
Record Linkage for Malaria Deaths Data Recovery and Surveillance in Brazil

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
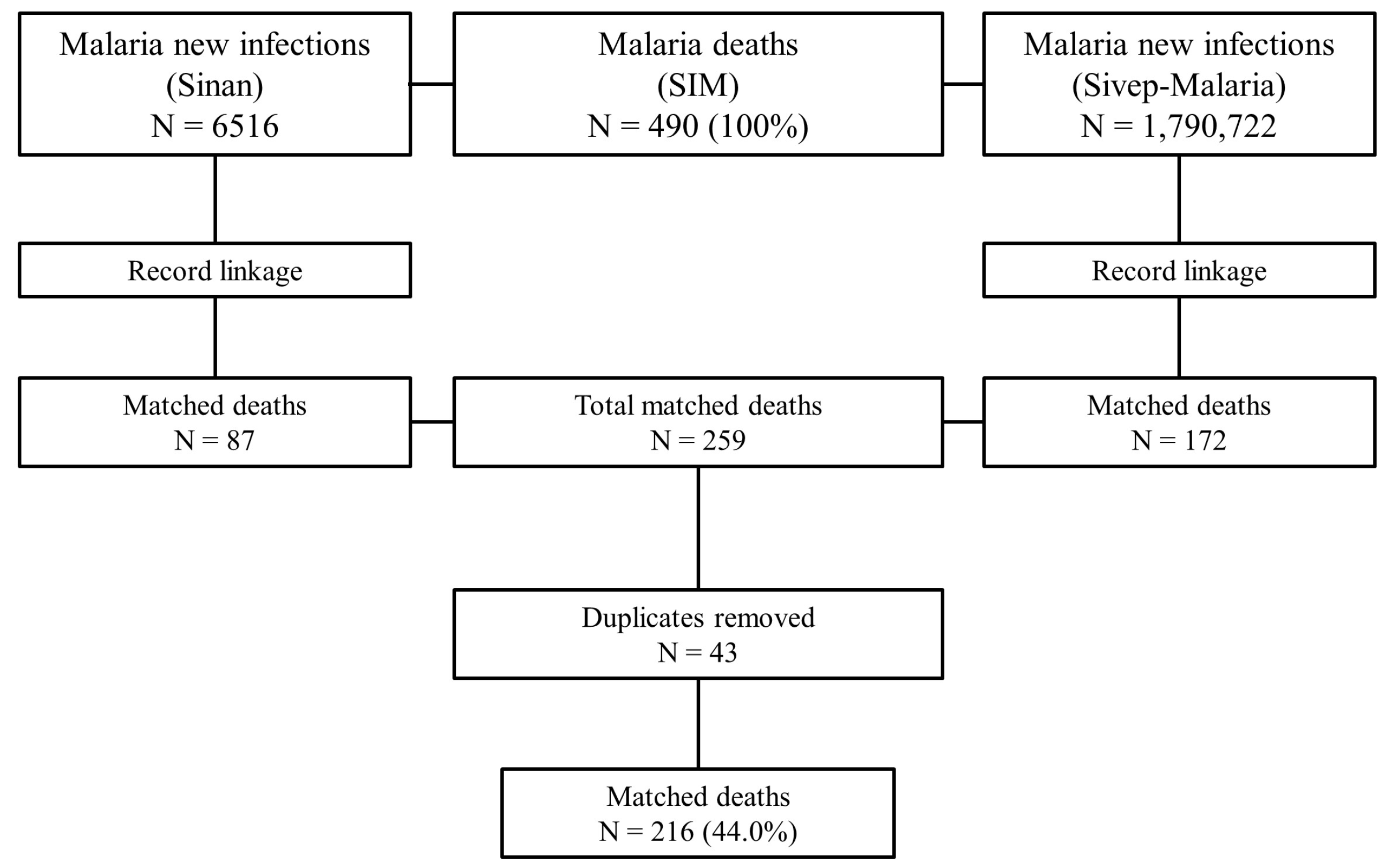
Specific Linkage Procedures
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coelho, G.C.; Chioro, A. Afinal, quantos Sistemas de Informação em Saúde de base nacional existem no Brasil? Cad. Saúde Pública 2021, 37, e00182119. [Google Scholar] [CrossRef] [PubMed]
- Garcia, K.K.S.; de Miranda, C.B.; de Sousa, F.N.E.F. Procedures for health data linkage: Applications in health surveillance. Epidemiol. Serv. Saude 2022, 31, e20211272. [Google Scholar] [CrossRef] [PubMed]
- Avoundjian, T.; Dombrowski, J.C.; Golden, M.R.; Hughes, J.P.; Guthrie, B.L.; Baseman, J.; Sadinle, M. Comparing Methods for Record Linkage for Public Health Action: Matching Algorithm Validation Study. JMIR Public Health Surveill. 2020, 6, e15917. [Google Scholar] [CrossRef] [PubMed]
- Enamorado, T.; Imai, K. Validating Self-Reported Turnout by Linking Public Opinion Surveys with Administrative Records. Public Opin. Q. 2019, 83, 723–748. [Google Scholar] [CrossRef]
- Maia, L.T.S.; Souza, W.V.; Mendes, A.C.G. A contribuição do linkage entre o SIM e SINASC para a melhoria das informações da mortalidade infantil em cinco cidades brasileiras. Rev. Bras. Saúde Matern. Infant. 2015, 15, 57–66. [Google Scholar] [CrossRef]
- Rocha, M.S.; Oliveira, G.P.; Guillen, L.C.T.; Coeli, C.M.; Saraceni, V.; Pinheiro, R.S. Uso de linkage entre diferentes bases de dados para qualificação de variáveis do Sinan-TB e a partir de regras de scripting. Cad. Saúde Pública 2019, 35, e00074318. [Google Scholar] [CrossRef]
- Shah, G.H.; Lertwachara, K.; Ayanso, A. Record linkage in healthcare: Applications, opportunities, and challenges for public health. Int. J. Healthc. Deliv. Reform Initiat. 2010, 2, 29–47. [Google Scholar] [CrossRef]
- Sayers, A.; Ben-Shlomo, Y.; Blom, A.W.; Steele, F. Probabilistic record linkage. Int. J. Epidemiol. 2016, 45, 954–964. [Google Scholar] [CrossRef]
- Zhu, Y.; Matsuyama, Y.; Ohashi, Y.; Setoguchi, S. When to conduct probabilistic linkage vs. deterministic linkage? A simulation study. J. Biomed. Inform. 2015, 56, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Brasil. Ministério da Saúde. Ficha de Notificação Sivep-Malária Atualizado em 30 de jun. 2022. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/publicacoes-svs/malaria/ficha-de-notificacao-sivep-malaria-v03-08-2020.pdf/@@download/file/Ficha%20de%20Notifica%C3%A7%C3%A3o%20Sivep-Mal%C3%A1ria%20v03-08-2020.pdf (accessed on 31 August 2022).
- Brasil. Ministério da Saúde. Portal Sinan–Malária: Ficha de Notificação/Investigação Individual Para Malária. Available online: http://portalsinan.saude.gov.br/images/documentos/Agravos/Malaria/Malaria_v5.pdf (accessed on 31 August 2022).
- Lorenz, C.; Virginio, F.; Aguiar, B.S.; Suesdek, L.; Chiaravalloti-Neto, F. Spatial and temporal epidemiology of malaria in extra-Amazonian regions of Brazil. Malar J. 2015, 14, 408. [Google Scholar] [CrossRef] [PubMed]
- Garcia, K.K.S.; Abrahão, A.A.; Oliveira, A.F.M.; Henriques, K.M.D.; de Pina-Costa, A.; Siqueira, A.M.; Ramalho, W.M. Malaria time series in the extra-Amazon region of Brazil: Epidemiological scenario and a two-year prediction model. Malaria J. 2022, 21(1), 157. [Google Scholar] [CrossRef] [PubMed]
- Brazilian Ministry of Health. Secretariat of Health Surveillance, Department of Immunization and Communicable Diseases, General Coordination of Surveillance of Zoonoses and Vector-Transmitted Diseases. Epidemiological Bulletin–Malaria: 2020. Nov. 2020; p. 118. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/boletins-epidemiologicos/especiais/2020/boletim_especial_malaria_1dez20_final.pdf (accessed on 31 August 2022).
- Malta, D.C.; Duarte, E.C. Causas de mortes evitáveis por ações efetivas dos serviços de saúde: Uma revisão da literatura. Ciênc Saúde Coletiva 2007, 12, 765–776. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023; Available online: https://www.R-project.org/ (accessed on 31 August 2022).
- Churches, T.; Christen, P.; Lim, K.; Zhu, J.X. Preparation of name and address data for record linkage using hidden Markov models. BMC Med. Inform. Decis. Mak. 2002, 2, 9. [Google Scholar] [CrossRef] [PubMed]
- Yaohao, P.; Mation, L.F. O Desafio do Pareamento de Grandes Bases de Dados: Mapeamento de Métodos de Record Linkage Probabilístico e Diagnóstico de Sua Viabilidade Empírica; Instituto de Pesquisa Econômica Aplicada (IPEA): Rio de Janeiro, Brazil, 2018; ISSN 1415-4765. [Google Scholar]
- Organização Mundial da Saúde (OMS). Malaria. Update at July 26, 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/malaria#:~:text=Left%20untreated%2C%20P.,a%20period%20of%2024%20hours (accessed on 5 September 2022).
- Zhang, S.; Hu, Y.; Bian, G. Research on string similarity algorithm based on Levenshtein Distance. In Proceedings of the 2017 IEEE 2nd Advanced Information Technology, Electronic and Automation Control Conference (IAEAC), Chongqing, China, 25–26 March 2017; pp. 2247–2251. [Google Scholar]
- Liao, H.; Xu, Z. Approaches to manage hesitant fuzzy linguistic information based on the cosine distance and similarity measures for HFLTSs and their application in qualitative decision making. Expert Syst. Appl. 2015, 42, 5328–5336. [Google Scholar] [CrossRef]
- Guo, H.; Li, Y.; Liu, Y.; Li, W.; Li, X. Evaluation of string comparators for record linkage in Chinese environment. Int. J. Wavelets Multiresolut. Inf. Process. 2022, 20, 2250023. [Google Scholar] [CrossRef]
- David, R.; Jennifer, B.; Joran, E. FuzzyJoin. New York: Datacamp. 2020 [update 2020 May 15]. Available online: https://cran.r-project.org/web/packages/fuzzyjoin/fuzzyjoin.pdf (accessed on 2 September 2022).
- Dusetzina, S.B.; Tyree, S.; Meyer, A.M.; Meyer, A.; Green, L.; Carpenter, W.R. Linking Data for Health Services Research: A Framework and Instructional Guide; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2014. [Google Scholar]
- Coeli, C.M.; Saraceni, V.; Medeiros, P.M., Jr.; da Silva Santos, H.P.; Guillen, L.C.T.; Alves, L.G.S.B.; Hone, T.; Millett, C.; Trajman, A.; Durovni, B. Record linkage under suboptimal conditions for data-intensive evaluation of primary care in Rio de Janeiro, Brazil. BMC Med. Inform. Decis. Mak. 2021, 21, 190. [Google Scholar] [CrossRef]
- Castro, C.M.S.; Costa, M.F.L.; Cesar, C.C.; Neves, J.A.B.; Sampaio, R.F. Influência da escolaridade e das condições de saúde no trabalho remunerado de idosos brasileiros. Cien. Saude Colet. 2019, 24, 4153–4162. [Google Scholar] [CrossRef]
- Grannis, S.J.; Overhage, J.M.; Hui, S.; McDonald, C.J. Analysis of a probabilistic record linkage technique without human review. AMIA Annu. Symp. Proc. 2003, 2003, 259–263. [Google Scholar]
- Enamorado, T.; Fifield, B.; Imai, K. FastLink. New York: Datacamp. 2020 [update 2020 Apr 29]. Available online: https://cran.r-project.org/web/packages/fastLink/fastLink.pdf (accessed on 2 September 2022).
- Camarg, K.R.d., Jr.; Coeli, C.M. Reclink: Aplicativo para o relacionamento de bases de dados, implementando o método probabilistic record linkage. Cad. Saúde Pública 2000, 16, 439–447. [Google Scholar] [CrossRef]
- Nahorniak, J.; Bovbjerg, V.; Case, S.; Kincl, L. Application of data linkage techniques to Pacific Northwest commercial fishing injury and fatality data. Inj. Epidemiol. 2021, 8, 26. [Google Scholar] [CrossRef]
- Brasil. Presidência da República. Secretaria-Geral. Subchefia para Assuntos Jurídicos. Lei Geral de Proteção de Dados Pessoais (LGPD)-LEI Nº 13.709, DE 14 DE AGOSTO DE 2018. Available online: http://www.planalto.gov.br/ccivil_03/_ato2015-2018/2018/lei/L13709compilado.htm (accessed on 5 September 2022).
- Coelho, G.E.; Leal, P.L.; Cerroni, M.D.P.; Simplicio, A.C.R.; Siqueira, J.B., Jr. Sensitivity of the Dengue Surveillance System in Brazil for Detecting Hospitalized Cases. PLoS Negl. Trop. Dis. 2016, 10, e0004705. [Google Scholar] [CrossRef]
- Fonseca, M.G.P.; Coeli, C.M.; Lucena, F.D.F.D.A.; Veloso, V.G.; Carvalho, M.S. Accuracy of a probabilistic record linkage strategy applied to identify deaths among cases reported to the Brazilian AIDS surveillance database. Cad. Saúde Pública 2010, 26, 1431–1438. [Google Scholar] [CrossRef]
- Oliveira, G.P.D.; Bierrenbach, A.L.D.S.; Camargo Júnior, K.R.D.; Coeli, C.M.; Pinheiro, R.S. Accuracy of probabilistic and deterministic record linkage: The case of tuberculosis. Rev. Saude Publica 2016, 50. [Google Scholar] [CrossRef]


{kind=link}
| Concordance | Variables Used | Pairs | % |
|---|---|---|---|
| 3 variables | Patient’s name | 65 | 30.1% |
| Mother’s name | |||
| Date of birth | |||
| 2 variables | Patient’s name | 22 | 10.2% |
| Mother’s name | |||
| Patient’s name | 43 | 19.9% | |
| Date of birth | |||
| Mother’s name | 20 | 9.3% | |
| Date of birth | |||
| 1 variable | Patient’s name | 18 | 8.3% |
| Mother’s name | 10 | 4.6% | |
| Date of birth | 38 | 17.6% | |
| Total | 216 | 100.0% | |
| Total Deaths | % | Paired Deaths | % | 95% CI | p-Value (Chi-Squared) | |
|---|---|---|---|---|---|---|
| N = 490 | N = 216 | |||||
| Sex | 0.8 | |||||
| Male | 285 | 58.2% | 128 | 59.3% | (52–66) | |
| Female | 205 | 41.8% | 88 | 40.7% | (34–48) | |
| Age Group | 0.014 | |||||
| <1 | 24 | 4.9% | 9 | 4.2% | (2.0–8.0) | |
| 1–10 | 40 | 8.2% | 21 | 9.7% | (6.3–15) | |
| 11–20 | 38 | 7.8% | 21 | 9.7% | (6.3–15) | |
| 21–30 | 56 | 11.4% | 29 | 13.4% | (9.3–19) | |
| 31–40 | 70 | 14.3% | 46 | 21.3% | (16–27) | |
| 41–50 | 54 | 11% | 32 | 14.8% | (10–20) | |
| 51–60 | 63 | 12.9% | 25 | 11.6% | (7.8–17) | |
| 61–70 | 49 | 10% | 14 | 6.5% | (3.7–11) | |
| 71–80 | 47 | 9.6% | 9 | 4.2% | (2.0–8.0) | |
| >80 | 48 | 9.80% | 10 | 4.60% | (2.4–8.6) | |
| Blank | 1 | 0.20% | - | - | - | |
| Race/Ethnicity | 0.8 | |||||
| White | 120 | 24.50% | 53 | 24.50% | (19–31) | |
| Black | 35 | 7.10% | 14 | 6.50% | (3.7–11) | |
| Yellow | 2 | 0.40% | - | - | - | |
| Brown | 258 | 52.70% | 112 | 51.90% | (45–59) | |
| Indigenous | 65 | 13.30% | 29 | 13.40% | (9.3–19) | |
| Blank | 10 | 2% | 8 | 3.70% | (1.7–7.4) | |
| Years of Education | 0.004 * | |||||
| None | 86 | 17.60% | 18 | 8.30% | (5.2–13) | |
| 1–3 years | 70 | 14.30% | 24 | 11.10% | (7.4–16) | |
| 4–7 years | 74 | 15.10% | 32 | 14.80% | (10–20) | |
| 8–11 years | 76 | 15.50% | 44 | 20.40% | (15–26) | |
| 12 years or more | 56 | 11.40% | 42 | 19.40% | (15–25) | |
| Ignored | 48 | 9.80% | 19 | 8.80% | (5.5–14) | |
| Blank | 80 | 16.30% | 37 | 17.10% | (12–23) | |
| Cause of death (ICD-10) | 0.2 | |||||
| B50–Plasmodium falciparum (Pf) | 101 | 20.6% | 54 | 25% | (19–31) | |
| B51–Plasmodium vivax (Pv) | 183 | 37.3% | 79 | 36.6% | (30–43) | |
| B52–Plasmodium malariae (Pm) | 5 | 1% | 3 | 1.4% | (0.36–4.3) | |
| B53–Other Forms | 6 | 1.2% | 5 | 2.3% | (0.86–5.6) | |
| B54–Not Specified | 151 | 30.8% | 66 | 30.6% | (25–37) | |
| Malaria–associated cause | 44 | 9% | 9 | 4.2% | (2.0–8.0) | |
| Received medical care? | 0.4 | |||||
| Yes | 311 | 63.5% | 150 | 69.4% | (63–75) | |
| No | 49 | 10% | 17 | 7.9% | (4.8–13) | |
| Unknown | 21 | 4.3% | 10 | 4.6% | (2.4–8.6) | |
| Blank | 109 | 22.2% | 39 | 18.1% | (13–24) | |
| Was the death investigated? | 0.3 | |||||
| Yes | 94 | 19.2% | 51 | 23.6% | (18–30) | |
| No | 236 | 48.2% | 94 | 43.5% | (37–50) | |
| Blank | 160 | 32.7% | 71 | 32.9% | (27–40) | |
| Year of Occurrence | >0.9 | |||||
| 2011 | 72 | 14.7% | 29 | 13.4% | (9.3–19) | |
| 2012 | 66 | 13.5% | 32 | 14.8% | (10–20) | |
| 2013 | 45 | 9.2% | 19 | 8.8% | (5.5–14) | |
| 2014 | 38 | 7.8% | 20 | 9.3% | (5.9–14) | |
| 2015 | 38 | 7.8% | 12 | 5.6% | (3.0–9.7) | |
| 2016 | 39 | 8% | 19 | 8.8% | (5.5–14) | |
| 2017 | 39 | 8% | 15 | 6.9% | (4.1–11) | |
| 2018 | 61 | 12.4% | 30 | 13.9% | (9.7–19) | |
| 2019 | 39 | 8% | 14 | 6.5% | (3.7–11) | |
| 2020 | 53 | 10.8% | 26 | 12% | (8.2–17) | |
| State of Occurrence | 0.9 | |||||
| Rondônia | 37 | 7.6% | 14 | 6.5% | (3.7–11) | |
| Acre | 22 | 4.5% | 3 | 1.4% | (0.36–4.3) | |
| Amazonas | 97 | 19.8% | 40 | 18.5% | (14–24) | |
| Roraima | 51 | 10.4% | 17 | 7.9% | (4.8–13) | |
| Pará | 73 | 14.9% | 28 | 13% | (8.9–18) | |
| Amapá | 31 | 6.3% | 18 | 8.3% | (5.2–13) | |
| Tocantins | 2 | 0.4% | 1 | 0.5% | (0.02–3.0) | |
| Maranhão | 20 | 4.1% | 4 | 1.9% | (0.59–5.0) | |
| Piauí | 6 | 1.2% | 4 | 1.9% | (0.59–5.0) | |
| Ceará | 3 | 0.6% | 1 | 0.5% | (0.02–3.0) | |
| Rio Grande do Norte | 3 | 0.6% | 1 | 0.5% | (0.02–3.0) | |
| Paraíba | 2 | 0.4% | - | - | - | |
| Pernambuco | 7 | 1.4% | 2 | 0.9% | (0.16–3.7) | |
| Alagoas | 1 | 0.2% | 1 | 0.5% | (0.02–3.0) | |
| Sergipe | 1 | 0.2% | 1 | 0.5% | (0.02–3.0) | |
| Bahia | 11 | 2.2% | 6 | 2.8% | (1.1–6.2) | |
| Minas Gerais | 25 | 5.1% | 13 | 6% | (3.4–10) | |
| Espírito Santo | 5 | 1% | 3 | 1.4% | (0.36–4.3) | |
| Rio de Janeiro | 9 | 1.8% | 7 | 3.2% | (1.4–6.8) | |
| São Paulo | 33 | 6.7% | 23 | 10.6% | (7.0–16) | |
| Paraná | 5 | 1% | 3 | 1.4% | (0.36–4.3) | |
| Santa Catarina | 6 | 1.2% | 3 | 1.4% | (0.36–4.3) | |
| Rio Grande do Sul | 5 | 1% | 3 | 1.4% | (0.36–4.3) | |
| Mato Grosso do Sul | 2 | 0.4% | 1 | 0.5% | (0.02–3.0) | |
| Mato Grosso | 16 | 3.3% | 8 | 3.7% | (1.7–7.4) | |
| Goiás | 10 | 2.0% | 5 | 2.3% | (0.86–5.6) | |
| Distrito Federal | 7 | 1.4% | 6 | 2.8% | (1.1–6.2) |
| B50—Pf | B51—Pv | B52—Pm | B53—Other Forms of Malaria | B54—Unspecified Malaria | Malaria—Associated Cause | Total | |
|---|---|---|---|---|---|---|---|
| Pf | 39 (72.2%) | 2 (2.5%) | 2 (66.7%) | 1 (20.0%) | 26 (39.4%) | 1 (11.1%) | 71 (32.9%) |
| Pv | 10 (18.5%) | 75 (94.9%) | 0 (0.0%) | 3 (60.0%) | 32 (48.5%) | 7 (77.8%) | 127 (58.8%) |
| Mixed | 4 (7.4%) | 1 (1.3%) | 0 (0.0%) | 1 (20.0%) | 5 (7.6%) | 1 (11.1%) | 12 (5.6%) |
| Pm | 0 (0.0%) | 0 (0.0%) | 1 (33.3%) | 0 (0.0%) | 1 (1.5%) | 0 (0.0%) | 2 (0.9%) |
| P. ovale | 1 (1.9%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (1.5%) | 0 (0.0%) | 2 (0.9%) |
| Non-Pf | 0 (0.0%) | 1 (1.3%) | 0 (0.0%) | 0 (0.0%) | 1 (1.5%) | 0 (0.0%) | 2 (0.9%) |
| Total | 54 (25.0%) | 79 (36.6%) | 3 (1.4%) | 5 (2.3%) | 66 (30.6%) | 9 (4.2%) | 216 (100.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia, K.K.S.; Xavier, D.B.; Soremekun, S.; Abrahão, A.A.; Drakeley, C.; Ramalho, W.M.; Siqueira, A.M. Record Linkage for Malaria Deaths Data Recovery and Surveillance in Brazil. Trop. Med. Infect. Dis. 2023, 8, 519. https://doi.org/10.3390/tropicalmed8120519
Garcia KKS, Xavier DB, Soremekun S, Abrahão AA, Drakeley C, Ramalho WM, Siqueira AM. Record Linkage for Malaria Deaths Data Recovery and Surveillance in Brazil. Tropical Medicine and Infectious Disease. 2023; 8(12):519. https://doi.org/10.3390/tropicalmed8120519
Chicago/Turabian StyleGarcia, Klauss Kleydmann Sabino, Danielly Batista Xavier, Seyi Soremekun, Amanda Amaral Abrahão, Chris Drakeley, Walter Massa Ramalho, and André M. Siqueira. 2023. "Record Linkage for Malaria Deaths Data Recovery and Surveillance in Brazil" Tropical Medicine and Infectious Disease 8, no. 12: 519. https://doi.org/10.3390/tropicalmed8120519
APA StyleGarcia, K. K. S., Xavier, D. B., Soremekun, S., Abrahão, A. A., Drakeley, C., Ramalho, W. M., & Siqueira, A. M. (2023). Record Linkage for Malaria Deaths Data Recovery and Surveillance in Brazil. Tropical Medicine and Infectious Disease, 8(12), 519. https://doi.org/10.3390/tropicalmed8120519