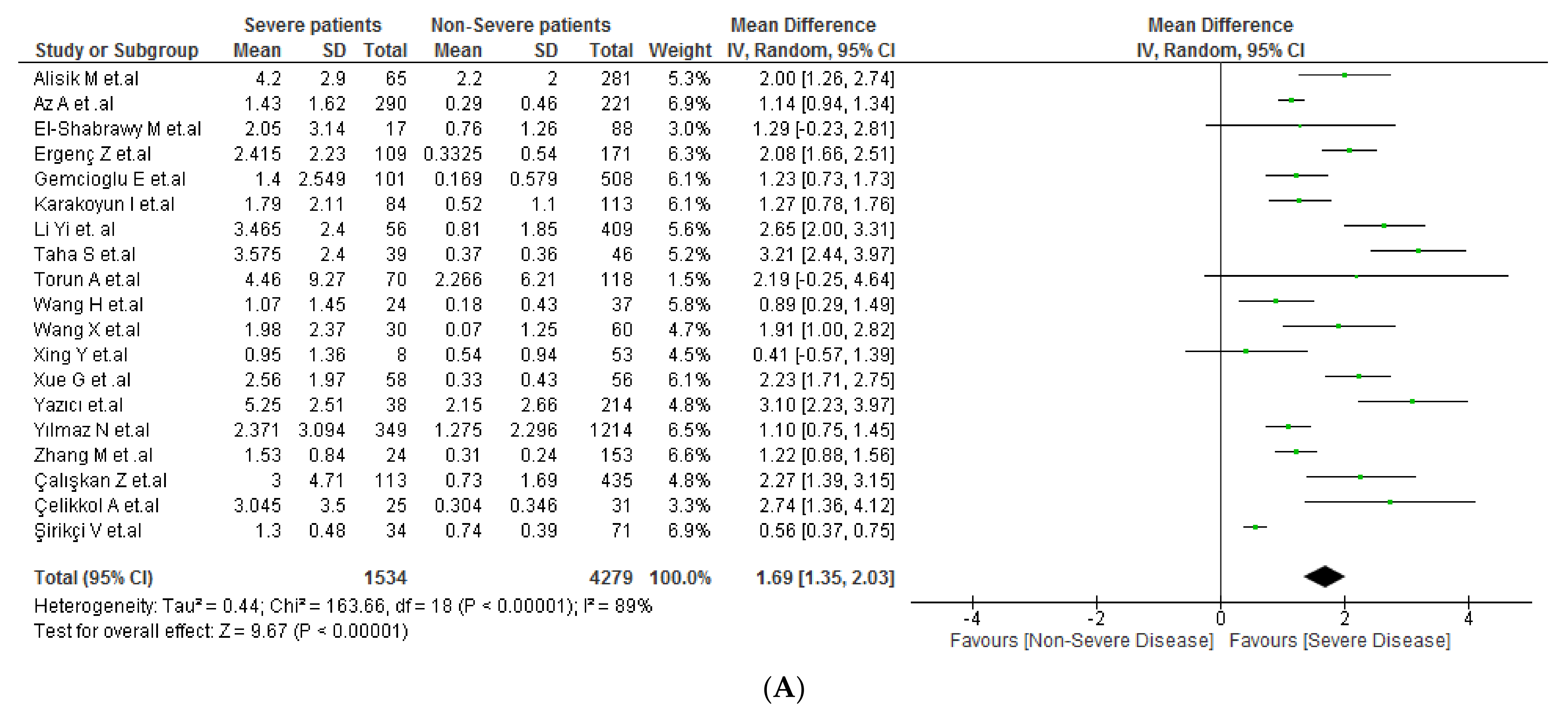
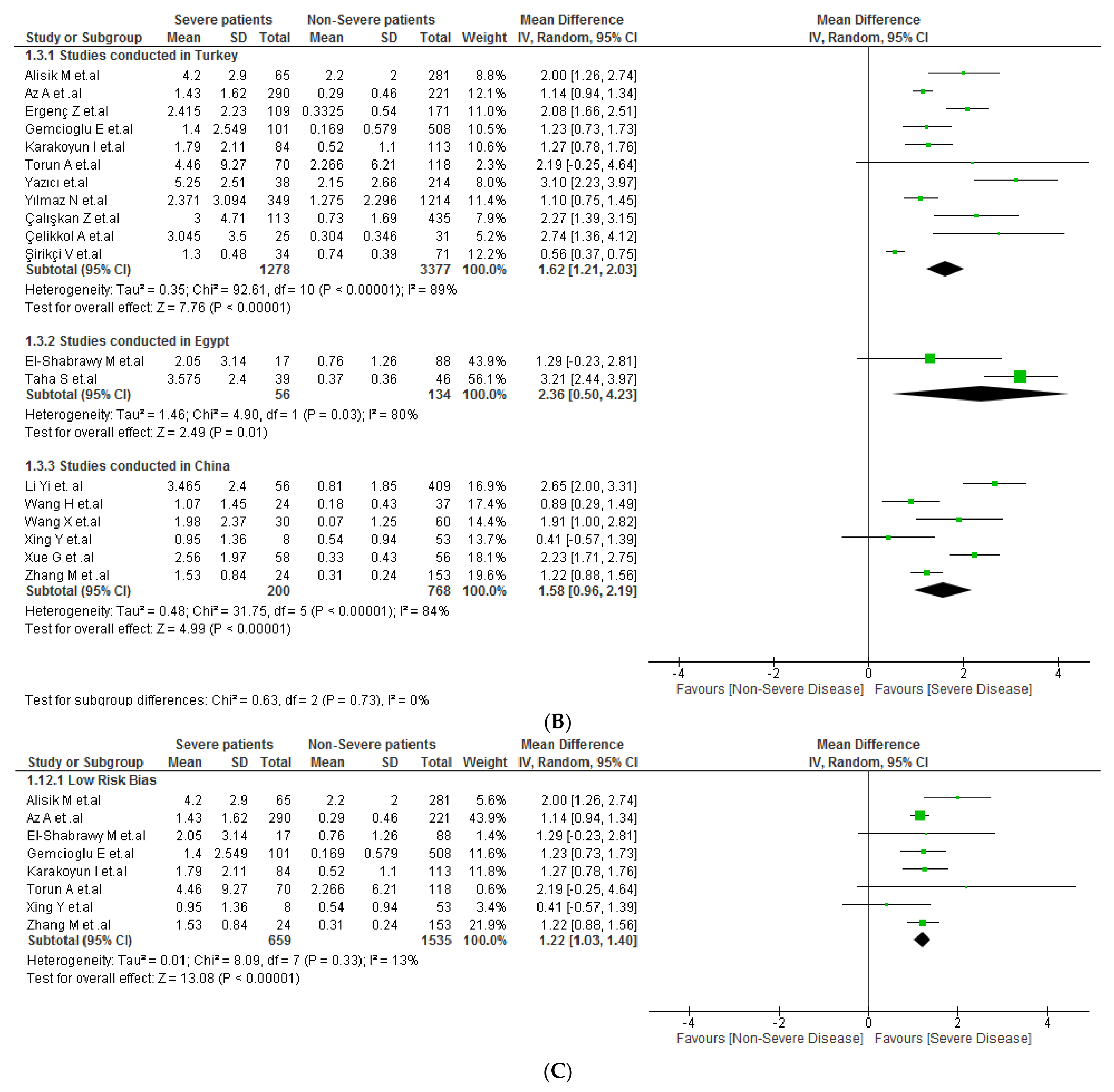
3.4. CAR and COVID-19 Severity
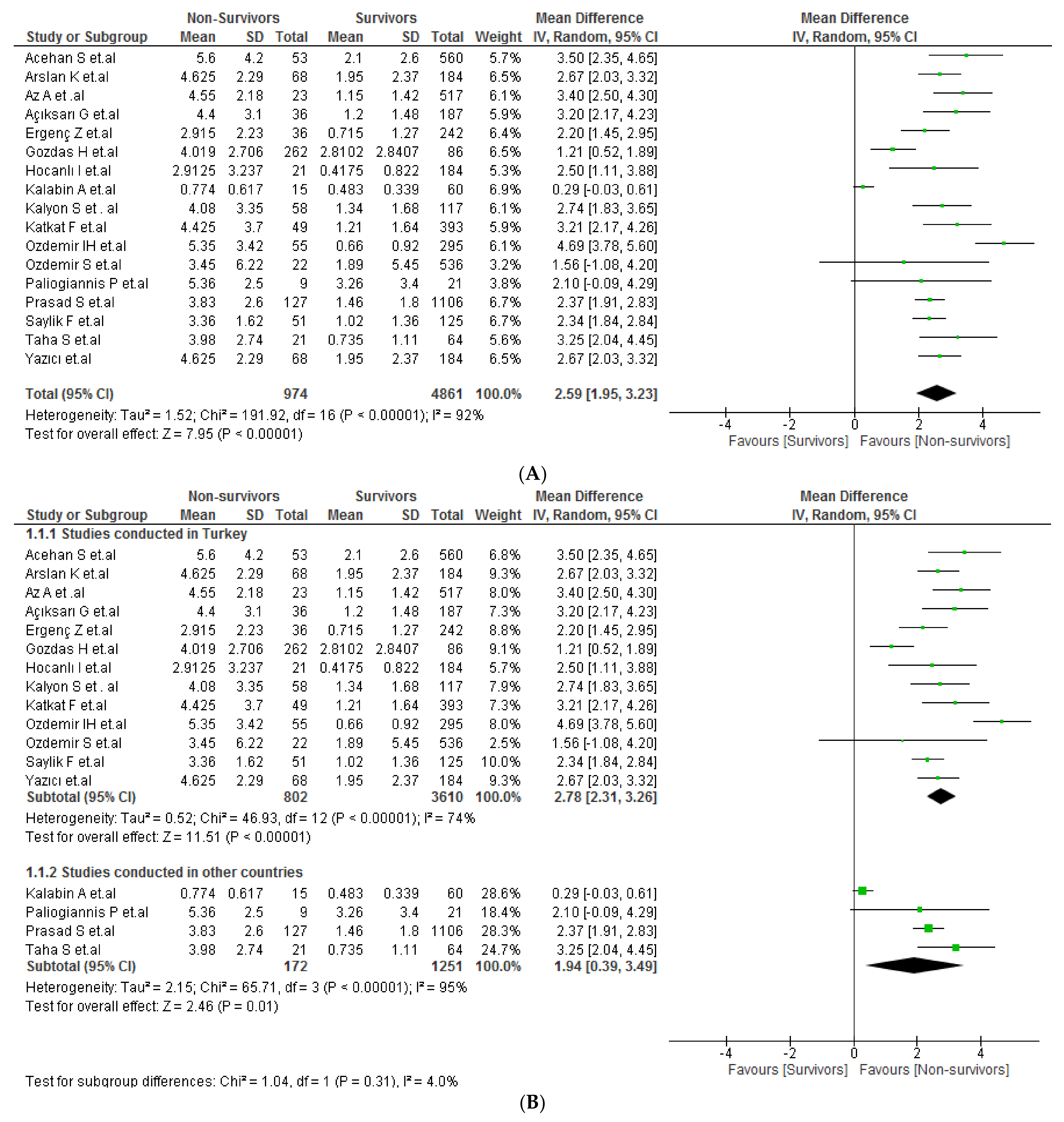
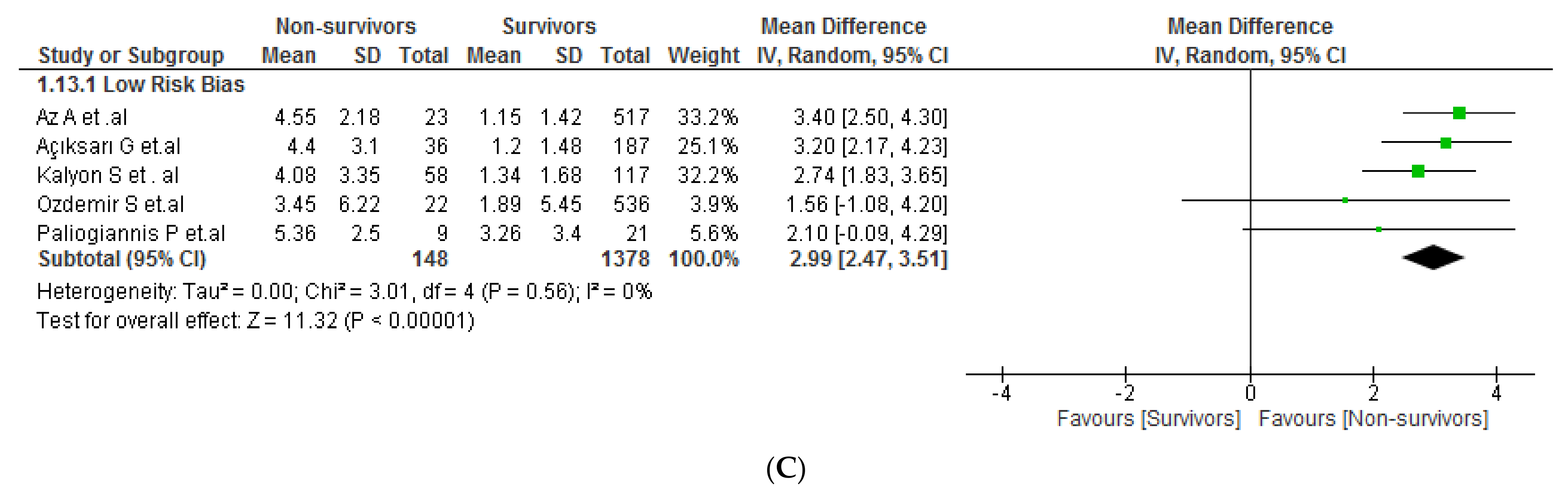
3.5. CAR and COVID-19 Mortality
3.6. Publication Bias
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bonilla-Aldana, D.K.; Quintero-Rada, K.; Montoya-Posada, J.P.; Ramírez-Ocampo, S.; Paniz-Mondolfi, A.; Rabaan, A.A.; Sah, R.; Rodríguez-Morales, A.J. SARS-CoV, MERS-CoV and Now the 2019-Novel CoV: Have We Investigated Enough about Coronaviruses?—A Bibliometric Analysis. Travel Med. Infect. Dis. 2020, 33, 101566. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus (COVID-19) Dashboard | WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 13 November 2021).
- Ray, D.; Salvatore, M.; Bhattacharyya, R.; Wang, L.; Du, J.; Mohammed, S.; Purkayastha, S.; Halder, A.; Rix, A.; Barker, D.; et al. Predictions, Role of Interventions and Effects of a Historic National Lockdown in India’s Response to the COVID-19 Pandemic: Data Science Call to Arms. Harv. Data Sci. Rev. 2020. [Google Scholar] [CrossRef]
- Li, L.Q.; Huang, T.; Wang, Y.Q.; Wang, Z.P.; Liang, Y.; Huang, T.B.; Zhang, H.Y.; Sun, W.; Wang, Y. COVID-19 Patients’ Clinical Characteristics, Discharge Rate, and Fatality Rate of Meta-Analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Tian, W.; Jiang, W.; Yao, J.; Nicholson, C.J.; Li, R.H.; Sigurslid, H.H.; Wooster, L.; Rotter, J.I.; Guo, X.; Malhotra, R. Predictors of Mortality in Hospitalized COVID-19 Patients: A Systematic Review and Meta-analysis. J. Med. Virol. 2020, 92, 1875–1883. [Google Scholar] [CrossRef] [PubMed]
- Ulloque-Badaracco, J.R.; Alarcon-Braga, E.A.; Hernandez-Bustamante, E.A.; Al-kassab-Córdova, A.; Mosquera-Rojas, M.D.; Ulloque-Badaracco, R.R.; Huayta-Cortez, M.A.; Maita-Arauco, S.H.; Herrera-Añazco, P.; Benites-Zapata, V.A. Fibrinogen-to-Albumin Ratio and Blood Urea Nitrogen-to-Albumin Ratio in COVID-19 Patients: A Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2022, 7, 150. [Google Scholar] [CrossRef]
- Ulloque-Badaracco, J.R.; Hernandez-Bustamante, E.A.; Herrera-Añazco, P.; Benites-Zapata, V.A. Prognostic Value of Apolipoproteins in COVID-19 Patients: A Systematic Review and Meta-Analysis. Travel Med. Infect. Dis. 2021, 44, 102200. [Google Scholar] [CrossRef] [PubMed]
- Ulloque-Badaracco, J.R.; Salas-Tello, W.I.; Al-kassab-Córdova, A.; Alarcón-Braga, E.A.; Benites-Zapata, V.A.; Maguiña, J.L.; Hernandez, A.V. Prognostic Value of Neutrophil-to-Lymphocyte Ratio in COVID-19 Patients: A Systematic Review and Meta-Analysis. Int. J. Clin. Pract. 2021, 75, e14596. [Google Scholar] [CrossRef]
- Ulloque-Badaracco, J.R.; Mosquera-Rojas, M.D.; Hernandez-Bustamante, E.A.; Alarcón-Braga, E.A.; Herrera-Añazco, P.; Benites-Zapata, V.A. Prognostic Value of Albumin-to-Globulin Ratio in COVID-19 Patients: A Systematic Review and Meta-Analysis. Heliyon 2022, 8, e09457. [Google Scholar] [CrossRef]
- Kim, M.H.; Ahn, J.Y.; Song, J.E.; Choi, H.; Ann, H.W.; Kim, J.K.; Kim, J.H.; Jeon, Y.D.; Kim, S.B.; Jeong, S.J.; et al. The C-Reactive Protein/Albumin Ratio as an Independent Predictor of Mortality in Patients with Severe Sepsis or Septic Shock Treated with Early Goal-Directed Therapy. PLoS ONE 2015, 10, e0132109. [Google Scholar] [CrossRef]
- Luo, B.; Sun, M.; Huo, X.; Wang, Y. Two New Inflammatory Markers Related to the CURB-65 Score for Disease Severity in Patients with Community-Acquired Pneumonia: The Hypersensitive C-Reactive Protein to Albumin Ratio and Fibrinogen to Albumin Ratio. Open Life Sci. 2021, 16, 84–91. [Google Scholar] [CrossRef]
- Zhang, D.; Yan, H.; Wei, Y.; Liu, X.; Zhuang, Z.; Dai, W.; Li, J.; Li, W.; Hang, C. C-Reactive Protein/Albumin Ratio Correlates With Disease Severity and Predicts Outcome in Patients With Aneurysmal Subarachnoid Hemorrhage. Front. Neurol. 2019, 10, 1186. [Google Scholar] [CrossRef]
- Feketea, G.M.; Vlacha, V. The Diagnostic Significance of Usual Biochemical Parameters in Coronavirus Disease 19 (COVID-19): Albumin to Globulin Ratio and CRP to Albumin Ratio. Front. Med. 2020, 7, 566591. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- McGowan, J.; Sampson, M.; Salzwedel, D.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App Forsystematic Reviews. Syst. Rev. 2016, 5, 1–10. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 September 2021).
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the Sample Mean and Standard Deviation from the Sample Size, Median, Range and/or Interquartile Range. BMC Med. Res. Methodol. 2014, 14, 1–13. [Google Scholar] [CrossRef]
- Zhang, M.; Xiao, E.; Liu, J.; Cai, Y.; Yu, Q. An Emerging Marker Predicting the Severity of COVID-19: Neutrophil-Lymphocyte Count Ratio. ResearchSquare 2020. [Google Scholar] [CrossRef]
- Acehan, S.; Gülen, M.; Işıkber, C.; Kaya, A.; Unlu, N.; İnce, Ç.; Toptaş Fırat, B.; Köksaldı Şahin, G.; Erdem Sümbül, H.; Satar, S. C-Reactive Protein to Albumin Ratio Is Associated with Increased Risk of Mortality in COVID-19 Pneumonia Patients. Cukurova Med. J. 2021, 46, 1449–1458. [Google Scholar] [CrossRef]
- Açıksarı, G.; Koçak, M.; Çağ, Y.; Altunal, L.N.; Atıcı, A.; Çelik, F.B.; Bölen, F.; Açıksarı, K.; Çalışkan, M. Prognostic Value of Inflammatory Biomarkers in Patients with Severe COVID-19: A Single-Center Retrospective Study. Biomark. Insights 2021, 16. [Google Scholar] [CrossRef]
- Alisik, M.; Erdogan, U.; Ates, M.; Sert, M.; Yis, O.; Bugdayci, G. Predictive Values of Immature Granulocyte and Other Inflammatory Parameters on Disease Severity of COVID-19 Patients. Int. J. Med. Biochem. 2021, 4, 143–149. [Google Scholar] [CrossRef]
- Az, A.; Sogut, O.; Akdemir, T.; Ergenc, H.; Dogan, Y.; Cakirca, M. Impacts of Demographic and Clinical Characteristics on Disease Severity and Mortality in Patients with Confirmed COVID-19. Int. J. Gen. Med. 2021, 14, 2989–3000. [Google Scholar] [CrossRef] [PubMed]
- El-Shabrawy, M.; Alsadik, M.E.; El-Shafei, M.; Abdelmoaty, A.A.; Alazzouni, A.S.; Esawy, M.M.; Shabana, M.A. Interleukin-6 and C-Reactive Protein/Albumin Ratio as Predictors of COVID-19 Severity and Mortality. Egypt. J. Bronchol. 2021, 15, 1–7. [Google Scholar] [CrossRef]
- Gemcioglu, E.; Davutoglu, M.; Catalbas, R.; Karabuga, B.; Kaptan, E.; Aypak, A.; Kalem, A.K.; Ozdemir, M.; Yescedililova, N.Y.; Kalkan, E.A.; et al. Predictive Values of Biochemical Markers as Early Indicators for Severe COVID-19 Cases in Admission. Future Virol. 2021, 16, 353–367. [Google Scholar] [CrossRef]
- Kalabin, A.; Mani, V.R.K.; Valdivieso, S.C.; Donaldson, B. Does C Reactive Protein/Albumin Ratio Have Prognostic Value in Patients with COVID-19. J. Infect. Dev. Ctries. 2021, 15, 1086–1093. [Google Scholar] [CrossRef]
- Kalyon, S.; Gültop, F.; Şimşek, F.; Adaş, M. Relationships of the Neutrophil-Lymphocyte and CRP-Albumin Ratios with the Duration of Hospitalization and Fatality in Geriatric Patients with COVID-19. J. Int. Med. Res. 2021, 49. [Google Scholar] [CrossRef]
- Karakoyun, I.; Colak, A.; Turken, M.; Altin, Z.; Arslan, F.D.; Iyilikci, V.; Yilmaz, N.; Kose, S. Diagnostic Utility of C-Reactive Protein to Albumin Ratio as an Early Warning Sign in Hospitalized Severe COVID-19 Patients. Int. Immunopharmacol. 2021, 91, 107285. [Google Scholar] [CrossRef]
- Özdemir, İ.H.; Özlek, B.; Çetin, N. Permanent Atrial Fibrillation Portends Poor Outcomes in Hospitalized Patients with COVID-19: A Retrospective Observational Study. J. Electrocardiol. 2021, 65, 113–120. [Google Scholar] [CrossRef]
- Özdemir, S.; Akça, H.Ş.; Algın, A.; Altunok, İ.; Eroğlu, S.E. Effectiveness of the Rapid Emergency Medicine Score and the Rapid Acute Physiology Score in Prognosticating Mortality in Patients Presenting to the Emergency Department with COVID-19 Symptoms. Am. J. Emerg. Med. 2021, 49, 259–264. [Google Scholar] [CrossRef]
- Paliogiannis, P.; Zinellu, A.; Scano, V.; Mulas, G.; de Riu, G.; Pascale, R.M.; Arru, L.B.; Carru, C.; Pirina, P.; Mangoni, A.A.; et al. Laboratory Test Alterations in Patients with COVID-19 and Non COVID-19 Interstitial Pneumonia: A Preliminary Report. J. Infect. Dev. Ctries 2020, 14, 685–690. [Google Scholar] [CrossRef]
- Saylik, F.; Akbulut, T.; Kaya, S. Can C-Reactive Protein to Albumin Ratio Predict In-Hospital Death Rate Due to COVID-19 in Patients with Hypertension? Angiology 2021, 72, 947–952. [Google Scholar] [CrossRef]
- Sirikci, V.; Findikli, H.A.; Erdogan, M. The Relationship between Disease Severıty and CRP/Albumin Levels in Cases Wıth Covid-19 Pneumonia. J. Pioneer. Med. Sci. 2021, 10, 1–5. Available online: https://www.jpmsonline.com/jpms-vol10-issue2-pages1-5-oa-html/ (accessed on 1 September 2021).
- Taha, S.I.; Shata, A.K.; El-Sehsah, E.M.; Fouad, S.H.; Moussa, A.H.; Abdalgeleel, S.A.; Moustafa, N.M.; Youssef, M.K. The Role of CRP, Interleukin-6 and Their Derived Immune-Inflammatory Indices in Early Prediction of Severity and Mortality of COVID-19 Patients. Microbes and Infectious Diseases 2022, 13–26. [Google Scholar] [CrossRef]
- Torun, A.; Çakirca, T.D.; Çakirca, G.; Portakal, R.D. The Value of C-Reactive Protein/Albumin, Fibrinogen/Albumin, and Neutrophil/Lymphocyte Ratios in Predicting the Severity of CoVID-19. Revista da Associação Médica Brasileira 2021, 67, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Xu, Y.; Huang, H.; Jiang, D.; Zhou, C.; Liao, H.; Chen, X. An Increased Pretreatment C-Reactive Protein-to-Albumin Ratio Predicts Severe Novel Coronavirus-Infected Pneumonia. ResearchSquare 2020. [Google Scholar] [CrossRef]
- Wang, H.; Xing, Y.; Yao, X.; Li, Y.; Huang, J.; Tang, J.; Zhu, S.; Zhang, Y.; Xiao, J. Retrospective Study of Clinical Features of COVID-19 in Inpatients and Their Association with Disease Severity. Med. Sci. Monit. 2020, 26, e927674-1–e927674-9. [Google Scholar] [CrossRef]
- Xing, Y.; Wang, H.; Yao, X.H.; Li, Y.; Huang, J.T.; Tang, J.; Zhu, S.; Liu, Y.Q.; Xiao, J. Analysis of Factors for Disease Progression in 61 Patients with COVID-19 in Xiaogan, Hubei, China. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 12490–12499. [Google Scholar] [CrossRef]
- Xue, G.; Gan, X.; Wu, Z.; Xie, D.; Xiong, Y.; Hua, L.; Zhou, B.; Zhou, N.; Xiang, J.; Li, J. Novel Serological Biomarkers for Inflammation in Predicting Disease Severity in Patients with COVID-19. Int. Immunopharmacol. 2020, 89, 107065. [Google Scholar] [CrossRef]
- Yılmaz Demirci, N.; Uğraş Dikmen, A.; Taşçı, C.; Doğan, D.; Arslan, Y.; Öcal, N.; Taşar, M.; Bozlar, U.; Artuk, C.; Yılmaz, G.; et al. Relationship between Chest Computed Tomography Findings and Clinical Conditions of Coronavirus Disease (COVID-19): A Multicentre Experience. Int. J. Clin. Pract. 2021, 75, e14459. [Google Scholar] [CrossRef]
- Li, Y.; Li, H.; Song, C.; Lu, R.; Zhao, Y.; Lin, F.; Han, D.; Chen, L.; Pan, P.; Dai, M. Early Prediction of Disease Progression in Patients with Severe COVID-19 Using C-Reactive Protein to Albumin Ratio. Dis. Markers 2021, 2021, 1–11. [Google Scholar] [CrossRef]
- Gozdas, H.T.; Kayis, S.A.; Damarsoy, T.; Ozsari, E.; Turkoglu, M.; Yildiz, I.; Demirhan, A. Multi-Inflammatory Index as a Novel Mortality Predictor in Critically Ill COVID-19 Patients. J. Intensive Care Med. 2022, 37. [Google Scholar] [CrossRef]
- Yazar, S.; Arslan, K.; Sehit, S.; Varank, İ.; Baş, S.; Şehit, S. The Relationship between the Prognostic Nutritional Index and the Clinical Course of COVID-19: A Single-Center Experience. J. Med. Palliat. Care 2022, 3, 92–97. [Google Scholar] [CrossRef]
- Hocanli, I.; Kabak, M. The Clinical Importance of C-Reactive Protein to Albumin Ratio (CAR) in Patients Diagnosed with COVID-19. J. Contemp. Med. 2022, 12, 266–270. [Google Scholar] [CrossRef]
- Prasad, S.; Patel, S.; Behera, A.K.; Gitismita, N.; Shah, S.; Nanda, R.; Mohapatra, E. Early Biochemical Markers in Predicting the Clinical Outcome of COVID-19 Patients Admitted in Tertiary Care Hospital in Chhattisgarh, India. J. Lab. Physicians 2022. [Google Scholar] [CrossRef]
- Katkat, F.; Kalyoncuoglu, M.; Karahan, S.; Ozcan, S.; Atam Tasdemir, Z.; Kucuk, H.; Karabulut, U.; Guner, A.; Biter, I.; Nihan, F.; et al. The Predictive Ability of the C-Reactive Protein to Albumin Ratio as A Mortality Predictor in Hospitalized Severe SARS-CoV-2 Infected Patients with Cardiovascular Diseases. Med. Bull. Haseki. 2022, 60, 152–160. [Google Scholar] [CrossRef]
- Ergenc, Z.; Ergenç, H.; Araç, S.; Usanmaz, M.; Alkılınç, E.; Kaya, G.; Karacaer, C.; Nalbant, A.; Kaya, T. Novel Biochemical Prognostic Indicators in COVID-19: Can CRP/Albumin, Urea/Albumin, and LDH/Albumin Ratios Be Used to Predict Mortality and Length of Hospitalization? Med. Sci. Discov. 2022, 9, 310–318. [Google Scholar] [CrossRef]
- Çalışkan, Z.; Bozdağ, E.; Sönmez, S.; Dağıstanlı, S.; Bulut, N.; Dinçer, Y. Assessment of 7 Inflammatory Indexes as an Early Predictor of COVID-19 Severity. Cerrah-Med. J. 2022. [Google Scholar] [CrossRef]
- Çelikkol, A.; Güzel, E.Ç.; Doğan, M.; Erdal, B.; Yilmaz, A. C-Reactive Protein-to-Albumin Ratio as a Prognostic Inflammatory Marker in COVID-19. J. Lab. Physicians 2022, 14, 74–83. [Google Scholar] [CrossRef]
- Yazıcı, M.M.; Altuntaş, G.; Aygün, A.; Nalbant, E. The Value of the C-Reactive Protein/Albumin and Fibrinogen/Albumin Ratios in Predicting Disease Severity and Mortality in Elderly COVID-19 Patients. Med. Sci. Discov. 2022, 9, 362–367. [Google Scholar] [CrossRef]
- Choudhary, S.; Sharma, K.; Silakari, O. The Interplay between Inflammatory Pathways and COVID-19: A Critical Review on Pathogenesis and Therapeutic Options. Microb. Pathog. 2021, 150, 104673. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Japar, K.V.; Kwenandar, F.; Damay, V.; Siregar, J.I.; Lugito, N.P.H.; Tjiang, M.M.; Kurniawan, A. Inflammatory and Hematologic Markers as Predictors of Severe Outcomes in COVID-19 Infection: A Systematic Review and Meta-Analysis. Am. J. Emerg. Med. 2021, 41, 110–119. [Google Scholar] [CrossRef]
- Ghahramani, S.; Tabrizi, R.; Lankarani, K.B.; Kashani, S.M.A.; Rezaei, S.; Zeidi, N.; Akbari, M.; Heydari, S.T.; Akbari, H.; Nowrouzi-Sohrabi, P.; et al. Laboratory Features of Severe vs. Non-Severe COVID-19 Patients in Asian Populations: A Systematic Review and Meta-Analysis. Eur. J. Med. Res. 2020, 25, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kilercik, M.; Demirelce, Ö.; Serdar, M.A.; Mikailova, P.; Serteser, M. A New Haematocytometric Index: Predicting Severity and Mortality Risk Value in COVID-19 Patients. PLoS ONE 2021, 16, e0254073. [Google Scholar] [CrossRef]
- Zhou, W.; Zhang, G.L. C-Reactive Protein to Albumin Ratio Predicts the Outcome in Renal Cell Carcinoma: A Meta-Analysis. PLoS ONE 2019, 14, e0224266. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Hu, X.; Huang, Y.; Xu, W.Y.; Wu, Y.M.; Li, P.F.; Che, G.W. Prognostic Value of the C-Reactive Protein to Albumin Ratio in Esophageal Cancer: A Systematic Review and Meta-Analysis. Kaohsiung. J. Med. Sci. 2020, 36, 54–61. [Google Scholar] [CrossRef]
- Zang, Y.; Fan, Y.; Gao, Z. Pretreatment C-Reactive Protein/Albumin Ratio for Predicting Overall Survival in Pancreatic Cancer: A Meta-Analysis. Medicine 2020, 99, e20595. [Google Scholar] [CrossRef]
- Fan, Y.; Xiang, S.; Dai, Z.; Zou, C.; Wang, X.; Gao, Z. Prognostic Significance of C-Reactive Protein to Albumin Ratio in Colorectal Cancer Patients: A Meta-Analysis. Int. J. Colorectal Dis. 2019, 34, 1105–1111. [Google Scholar] [CrossRef]
- Wong, T.C.; Su, H.Y.; Chen, Y.T.; Wu, P.Y.; Chen, H.H.; Chen, T.H.; Hsu, Y.H.; Yang, S.H. Ratio of C-Reactive Protein to Albumin Predicts Muscle Mass in Adult Patients Undergoing Hemodialysis. PLoS ONE 2016, 1, e0165403. [Google Scholar] [CrossRef]
- Kaplan, M.; Duzenli, T.; Tanoglu, A.; Cakir Guney, B.; Onal Tastan, Y.; Bicer, H.S. Presepsin:Albumin Ratio and C-Reactive Protein:Albumin Ratio as Novel Sepsis-Based Prognostic Scores: A Retrospective Study. Wien. Klin. Wochenschr. 2020, 132, 182–187. [Google Scholar] [CrossRef]
- Oh, T.K.; Song, I.A.; Lee, J.H. Clinical Usefulness of C-Reactive Protein to Albumin Ratio in Predicting 30-Day Mortality in Critically Ill Patients: A Retrospective Analysis. Sci. Rep. 2018, 8, 14977. [Google Scholar] [CrossRef]
- Bai, M.; Wu, Y.; Ji, Z.; Wang, S.; Lin, Z.; Pan, S.; Huang, K. Prognostic Value of C-Reactive Protein/Albumin Ratio in Neurocritically Ill Patients. Minerva Anestesiol. 2019, 85, 1299–1307. [Google Scholar] [CrossRef]
- Ita, K. Coronavirus Disease (COVID-19): Current Status and Prospects for Drug and Vaccine Development. Arch. Med. Res. 2021, 52, 15–24. [Google Scholar] [CrossRef]
- Parasher, A. COVID-19: Current Understanding of Its Pathophysiology, Clinical Presentation and Treatment. Postgrad Med. J. 2021, 97, 312–320. [Google Scholar] [CrossRef]
- Wang, H.; Chang, Y.; Cui, Z.Z.; Liu, Z.J.; Ma, S.F.; Ma, S.F. Admission C-Reactive Protein-to-Albumin Ratio Predicts the 180-Day Mortality of AIDS-Related Pneumocystis Pneumonia. AIDS Res. Hum. Retroviruses 2020, 36, 753–761. [Google Scholar] [CrossRef]
- Duman, H.; Çinier, G.; Bakırcı, E.M.; Duman, H.; Şimşek, Z.; Hamur, H.; Değirmenci, H.; Emlek, N. Relationship Between C-Reactive Protein to Albumin Ratio and Thrombus Burden in Patients with Acute Coronary Syndrome. Clin. Appl. Thromb. Hemost. 2019, 25, 1–6. [Google Scholar] [CrossRef]
- Kocatürk, M.; Kocatürk, Ö. Assessment of Relationship between C-Reactive Protein to Albumin Ratio and 90-Day Mortality in Patients with Acute Ischaemic Stroke. Neurol. Neurochir. Pol. 2019, 53, 205–211. [Google Scholar] [CrossRef]
- Süleymanoğlu, M.; Burak, C.; Gümüşdağ, A.; Yesin, M.; Rencüzoğulları, İ.; Karabağ, Y.; Çağdaş, M.; Çap, M. Assessment of the Relation between C-Reactive Protein to Albumin Ratio and the Severity and Complexity of Peripheral Arterial Disease. Vascular 2020, 28, 731–738. [Google Scholar] [CrossRef]
- Yayla, K.G.; Yayla, Ç. C-Reactive Protein-to-Albumin Ratio and Progression of Abdominal Aortic Aneurysm. Angiology 2021, 72, 490. [Google Scholar] [CrossRef]
- Aksoy, F.; Uysal, D.; Ibrişim, E. Relationship between C-Reactive Protein/Albumin Ratio and New-Onset Atrial Fibrillation after Coronary Artery Bypass Grafting. Revista da Associacao Medica Brasileira (1992) 2020, 66, 1070–1076. [Google Scholar] [CrossRef]
- Babapoor-Farrokhran, S.; Gill, D.; Walker, J.; Rasekhi, R.T.; Bozorgnia, B.; Amanullah, A. Myocardial Injury and COVID-19: Possible Mechanisms. Life Sci. 2020, 253, 117723. [Google Scholar] [CrossRef]
- Long, B.; Brady, W.J.; Koyfman, A.; Gottlieb, M. Cardiovascular Complications in COVID-19. Am. J. Emerg. Med. 2020, 8, 1504–1507. [Google Scholar] [CrossRef]
- Bridwell, R.; Long, B.; Gottlieb, M. Neurologic Complications of COVID-19. Am. J. Emerg. Med. 2020, 38, e3–e7. [Google Scholar] [CrossRef]
- Nannoni, S.; de Groot, R.; Bell, S.; Markus, H.S. Stroke in COVID-19: A Systematic Review and Meta-Analysis. Int. J. Stroke 2021, 16, 137–149. [Google Scholar] [CrossRef]
- Yılmaz, P.Ö.; Karacan, E. The Effects of C-Reactive Protein/Albumin Ratio and Hematologic Parameters on Predicting the Prognosis for Emergency Surgical Patients in Intensive Care. Ulus Travma Acil. Cerrahi. Derg. 2021, 27, 67–72. [Google Scholar] [CrossRef]
- Xu, H.; Hu, L.; Wei, X.; Niu, J.; Gao, Y.; He, J.; Hou, J. The Predictive Value of Preoperative High-Sensitive C-Reactive Protein/Albumin Ratio in Systemic Inflammatory Response Syndrome After Percutaneous Nephrolithotomy. J. Endourol. 2019, 33, 1–8. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, G.; Garcia-Tsao, G.; Pagliaro, L. Natural History and Prognostic Indicators of Survival in Cirrhosis: A Systematic Review of 118 Studies. J. Hepatol. 2006, 44, 217–231. [Google Scholar] [CrossRef]
- Kodner, C. Nephrotic Syndrome in Adults: Diagnosis and Management—PubMed. Am. Fam. Physician 2009, 80, 1129–1134. [Google Scholar]
- Oikonomou, T.; Goulis, I.; Kiapidou, S.; Tagkou, N.; Akriviadis, E.; Papatheodoridis, G.; Cholongitas, E. The Significance of C-Reactive Protein to Albumin Ratio in Patients with Decompensated Cirrhosis. Ann. Gastroenterol. 2020, 33, 667. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Participants (Male) | Mean/Median Age (IQR/SD) | Outcome | CAR Mean (SD) in Severe Patients | CAR Mean (SD) in Non-Severe Patients | CAR Cutoff Value | Area Under the Curve (AUC) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Zhang M et al. [19] | 2020 | China | 177 (99) | 42 (15) | Severity | 1.53 (0.84) | 0.31 (0.24) | 0.73 | 0.908 | 79.2 | 95.1 |
| Karakoyun I et al. [28] | 2021 | Turkey | 197 (108) | 54 (18) | Severity | 1.79 (2.11) | 0.52 (1.1) | 0.9 | 0.718 | 69.1 | 70.8 |
| El-Shabrawy M et al. [24] | 2021 | Egypt | 116 (63) | 54 (20–88) | Severity | 2.05 (3.14) | 0.76 (1.26) | 0.89 | 0.922 | 82.4 | 90.9 |
| Wang X et al. [36] | 2020 | China | 90 (48) | 63 (46–84) | Severity | 1.98 (2.37) | 0.07 (0.125) | 0.296 | 0.812 | 76.7 | 80.4 |
| Xue G et al. [39] | 2020 | China | 114 (64) | 62 (51–70) | Severity | 2.56 (1.97) | 0.33 (0.43) | 0.71 | 0.81 | 82.76 | 80.36 |
| Wang H et al. [37] | 2020 | China | 61 (31) | 53 (40–62) | Severity | 1.07 (1.45) | 0.18 (0.43) | NR | NR | NR | NR |
| Torun A et al. [35] | 2021 | Turkey | 188 (93) | 60 (12) | Severity | 4.46 (9.27) | 2.266 (6.21) | 0.754 | 0.841 | 82.6 | 66.7 |
| Gemcioglu E et al. [25] | 2021 | Turkey | 609 (348) | 49 (26.5) | Severity | 1.4 (2.549) | 0.169 (0.579) | 0.625 | 0.765 | 68.32 | 75.49 |
| Yılmaz N et al. [40] | 2021 | Turkey | 1563 (925) | 51 (19.5) | Severity | 2.37 (3.09) | 1.27 (2.29) | NR | NR | NR | NR |
| Şirikçi V et al. [33] | 2021 | Turkey | 105 (39) | 63 (14) | Severity | 1.3 (0.48) | 0.74 (0.39) | 1 | 0.7 | 76.5 | 76.1 |
| Xing Y et al. [38] | 2020 | China | 61 (31) | 53 (41–63) | Severity | 0.95 (1.36) | 0.54 (0.94) | NR | NR | NR | NR |
| Alisik M et al. [22] | 2021 | Turkey | 326 (168) | 51 (35–68) | Severity | 4.2 (2.9) | 2.2 (2) | 1.21 | 0.86 | 86.2 | 75.9 |
| Li Y et al. [41] | 2021 | China | 465 (248) | 62 (54–69) | Severity | 3.465 (2.4) | 0.81 (1.85) | 1.843 | 0.107 | NR | NR |
| Taha S et al. [34] | 2021 | Egypt | 85 (48) | 55 (42–65). | Severity Mortality | 3.575 (2.4) | 0.37 (0.36) | 1.65 | 0.878 | 76.9 | 95.7 |
| Az A et al. [23] | 2021 | Turkey | 540 (302) | 48 (14.6) | Severity Mortality | 1.43 (1.62) | 0.29 (0.46) | NR | NR | NR | NR |
| Çelikkol A et al. [49] | 2022 | Turkey | 56 (23) | 47.5 (18.8) | Severity | 3.045 (3.4) | 0.304(0.346) | 0.475 | 0.934 | 90.91 | 86.21 |
| Çalışkan Z et al. [48] | 2022 | Turkey | 548 (286) | 64 (21) | Severity | 3 (4.71) | 0.73 (1.69) | 2.19 | 0.763 | 78.55 | 63.11 |
| Ergenç Z et al. [47] | 2022 | Turkey | 280 (133) | 58.34 (18.64) | Severity Mortality | 2.415 (2.23) | 0.3325 (0.54) | NR | NR | NR | NR |
| Yazıcı et al. [50] | 2022 | Turkey | 252 (107) | 77 (70–83) | Severity Mortality | 5.25 (2.51) | 2.15 (2.66) | 4.2 | 0.786 | 73.7 | 75.2 |
| Author | Year | Country | Participants (Male) | Mean/Median Age (IQR/SD) | Outcome | CAR Mean (SD) in Non-Survivors Patients | CAR Mean (SD) in Survivors Patients | CAR Cutoff Value | Area Under the Curve (AUC) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Taha S et al. [34] | 2021 | Egypt | 85 (48) | 55 (42–65). | Mortality Severity | 3.98 (2.74) | 0.735 (1.11) | 4.21 | 0.812 | 57.1 | 90.6 |
| Az A et al. [23] | 2021 | Turkey | 540 (302) | 48 (14.6) | Mortality Severity | 4.55 (2.18) | 1.15 (1.42) | NR | NR | NR | NR |
| Açıksarı G et al. [21] | 2021 | Turkey | 223 (118) | 60 (19) | Mortality | 4.4 (3.1) | 1.2 (1.48) | 0.34 | 0.81 | NR | NR |
| Saylik F et al. [32] | 2021 | Turkey | 176 (51) | 64 (10) | Mortality | 3.36 (1.62) | 1.02 (1.36) | 2.075 | 0.778 | 82.3 | 72.8 |
| Kalabin A et al. [26] | 2021 | United States of America | 75 (49) | 63 (14) | Mortality | 0.774 (0.617) | 0.483 (0.339) | 0.54 | NR | NR | NR |
| Paliogiannis P et al. [31] | 2020 | Italy | 30 (16) | 72 (65–68) | Mortality | 5.36 (2.5) | 3.26 (3.4) | NR | NR | NR | NR |
| Kalyon S et al. [27] | 2020 | Turkey | 175 (72) | 73 (65–95) | Mortality | 4.08 (3.35) | 1.34 (1.68) | 2.3 | 0.781 | 70.69 | 72.65 |
| Özdemir IH et al. [29] | 2021 | Turkey | 350 (194) | 55 (39–70) | Mortality | 5.35 (3.42) | 0.66 (0.92) | NR | NR | NR | NR |
| Özdemir S et al. [30] | 2021 | Turkey | 558 (310) | 48 (19–96) | Mortality | 3.45 (6.22) | 1.89 (5.45) | NR | NR | NR | NR |
| Acehan S et al. [20] | 2021 | Turkey | 613 (358) | 59 (19.5) | Mortality | 5.6 (4.2) | 2.1 (2.6) | 2.1561 | 0.79 | 73.6 | 68.4 |
| Katkat F et al. [46] | 2022 | Turkey | 442 (247) | 58 (18–99) | Mortality | 4.425(3.7) | 1.21(1.64) | 2.2 | 0.809 | 76 | 75 |
| Prasad S et al. [45] | 2022 | India | 1233 (853) | 53.5(15.79) | Mortality | 3.83 (2.6) | 1.46 (1.8) | 2.08 | 0.794 | 70.1 | 27.2 |
| Hocanlı I et al. [44] | 2022 | Turkey | 205 (113) | 53.5 (34.7–87) | Mortality | 2.912 (3.23) | 0.41 (0.82) | 1.39 | 0.862 | 76 | 81 |
| Arslan K et al. [43] | 2022 | Turkey | 1579 (824) | 54 (43–65) | Mortality | 2.34 (1.08) | 0.472 (0.8) | 1.09 | 0.851 | 94.6 | 74.1 |
| Gozdas H et al. [42] | 2022 | Turkey | 348 (205) | 74 (65–83) | Mortality | 4.01 (2.70) | 2.81 (2.84) | NR | NR | NR | NR |
| Ergenç Z et al. [47] | 2022 | Turkey | 280 (133) | 58.34 (18.64) | Mortality Severity | 0.715 (1.27) | 2.915 (2.23) | NR | NR | NR | NR |
| Yazıcı et al. [50] | 2022 | Turkey | 252 (107) | 77 (70–83) | Mortality Severity | 4.625 (2.29) | 1.95 (2.37) | 3 | 0.767 | 76.5 | 70.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zavalaga-Zegarra, H.J.; Palomino-Gutierrez, J.J.; Ulloque-Badaracco, J.R.; Mosquera-Rojas, M.D.; Hernandez-Bustamante, E.A.; Alarcon-Braga, E.A.; Benites-Zapata, V.A.; Herrera-Añazco, P.; Hernandez, A.V. C-Reactive Protein-to-Albumin Ratio and Clinical Outcomes in COVID-19 Patients: A Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2022, 7, 186. https://doi.org/10.3390/tropicalmed7080186
Zavalaga-Zegarra HJ, Palomino-Gutierrez JJ, Ulloque-Badaracco JR, Mosquera-Rojas MD, Hernandez-Bustamante EA, Alarcon-Braga EA, Benites-Zapata VA, Herrera-Añazco P, Hernandez AV. C-Reactive Protein-to-Albumin Ratio and Clinical Outcomes in COVID-19 Patients: A Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease. 2022; 7(8):186. https://doi.org/10.3390/tropicalmed7080186
Chicago/Turabian StyleZavalaga-Zegarra, Hernán J., Juan J. Palomino-Gutierrez, Juan R. Ulloque-Badaracco, Melany D. Mosquera-Rojas, Enrique A. Hernandez-Bustamante, Esteban A. Alarcon-Braga, Vicente A. Benites-Zapata, Percy Herrera-Añazco, and Adrian V. Hernandez. 2022. "C-Reactive Protein-to-Albumin Ratio and Clinical Outcomes in COVID-19 Patients: A Systematic Review and Meta-Analysis" Tropical Medicine and Infectious Disease 7, no. 8: 186. https://doi.org/10.3390/tropicalmed7080186
APA StyleZavalaga-Zegarra, H. J., Palomino-Gutierrez, J. J., Ulloque-Badaracco, J. R., Mosquera-Rojas, M. D., Hernandez-Bustamante, E. A., Alarcon-Braga, E. A., Benites-Zapata, V. A., Herrera-Añazco, P., & Hernandez, A. V. (2022). C-Reactive Protein-to-Albumin Ratio and Clinical Outcomes in COVID-19 Patients: A Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease, 7(8), 186. https://doi.org/10.3390/tropicalmed7080186