
Comparison of COVID-19 Severity and Mortality Rates in the First Four Epidemic Waves in Hungary in a Single-Center Study with Special Regard to Critically Ill Patients in an Intensive Care Unit



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Sources
2.2. Definitions
2.3. Participants and Study Size
2.4. Blood Culture Sample Collection and Laboratory Procedures
2.5. Statistical Methods
3. Results
3.1. Epidemiological Description of Epidemic Waves
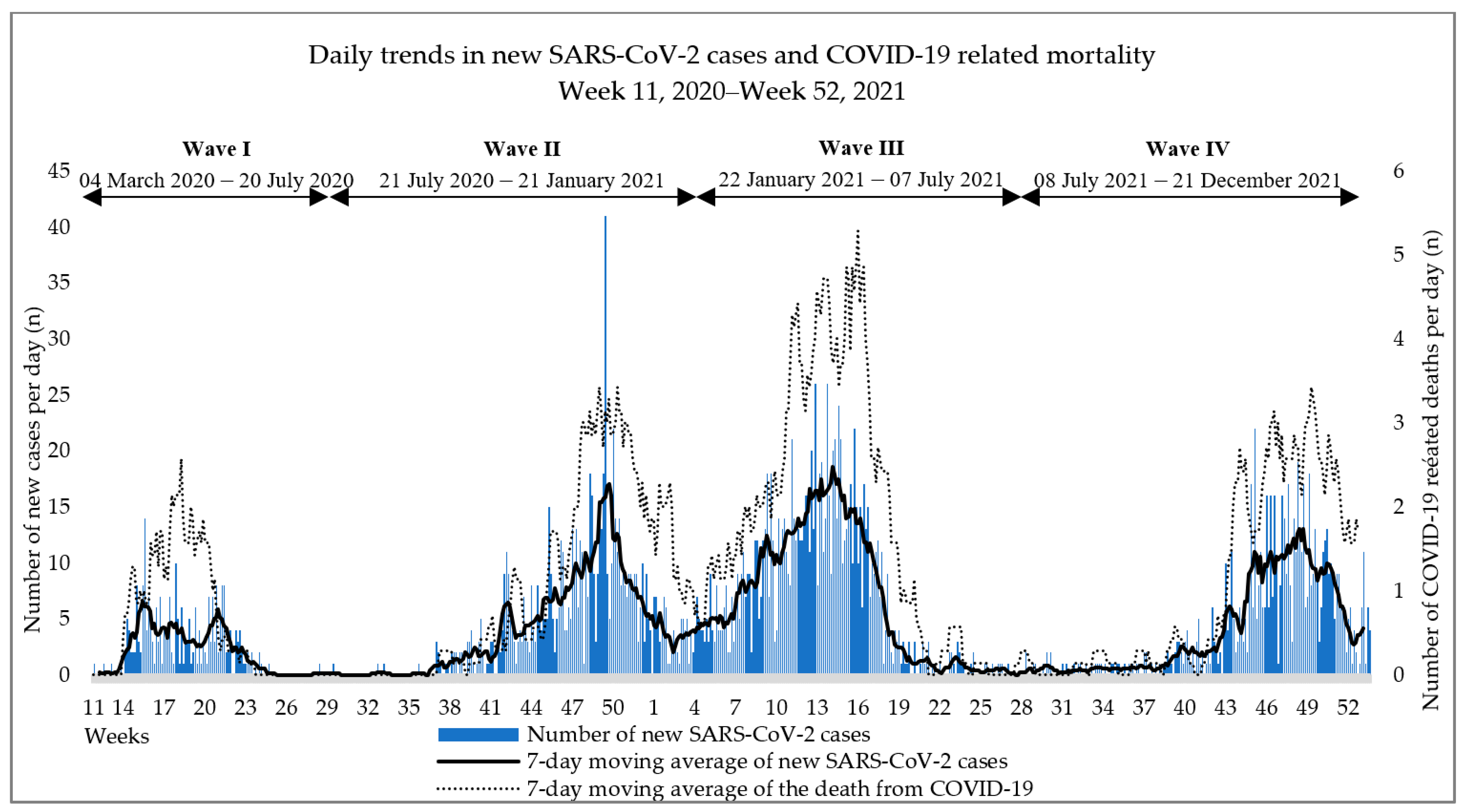
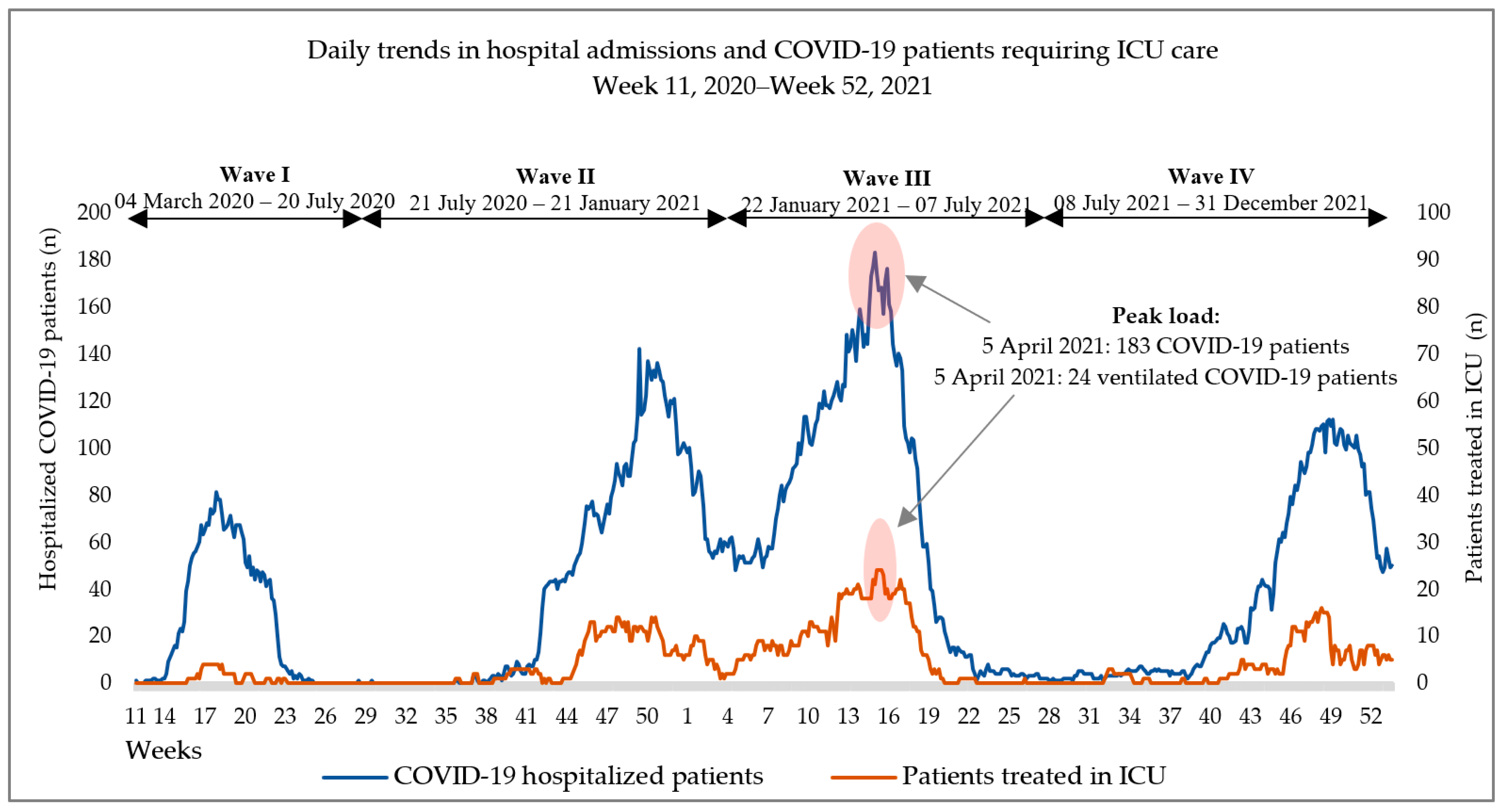
3.2. Epidemic Dynamics
3.3. Severity of Course and Disease Outcome
3.4. Proportions of Vaccinated Patients in the Total Study Population and the Impact of Vaccination on Mortality and ICU Admission
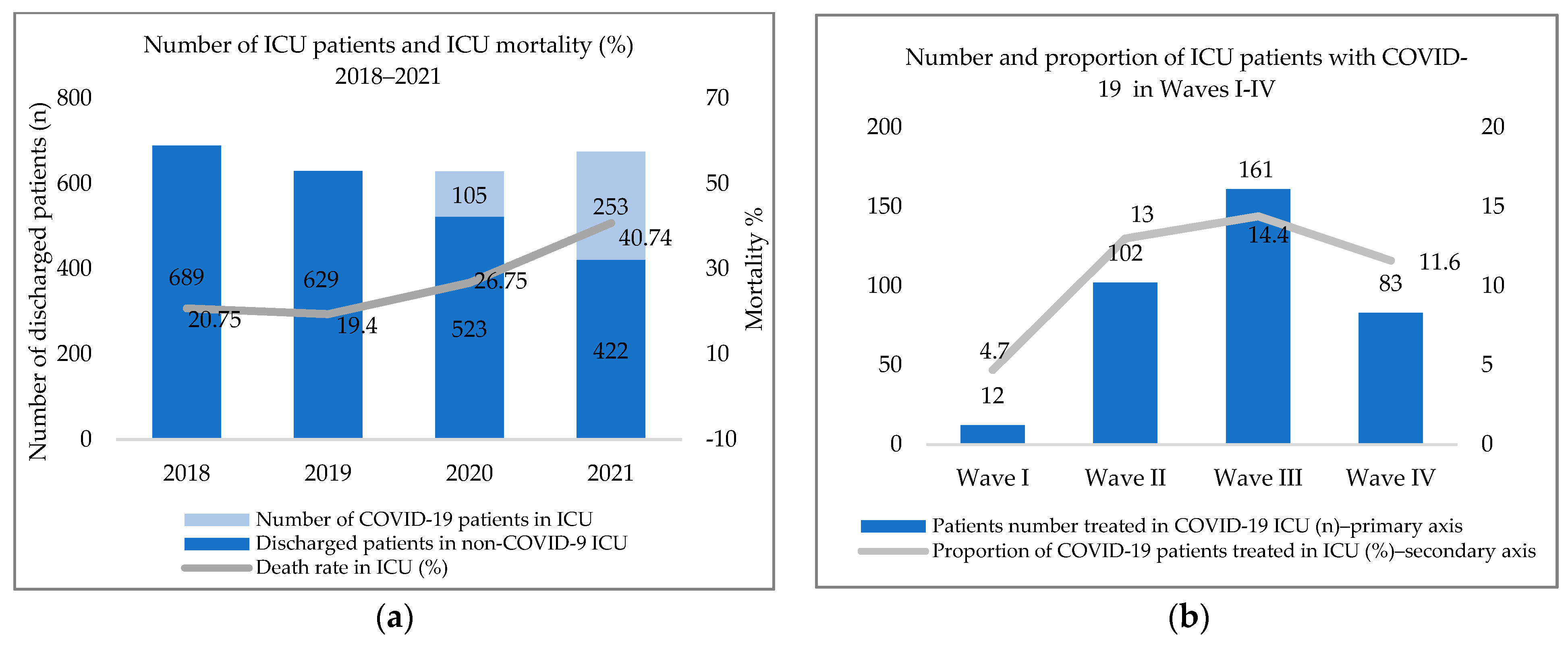
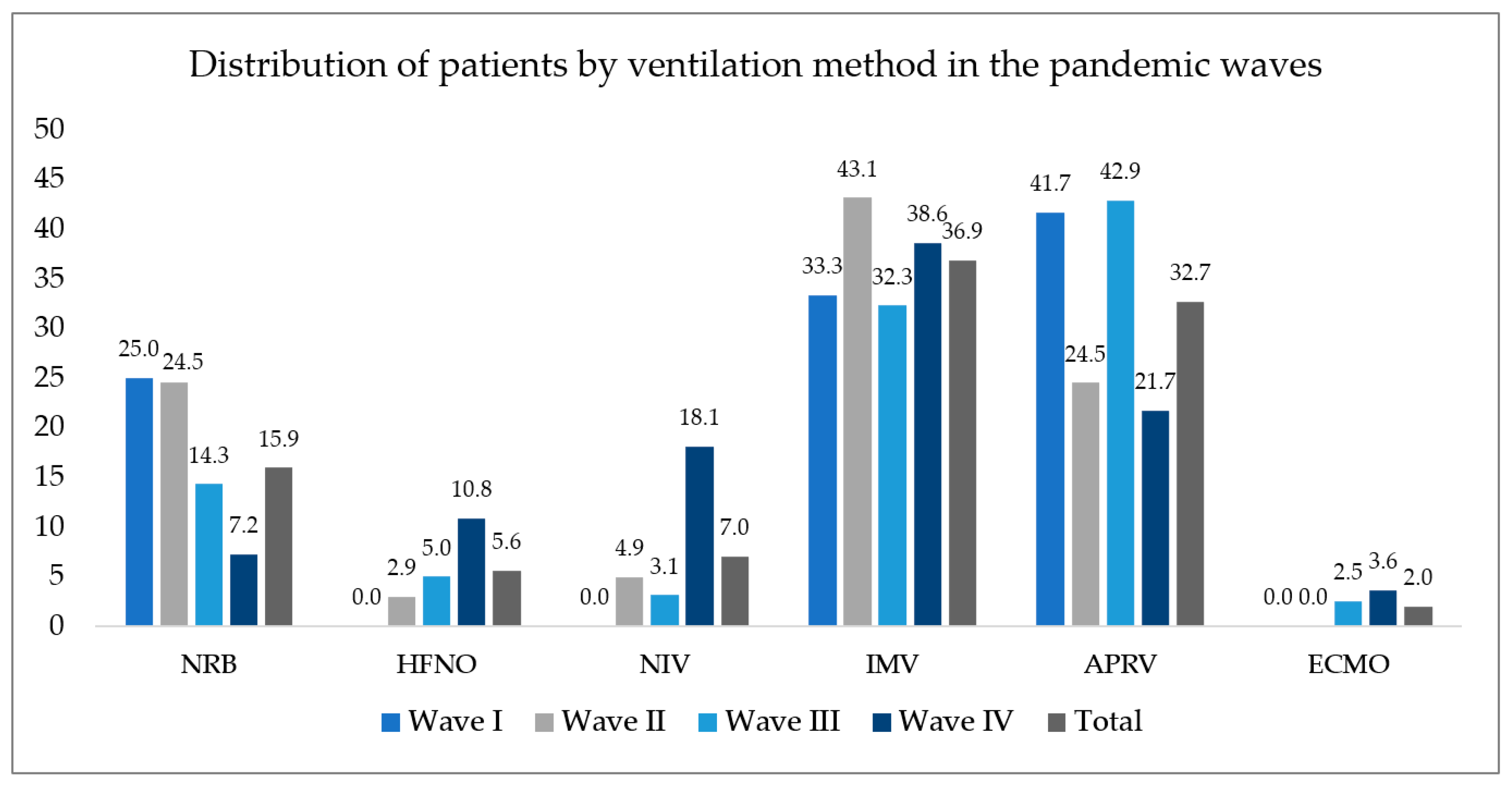
3.5. Distribution of and Mortality among Critically Ill Patients
3.5.1. Need for ICU Admission
3.5.2. Mortality in Critically Ill Patients
3.5.3. Bloodstream Infections
3.5.4. Effect of Invasive Ventilation on the Development of Bloodstream Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wave I | Wave II | Wave III | Wave IV | p Value | |
|---|---|---|---|---|---|
| General weakness or fatigue | 100 (39.1%) | 330 (42%) | 480 (43%) | 336 (46.9%) | 0.1 |
| Fever (>38) | 121 (47.3%) | 336 (42.8%) | 508 (45.5%) | 280 (39.1%) | 0.028 |
| High temperature (<38) | 29 (11.3%) | 116 (14.8%) | 98 (8.8%) | 68 (9.5%) | <0.01 |
| Cough | 111 (43.4%) | 312 (39.7%) | 484 (43.4%) | 321 (44.8%) | 0.223 |
| Shortness of breath or difficulty breathing | 105 (41%) | 332 (42.3%) | 610 (54.7%) | 335 (46.8%) | <0.01 |
| Haemoptysis | 0 | 8 (1%) | 12 (1.1%) | 5 (0.7%) | 0.356 |
| Respiratory failure | 13 (5.1%) | 93 (11.8%) | 139 (12.5%) | 77 (10.8%) | 0.008 |
| Back pain | 4 (1.6%) | 58 (7.4%) | 497 (44.5%) | 355 (49.6%) | <0.01 |
| Chills | 12 (4.7%) | 31 (3.9%) | 37 (3.3%) | 26 (3.6%) | 0.726 |
| Headache | 5 (2%) | 43 (5.5%) | 79 (7.1%) | 39 (5.4%) | 0.014 |
| Joint/muscle or body aches | 0 | 33 (4.2%) | 67 (6%) | 27 (3.8%) | <0.01 |
| Chest pain | 12 (4.7%) | 47 (6%) | 88 (7.9%) | 63 (8.8%) | 0.057 |
| Sore throat | 9 (3.5%) | 21 (2.7%) | 26 (2.3%) | 15 (2.1%) | 0.613 |
| Nasal congestion or runny nose | 2 (0.8%) | 6 (0.8%) | 3 (0.3%) | 6 (0.8%) | 0.352 |
| Loss of or change in taste or smell | 3 (1.2%) | 38 (4.8%) | 36 (3.2%) | 24 (3.4%) | 0.036 |
| Vomiting | 7 (2.7%) | 42 (5.4%) | 70 (6.3%) | 48 (6.7%) | 0.102 |
| Nausea | 11 (4.3%) | 46 (5.9%) | 52 (4.7%) | 41 (5.7%) | 0.538 |
| Diarrhea | 14 (5.5%) | 101 (12.9%) | 185 (16.6%) | 87 (12.2%) | <0.01 |
| Loss of appetite | 12 (4.7%) | 105 (13.4%) | 156 (14%) | 126 (17.6%) | <0.01 |
| Abdominal pain | 8 (3.1%) | 24 (3.1%) | 20 (1.8%) | 25 (3.5%) | 0.122 |
| Loss of consciousness | 24 (9.4%) | 48 (6.1%) | 37 (3.3%) | 17 (2.4%) | <0.01 |
| Dizziness | 1 (0.4%) | 58 (7.4%) | 54 (4.8%) | 33 (4.6%) | <0.01 |
| Impaired consciousness | 21 (8.2%) | 39 (5%) | 46 (4.1%) | 32 (4.5%) | 0.05 |
| Seizure | 1 (0.4%) | 5 (0.6%) | 6 (0.5%) | 9 (1.3%) | 0.283 |
References
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 18 September 2022).
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gralinski, L.E.; Menachery, V.D. Return of the Coronavirus: 2019-nCoV. Viruses 2020, 12, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Cholankeril, G.; Podboy, A.; Aivaliotis, V.I.; Tarlow, B.; Pham, E.A.; Spencer, S.P.; Kim, D.; Hsing, A.; Ahmed, A. High Prevalence of Concurrent Gastrointestinal Manifestations in Patients with Severe Acute Respiratory Syndrome Coronavirus 2: Early Experience from California. Gastroenterology 2020, 159, 775–777. [Google Scholar] [CrossRef]
- Xiao, F.; Tang, M.; Zheng, X.; Liu, Y.; Li, X.; Shan, H. Evidence for Gastrointestinal Infection of SARS-CoV-2. Gastroenterology 2020, 158, 1831–1833.e1833. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Liu, Y.; Mao, B.; Liang, S.; Yang, J.W.; Lu, H.W.; Chai, Y.H.; Wang, L.; Zhang, L.; Li, Q.H.; Zhao, L.; et al. Association between age and clinical characteristics and outcomes of COVID-19. Eur. Respir. J. 2020, 55, 2001112. [Google Scholar] [CrossRef] [Green Version]
- Tian, J.; Yuan, X.; Xiao, J.; Zhong, Q.; Yang, C.; Liu, B.; Cai, Y.; Lu, Z.; Wang, J.; Wang, Y.; et al. Clinical characteristics and risk factors associated with COVID-19 disease severity in patients with cancer in Wuhan, China: A multicentre, retrospective, cohort study. Lancet Oncol. 2020, 21, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered from Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265–1273. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Centre for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.H.; Li, T.Y.; He, Z.C.; Ping, Y.F.; Liu, H.W.; Yu, S.C.; Mou, H.M.; Wang, L.H.; Zhang, H.R.; Fu, W.J.; et al. A pathological report of three COVID-19 cases by minimal invasive autopsies. Zhonghua Bing Li Xue Za Zhi = Chin. J. Pathol. 2020, 49, 411–417. [Google Scholar] [CrossRef]
- Armstrong, R.A.; Kane, A.D.; Kursumovic, E.; Oglesby, F.C.; Cook, T.M. Mortality in patients admitted to intensive care with COVID-19: An updated systematic review and meta-analysis of observational studies. Anaesthesia 2021, 76, 537–548. [Google Scholar] [CrossRef]
- Bennett, K.E.; Mullooly, M.; O’Loughlin, M.; Fitzgerald, M.; O’Donnell, J.; O’Connor, L.; Oza, A.; Cuddihy, J. Underlying conditions and risk of hospitalisation, ICU admission and mortality among those with COVID-19 in Ireland: A national surveillance study. Lancet Reg. Health Eur. 2021, 5, 100097. [Google Scholar] [CrossRef]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Buetti, N.; Ruckly, S.; de Montmollin, E.; Reignier, J.; Terzi, N.; Cohen, Y.; Siami, S.; Dupuis, C.; Timsit, J.F. COVID-19 increased the risk of ICU-acquired bloodstream infections: A case-cohort study from the multicentric OUTCOMEREA network. Intensive Care Med. 2021, 47, 180–187. [Google Scholar] [CrossRef]
- Bonazzetti, C.; Morena, V.; Giacomelli, A.; Oreni, L.; Casalini, G.; Galimberti, L.R.; Bolis, M.; Rimoldi, M.; Ballone, E.; Colombo, R.; et al. Unexpectedly High Frequency of Enterococcal Bloodstream Infections in Coronavirus Disease 2019 Patients Admitted to an Italian ICU: An Observational Study. Crit. Care Med. 2021, 49, e31–e40. [Google Scholar] [CrossRef]
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 and Novel Therapeutics Against Coronavirus (COVID-19). In StatPearls; StatPearls Publishing, Copyright © 2022; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- World Health Organization. Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed on 31 October 2022).
- Barcs, I. Succession wars in the microbial world II.—From the Neander Valley to the Omicron [Örökösödési háborúk a mikrovilágban II.—A Neander-völgytől az omikronig]. Orv. Lapja 2022, 19, 30–33. (In Hungarian) [Google Scholar]
- Nagy, É.; Cseh, V.; Barcs, I.; Ludwig, E. The Impact of Comorbidities and Obesity on the Severity and Outcome of COVID-19 in Hospitalized Patients-A Retrospective Study in a Hungarian Hospital. Int. J. Environ. Res. Public Health 2023, 20, 1372. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Human Resources Hungary. Handbook for the Prevention and Therapy of Infections (COVID-19) of the New Coronavirus (SARS-CoV-2) Identified in 2020 [2020. Évben Azonosított új Koronavírus (SARS-CoV-2) Okozta Fertőzések (COVID-19) Megelőzésének és Terápiájának Kézikönyve]. Available online: https://kollegium.aeek.hu/Dokumentumok?AspxAutoDetectCookieSupport=1 (accessed on 1 September 2021). (In Hungarian).
- European Union. Legislation 2012/506/EU: Commission Implementing Decision of 8 August 2012 Amending Decision 2002/253/EC Laying down Case Definitions for Reporting Communicable Diseases to the Community Network under Decision No 2119/98/EC of the European Parliament and of the Council (Notified under Document C(2012) 5538) (1). Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=OJ:L:2012:262:FULL&from=EN (accessed on 3 November 2022).
- European Committee on Antimicrobial Susceptibility Testing. Clinical Breakpoints and Dosing of Antibiotics. Available online: https://www.eucast.org/clinical_breakpoints/ (accessed on 13 November 2022).
- National Public Health Centre. Microbiological Announcement—Screening of Multidrug-Resistant Pathogens-Methodological Recommendation for Microbiology Laboratories. Available online: https://www.nnk.gov.hu/attachments/article/1476/2021.%204.%20sz%C3%A1m%20Mikrobiol%C3%B3giai%20K%C3%B6rlev%C3%A9l.pdf (accessed on 28 October 2022).
- European Committee on Antimicrobial Susceptibility Testing. EUCAST Guideline for the Detection of Resistance Mechanisms and Specific Resistances of Clinical and/or Epidemiological Importance. Available online: https://www.eucast.org/resistance_mechanisms (accessed on 28 October 2022).
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Palásti, P.; Visnyovszki, Á.; Csizmadia, S.; Matúz, M.; Szabó, Z.; Hajdú, E.; Vattay, D.; Palkó, A.; Kincses, T.Z.; Fejes, Z. The first wave of the COVID-19 epidemic in Southern Hungary: Epidemiology, symptoms and signs. Imaging 2021, 13, 142–151. [Google Scholar] [CrossRef]
- Bozóky, G.; Ruby, É.; Mohos, A.; Bozóky, I.; Göcző, K. Thromboembolic complications in COVID-19 patients [Thromboemboliás szövődmények COVID–19-betegekben]. Orv. Hetil. 2021, 162, 1710–1716. (In Hungarian) [Google Scholar] [CrossRef] [PubMed]
- Horváth, J.K.; Komlós, K.; Krisztalovics, K.; Röst, G.; Oroszi, B. The first two years of the COVID-19 epidemic in Hungary [A COVID-19 világjárvány első két éve Magyarországon]. Népegészségügy 2022, 1, 19. (In Hungarian) [Google Scholar]
- Oroszi, B.; Horváth, J.; Túri, G.; Krisztalovics, K.; Röst, G. The role of epidemiological surveillance and mathematical forecasting in preventing and mitigating epidemic waves—What has been accomplished and what should be achieved [Az epidemiológiai surveillance és járványmatematikai előrejelzések szerepe a pandémiás hullámok megelőzésében, mérséklésében—Hol tartunk most, és hová kellene eljutni]. Sci. Et Secur. 2021, 2, 38–53. (In Hungarian) [Google Scholar] [CrossRef]
- Turk, C.; Turk, S.; Malkan, U.Y.; Haznedaroglu, I.C. Three critical clinicobiological phases of the human SARS-associated coronavirus infections. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 8606–8620. [Google Scholar] [CrossRef]
- Giacobbe, D.R.; Battaglini, D.; Ball, L.; Brunetti, I.; Bruzzone, B.; Codda, G.; Crea, F.; De Maria, A.; Dentone, C.; Di Biagio, A.; et al. Bloodstream infections in critically ill patients with COVID-19. Eur. J. Clin. Investig. 2020, 50, e13319. [Google Scholar] [CrossRef]
- Cataldo, M.A.; Tetaj, N.; Selleri, M.; Marchioni, L.; Capone, A.; Caraffa, E.; Caro, A.D.; Petrosillo, N. Incidence of bacterial and fungal bloodstream infections in COVID-19 patients in intensive care: An alarming “collateral effect”. J. Glob. Antimicrob. Resist. 2020, 23, 290–291. [Google Scholar] [CrossRef]
- National Health Insurance Fund of Hungary [Nemzeti Egészségbiztosítási Alapkezelő]. Statement of Hospital and Patients Management [Kórházi Ágyszám—És Betegforgalmi Kimutatás]. Available online: http://www.neak.gov.hu/felso_menu/szakmai_oldalak/publikus_forgalmi_adatok/gyogyito_megelozo_forgalmi_adat/fekvobeteg_szakellatas_stat/korhazi_agyszam.html (accessed on 8 December 2022). (In Hungarian)
- Aziz, M.; Haghbin, H.; Abu Sitta, E.; Nawras, Y.; Fatima, R.; Sharma, S.; Lee-Smith, W.; Duggan, J.; Kammeyer, J.A.; Hanrahan, J.; et al. Efficacy of tocilizumab in COVID-19: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 1620–1630. [Google Scholar] [CrossRef] [PubMed]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Bernard-Raichon, L.; Venzon, M.; Klein, J.; Axelrad, J.E.; Zhang, C.; Sullivan, A.P.; Hussey, G.A.; Casanovas-Massana, A.; Noval, M.G.; Valero-Jimenez, A.M.; et al. Gut microbiome dysbiosis in antibiotic-treated COVID-19 patients is associated with microbial translocation and bacteremia. Nat. Commun. 2022, 13, 5926. [Google Scholar] [CrossRef] [PubMed]




| Wave I a | Wave II b | Wave III c | Wave IV d | Total | |
|---|---|---|---|---|---|
| Number of SARS-CoV-2 cases (n/%) | 256 (8.9%) | 785 (27.3%) | 1116 (38.8%) | 716 (24.9%) | 2873 |
| Median age ± SD (IQR, min–max) | 75.5 ± 12.67 (66–84) | 71 ± 15.14 (61.5–80) | 67 ± 15.64 (54–76) | 69 ± 15.94 (57–79) | 69 ± 15.57 (58–79) |
| Male (n/%) | 115 (44.9%) | 391 (49.8%) | 564 (50.5%) | 355 (49.6%) | 1425 (49.6%) |
| Mean number of days of care at the COVID-19 ward ± SD (IQR, min–max) | 15.27 ± 11.89 (5–24) | 12.1 ± 11.61 (3–17) | 11.15 ± 6.97 (7–14) | 10.08 ± 6.91 (6–13) | 11.51 ± 9.06 (6–15) |
| Number of ICU patients (n/%) | 12 (4.7%) | 102 (13%) | 161 (14.4%) | 83 (11.6%) | 358 (12.5%) |
| Mean number of days of ICU care ± SD (IQR, min–max) | 6.58 ± 5.50 (2.25–10.25) | 11.57 ± 11.50 (3–15.25) | 9.96 ± 7.42 (4–13) | 10.27 ± 8.87 (4–14) | 10.38 ± 9.06 (4–13.25) |
| Severity | Wave I | Wave II | Wave III | Wave IV | p Value |
|---|---|---|---|---|---|
| Asymptomatic | 37 (14.5%) | 138 (17.6%) | 116 (10.4%) | 49 (6.8%) | <0.001 |
| Mild | 24 (9.4%) | 78 (9.9%) | 59 (5.3%) | 89 (12.4%) | <0.001 |
| Moderate | 170 (66.4%) | 354 (45.1%) | 274 (24.6%) | 266 (37.2%) | <0.001 |
| Severe | 13 (5.1%) | 128 (16.3%) | 521 (46.7%) | 234 (32.7%) | <0.001 |
| Critical | 12 (4.7%) | 87 (11.1%) | 146 (13.1%) | 78 (10.9%) | 0.002 |
| Radiologically confirmed pneumonia | 146 (57%) | 476 (60,6%) | 850 (76.2%) | 468 (65.4%) | <0.001 |
| Outcome | |||||
| Recovered | 70 (27.3%) | 336 (42.8%) | 656 (58.8%) | 412 (57.5%) | <0.001 |
| Died | 75 (29.3%) | 196 (25%) | 295 (26.4%) | 197 (27.5%) | 0.504 |
| Hospital discharged—not recovered | 111 (43.4%) | 253 (32.2%) | 165 (14.8%) | 107 (14.9%) | <0.001 |
| Vaccinated (n/%) | aOR [95% CI] | ||
|---|---|---|---|
| Mortality | ICU Admission | ||
| Wave III. | 42 (3.8%) | 0.39 * [0.18–0.84] | 0.11 * [0.02–0.84] |
| Wave IV. | 357 (49.9%) | 0.94 [0.56–1.56] | 0.69 * [0.48–0.98] |
| Wave I | Wave II | Wave III | Wave IV | Total | |
|---|---|---|---|---|---|
| Number of COVID-19 cases | 12 | 102 | 161 | 83 | 358 |
| Median age ± SD (IQR, min–max) | 68 ± 9.57 (58.75–73.75) | 68 ± 10.99 (62–75) | 67 ± 12.57 (58–72) | 62 ± 14.15 (51–71) | 66 ± 12.65 (58–73) |
| Male (n/%) | 8 (66.7%) | 71 (69.6%) | 95 (59%) | 46 (55.4%) | 220 (61.5%) |
| Mortality (n/%) | 5 (41.7%) | 52 (51%) | 117 (72.7%) | 53 (63.9%) | 227 (63.4%) |
| Vaccination (n/%) | 0 | 0 | 1 (0.6%) | 35 (42.2%) | 36 (10.1%) |
| Presence of Comorbidity (n/%) | 12 (100%) | 95 (93.1%) | 148 (91.9%) | 68 (81.9%) | 323 (90.2%) |
| Obesity (n/%) | 6 (50%) | 41 (40.2) | 79 (49.1%) | 41 (49.4%) | 167 (46.6%) |
| Hypertonia (n/%) | 8 (66.7%) | 75 (73.5%) | 112 (69.6%) | 49 (59%) | 244 (68.2%) |
| Diabetes mellitus (n/%) | 6 (50%) | 40 (39.2%) | 49 (30.4%) | 28 (33.7%) | 123 (34.4%) |
| Cardiovascular disease (n/%) | 8 (66.7%) | 46 (45.1%) | 59 (26.6%) | 25 (30.1%) | 138 (38.5%) |
| Cancer (n/%) | 2 (16.7%) | 10 (9.8%) | 25 (15.5%) | 7 (8.4%) | 44 (12.3%) |
| Chronic kidney disease (n/%) | 3 (25%) | 13 (12.7%) | 11 (6.8%) | 4 (4.8%) | 31 (8.7%) |
| BSI (n/%) | 1 (8.3%) | 34 (33.3%) | 73 (45.3) | 28 (33.7) | 136 (38.0%) |
| VAP (n/%) * | 0 | 20 (29) | 33 (26.4) | 20 (37.7) | 73 (28.5) |
| HAP (n/%) | 0 | 1 (1.0) | 2 (1.2) | 2 (2.4) | 5 (1.4) |
| UTI (n/%) | 0 | 4 (3.9) | 1 (0.6) | 2 (2.4) | 6 (1.7) |
| Other infections # (n/%) | 0 | 5 (4.9) | 8 (5.0) | 1 (1.2) | 14 (3.9) |
| aOR [95% CI] | |||||
|---|---|---|---|---|---|
| Wave I | Wave II | Wave III | Wave IV | Total | |
| Age | 1.04 [0.90–1.19] | 1.01 [0.96–1.05] | 1.04 * [1.00–1.08] | 1.07 * [1.02–1.13] | 1.03 * [1.01–1.05] |
| Male sex | 0.53 [0.015–9.92] | 2.54 [0.98–6.58] | 0.93 [0.41–2.05] | 1.75 [0.55–5.59] | 1.28 [0.79–2.06] |
| Vaccination | N.A. | N.A. | N.A. | 0.57 [0.20–1.66] | 0.81 [0.39–1.67] |
| Comorbidity present | N.A. | 3.73 [0.61–22.71] | 1.88 [0.44–8.15] | 1.48 [0.38–5.72] | 1.59 [0.74–3.44] |
| Obesity | 2.35 [0.16–34.19] | 1.26 [0.52–3.04] | 1.49 [0.64–3.49] | 1.63 [0.55–4.86] | 1.54 [0.95–2.50] |
| Hypertonia | N.A. | 0.49 [0.18–1.36] | 1.09 [0.45–2.60] | 0.55 [0.17–1.77] | 0.75 [0.44–1.26] |
| Diabetes mellitus | N.A. | 1.02 [0.42–2.43] | 1.05 [0.45–2.45] | 1.34 [0.42–4.36] | 1.02 [0.62–1.67] |
| Cardiovascular disease | N.A. | 1.58 [0.64–3.91] | 0.98 [0.41–2.38] | 1.14 [0.29–4.49] | 1.20 [0.72–2.00] |
| Cancer | N.A. | 2.54 [0.57–11.40] | 1.41 [0.48–4.18] | 1.34 [0.18–10.20] | 1.73 [0.83–3.60] |
| Chronic kidney disease | N.A. | 2.75 [0.71–10.70] | 0.79 [0.19–3-49] | 0.08 [0.00–1.56] | 0.85 [0.38–1.91] |
| BSI | N.A. | 1.90 [0.79–4.53] | 9.72 ** [3.68–25.67] | 1.06 [0.37–3.05] | 3.32 ** [2.01–5.48] |
| VAP | N.A. | 1.98 [0.55–7.11] | 7.38 [0.89–64.41] | 0.75 [0.12–4.77] | 1.86 [0.87–3.98] |
| Other infections # | N.A. | 0.61 [0.16–2.36] | 1.22 [0.31–4.91] | 1.65 [0.26–10.64] | 0.89 [0.41–1.94] |
| Identified Microorganisms in Bloodstream Infections (N = 223) | Number of Microorganisms (N/%) | MDR (N/%) |
|---|---|---|
| Staphylococcus aureus | 26 (11.7%) | 12 (46.2%) |
| Coagulase-negative staphylococci (CoNS) * | 7 (3.1%) | - |
| Streptococcus pneumoniae | 2 (0.9%) | - |
| Other Streptococcus sp. | 5 (2.2%) | - |
| Enterococcus faecalis | 27 (12.1%) | - |
| Enterococcus faecium | 16 (7.2) | 6 (37.5%) |
| Escherichia coli | 6 (2.7%) | 2 (33.3%) |
| Klebsiella pneumoniae | 22 (9.9%) | 13 (59.1%) |
| Klebsiella aerogenes | 7 (3.1%) | 3 (42.9%) |
| Enterobacter cloacae | 13 (5.8%) | 5 (38.5%) |
| Other Enterobacter sp. | 9 (4.0%) | 3 (33.3%) |
| Citrobacter sp. | 2 (0.9%) | - |
| Proteus sp. | 4 (1.8%) | - |
| Acinetobacter baumannii | 11 (4.9%) | 4 (36.4%) |
| Other Acinetobacter sp. | 5 (2.2%) | 1 (20%) |
| Pseudomonas aeruginosa | 18 (8.1%) | - |
| Serratia marcescens | 6 (2.7%) | - |
| Stenotrophomonas maltophilia | 20 (9.0%) | - |
| Other Gram-positive | 4 (1.8%) | - |
| Other Gram-negative | 3 (1.3%) | - |
| Candida albicans | 5 (2.2%) | - |
| Other Candida sp. | 5 (2.2%) | - |
| Bacteria identified as contaminants (n = 171) | ||
| Coagulase-negative staphylococci (CoNS) | 157 (91.8%) | - |
| Corynebacterium sp. | 6 (3.5%) | - |
| Micrococcus sp. | 3 (1.8%) | - |
| Peptococcus sp. | 1 (0.6%) | - |
| Cutibacterium sp. (Propionibacterium sp.) | 3 (1.8%) | - |
| Gram-positive rods | 1 (0.6%) | - |
| Invasive Mechanical Ventilation (IMV) | p Value † | ||
|---|---|---|---|
| BSI Group * | Non-BSI Group ** | ||
| Wave I | 1/1 (100%) | 8/11 (72.7%) | 1.0 |
| Wave II | 29/34 (85.3%) | 40/68 (58.8%) | 0.007 |
| Wave III | 72/73 (98.6%) | 53/88 (60.2%) | <0.001 |
| Wave IV | 24/28 (85.7%) | 29/55 (52.7%) | 0.003 |
| Total | 126/136 (92.6%) | 130/222 (58.6%) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagy, É.; Golopencza, P.; Barcs, I.; Ludwig, E. Comparison of COVID-19 Severity and Mortality Rates in the First Four Epidemic Waves in Hungary in a Single-Center Study with Special Regard to Critically Ill Patients in an Intensive Care Unit. Trop. Med. Infect. Dis. 2023, 8, 153. https://doi.org/10.3390/tropicalmed8030153
Nagy É, Golopencza P, Barcs I, Ludwig E. Comparison of COVID-19 Severity and Mortality Rates in the First Four Epidemic Waves in Hungary in a Single-Center Study with Special Regard to Critically Ill Patients in an Intensive Care Unit. Tropical Medicine and Infectious Disease. 2023; 8(3):153. https://doi.org/10.3390/tropicalmed8030153
Chicago/Turabian StyleNagy, Éva, Péter Golopencza, István Barcs, and Endre Ludwig. 2023. "Comparison of COVID-19 Severity and Mortality Rates in the First Four Epidemic Waves in Hungary in a Single-Center Study with Special Regard to Critically Ill Patients in an Intensive Care Unit" Tropical Medicine and Infectious Disease 8, no. 3: 153. https://doi.org/10.3390/tropicalmed8030153
APA StyleNagy, É., Golopencza, P., Barcs, I., & Ludwig, E. (2023). Comparison of COVID-19 Severity and Mortality Rates in the First Four Epidemic Waves in Hungary in a Single-Center Study with Special Regard to Critically Ill Patients in an Intensive Care Unit. Tropical Medicine and Infectious Disease, 8(3), 153. https://doi.org/10.3390/tropicalmed8030153