
Prevalence and Infection Intensity of Human and Animal Tungiasis in Napak District, Karamoja, Northeastern Uganda

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
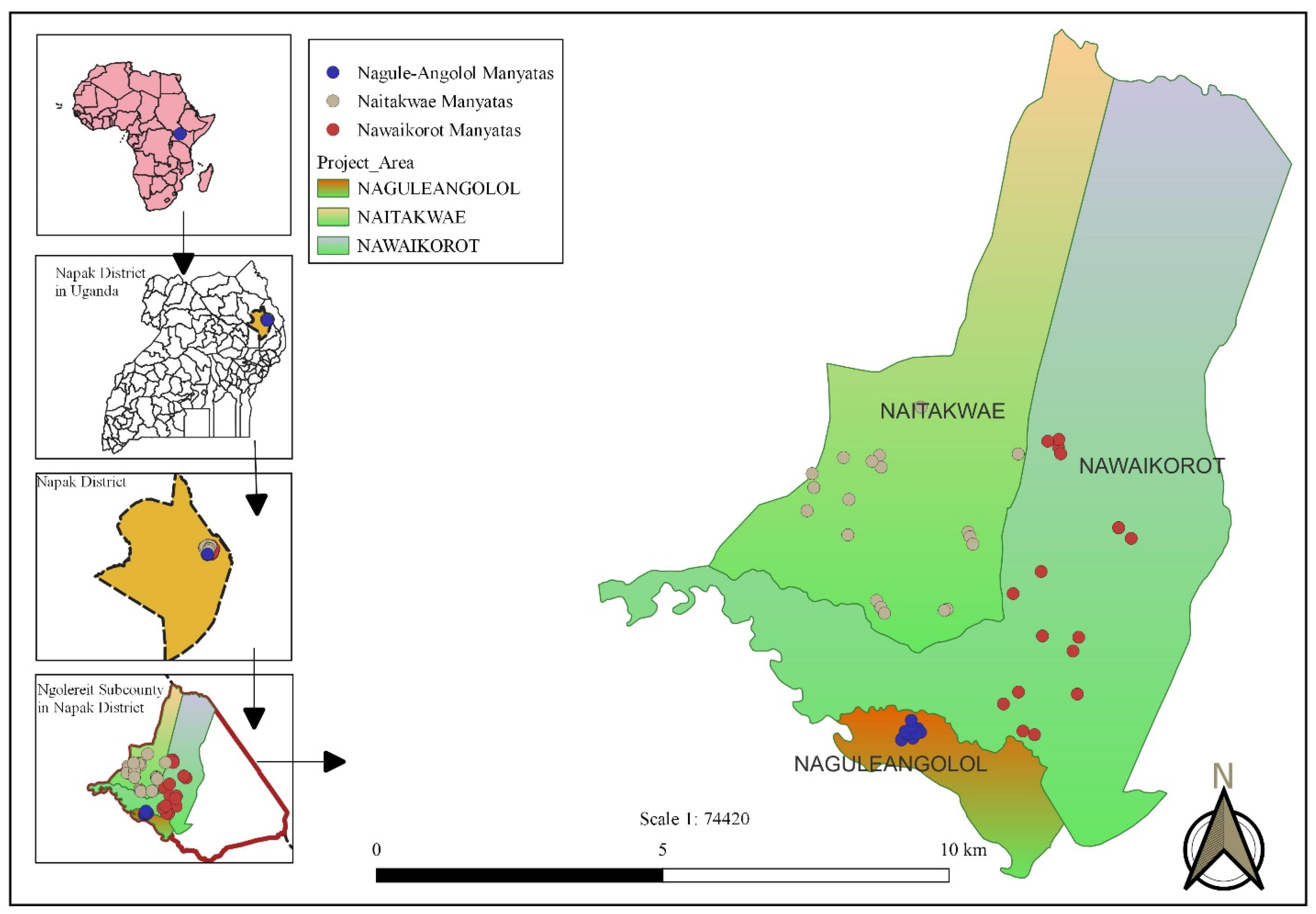
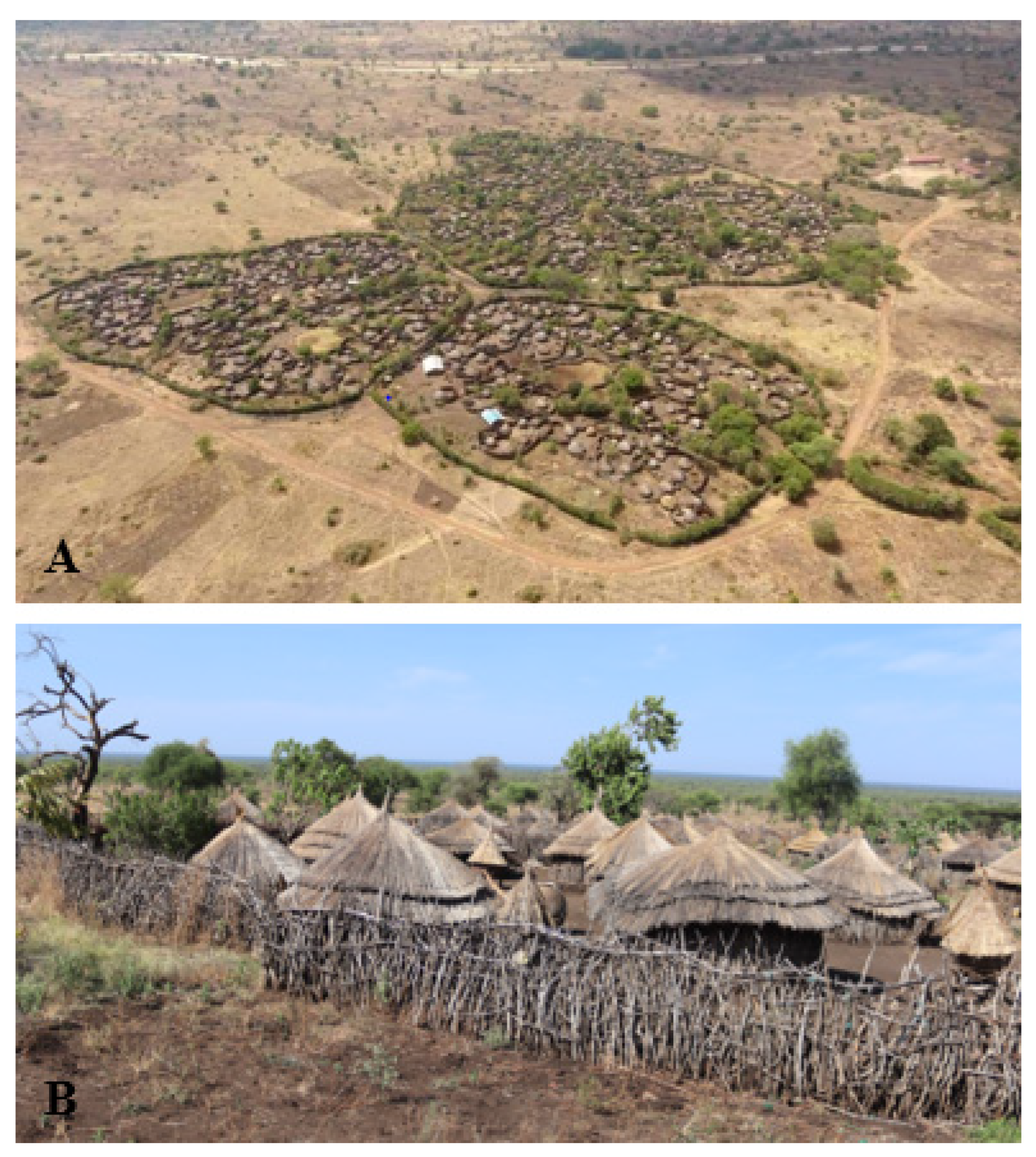
2.1. Study Area and Study Population
2.2. Study Design
2.3. Data Collection
2.4. Data Management and Statistical Analysis
3. Results
3.1. Census and Characteristics of the Study Population
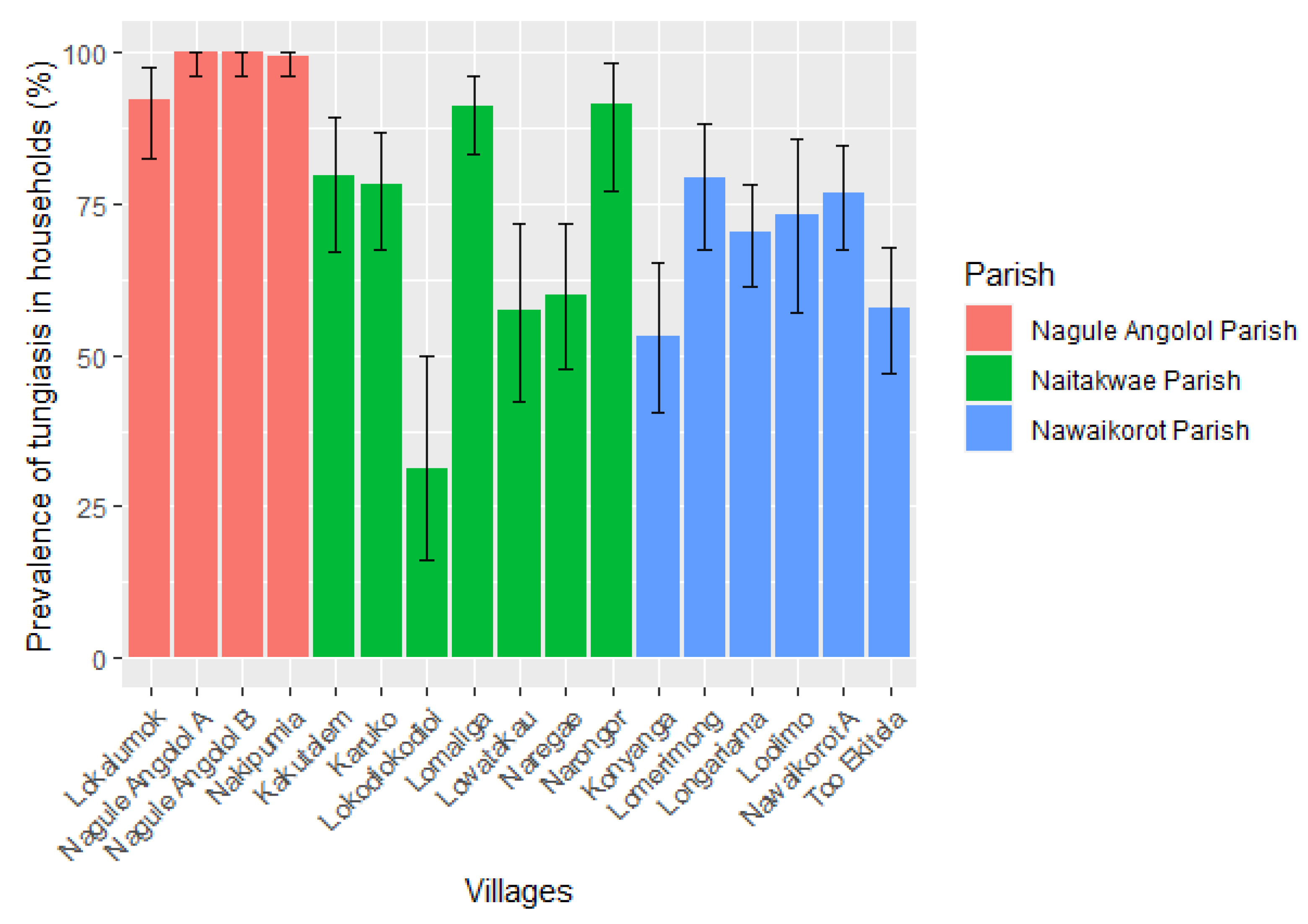
3.2. Prevalence of Tungiasis in Households and Residents
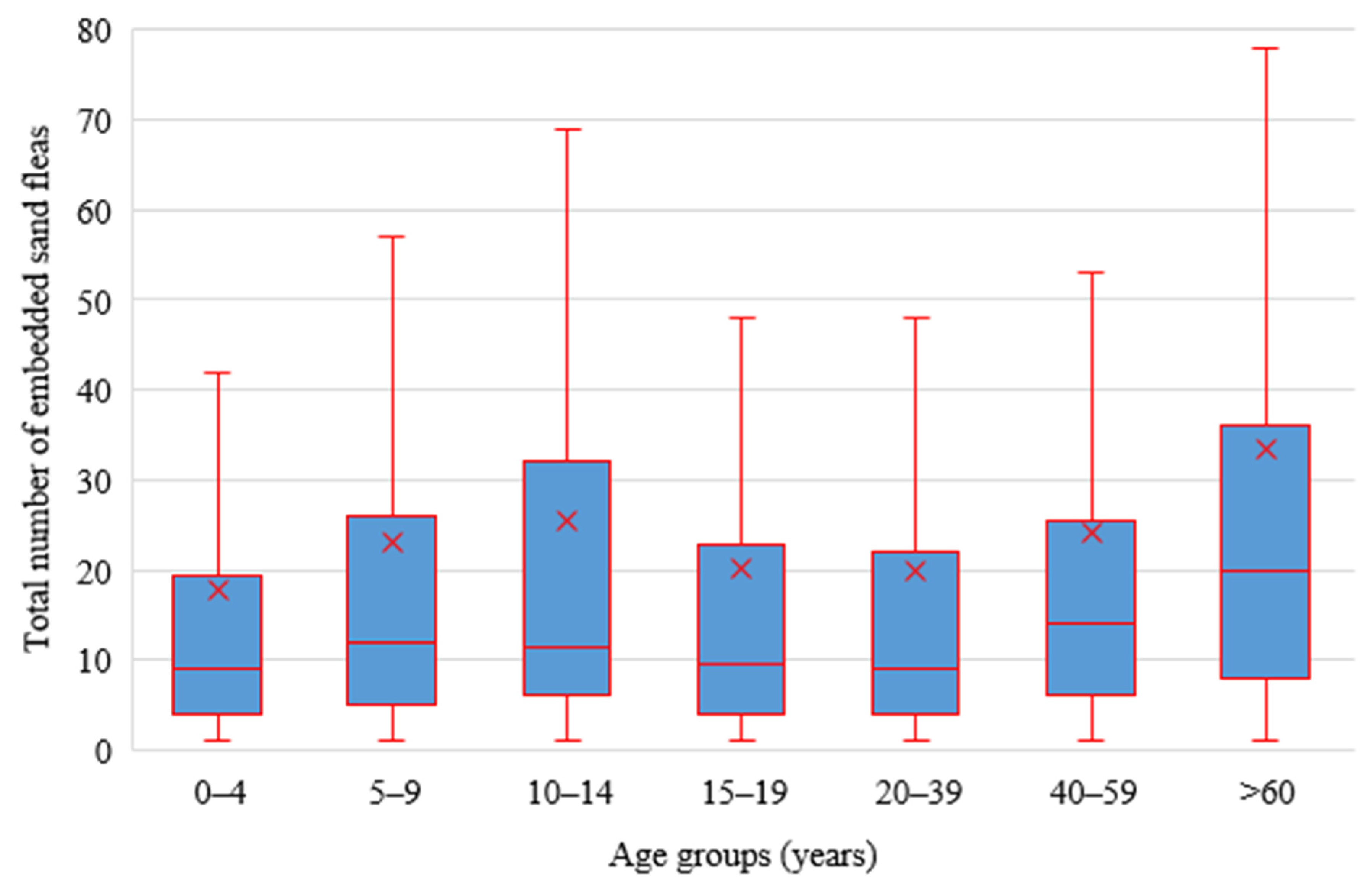
3.3. Intensity of Human Infections
3.4. Occurrence of Other Skin Pathology in Humans
3.5. Tungiasis among Visitors
3.6. Prevalence and Intensity of Animal Tungiasis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heukelbach, J.; De Oliveira, F.A.S.; Hesse, G.; Feldmeier, H. Tungiasis: A neglected health problem of poor communities. Trop. Med. Int. Health 2001, 6, 267–272. [Google Scholar] [CrossRef]
- Feldmeier, H.; Heukelbach, J.; Ugbomoiko, U.S.; Sentongo, E.; Mbabazi, P.; Von Samson-Himmelstjerna, G.; Krantz, I. The International Expert Group for Tungiasis Tungiasis—A Neglected Disease with Many Challenges for Global Public Health. PLoS Negl. Trop. Dis. 2014, 8, e3133. [Google Scholar] [CrossRef] [PubMed]
- Heukelbach, J.; Franck, S.; Feldmeier, H.; Kirk, R.; Sati, M.H. High attack rate of Tunga penetrans (Linnaeus 1758) infestation in an impoverished Brazilian community. Trans. R. Soc. Trop. Med. Hyg. 2004, 98, 431–434. [Google Scholar] [CrossRef] [PubMed]
- Feldmeier, H.; Kehr, J.D.; Poggensee, G.; Heukelbach, J. High exposure to Tunga penetrans (Linnaeus, 1758) correlates with intensity of infestation. Mem. Inst. Oswaldo Cruz 2006, 101, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Ugbomoiko, U.S.; Ofoezie, I.E.; Heukelbach, J. Tungiasis: High prevalence, parasite load, and morbidity in a rural community in Lagos State, Nigeria. Int. J. Dermatol. 2007, 46, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Wiese, S.; Elson, L.; Reichert, F.; Mambo, B.; Feldmeier, H. Prevalence, intensity and risk factors of tungiasis in Kilifi County, Kenya: I. Results from a community-based study. PLoS Negl. Trop. Dis. 2017, 11, e0005925. [Google Scholar] [CrossRef] [PubMed]
- Miller, H.; Ocampo, J.; Ayala, A.; Trujillo, J.T.; Feldmeier, H. Very severe tungiasis in Amerindians in the Amazon lowland of Colombia: A case series. PLoS Negl. Trop. Dis. 2019, 13, e0007068. [Google Scholar] [CrossRef] [PubMed]
- Mutebi, F.; Krücken, J.; Feldmeier, H.; Waiswa, C.; Mencke, N.; Eneku, W.; von Samson-Himmelstjerna, G. High intensity of Tunga penetrans infection causing severe disease among pigs in Busoga, South Eastern Uganda. BMC Vet. Res. 2017, 13, 206. [Google Scholar] [CrossRef]
- Villagrana, S.M.N.; Santisteban, A.G.N. Tungiasis: A highly neglected disease among neglected diseases. Case series from Nduta refugee camp (Tanzania). Oxf. Med. Case Rep. 2019, 2019, omz049. [Google Scholar] [CrossRef] [PubMed]
- Swaminathan, A.; Gosbell, I.; Zwar, N.; Douglas, M.W. Tungiasis in recently arrived African refugees. Med. J. Aust. 2005, 183, 51. [Google Scholar] [CrossRef]
- Nazzaro, G.; Genovese, G.; Veraldi, S. Clinical and histopathologic study of 39 patients with imported tungiasis. J. Cutan. Pathol. 2019, 46, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Linardi, P.M.; Avelar, D.M.D. Neosomes of tungid fleas on wild and domestic animals. Parasitol. Res. 2014, 113, 3517–3533. [Google Scholar] [CrossRef]
- Pampiglione, S.; Fioravanti, M.; Gustinelli, A.; Onore, G.; Mantovani, B.; Luchetti, A.; Trentini, M. Sand flea (Tunga spp.) infections in humans and domestic animals: State of the art. Med. Vet. Entomol. 2009, 23, 172–186. [Google Scholar] [CrossRef]
- Mutebi, F.; Krücken, J.; Feldmeier, H.; von Samsom-Himmelstjerna, G. Clinical implications and treatment options of tungiasis in domestic animals. Parasitol. Res. 2021, 120, 4113–4123. [Google Scholar] [CrossRef] [PubMed]
- Ugbomoiko, U.S.; Ariza, L.; Heukelbach, J. Pigs are the most important animal reservoir for Tunga penetrans (jigger flea) in rural Nigeria. Trop. Dr. 2008, 38, 226–227. [Google Scholar] [CrossRef]
- Heukelbach, J.; Costa, A.M.L.; Wilcke, T.; Mencke, N.; Feldmeier, H. The animal reservoir of Tunga penetrans in severely affected communities of north-east Brazil. Med. Vet. Entomol. 2004, 18, 329–335. [Google Scholar] [CrossRef]
- Mutebi, F.; Krücken, J.; Feldmeier, H.; Waiswa, C.; Mencke, N.; Sentongo, E.; von Samson-Himmelstjerna, G. Animal Reservoirs of Zoonotic Tungiasis in Endemic Rural Villages of Uganda. PLoS Negl. Trop. Dis. 2015, 9, e0004126. [Google Scholar] [CrossRef] [PubMed]
- Pilger, D.; Schwalfenberg, S.; Heukelbach, J.; Witt, L.; Mehlhorn, H.; Mencke, N.; Khakban, A.; Feldmeier, H. Investigations on the biology, epidemiology, pathology, and control of Tunga penetrans in Brazil: VII. The importance of animal reservoirs for human infestation. Parasitol. Res. 2008, 102, 875–880. [Google Scholar] [CrossRef]
- Nagy, N.; Abari, E.; D’Haese, J.; Calheiros, C.; Heukelbach, J.; Mencke, N.; Feldmeier, H.; Mehlhorn, H. Investigations on the life cycle and morphology of Tunga penetrans in Brazil. Parasitol. Res. 2007, 101, 233–242. [Google Scholar] [CrossRef]
- Linardi, P.M.; Calheiros, C.M.L.; Campelo-Junior, E.B.; Duarte, E.M.; Heukelbach, J.; Feldmeier, H. Occurence of off-host stages of Tunga penetrans (Siphonaptera) in various environments in Brazil. Ann. Trop. Med. Parasitol. 2010, 104, 337–345. [Google Scholar] [CrossRef]
- Eisele, M.; Heukelbach, J.; Van Marck, E.; Mehlhorn, H.; Meckes, O.; Franck, S.; Feldmeier, H. Investigations on the biology, epidemiology, pathology and control of Tunga penetrans in Brazil: I. Natural history of tungiasis in man. Parasitol. Res. 2003, 90, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Deka, M. Mapping the Geographic Distribution of Tungiasis in Sub-Saharan Africa. Trop. Med. Infect. Dis. 2020, 5, 122. [Google Scholar] [CrossRef] [PubMed]
- Deka, M.A.; Heukelbach, J. Distribution of tungiasis in Latin America: Identification of areas for potential disease transmission using an ecological niche model. Lancet Reg. Health-Am. 2021, 5, 100080. [Google Scholar] [CrossRef]
- Muehlen, M.; Heukelbach, J.; Wilcke, T.; Winter, B.; Mehlhorn, H.; Feldmeier, H. Investigations on the biology, epidemiology, pathology and control of Tunga penetrans in Brazil II. Prevalence, parasite load, topographic distribution of lesions in the population of a traditional fishing Village. Parasitol. Res. 2003, 90, 449–455. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, R.W.; De Almeida, A.B.; Barbosa-Silva, S.C.; Amorim, M.; Ribeiro, P.C.; Serra-Freire, N.M. The patterns of tungiasis in Araruama township, state of Rio de Janeiro, Brazil. Mem. Inst. Oswaldo Cruz 2003, 98, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Damazio, O.R.D.S.; Silva, M.V.D. Tungiasis in school children in Criciuma, Santa Catarina State, South Brazil. Rev. Inst. Med. Trop. São Paulo 2009, 5, 103–108. [Google Scholar] [CrossRef]
- Mwai, J.; Nyole, D.; Abdi, M.H.; Omogi, J. Factors associated with tungiasis among school-age children in Kwale County, rural Kenya. Int. Health 2022, 15, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Mwangi, J.N.; Ozwara, H.S.; Gicheru, M.M. Epidemiology of tunga penetrans infestation in selected areas in Kiharu constituency, Murang’a County, Kenya. Trop. Dis. Travel Med. Vaccines 2015, 1, 13. [Google Scholar] [CrossRef]
- Elson, L.; Wiese, S.; Feldmeier, H.; Fillinger, U. Prevalence, intensity and risk factors of tungiasis in Kilifi County, Kenya II: Results from a school-based observational study. PLoS Negl. Trop. Dis. 2019, 13, e0007326. [Google Scholar] [CrossRef]
- Nyangacha, R.M.; Odongo, D.; Oyieke, F.; Bii, C.; Muniu, E.; Chasia, S.; Ochwoto, M. Spatial distribution, prevalence and potential risk factors of Tungiasis in Vihiga County, Kenya. PLoS Negl. Trop. Dis. 2019, 13, e0007244. [Google Scholar] [CrossRef] [Green Version]
- Njau, N.N.; Wanzala, P.; Mutugi, M.; Ariza, L.; Heukelbach, J. Tungiasis (jigger infestation) in Rural Kenya, an emerging infectious disease. Retrovirology 2012, 9, P37. [Google Scholar] [CrossRef]
- Njeumi, F.; Nsangou, C.; Ndjend, A.G. Tunga penetrans in Cameroon. Rev. Méd. Vét. 2004, 153, 177–180. [Google Scholar]
- Collins, G.; McLeod, T.; Konfor, N.I.; Lamnyam, C.B.; Ngarka, L.; Njamnshi, N.L. Tungiasis: A neglected health problem in rural Cameroon. Int. J. Collab. Res. Intern. Med. Public Health 2009, 1, 2–10. [Google Scholar]
- Girma, M.; Astatkie, A.; Asnake, S. Prevalence and risk factors of tungiasis among children of Wensho district, southern Ethiopia. BMC Infect. Dis. 2018, 18, 456. [Google Scholar] [CrossRef]
- Jorga, S.D.; Dessie, Y.L.; Kedir, M.R.; Donacho, D.O. Prevalence of Tungiasis and its risk factors of among children of Mettu woreda, southwest Ethiopia, 2020. PLoS ONE 2022, 17, e0262168. [Google Scholar] [CrossRef] [PubMed]
- Ade-Serrano, M.A.; Ejezie, G.C. Prevalence of tungiasis in Oto-Ijanikin village, Badagry, Lagos State, Nigeria. Ann. Trop. Med. Parasitol. 1981, 75, 471–472. [Google Scholar] [CrossRef]
- Arene, F. The prevalence of sand flea (Tunga penetrans) among primary and post-primary school pupils in Choba area of the Niger Delta. Public Health 1984, 98, 282–283. [Google Scholar] [CrossRef]
- Nsanzimana, J.; Karanja, S.; Kayongo, M.; Nyirimanzi, N.; Umuhoza, H.; Murangwa, A.; Muganga, R.; Musafili, A. Factors associated with tungiasis among primary school children: A cross-sectional study in a rural district in Rwanda. BMC Public Health 2019, 19, 1192. [Google Scholar] [CrossRef]
- Mazigo, H.; Bahemana, E.; Konje, E.; Dyegura, O.; Mnyone, L.; Kweka, E.; Kidenya, B.; Heukelbach, J. Jigger flea infestation (tungiasis) in rural western Tanzania: High prevalence and severe morbidity. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 259–263. [Google Scholar] [CrossRef]
- Wafula, S.T.; Ssemugabo, C.; Namuhani, N.; Musoke, D.; Ssempebwa, J.; Halage, A.A. Prevalence and risk factors associated with tungiasis in Mayuge district, Eastern Uganda. Pan Afr. Med. J. 2016, 24, 77. [Google Scholar] [CrossRef] [PubMed]
- Ugbomoiko, U.S.; Ariza, L.; Babamale, A.O.; Heukelbach, J. Prevalence and clinical aspects of tungiasis in south-west Nigerian schoolchildren. Trop. Dr. 2016, 47, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Chadee, D.D. Tungiasis among five communities in South Western Trinidad, West Indies. Ann. Trop. Med. Parasitol. 1998, 92, 107–113. [Google Scholar] [PubMed]
- Harvey, T.V.; Linardi, P.M.; Carlos, R.S.A.; Heukelbach, J. Tungiasis in domestic, wild, and synanthropic animals in Brazil. Acta Trop. 2021, 222, 106068. [Google Scholar] [CrossRef] [PubMed]
- Larson, P.S.; Ono, M.; Changoma, M.; Goto, K.; Kaneko, S.; Moji, K.; Minakawa, N. Presence of dogs and proximity to a wildlife reserve increase household level risk of tungiasis in Kwale, Kenya. Trop. Med. Health 2021, 49, 54. [Google Scholar] [CrossRef]
- Gitau, A.K.; Oyieke, F.A.; Mukabana, W.R. Assessment of the role played by domestic animals in jigger infection in Kandara sub-county, Kenya (case control study). Pan Afr. Med. J. 2021, 39, 231. [Google Scholar]
- Feldmeier, H.; Eisele, M.; Van Marck, E.; Mehlhorn, H.; Ribeiro, R. Investigations on the biology, epidemiology, pathology and control of Tunga penetrans in Brazil: IV. Clinical and histopathology. Parasitol. Res. 2004, 94, 275–282. [Google Scholar] [CrossRef]
- Feldmeier, H.; Eisele, M.; Saboia-Moura, R.C.; Heukelbach, J. Severe tungiasis in underprevileged communities: Case series from Brazil. Emerg. Infect. Dis. 2003, 9, 949–955. [Google Scholar] [CrossRef]
- Feldmeier, H.; Heukelbach, J.; Eisele, M.; Sousa, A.Q.; Barbosa, L.M.M.; Carvalho, C.B.M. Bacterial superinfection in human tungiasis. Trop. Med. Int. Health 2002, 7, 559–564. [Google Scholar] [CrossRef]
- Nyangacha, R.M.; Odongo, D.; Oyieke, F.; Ochwoto, M.; Korir, R.; Ngetich, R.K.; Nginya, G.; Makwaga, O.; Bii, C.; Mwitari, P.; et al. Secondary bacterial infections and antibiotic resistance among tungiasis patients in Western, Kenya. PLoS Negl. Trop. Dis. 2017, 11, e0005901. [Google Scholar] [CrossRef]
- Veraldi, S.; Dassoni, F.; Çuka, E.; Nazzaro, G. Two Cases of Imported Tungiasis with Severe Staphylococcus aureus Superinfection. Acta Derm.-Venereol. 2014, 94, 463–464. [Google Scholar] [CrossRef]
- Vaira, F.; Nazzaro, G.; Veraldi, S. Tungiasis: “the greatest curse that has ever afflicted Africa”. JAMA Dermatol. 2014, 150, 708. [Google Scholar] [PubMed]
- Mazigo, H.D.; Bahamana, E.; Dyegura, O.; Mnyone, L.L.; Kweka, E.J.; Zinga, M.; Konje, E.T.; Waihenya, R.; Heukelbach, J. Severe tungiasis in Western Tanzania: Case series. J. Public Health Afr. 2011, 2, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Tonge, B.L. Tetanus from chigger flea sores. J. Trop. Paediatr. 1989, 35, 94. [Google Scholar] [CrossRef]
- Wilcke, T.; Feldmeier, H.; Heukelbach, J. Severe tungiasis in a patient with Klippel-Trenaunay syndrome. Int. J. Dermatol. 2004, 43, 586–587. [Google Scholar] [CrossRef] [PubMed]
- Heukelbach, J.; Sahebali, S.; Van Marck, E.; Moura, R.S.; Feldmeier, H. An unusual case of ectopic tungiasis with pseudoepitheliomatous hyperplasia. Braz. J. Infect. Dis. 2004, 8, 465–468. [Google Scholar] [CrossRef]
- Wiese, S.; Elson, L.; Feldmeier, H. Tungiasis-related life quality impairment in children living in rural Kenya. PLoS Negl. Trop. Dis. 2018, 12, e0005939. [Google Scholar] [CrossRef]
- Feldmeier, H.; Krantz, I. A way of measuring poverty that could further a change for the better. Bull. World Health Organ. 2008, 2008, 496. [Google Scholar] [CrossRef]
- Ministry of Health Uganda. Sustainability Plan for Neglected Tropical Diseases Control Program 2020–2025; Vector Borne and Neglected Tropical Diseases Division, Ed.; MOH: Kampala, Uganda, 2021; p. 70.
- Mutebi, F.; Krücken, J.; von Samson-Himmelstjerna, G.; Waiswa, C.; Mencke, N.; Eneku, W.; Andrew, T.; Feldmeier, H. Animal and human tungiasis-related knowledge and treatment practices among animal keeping households in Bugiri District, South-Eastern Uganda. Acta Trop. 2018, 177, 81–88. [Google Scholar] [CrossRef] [PubMed]
- United Nations Population Fund. Leaving no One Behind in Karamoja; Population Matters August 2018; UNFPA: Kololo, Kampala, Uganda, 2018; pp. 1–8. [Google Scholar]
- UBOS. The Uganda National Household Survey 2019/2020; UBOS: Kampala, Uganda, 2021.
- Ariza, L.; Wilcke, T.; Jackson, A.; Gomide, M.; Ugbomoiko, U.S.; Feldmeier, H.; Heukelbach, J. A simple method for rapid community assessment of tungiasis. Trop. Med. Int. Health 2010, 15, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Heukelbach, J.; Wilcke, T.; Feldmeier, H.; Harms, G. SEASONAL VARIATION OF TUNGIASIS IN AN ENDEMIC COMMUNITY. Am. J. Trop. Med. Hyg. 2005, 72, 145–149. [Google Scholar] [CrossRef]
- Ugbomoiko, U.S.; Ariza, L.; Ofoezie, I.E.; Heukelbach, J. Risk Factors for Tungiasis in Nigeria: Identification of Targets for Effective Intervention. PLoS Negl. Trop. Dis. 2007, 1, e87. [Google Scholar] [CrossRef]
- Wilcke, T.; Heukelbach, J.; Moura, R.C.S.; Kerr-Pontes, L.R.S.; Feldmeier, H. High prevalence of tungiasis in a poor neighbourhood in Fortaleza, Northeast Brazil. Acta Trop. 2002, 83, 255–258. [Google Scholar] [CrossRef]
- Chadee, D.D. Distribution patterns of Tunga penetrans within a community in South Western Trinidad, West Indies. J. Trop. Med. Hyg. 1994, 97, 167–170. [Google Scholar] [PubMed]
- Chaplin, D.; Byekwaso, F.; Semambo, M.; Mujuni, G.; Bantaze, J.; Nyasimi, M.; Wabyona, E.; Krishnaswamy, S. The Impacts of Climate Change on Food Security and Livelihoods in Karamoja; CGIAR Research Program on Climate Change: Copenhagen, Denmark, 2017. [Google Scholar]
- Muehlen, M.; Feldmeier, H.; Wilcke, T.; Winter, B.; Heukelbach, J. Identifying risk factors for tungiasis and heavy infestation in a resource-poor community in northeast Brazil. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Okoth, A.A. Morbidity, Risk Factors and Flea Species Responsible for Tungiasis in Selected Villages in Kisumu County, Kenya; Kenyatta University: Nairobi, Kenya, 2015. [Google Scholar]
- Thielecke, M.; Raharimanga, V.; Rogier, C.; Stauss-Grabo, M.; Richard, V.; Feldmeier, H. Prevention of Tungiasis and Tungiasis-Associated Morbidity Using the Plant-Based Repellent Zanzarin: A Randomized, Controlled Field Study in Rural Madagascar. PLoS Negl. Trop. Dis. 2013, 7, e2426. [Google Scholar] [CrossRef] [PubMed]
- Winter, B.; Oliveira, F.A.S.; Wilcke, T.; Heukelbach, J.; Feldmeier, H. Tungiasis-related knowledge and treatment practices in two endemic communities in North East Brazil. J. Infect. Dev. Ctries. 2009, 3, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Nordin, P.; Thielecke, M.; Ngomi, N.; Mudanga, G.M.; Krantz, I.; Feldmeier, H. Treatment of tungiasis with a two-component dimeticone: A comparison between moistening the whole foot and directly targeting the embedded sand fleas. Trop. Med. Health 2017, 45, 1–7. [Google Scholar] [CrossRef]
- Thielecke, M.; Nordin, P.; Ngomi, N.; Feldmeier, H. Treatment of Tungiasis with Dimeticone: A Proof-of-Principle Study in Rural Kenya. PLoS Negl. Trop. Dis. 2014, 8, e3058. [Google Scholar] [CrossRef] [PubMed]
- Burgess, I.F. The mode of action of dimeticone 4% lotion against head lice, Pediculus capitis. BMC Pharmacol. 2009, 9, 3. [Google Scholar] [CrossRef]
- Feldmeier, H. Treatment of Parasitic Skin Diseases with Dimeticones A New Family of Compounds with a Purely Physical Mode of Action. Trop. Med. Health 2014, 42, S15–S20. [Google Scholar] [CrossRef]
- Miller, H.; Trujillo-Trujillo, J.; Mutebi, F.; Feldmeier, H. Efficacy and safety of dimeticones in the treatment of epidermal parasitic skin diseases with special emphasis on tungiasis: An evidence-based critical review. Braz. J. Infect. Dis. 2020, 24, 170–177. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Village | Number Examined | Number Infected (n, %) | 95% CI |
|---|---|---|---|
| Naitakwae Parish | |||
| Kakutalem | 165 | 97 (58.8) | 50.9–66.4 |
| Karuko | 223 | 114 (51.1) | 44.4–57.9 |
| Naregae | 189 | 81 (42.9) | 35.7–50.2 |
| Narongor | 124 | 79 (63.7) | 54.6–72.2 |
| Lokodiokodioi | 104 | 12 (11.5) | 6.1–19.3 |
| Lomaliga | 304 | 195 (64.1) | 58.5–69.5 |
| Lowatakau | 138 | 37 (26.8) | 19.6–35.0 |
| Naitakwae prevalence | 1247 | 615 (49.3) | 46.5–52.1 |
| Nawaikorot Parish | |||
| Konyanga | 148 | 68 (46.0) | 37.7–54.3 |
| Nawaikorot A | 240 | 136 (56.7) | 50.1–63.0 |
| Too Ekitela | 210 | 74 (35.2) | 28.8–42.1 |
| Lomerimong | 158 | 92 (58.2) | 50.1–66.0 |
| Longariama | 347 | 150 (43.2) | 38.0–48.6 |
| Loolimo | 91 | 51 (56.0) | 45.3–66.4 |
| Nawaikorot prevalence | 1194 | 571 (47.8) | 45.0–50.7 |
| Nagule Angolol Parish | |||
| Nagule Angolol A | 434 | 399 (91.9) | 89.0–94.3 |
| Nagule Angolol B | 283 | 256 (90.5) | 86.4–93.6 |
| Nakipumia | 629 | 523 (83.1) | 80.0–86.0 |
| Lokalumok | 248 | 170 (68.5) | 62.4–74.3 |
| Nagule Angolol prevalence | 1594 | 1348 (84.6) | 82.7–86.3 |
| Overall | 4035 | 2534 (62.8) | 61.3–64.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mutebi, F.; McNeilly, H.; Thielecke, M.; Reichert, F.; Wiese, S.; Mukone, G.; Feldmeier, H. Prevalence and Infection Intensity of Human and Animal Tungiasis in Napak District, Karamoja, Northeastern Uganda. Trop. Med. Infect. Dis. 2023, 8, 111. https://doi.org/10.3390/tropicalmed8020111
Mutebi F, McNeilly H, Thielecke M, Reichert F, Wiese S, Mukone G, Feldmeier H. Prevalence and Infection Intensity of Human and Animal Tungiasis in Napak District, Karamoja, Northeastern Uganda. Tropical Medicine and Infectious Disease. 2023; 8(2):111. https://doi.org/10.3390/tropicalmed8020111
Chicago/Turabian StyleMutebi, Francis, Hannah McNeilly, Marlene Thielecke, Felix Reichert, Susanne Wiese, George Mukone, and Hermann Feldmeier. 2023. "Prevalence and Infection Intensity of Human and Animal Tungiasis in Napak District, Karamoja, Northeastern Uganda" Tropical Medicine and Infectious Disease 8, no. 2: 111. https://doi.org/10.3390/tropicalmed8020111
APA StyleMutebi, F., McNeilly, H., Thielecke, M., Reichert, F., Wiese, S., Mukone, G., & Feldmeier, H. (2023). Prevalence and Infection Intensity of Human and Animal Tungiasis in Napak District, Karamoja, Northeastern Uganda. Tropical Medicine and Infectious Disease, 8(2), 111. https://doi.org/10.3390/tropicalmed8020111