

Spatiotemporal Distribution of Tuberculosis in the Oromia Region of Ethiopia: A Hotspot Analysis

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
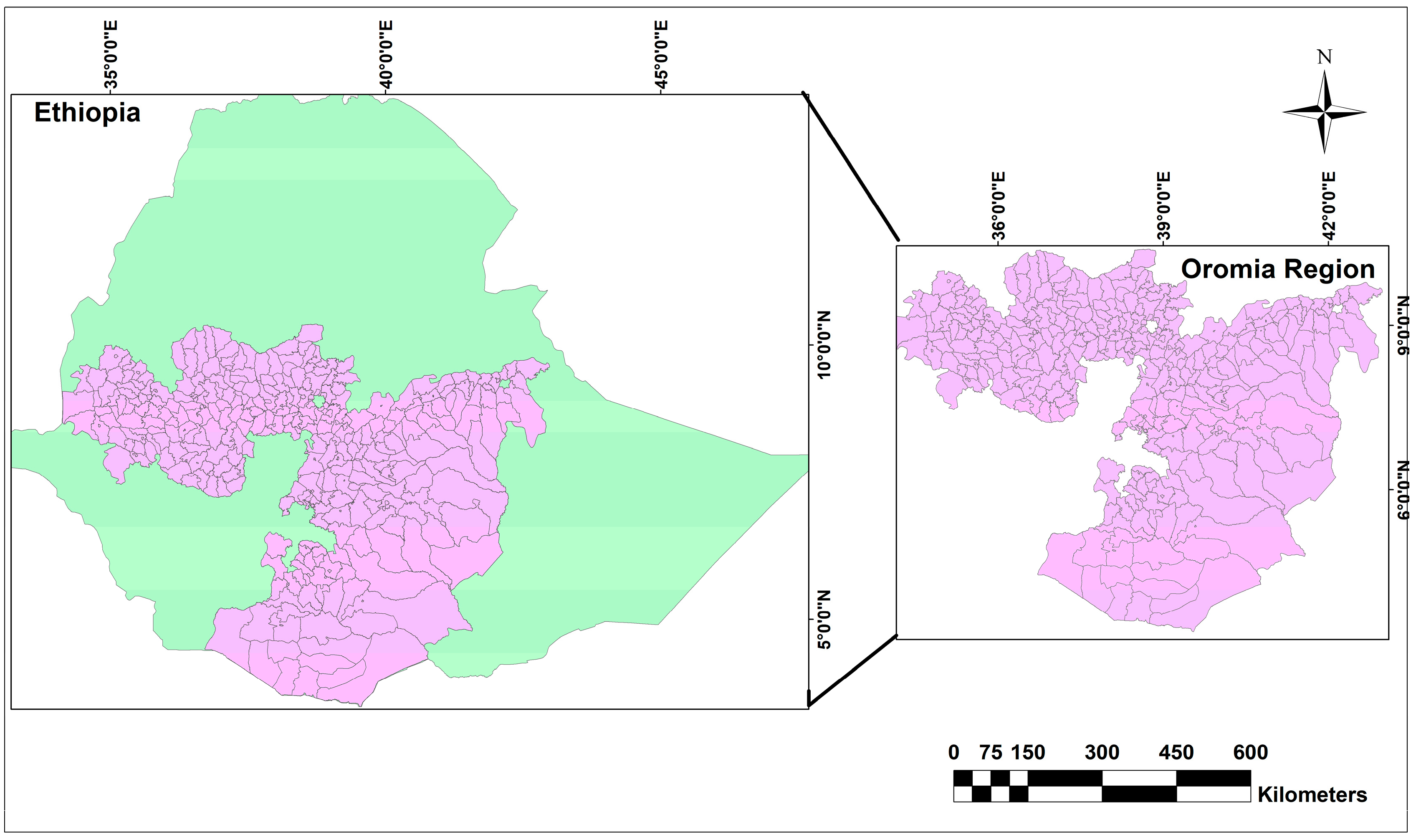
2.1. Study Setting
2.2. Data Sources
2.3. Measurement
2.4. Data Analysis
3. Results
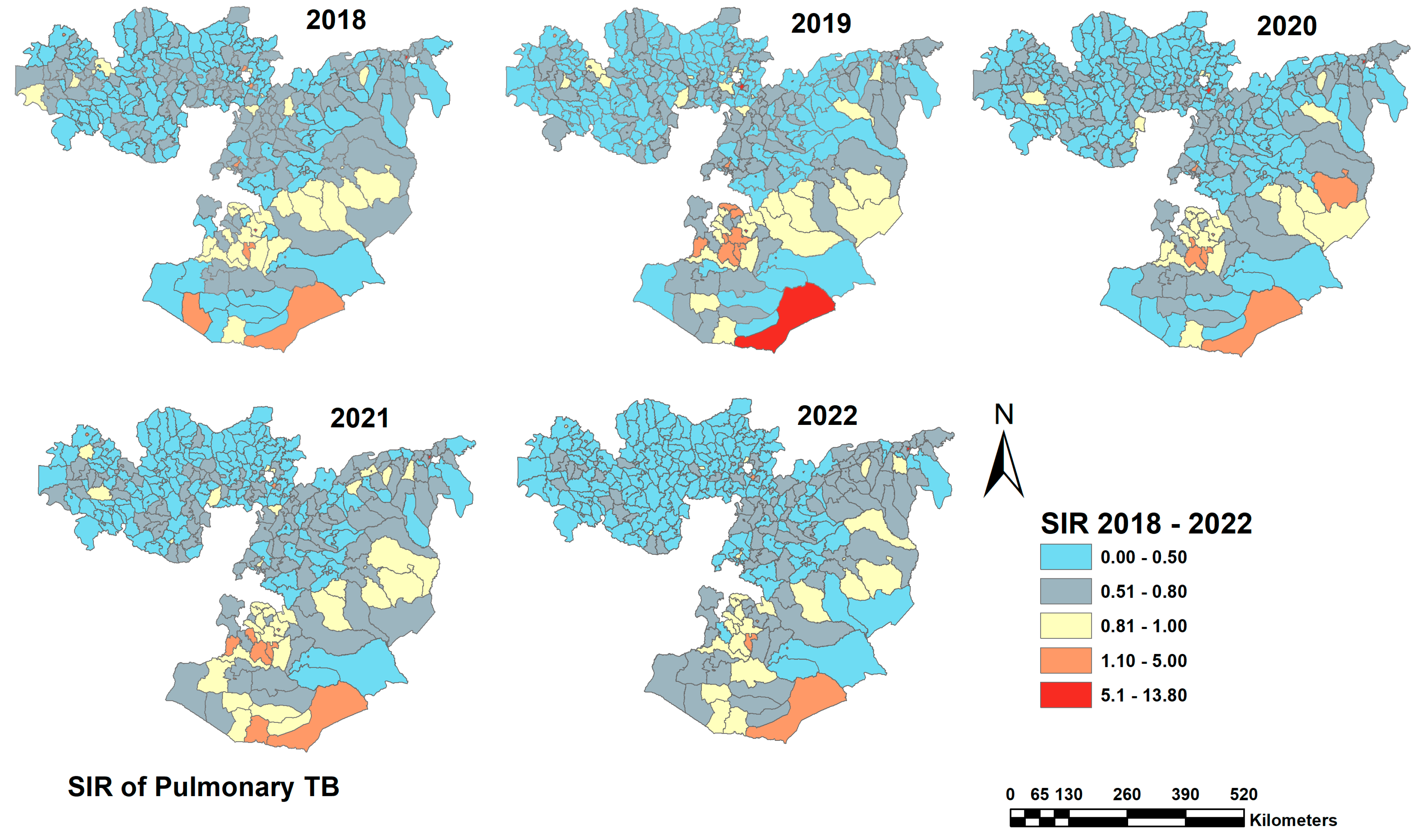
3.1. Case Notification
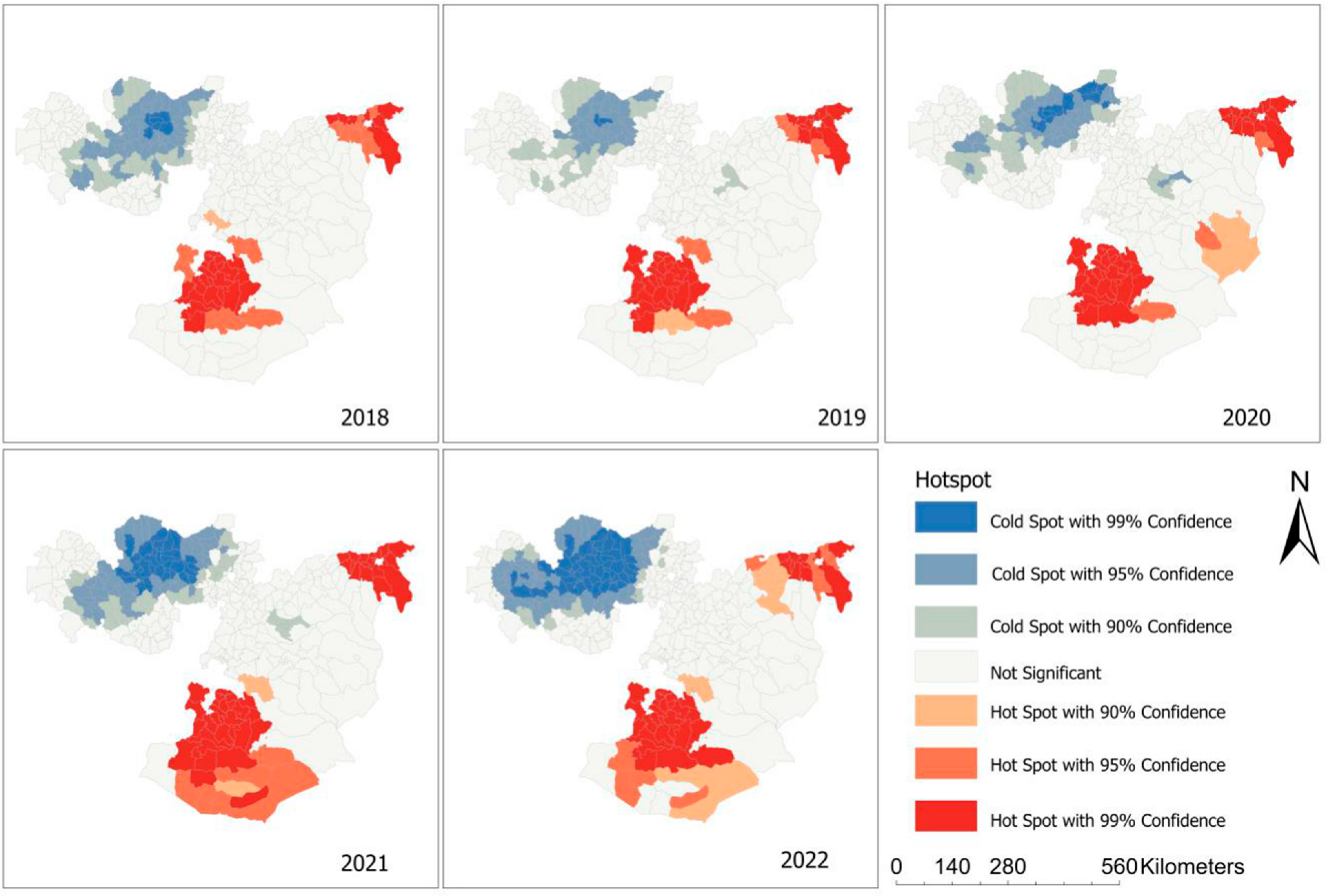
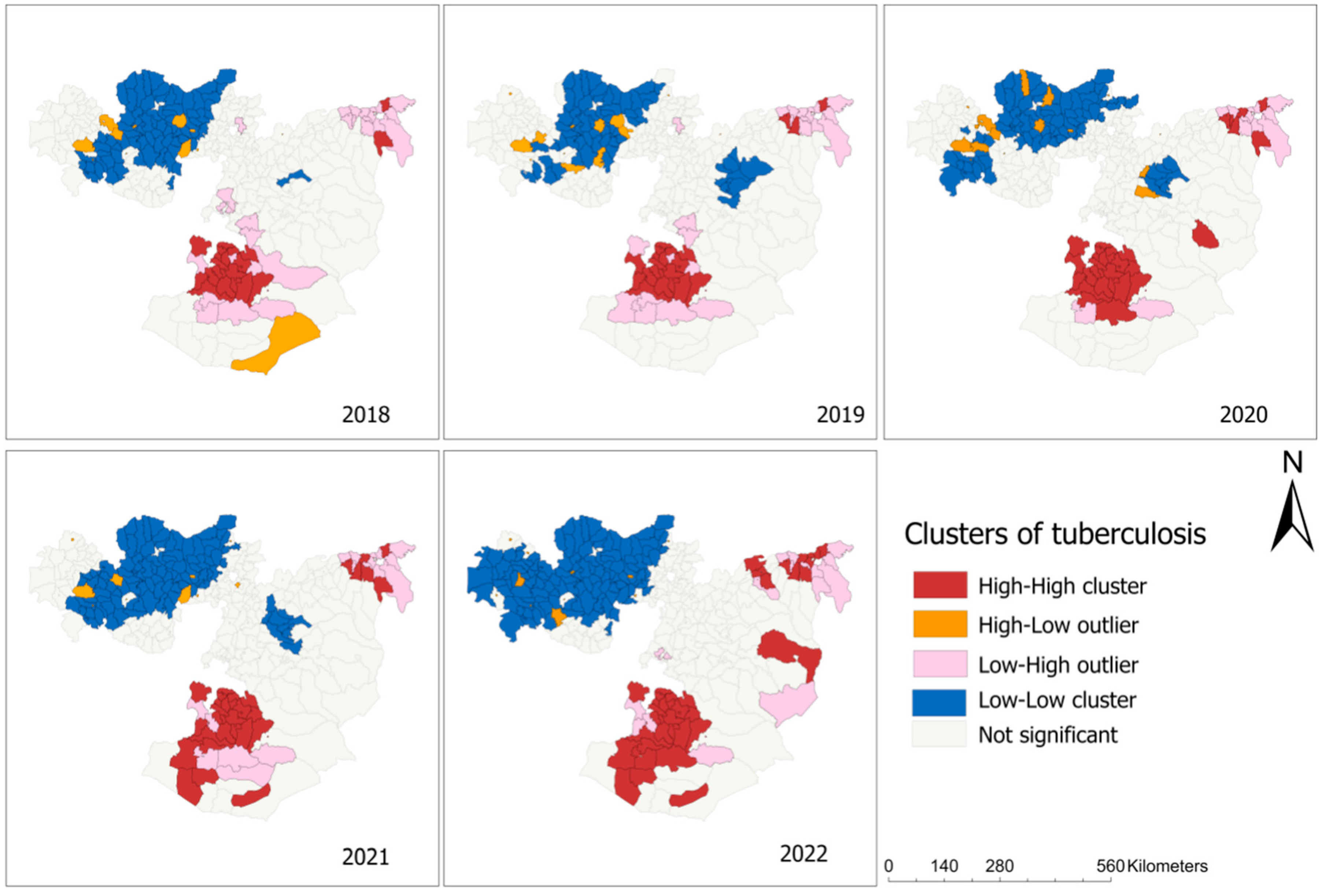
3.2. Spatial Clustering of TB
3.3. The Result from the Non-Spatial Univariate Bayesian Regression Model
3.4. The Result of the Spatiotemporal Bayesian Regression Model
4. Discussion
District-Level Primary Health Care Service Strongly Affected TB Case Notification
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviation
| CrI | credible interval |
| DIC | Devian Information Criteria |
| DHIS | District Health Information System |
| DOTS | Directly Observed Treatment Short Course |
| GIS | geographical information system |
| HIV | human immunodeficiency virus |
| HMIS | Health Management Information System |
| RR | relative risk |
| SIR | standardized incidence ratio |
| SD | standard deviation |
| TB | tuberculosis |
| VIF | variance inflation factors |
| WHO | World Health Organization |
References
- World Health Organization (WHO). Global Tuberculosis Report; WHO: Geneva, Switzerland, 2022; ISBN 9789240061729.
- World Health Organization (WHO). Global Tuberculosis Report; WHO: Geneva, Switzerland, 2021; ISBN 9780415475976.
- Titosse, A.C.; Pimenta Rodrigues, M.V.; Marques Ramos, A.P.; Prado Osco, L.; Giuffrida, R.; Da Silva Fonseca, E.; Azevedo Arana, A.R. Tuberculosis Space-Temporal Distribution from 2011 to 2016 in the Municipality of Maputo, Mozambique. Población Salud Mesoamérica 2020, 18, 270–300. [Google Scholar] [CrossRef]
- Woldeyohannes, S.M. Worldwide Spatial and Temporal Distribution of Tuberculosis (TB). J. AIDS Clin. Res. 2015, 6, 452. [Google Scholar] [CrossRef]
- Asemahagn, M.A.; Alene, G.D.; Yimer, S.A. Spatial-Temporal Clustering of Notified Pulmonary Tuberculosis and Its Predictors in East Gojjam Zone, Northwest Ethiopia. PLoS ONE 2021, 16, e0245378. [Google Scholar] [CrossRef]
- Wang, L.; Xu, C.; Hu, M.; Qiao, J.; Chen, W.; Li, T.; Qian, S.; Yan, M. Spatio-Temporal Variation in Tuberculosis Incidence and Risk Factors for the Disease in a Region of Unbalanced Socio-Economic Development. BMC Public Health 2021, 21, 1817. [Google Scholar] [CrossRef]
- Tadesse, S.; Enqueselassie, F.; Hagos, S. Spatial and Space-Time Clustering of Tuberculosis in Gurage Zone, Southern Ethiopia. PLoS ONE 2018, 13, e0198353. [Google Scholar] [CrossRef]
- Dangisso, M.H.; Datiko, D.G.; Lindtjørn, B. Spatio-Temporal Analysis of Smear-Positive Tuberculosis in the Sidama Zone, Southern Ethiopia. PLoS ONE 2015, 10, e0126369. [Google Scholar] [CrossRef]
- Shaweno, D.; Shaweno, T.; Trauer, J.M.; Denholm, J.T.; McBryde, E.S. Heterogeneity of Distribution of Tuberculosis in Sheka Zone, Ethiopia: Drivers and Temporal Trends. Int. J. Tuberc. Lung Dis. 2017, 21, 79–85. [Google Scholar] [CrossRef]
- Alene, K.A.; Clements, A.C.A. Spatial Clustering of Notified Tuberculosis in Ethiopia: A Nationwide Study. PLoS ONE 2019, 14, e0221027. [Google Scholar] [CrossRef]
- Oromia Region, Investment Commission (OIC). 2021. Available online: http://oromiainvest.com/oromia_at_a_glance/# (accessed on 20 May 2021).
- Ministry of Health (MoH). Health Management Information System (HMIS)/Monitoring and Evaluation (M&E); Ministry of Health (MoH): Addis Ababa, Ethiopia, 2008; pp. 26–29.
- Bogale, A. Implementation Status of Health Management Information System in Hospitals of South West Shoa Zone, Oromia, Central Ethiopia. Clin. Outcomes Res. 2021, 13, 1–8. [Google Scholar] [CrossRef]
- Ministry of Health (MoH). Guidelines for Management of TB, DR-TB and Lerosy in Ethiopia Sixth Edition August 2018 Addis Ababa; Ministry of Health: Addis Ababa, Ethiopia, 2018; ISBN 9781626239777.
- NASA Prediction of Worldwide Energy Resources. Available online: https://power.larc.nasa.gov/ (accessed on 10 April 2023).
- Ministry of Health (MoH); Health Management Information System (HMIS). Indicators Reference Guide Technical Standards; Ministry of Health: Addis Ababa, Ethiopia, 2017; Volume 1.
- Zhang, K.; Liu, J.; Liu, Y.; Zhang, P.; Carroll, R.J. Bayesian Adjustment for Measurement Error in an Offset Variable in a Poisson Regression Model. Stat. Model. 2022, 22, 509–526. [Google Scholar] [CrossRef]
- Moraga, P. Geospatial Health Data; CRC Press: Boca Raton, FL, USA, 2019; ISBN 9780367357955. [Google Scholar]
- Togun, T.; Kampmann, B.; Stoker, N.G.; Lipman, M. Anticipating the Impact of the COVID-19 Pandemic on TB Patients and TB Control Programs. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 21. [Google Scholar] [CrossRef] [PubMed]
- Arega, B.; Negesso, A.; Taye, B.; Weldeyohhans, G.; Bewket, B.; Negussie, T.; Teshome, A.; Endazenew, G. Impact of COVID-19 Pandemic on TB Prevention and Care in Addis Ababa, Ethiopia: A Retrospective Database Study. BMJ Open 2022, 12, e053290. [Google Scholar] [CrossRef] [PubMed]
- Tadesse, T.; Demissie, M.; Berhane, Y.; Kebede, Y.; Abebe, M. Incidence of Smear-Positive Tuberculosis in Dabat, Northern Ethiopia. Int. J. Tuberc. Lung Dis. 2013, 17, 630–635. [Google Scholar] [CrossRef] [PubMed]
- Gashu, Z.; Jerene, D.; Datiko, D.G.; Hiruy, N.; Negash, S.; Melkieneh, K.; Bekele, D.; Nigussie, G.; Suarez, P.G.; Hadgu, A. Seasonal Patterns of Tuberculosis Case Notification in the Tropics of Africa: A Six-Year Trend Analysis in Ethiopia. PLoS ONE 2018, 13, e0207552. [Google Scholar] [CrossRef]
- Alene, K.A.; Viney, K.; McBryde, E.S.; Clements, A.C.A. Spatiotemporal Transmission and Socio-Climatic Factors Related to Paediatric Tuberculosis in North-Western Ethiopia. Geospat. Health 2017, 12, 342–350. [Google Scholar] [CrossRef]
- Wubuli, A.; Li, Y.; Xue, F.; Yao, X.; Upur, H.; Wushouer, Q. Seasonality of Active Tuberculosis Notification from 2005 to 2014 in Xinjiang, China. PLoS ONE 2017, 12, e0180226. [Google Scholar] [CrossRef]
- Alene, K.A.; Viney, K.; McBryde, E.S.; Clements, A.C.A. Spatial Patterns of Multi-Drug Resistant Tuberculosis and Relationships to Socioeconomic, Demographic and Household Factors in Northwest Ethiopia. PLoS ONE 2017, 12, e0171800. [Google Scholar] [CrossRef] [PubMed]
- Wubuli, A.; Xue, F.; Jiang, D.; Yao, X.; Upur, H. Socio-Demographic Predictors and Distribution of Pulmonary Tuberculosis (TB) in Xinjiang, China: A Spatial Analysis. PLoS ONE 2015, 2013, e0144010. [Google Scholar] [CrossRef]
- Clark, M.; Nowgesic, E. The Association of Housing Density, Isolation, and Tuberculosis in Canadian First Nations Communities. Int. J. Epidemiol. 2002, 31, 940–945. [Google Scholar] [CrossRef]
- Dangisso, M.H.; Datiko, D.G.; Lindtjørn, B. Accessibility to Tuberculosis Control Services and Tuberculosis Programme Performance in Southern Ethiopia. Glob. Health Action 2015, 8, 29443. [Google Scholar] [CrossRef]
- Yu, Y.; Wu, B.; Wu, C.; Wang, Q.; Hu, D.; Chen, W. Spatial-Temporal Analysis of Tuberculosis in Chongqing, China 2011–2018. BMC Infect. Dis. 2020, 20, 531. [Google Scholar] [CrossRef]
- Huang, L.; Li, X.-X.; Abe, E.M.; Xu, L.; Ruan, Y.; Cao, C.-L.; Li, S.-Z. Spatial-Temporal Analysis of Pulmonary Tuberculosis in the Northeast of the Yunnan Province, People’s Republic of China. Infect. Dis. Poverty 2017, 6, 53. [Google Scholar] [CrossRef] [PubMed]
- Jagielski, T.; Minias, A.; van Ingen, J.; Rastogi, N.; Brzostek, A.; Żaczek, A.; Dziadek, J. Methodological and Clinical Aspects of the Molecular Epidemiology of Mycobacterium Tuberculosis and Other Mycobacteria. Clin. Microbiol. Rev. 2016, 29, 239–290. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.Q.; Wu, Q.; Wang, A.M.; Bao, F.J.; Zhang, Y.Z.; Liu, J.; Yan, J.W.; Fang, X.H.; Li, L.; Zhang, Z.K.; et al. Epidemiological Characteristics of Pulmonary Tuberculosis in Anhui Province, Eastern China from 2013 to 2018. PLoS ONE 2020, 15, e0237311. [Google Scholar] [CrossRef]
- Bini, E.I.; Mata Espinosa, D.; Marquina Castillo, B.; Barrios Payán, J.; Colucci, D.; Cruz, A.F.; Zatarain, Z.L.; Alfonseca, E.; Pardo, M.R.; Bottasso, O.; et al. The Influence of Sex Steroid Hormones in the Immunopathology of Experimental Pulmonary Tuberculosis. PLoS ONE 2014, 9, e93831. [Google Scholar] [CrossRef]
- Gelaw, Y.; Yu, W.; Magalha, R.; Assefa, Y.; Williams, G. Effect of Temperature and Altitude Difference on Tuberculosis Notification: A Systematic Review. J. Glob. Infect. Dis. 2019, 11, 63–68. [Google Scholar] [CrossRef]
- Zhang, X.; Hao, Y.; Fei, Z.Y.; He, J. Effect of Meteorological Factors on Incidence of Tuberculosis: A 15-Year Retrospective Study Based on Chinese Medicine Theory of Five Circuits and Six Qi. Chin. J. Integr. Med. 2015, 21, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Li, X.X.; Wang, L.X.; Zhang, J.; Liu, Y.X.; Zhang, H.; Jiang, S.W.; Chen, J.X.; Zhou, X.N. Exploration of Ecological Factors Related to the Spatial Heterogeneity of Tuberculosis Prevalence in P. R. China. Glob. Health Action 2014, 7, 23620. [Google Scholar] [CrossRef] [PubMed]
- Kiani, B.; Raouf Rahmati, A.; Bergquist, R.; Hashtarkhani, S.; Firouraghi, N.; Bagheri, N.; Moghaddas, E.; Mohammadi, A. Spatio-Temporal Epidemiology of the Tuberculosis Incidence Rate in Iran 2008 to 2018. BMC Public Health 2021, 21, 1093. [Google Scholar] [CrossRef]
- Li, H.; Ge, M.; Zhang, M. Spatio-Temporal Distribution of Tuberculosis and the Effects of Environmental Factors in China. BMC Infect. Dis. 2022, 22, 565. [Google Scholar] [CrossRef]
- Keerqinfu; Zhang, Q.; Yan, L.; He, J. Time Series Analysis of Correlativity between Pulmonary Tuberculosis and Seasonal Meteorological Factors Based on Theory of Human-Environmental Inter Relation. J. Tradit. Chin. Med. Sci. 2018, 5, 119–127. [Google Scholar] [CrossRef]
- Guo, C.; Du, Y.; Shen, S.Q.; Lao, X.Q.; Qian, J.; Ou, C.Q. Spatiotemporal Analysis of Tuberculosis Incidence and Its Associated Factors in Mainland China. Epidemiol. Infect. 2017, 145, 2510–2519. [Google Scholar] [CrossRef] [PubMed]
- Cao, K.; Yang, K.; Wang, C.; Guo, J.; Tao, L.; Liu, Q.; Gehendra, M.; Zhang, Y.; Guo, X. Spatial-Temporal Epidemiology of Tuberculosis in Mainland China: An Analysis Based on Bayesian Theory. Int. J. Environ. Res. Public Health 2016, 13, 469. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; He, L.; Chen, Y.; Wang, Q.; Meng, Q.; Chang, W.; Xiong, L.; Yu, Z. The Influence of Meteorological Factors on Tuberculosis Incidence in Southwest China from 2006 to 2015. Sci. Rep. 2018, 8, 10053. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, M.; Wu, S.S.; Jiang, H.; Zhang, J.; Wang, S.; Ma, W.; Li, Q.; Ma, Y.; Liu, Y.; et al. Spatial Distribution of Tuberculosis and Its Association with Meteorological Factors in Mainland China. BMC Infect. Dis. 2019, 19, 379. [Google Scholar] [CrossRef]
- Li, Z.; Liu, Q.; Zhan, M.; Tao, B.; Wang, J.; Lu, W. Meteorological Factors Contribute to the Risk of Pulmonary Tuberculosis: A Multicenter Study in Eastern China. Sci. Total Environ. 2021, 793, 148621. [Google Scholar] [CrossRef]
- Van Gurp, M.; Rood, E.; Fatima, R.; Joshi, P.; Verma, S.C.; Khan, A.H.; Blok, L.; Mergenthaler, C.; Bakker, M.I. Finding Gaps in TB Notifications: Spatial Analysis of Geographical Patterns of TB Notifications, Associations with TB Program Efforts and Social Determinants of TB Risk in Bangladesh, Nepal and Pakistan. BMC Infect. Dis. 2020, 20, 490. [Google Scholar] [CrossRef]
- Datiko, D.G.; Yassin, M.A.; Theobald, S.J.; Blok, L.; Suvanand, S.; Creswell, J.; Cuevas, L.E. Health Extension Workers Improve Tuberculosis Case Finding and Treatment Outcome in Ethiopia: A Large-Scale Implementation Study. BMJ Glob. Health 2017, 2, e000390. [Google Scholar] [CrossRef]
- Tuberculosis and Leprosy National Strategic Plan (July 2021 to June 2026); Ministry of Health (MoH): Addis Ababa, Ethiopia, 20 July 2020; Volume 1, p. 71.
- Kulldorff, M. A Spatial Scan Statistic. Commun. Stat. Theory Methods 1997, 26, 1481–1496. [Google Scholar] [CrossRef]
- Waters, N. A Review of “Handbook of Applied Spatial Analysis: Software Tools, Methods and Applications”; Taylor & Francis: Abingdon, UK, 2012; Volume 102, ISBN 9783642036460. [Google Scholar]
- Consolidated Guidelines on HIV Prevention, Testing, Treatment, Service Delivery and Monitoring: Recommendations for a Public Health Approach; WHO: Geneva, Switzerland, 2021; ISBN 9789240031593.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Years | TB Case Notification per 100,000 Population ^ | HIV Case Notification per 100,000 Population * | ||
|---|---|---|---|---|
| Male | Female | Total | Total | |
| 2018 | 111.63 | 94.66 | 103.21 | 608.33 |
| 2019 | 118.01 | 94.20 | 106.19 | 373.68 |
| 2020 | 105.92 | 87.80 | 96.93 | 278.24 |
| 2021 | 116.65 | 94.16 | 105.49 | 344.18 |
| 2022 | 111.91 | 88.90 | 100.49 | 343.19 |
| Five years | 564.10 | 459.38 | 512.13 | |
| Year | Moran’s | Z-Score | p-Value | Pattern |
|---|---|---|---|---|
| 2018 | 0.084146 | 3.995610 | <0.001 | Clustered |
| 2019 | 0.065740 | 3.217874 | 0.0013 | Clustered |
| 2020 | 0.089804 | 4.292228 | <0.001 | Clustered |
| 2021 | 0.155662 | 7.454590 | <0.001 | Clustered |
| 2022 | 0.160383 | 7.759326 | <0.001 | Clustered |
| Annual Average | 0.121247 | 5.785267 | <0.001 | Clustered |
| Independent Variables | Coefficient (95%CrI) |
|---|---|
| Year | −0.058 (−0.071, −0.046) |
| HIV Positivity Rate | −0.012 (−0.017, −0.006) |
| Population density | 0.491 (0.390, 0.594) |
| Laboratory diagnostic coverage | 0.090 (0.014, 0.166) |
| Health Service coverage | 0.426 (0.347, 0.505) |
| Precipitation | 0.015 (−0.009, 0.038) |
| Temperature | 0.142 (0.070, 0.215) |
| Temperature (squared term) | 0.066 (0.037, 0.096) |
| Wind Speed | −0.140 (−0.212, −0.068) |
| DIC | 16,054.71 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bekele, D.; Aragie, S.; Alene, K.A.; Dejene, T.; Warkaye, S.; Mezemir, M.; Abdena, D.; Kebebew, T.; Botore, A.; Mekonen, G.; et al. Spatiotemporal Distribution of Tuberculosis in the Oromia Region of Ethiopia: A Hotspot Analysis. Trop. Med. Infect. Dis. 2023, 8, 437. https://doi.org/10.3390/tropicalmed8090437
Bekele D, Aragie S, Alene KA, Dejene T, Warkaye S, Mezemir M, Abdena D, Kebebew T, Botore A, Mekonen G, et al. Spatiotemporal Distribution of Tuberculosis in the Oromia Region of Ethiopia: A Hotspot Analysis. Tropical Medicine and Infectious Disease. 2023; 8(9):437. https://doi.org/10.3390/tropicalmed8090437
Chicago/Turabian StyleBekele, Dereje, Solomon Aragie, Kefyalew Addis Alene, Tariku Dejene, Samson Warkaye, Melat Mezemir, Dereje Abdena, Tesfaye Kebebew, Abera Botore, Geremew Mekonen, and et al. 2023. "Spatiotemporal Distribution of Tuberculosis in the Oromia Region of Ethiopia: A Hotspot Analysis" Tropical Medicine and Infectious Disease 8, no. 9: 437. https://doi.org/10.3390/tropicalmed8090437
APA StyleBekele, D., Aragie, S., Alene, K. A., Dejene, T., Warkaye, S., Mezemir, M., Abdena, D., Kebebew, T., Botore, A., Mekonen, G., Gutema, G., Dufera, B., Gemede, K., Kenate, B., Gobena, D., Alemu, B., Hailemariam, D., Muleta, D., Siu, G. K. H., & Tafess, K. (2023). Spatiotemporal Distribution of Tuberculosis in the Oromia Region of Ethiopia: A Hotspot Analysis. Tropical Medicine and Infectious Disease, 8(9), 437. https://doi.org/10.3390/tropicalmed8090437