
Schistosoma Infection Burden and Risk Factors among School-Aged Children in a Rural Area of the Democratic Republic of the Congo

Abstract
:1. Introduction
2. Materials and Methods
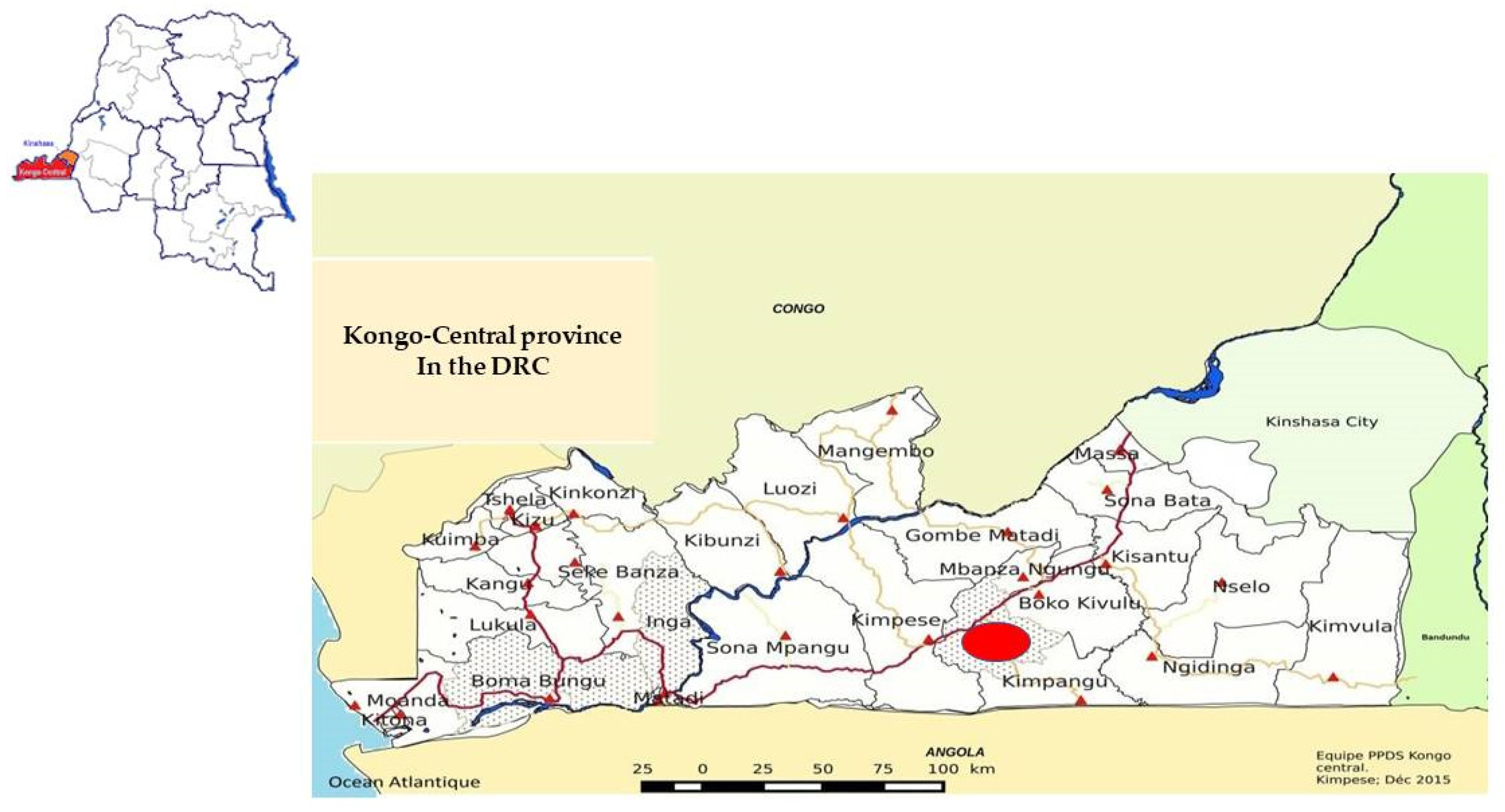
2.1. Study Setting
2.2. Study Design and Procedure
2.3. Laboratory Analysis
2.4. Statistical Analysis
2.5. Ethics Approval and Consent to Participate
3. Results
3.1. General Characteristics of Study Participants
3.2. Schistosoma Infection
3.3. Malaria Infection
3.4. Nutritional Status
3.5. Anemia
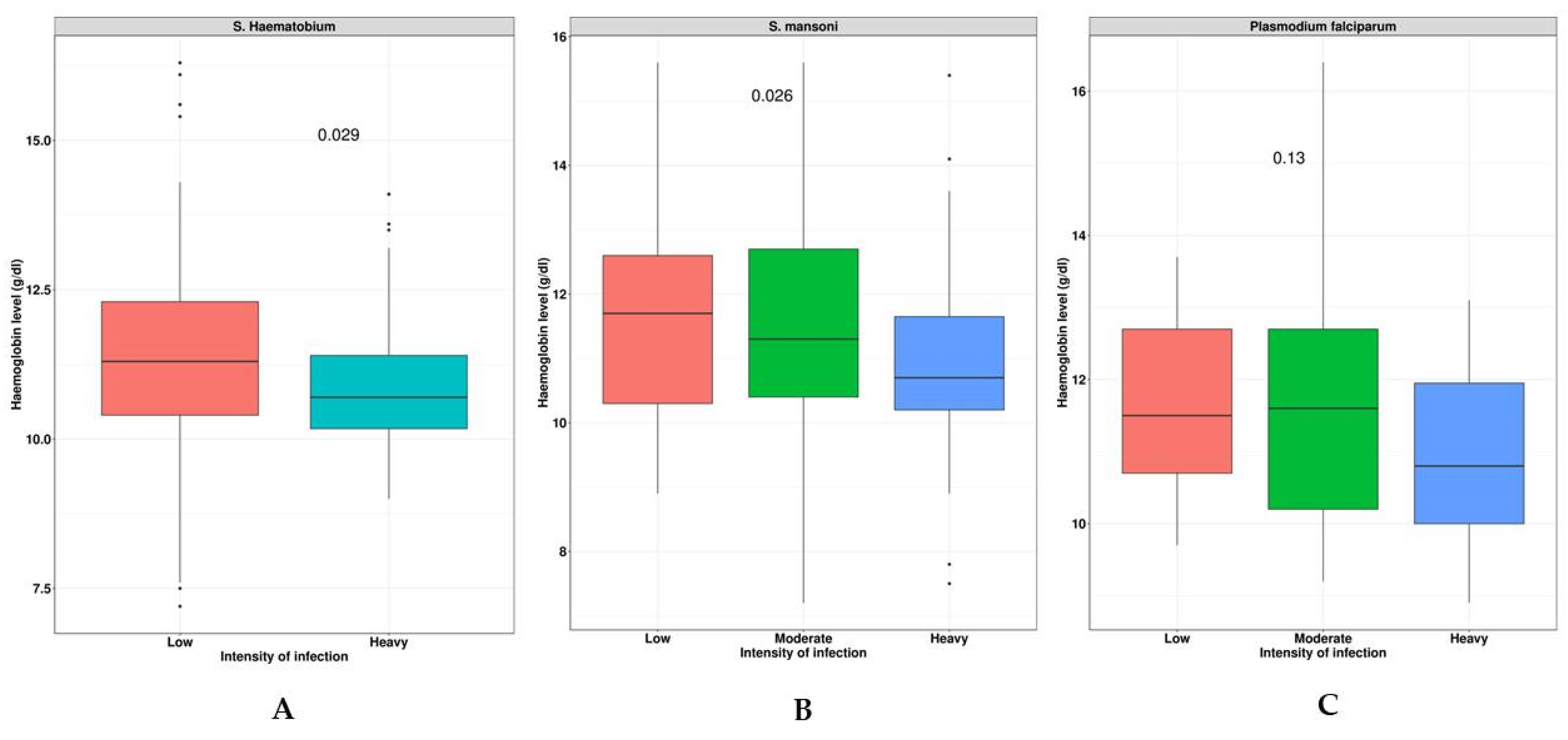
3.6. Schistosoma Species and Malaria Infection Intensities Correlate to Hb Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Schistosomiasis and soil-transmitted helminthiases: Numbers of person treated in 2019. Wkly. Epidemiol. Rec. 2020, 95, 629–640. [Google Scholar]
- Steinmann, P.; Keiser, J.; Bos, R.; Tanner, M.; Utzinger, J. Schistosomiasis and water resources development: Systematic review, meta-analysis, and estimates of people at risk. Lancet Infect. Dis. 2006, 6, 411–425. [Google Scholar] [CrossRef] [PubMed]
- King, C.H. Parasites and poverty: The case of schistosomiasis. Acta Trop. 2010, 113, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Grimes, J.E.; Croll, D.; Harrison, W.E.; Utzinger, J.; Freeman, M.C.; Templeton, M.R. The relationship between water, sanitation and schistosomiasis: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2014, 8, e3296. [Google Scholar] [CrossRef] [PubMed]
- Hailu, T.; Mulu, W.; Abera, B. Effects of Water Source, Sanitation and Hygiene on the Prevalence of Schistosoma mansoni among School Age Children in Jawe District, Northwest Ethiopia. Iran J. Parasitol. 2020, 15, 124–129. [Google Scholar] [CrossRef]
- Walker, J.W.; Kittur, N.; Binder, S.; Castleman, J.D.; Drake, J.M.; Campbell, C.H.; King, C.H.; Colley, D.G. Environmental Predictors of Schistosomiasis Persistent Hotspots following Mass Treatment with Praziquantel. Am. J. Trop. Med. Hyg. 2020, 102, 328–338. [Google Scholar] [CrossRef]
- LoVerde, P.T. Schistosomiasis. Adv. Exp. Med. Biol. 2019, 1154, 45–70. [Google Scholar]
- Gryseels, B. Schistosomiasis. Infect. Dis. Clin. N. Am. 2012, 26, 383–397. [Google Scholar] [CrossRef]
- Colley, D.G.; Bustinduy, A.L.; Secor, W.E.; King, C.H. Human schistosomiasis. Lancet 2014, 383, 2253–2264. [Google Scholar] [CrossRef]
- King, C.H.; Dangerfield-Cha, M. The unacknowledged impact of chronic schistosomiasis. Chronic Illn. 2008, 4, 65–79. [Google Scholar] [CrossRef]
- Friedman, J.F.; Kanzaria, H.K.; McGarvey, S.T. Human schistosomiasis and anemia: The relationship and potential mechanisms. Trends Parasitol. 2005, 21, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Ezeamama, A.E.; Bustinduy, A.L.; Nkwata, A.K.; Martinez, L.; Pabalan, N.; Boivin, M.J.; King, C.H. Cognitive deficits and educational loss in children with schistosome infection-A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12, e0005524. [Google Scholar] [CrossRef]
- Verhoef, H. Asymptomatic malaria in the etiology of iron deficiency anemia: A malariologist’s viewpoint. Am. J. Clin. Nutr. 2010, 92, 1285–1286. [Google Scholar] [CrossRef]
- Brooker, S.; Akhwale, W.; Pullan, R.; Estambale, B.; Clarke, S.E.; Snow, R.W.; Hotez, P.J. Epidemiology of plasmodium-helminth co-infection in Africa: Populations at risk, potential impact on anemia, and prospects for combining control. Am. J. Trop. Med. Hyg. 2007, 77 (Suppl. S6), 88–98. [Google Scholar] [CrossRef] [PubMed]
- Booth, M.; Vennervald, B.J.; Butterworth, A.E.; Kariuki, H.C.; Amaganga, C.; Kimani, G.; Mwatha, J.K.; Otedo, A.; Ouma, J.H.; Dunne, D.W. Exposure to malaria affects the regression of hepatosplenomegaly after treatment for Schistosoma mansoni infection in Kenyan children. BMC Med. 2004, 2, 36. [Google Scholar] [CrossRef] [PubMed]
- Hotez, P.J.; Kamath, A. Neglected tropical diseases in sub-saharan Africa: Review of their prevalence, distribution, and disease burden. PLoS Negl. Trop. Dis. 2009, 3, e412. [Google Scholar] [CrossRef]
- Mazigo, H.D.; Waihenya, R.; Lwambo, N.J.; Mnyone, L.L.; Mahande, A.M.; Seni, J.; Zinga, M.; Kapesa, A.; Kweka, E.J.; Mshana, S.E.; et al. Co-infections with Plasmodium falciparum, Schistosoma mansoni and intestinal helminths among schoolchildren in endemic areas of northwestern Tanzania. Parasit. Vectors 2010, 3, 44. [Google Scholar] [CrossRef]
- Kinung’hi, S.M.; Mazigo, H.D.; Dunne, D.W.; Kepha, S.; Kaatano, G.; Kishamawe, C.; Ndokeji, S.; Angelo, T.; Nuwaha, F. Coinfection of intestinal schistosomiasis and malaria and association with haemoglobin levels and nutritional status in school children in Mara region, Northwestern Tanzania: A cross-sectional exploratory study. BMC Res. Notes 2017, 10, 583. [Google Scholar] [CrossRef]
- World Health Organization. Ending the Neglect to Attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases 2021–2030; Overview; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/bitstream/handle/10665/332094/WHO-UCN-NTD-2020.01-eng.pdf (accessed on 25 May 2021).
- WHO Expert Committee on the Control of Schistosomiasis & World Health Organization. Prevention and Control of Schistosomiasis and Soil-Transmitted Helminthiasis: Report of a WHO Expert Committee; World Health Organization: Geneva, Switzerland, 2002; Available online: https://apps.who.int/iris/handle/10665/42588 (accessed on 6 August 2023).
- Hotez, P. DR Congo and Nigeria: New neglected tropical disease threats and solutions for the bottom 40. PLoS Negl. Trop. Dis. 2019, 13, e0007145. [Google Scholar] [CrossRef]
- Madinga, J.; Linsuke, S.; Mpabanzi, L.; Meurs, L.; Kanobana, K.; Speybroeck, N.; Lutumba, P.; Polman, K. Schistosomiasis in the Democratic Republic of Congo: A literature review. Parasit. Vectors 2015, 8, 601. [Google Scholar] [CrossRef]
- Work Bank Group. WASH Poor in a Water-Rich Country. A Diagnostic of Water, Sanitation, Hygiene, and Poverty in the Democratic Republic of Congo. Available online: https://openknowledge.worldbank.org/bitstream/handle/10986/27320/116679.pdf?sequence=4&isAllowed=y (accessed on 25 May 2021).
- World Health Organization. Status of Schistosomiasis in Endemic Country in 2020. Available online: https://apps.who.int/gho/cabinet/pc.jsp (accessed on 25 May 2021).
- Linsuke, S.; Nundu, S.; Mupoyi, S.; Mukele, R.; Mukunda, F.; Kabongo, M.M.; Inocêncio da Luz, R.; Van Geertruyden, J.P.; Van Sprundel, M.; Boelaert, M.; et al. High prevalence of Schistosoma mansoni in six health areas of—Kasansa health zone, Democratic Republic of the Congo: Short report. PLoS Negl. Trop. Dis. 2014, 8, e3387. [Google Scholar] [CrossRef] [PubMed]
- Kabongo, M.M.; Linsuke, S.; Baloji, S.; Mukunda, F.; Raquel, I.D.L.; Stauber, C.; Van Geertruyden, J.P.; Lutumba, P. Schistosoma mansoni infection and its association with nutrition and health outcomes: A household survey in school-aged children living in Kasansa, Democratic Republic of the Congo. Pan. Afr. Med. J. 2018, 31, 197. [Google Scholar] [CrossRef] [PubMed]
- Khonde, K.R.; Mbanzulu, M.K.; Bin, L. Prevalence of Schistosoma mansoni Infection in Four Health Areas of Kisantu Health Zone, Democratic Republic of the Congo. Adv. Med. 2016, 2016, 6596095. [Google Scholar]
- Mbuyi-Kalonji, L.; Barbe, B.; Nkoji, G.; Madinga, J.; Roucher, C.; Linsuke, S.; Hermy, M.; Heroes, A.S.; Mattheus, W.; Polman, K.; et al. Non-typhoidal Salmonella intestinal carriage in a Schistosoma mansoni endemic community in a rural area of the Democratic Republic of Congo. PLoS Negl. Trop. Dis. 2020, 14, e0007875. [Google Scholar] [CrossRef]
- World Health Organization. Helminth Control in School-Age Children: A Guide for Managers of Control Programmes, 2nd ed.; World Health Organization: Geneva, Switzerland, 2011; Available online: https://apps.who.int/iris/handle/10665/44671 (accessed on 25 May 2021).
- Kabore, A.; Ibikounle, M.; Tougoue, J.J.; Mupoyi, S.; Ndombe, M.; Shannon, S.; Ottesen, E.A.; Mukunda, F.; Awaca, N. Initiating NTD programs targeting schistosomiasis and soil-transmitted helminthiasis in two provinces of the Democratic Republic of the Congo: Establishment of baseline prevalence for mass drug administration. Acta Trop. 2017, 166, 177–185. [Google Scholar] [CrossRef]
- Katz, N.; Chaves, A.; Pellegrino, J. A simple device for quantitative stool thick-smear technique in Schistosomiasis mansoni. Rev. Inst. Med. Trop. Sao Paulo 1972, 14, 397–400. [Google Scholar]
- Mott, K.E.; Baltes, R.; Bambagha, J.; Baldassini, B. Field studies of a reusable polyamide filter for detection of Schistosoma haematobium eggs by urine filtration. Tropenmed Parasitol. 1982, 33, 227–228. [Google Scholar]
- World Health Organization. Basic Malaria Microscopy: Part I Learner’s Guide; Part II Tutor’s Guide; World Health Organization: Geneva, Switzerland, 1991. [Google Scholar]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Vitamin and Mineral Nutrition Information System; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- World Health Organization. Software for Assessing Growth of the World’s Children and Adolescents; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- World Health Organization. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Knoblauch, A.M.; Archer, C.; Owuor, M.; Schmidlin, S.; Divall, M.J.; Utzinger, J.; Winkler, M.S. Schistosomiasis and soil-transmitted helminth infections in schoolchildren in north-eastern Democratic Republic of the Congo. Trans. R Soc. Trop. Med. Hyg. 2016, 110, 424–426. [Google Scholar] [CrossRef]
- Kiazayawoko, F.; Situakibanza, H.N.; Mbula, M.; Bepouka, B.; Longokolo, M.; Mandina, M.; Amaela, E.; Mbonza; Muyilulu, J.J. Prévalence et Déterminants de la Schistosomiase Intestinale Chez Les Écoliers de l’Aire de Santé de Lemfu, Province du Kongo-Central, R.D. Congo; Congo Sciences: Kinshasa, Democratic Republic of the Congo, 2017; Volume 5. [Google Scholar]
- Nigo, M.M.; Odermatt, P.; Salieb-Beugelaar, G.B.; Morozov, O.; Battegay, M.; Hunziker, P.R. Epidemiology of Schistosoma mansoni infection in Ituri Province, north-eastern Democratic Republic of the Congo. PLoS Negl. Trop. Dis. 2021, 15, e0009486. [Google Scholar] [CrossRef]
- Mnkugwe, R.H.; Minzi, O.S.; Kinung’hi, S.M.; Kamuhabwa, A.A.; Aklillu, E. Prevalence and correlates of intestinal schistosomiasis infection among school-aged children in North-Western Tanzania. PLoS ONE 2020, 15, e0228770. [Google Scholar] [CrossRef] [PubMed]
- Noriode, R.M.; Idowu, E.T.; Otubanjo, O.A.; Mafe, M.A. Urinary schistosomiasis in school aged children of two rural endemic communities in Edo State, Nigeria. J. Infect. Public Health 2018, 11, 384–388. [Google Scholar] [CrossRef]
- Mbanzulu, K.M.; Zanga, J.K.; Mukendi, J.P.K.; Mbaya, N.F.; Matangila, J.R.; Muhindo, H.M.; Mpoyi Wa Mpoyi, S.; Aloni, M.N.; Wumba, R. The Impact of Artesunate-Amodiaquine on Schistosoma mansoni Infection among Children Infected by Plasmodium in Rural Area of Lemfu, Kongo Central, Democratic Republic of the Congo. Biomed Res. Int. 2018, 2018, 3487183. [Google Scholar] [CrossRef]
- Matangila, J.R.; Doua, J.Y.; Linsuke, S.; Madinga, J.; da Inocencio, L.R.; Van Geertruyden, J.P.; Lutumba, P. Malaria, schistosomiasis and soil transmitted helminth burden and their correlation with anemia in children attending primary schools in Kinshasa, Democratic Republic of Congo. PLoS ONE 2014, 9, e110789. [Google Scholar] [CrossRef]
- Lengeler, C.; Makwala, J.; Ngimbi, D.; Utzinger, J. Simple school questionnaires can map both Schistosoma mansoni and Schistosoma haematobium in the Democratic Republic of Congo. Acta Trop. 2000, 74, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Angora, E.K.; Boissier, J.; Menan, H.; Rey, O.; Tuo, K.; Toure, A.O.; Coulibaly, J.T.; Méité, A.; Raso, G.; N’goran, E.K.; et al. Prevalence and Risk Factors for Schistosomiasis among Schoolchildren in two Settings of Cote d’Ivoire. Trop. Med. Infect Dis. 2019, 4, 110. [Google Scholar] [CrossRef] [PubMed]
- Mazigo, H.D.; Uisso, C.; Kazyoba, P.; Nshala, A.; Mwingira, U.J. Prevalence, infection intensity and geographical distribution of schistosomiasis among pre-school and school aged children in villages surrounding Lake Nyasa, Tanzania. Sci. Rep. 2021, 11, 295. [Google Scholar] [CrossRef]
- Zeleke, A.J.; Addisu, A.; Tegegne, Y. Prevalence, Intensity, and Associated Factors of Schistosoma mansoni among School Children in Northwest Ethiopia. J. Parasitol. Res. 2020, 2020, 8820222. [Google Scholar] [CrossRef]
- Onyekwere, A.M.; Rey, O.; Nwanchor, M.C.; Alo, M.; Angora, E.K.; Allienne, J.F.; Boissier, J. Prevalence and risk factors associated with urogenital schistosomiasis among primary school pupils in Nigeria. Parasite Epidemiol. Control 2022, 18, e00255. [Google Scholar] [CrossRef]
- Senghor, B.; Diallo, A.; Sylla, S.N.; Doucoure, S.; Ndiath, M.O.; Gaayeb, L.; Djuikwo-Teukeng, F.F.; Bâ, C.T.; Sokhna, C. Prevalence and intensity of urinary schistosomiasis among school children in the district of Niakhar, region of Fatick, Senegal. Parasit. Vectors 2014, 7, 5. [Google Scholar] [CrossRef]
- Sow, S.; de Vlas, S.J.; Stelma, F.; Vereecken, K.; Gryseels, B.; Polman, K. The contribution of water contact behavior to the high Schistosoma mansoni Infection rates observed in the Senegal River Basin. BMC Infect. Dis. 2011, 11, 198. [Google Scholar] [CrossRef]
- Ayabina, D.V.; Clark, J.; Bayley, H.; Lamberton, P.H.L.; Toor, J.; Hollingsworth, T.D. Gender-related differences in prevalence, intensity and associated risk factors of Schistosoma infections in Africa: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2021, 15, e0009083. [Google Scholar] [CrossRef]
- Ogweno, G.; Mushi, V.; Silvestri, V.; Bonaventura, W.; Justine, N.C.; Noah, M.; Yoram, F.; Mohamed, H.; Tarimo, D. Burden and risk factors for Schistosoma mansoni infection among primary school children: A quantitative school-based cross-sectional survey in Busega district, Northern Tanzania. PLoS ONE 2023, 18, e0280180. [Google Scholar] [CrossRef]
- Kloos, H.; Correa-Oliveira, R.; dos Reis, D.C.; Rodrigues, E.W.; Monteiro, L.A.; Gazzinelli, A. The role of population movement in the epidemiology and control of schistosomiasis in Brazil: A preliminary typology of population movement. Mem. Inst. Oswaldo Cruz. 2010, 105, 578–586. [Google Scholar] [CrossRef]
- Isnard, A.; Chevillard, C. Recent advances in the characterization of genetic factors involved in human susceptibility to infection by schistosomiasis. Curr. Genom. 2008, 9, 290–300. [Google Scholar] [CrossRef]
- Ayeh-Kumi, P.F.; Addo-Osafo, K.; Attah, S.K.; Tetteh-Quarcoo, P.B.; Obeng-Nkrumah, N.; Awuah-Mensah, G.; Abbey, H.N.A.; Forson, A.; Cham, M.; Asare, L.; et al. Malaria, helminths and malnutrition: A cross-sectional survey of school children in the South-Tongu district of Ghana. BMC Res. Notes 2016, 9, 242. [Google Scholar] [CrossRef]
- Munisi, D.Z.; Buza, J.; Mpolya, E.A.; Kinung’hi, S.M. Schistosoma mansoni Infections, Undernutrition and Anaemia among Primary Schoolchildren in Two Onshore Villages in Rorya District, North-Western Tanzania. PLoS ONE 2016, 11, e0167122. [Google Scholar] [CrossRef]
- Mboera, L.E.; Senkoro, K.P.; Rumisha, S.F.; Mayala, B.K.; Shayo, E.H.; Mlozi, M.R. Plasmodium falciparum and helminth coinfections among schoolchildren in relation to agro-ecosystems in Mvomero District, Tanzania. Acta Trop. 2011, 120, 95–102. [Google Scholar] [CrossRef]
- Colt, S.; Miller, C.D.; Edielu, A.; Webb, E.L.; Mawa, P.A.; Wu, H.W.; Nakyesige, R.; Muheki, E.; Kabatereine, N.; Bustinduy, A.L.; et al. Relationships between Schistosoma mansoni infection intensity and nutritional status and anemia among preschool-aged children in Uganda. Clin. Infect. Dis. 2023, ciad470. [Google Scholar] [CrossRef]
- Aemero, M.; Berhe, N.; Erko, B. Status of Schistosoma mansoni prevalence and intensity of infection in geographically apart endemic localities of Ethiopia: A comparison. Ethiop. J. Health Sci. 2014, 24, 189–194. [Google Scholar] [CrossRef]
- Mutombo, N.; Landoure, A.; Man, W.Y.; Fenwick, A.; Dembele, R.; Sacko, M.; Keita, A.D.; Traoré, M.S.; Webster, J.P.; McLaws, M.L. The association between child Schistosoma spp. infections and morbidity in an irrigated rice region in Mali: A localized study. Acta Trop. 2019, 199, 105115. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Frequency | % (95% CI) |
|---|---|---|
| Overall | 480 | |
| Gender | ||
| Female | 239 | 49.8 (45.3–54.3) |
| Male | 241 | 50.2 (45.7–54.7) |
| Median age (IQR) | 9 (7–11) | |
| Age groups (years) | ||
| 5–9 | 251 | 52.3 (47.8–56.8) |
| 10–14 | 229 | 47.7 (43.2–52.2) |
| Household sanitation | ||
| Toilet in the household | 117 | 24.4 (20.5–28.2) |
| Taps in the household | 480 | 100 |
| Water contact | 428 | 89.2 (86.4–91.9) |
| Swimming in the river | 382 | 79.6 (75.9–83.2) |
| Washing dishes in the river | 281 | 58.5 (54.1–62.9) |
| Washing clothes in the river | 329 | 68.5 (64.4–72.7) |
| Parasitic infection | ||
| Schistosoma infection | 268 | 55.8 (51.4–60.3) |
| S. haematobium | 197 | 41.0 (36.6–45.5) |
| S. mansoni | 174 | 36.3 (31.9–40.6) |
| Mixed S. haematobium–S. mansoni | 103 | 38.4 (32.6–44.3) |
| Malaria infection | 81 | 16.9 (13.5–20.2) |
| P. falciparum | 70 | 14.6 (11.4–17.7) |
| P. malariae | 10 | 2.1 (0.8–3.4) |
| Mixed P. falciparum–P. malariae | 1 | 0.2 (0.0–0.01) |
| Coinfection Schistosoma–malaria | 31 | 6.5 (4.3–8.7) |
| Median Hb level, g/dL (IQR) | 11.6 (10.5–12.6) | |
| Anemia | 237 | 49.4 (44.9–53.9) |
| Mild anemia (Hb 10–11.4 g/dL) | 27.0 (21.3–32.7) | |
| Moderate anemia (Hb 7–9.9 g/dL) | 166 | 70.0 (64.2–75.9) |
| Severe anemia (Hb < 7 g/dL) | 7 | 2.9 (0.08–0.5) |
| Nutritional status | ||
| Stunting | 138 | 28.7 (24.7–32.8) |
| HAZ, mean ± SD | −1.7 ± 1.6 | |
| Underweight | 51 | 17.1 (12.8–21.4) |
| WAZ, mean ± SD | −1.5 ± 1.2 | |
| Thinness | 34 | 7.1 (4.8–9.4) |
| BAZ, mean ± SD | −0.9 ± 1.3 | |
| Variables | S. haematobium | S. mansoni | P. falciparum |
|---|---|---|---|
| No. of non-infected (%) | 283 (58.9) | 306 (63.8) | 409 (85.2) |
| No. of light infection (%) | 133 (67.5) | 37 (21.3) | 25 (5.2) |
| No. of moderate infection (%) | NA | 47 (27.0) | 27 (5.6) |
| No. of heavy infection (%) | 64 (32.5) | 90 (51.7) | 19 (3.9) |
| Geometric mean egg count (95% CI) | 16.6 (12.9–21.3) | 390.2 (300.2–507.3) | 927.4 (667.4–1288.7) |
| Variables | N | n (%) | cOR (95% CI) | p-Value | aOR (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Gender | ||||||
| Female | 239 | 136 (56.9) | Ref. | |||
| Male | 241 | 132 (54.8) | 0.9 (0.6–1.3) | 0.638 | 0.9 (0.6–1.3) | 0.638 |
| Age groups (years) | ||||||
| 5–9 | 251 | 118 (47.0) | Ref. | |||
| 10–14 | 229 | 150 (65.5) | 2.1 (1.5–3.1) | <0.001 | 2.2 (1.5–3.1) | <0.001 * |
| Swimming in the river | ||||||
| No | 98 | 53 (54.1) | Ref. | |||
| Yes | 382 | 215 (56.3) | 1.1 (0.7–1.7) | 0.696 | 1.1 (0.7–1.8) | 0.594 |
| Washing clothes in the river | ||||||
| No | 151 | 88 (58.3) | Ref. | |||
| Yes | 329 | 180 (54.7) | 0.9 (0.6–1.3) | 0.465 | 0.7 (0.4–1.3) | 0.253 |
| Washing dishes in the river | ||||||
| No | 199 | 111 (55.8) | Ref. | |||
| Yes | 281 | 157 (55.9) | 1.0 (0.7–1.4) | 0.984 | 1.3 (0.7–2.1) | 0.399 |
| Taps in the household | ||||||
| No | 480 | 268 (55.8) | Ref. | |||
| Yes | 0 | 0 (0) | (omitted) | – | – | – |
| Toilet in the household | ||||||
| No | 363 | 203 (55.9) | Ref. | |||
| Yes | 117 | 65 (55.6) | 1.0 (0.6–1.5) | 0.945 | 1.0 (0.7–1.6) | 0.925 |
| Variables | N | n (%) | cOR (95% CI) | p-Value | aOR (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Gender | ||||||
| Female | 239 | 121 (50.6) | Ref. | |||
| Male | 241 | 116 (48.1) | 0.9 (0.6–1.3) | 0.585 | 0.9 (0.6–1.4) | 0.785 |
| Age groups (years) | ||||||
| 5–9 | 251 | 133 (52.9) | Ref. | |||
| 10–14 | 229 | 104 (45.4) | 0.7 (0.5–1.1) | 0.098 | 0.6 (0.4–0.9) | 0.012 * |
| Schistosoma infection | ||||||
| No | 212 | 73 (34.4) | Ref. | |||
| Yes | 268 | 164 (61.2) | 3.0 (2.1–4.4) | <0.001 | 3.0 (2.0–4.6) | <0.001 * |
| Malaria infection | ||||||
| No | 399 | 201 (50.4) | Ref. | |||
| Yes | 81 | 36 (44.4) | 0.8 (0.5–1.3) | 0.331 | 1.0 (0.6–1.8) | 0.563 |
| Stunting | ||||||
| No | 342 | 201 (58.8) | Ref. | |||
| Yes | 136 | 36 (26.1) | 0.2 (0.2–0.4) | <0.001 | 0.3 (0.2–0.4) | <0.001 * |
| Underweight | ||||||
| No | 247 | 137 (55.5) | Ref. | |||
| Yes | 51 | 22 (43.1) | 0.6 (0.3–1.1) | 0.110 | – | - |
| Thinness | ||||||
| No | 446 | 222 (49.8) | Ref. | |||
| Yes | 34 | 15 (44.1) | 0.8 (0.4–1.6) | 0.525 | – | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Linsuke, S.; Ilombe, G.; Disonama, M.; Nzita, J.D.; Mbala, P.; Lutumba, P.; Van Geertruyden, J.-P. Schistosoma Infection Burden and Risk Factors among School-Aged Children in a Rural Area of the Democratic Republic of the Congo. Trop. Med. Infect. Dis. 2023, 8, 455. https://doi.org/10.3390/tropicalmed8090455
Linsuke S, Ilombe G, Disonama M, Nzita JD, Mbala P, Lutumba P, Van Geertruyden J-P. Schistosoma Infection Burden and Risk Factors among School-Aged Children in a Rural Area of the Democratic Republic of the Congo. Tropical Medicine and Infectious Disease. 2023; 8(9):455. https://doi.org/10.3390/tropicalmed8090455
Chicago/Turabian StyleLinsuke, Sylvie, Gillon Ilombe, Michel Disonama, Jean Deny Nzita, Placide Mbala, Pascal Lutumba, and Jean-Pierre Van Geertruyden. 2023. "Schistosoma Infection Burden and Risk Factors among School-Aged Children in a Rural Area of the Democratic Republic of the Congo" Tropical Medicine and Infectious Disease 8, no. 9: 455. https://doi.org/10.3390/tropicalmed8090455
APA StyleLinsuke, S., Ilombe, G., Disonama, M., Nzita, J. D., Mbala, P., Lutumba, P., & Van Geertruyden, J.-P. (2023). Schistosoma Infection Burden and Risk Factors among School-Aged Children in a Rural Area of the Democratic Republic of the Congo. Tropical Medicine and Infectious Disease, 8(9), 455. https://doi.org/10.3390/tropicalmed8090455