

International Migration, Refugees, and Spread of Tuberculosis in Brazil: Analysis of Clusters, Trends, and Associated Factors (2010–2021)

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Scenario
2.1.1. Study Population
2.1.2. Data Sources
2.2. Analysis Plan
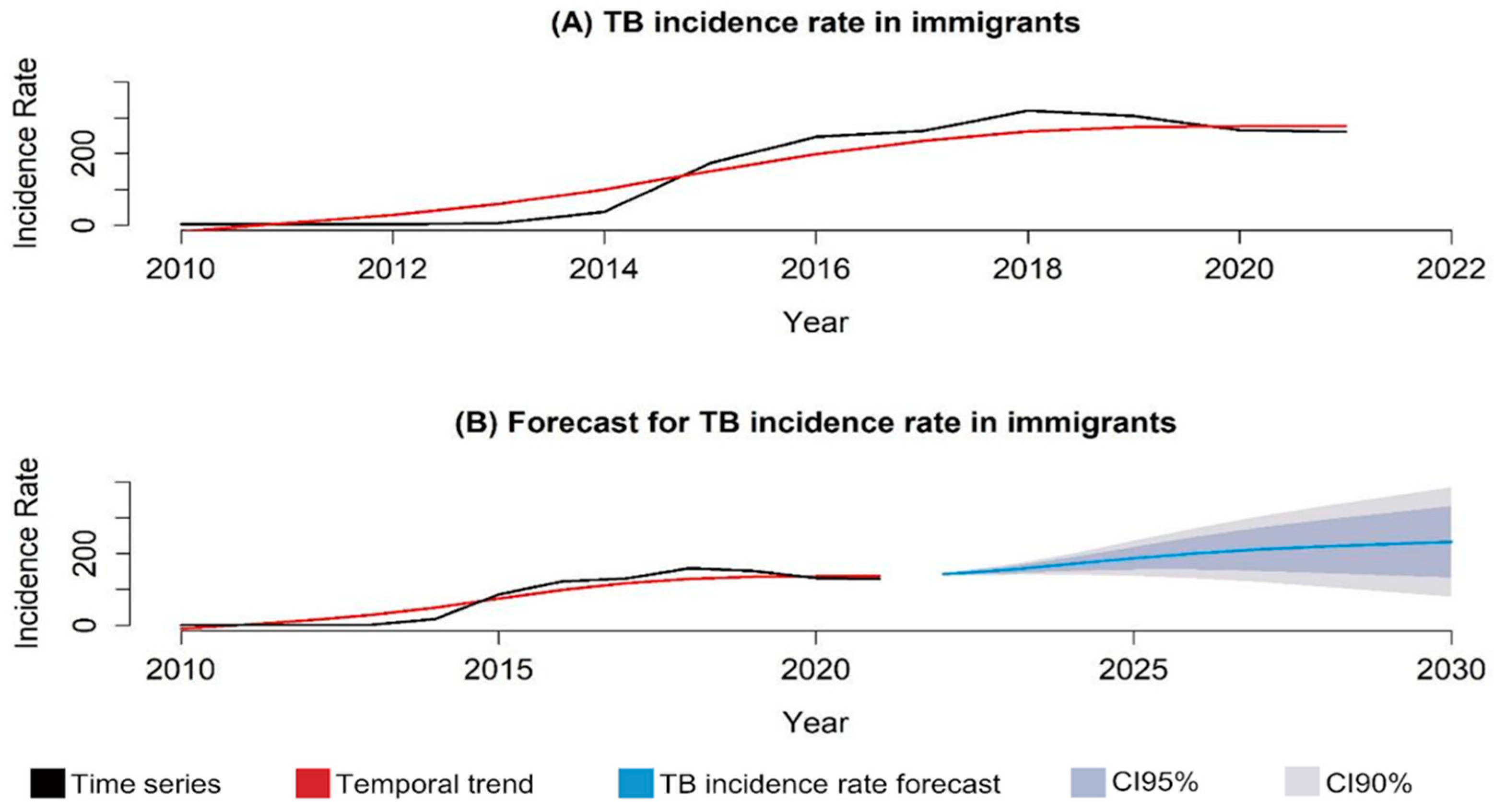
2.2.1. Time Series Analysis
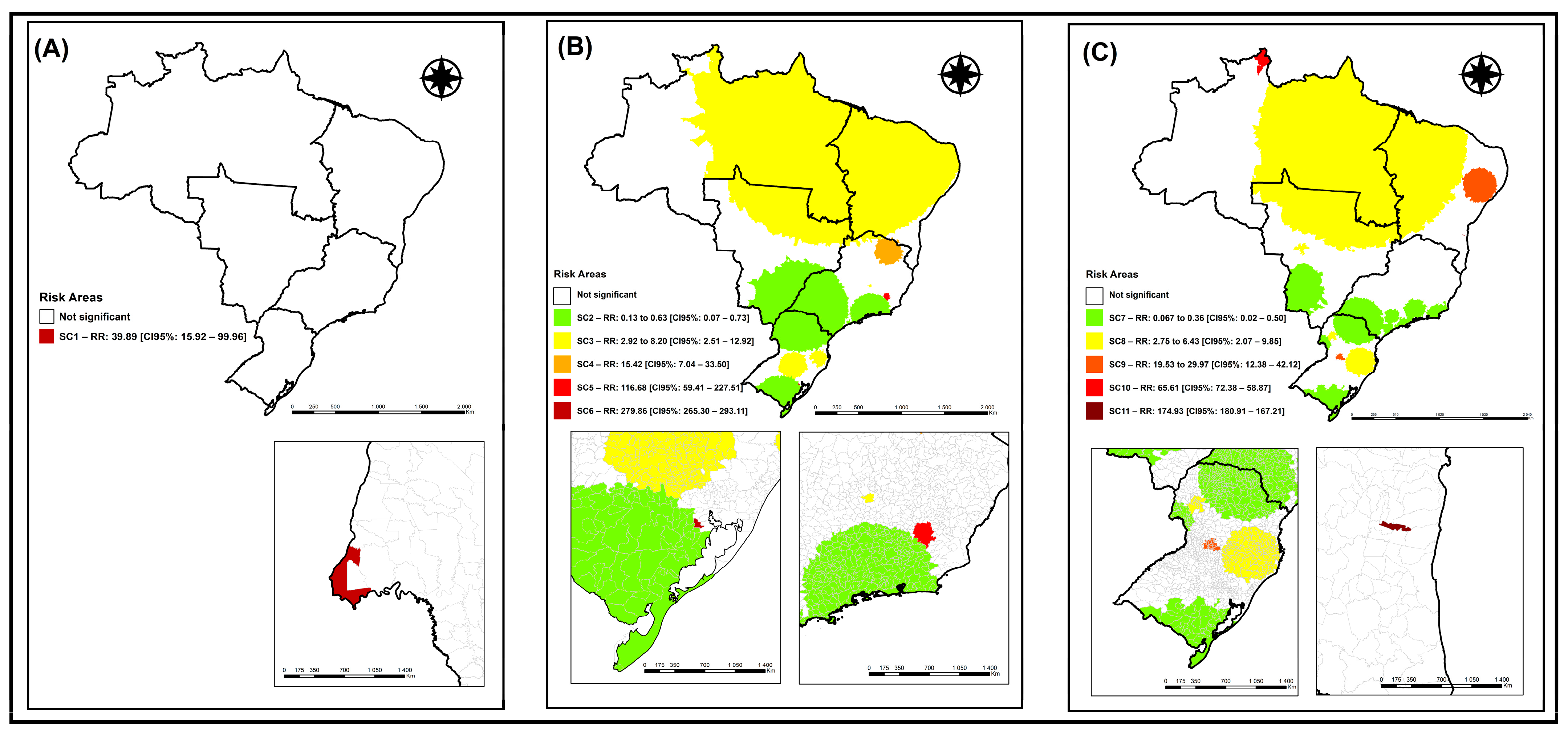
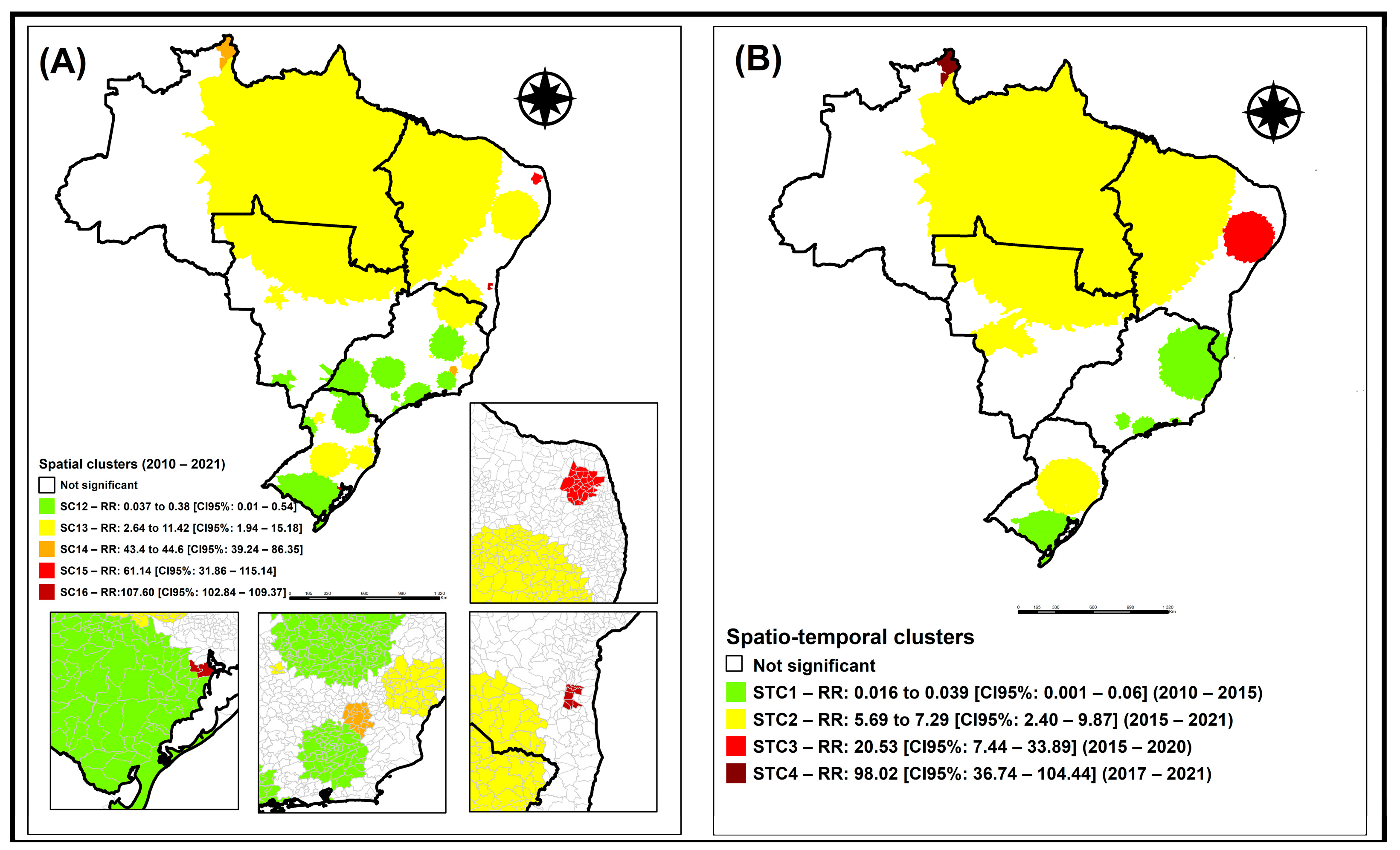
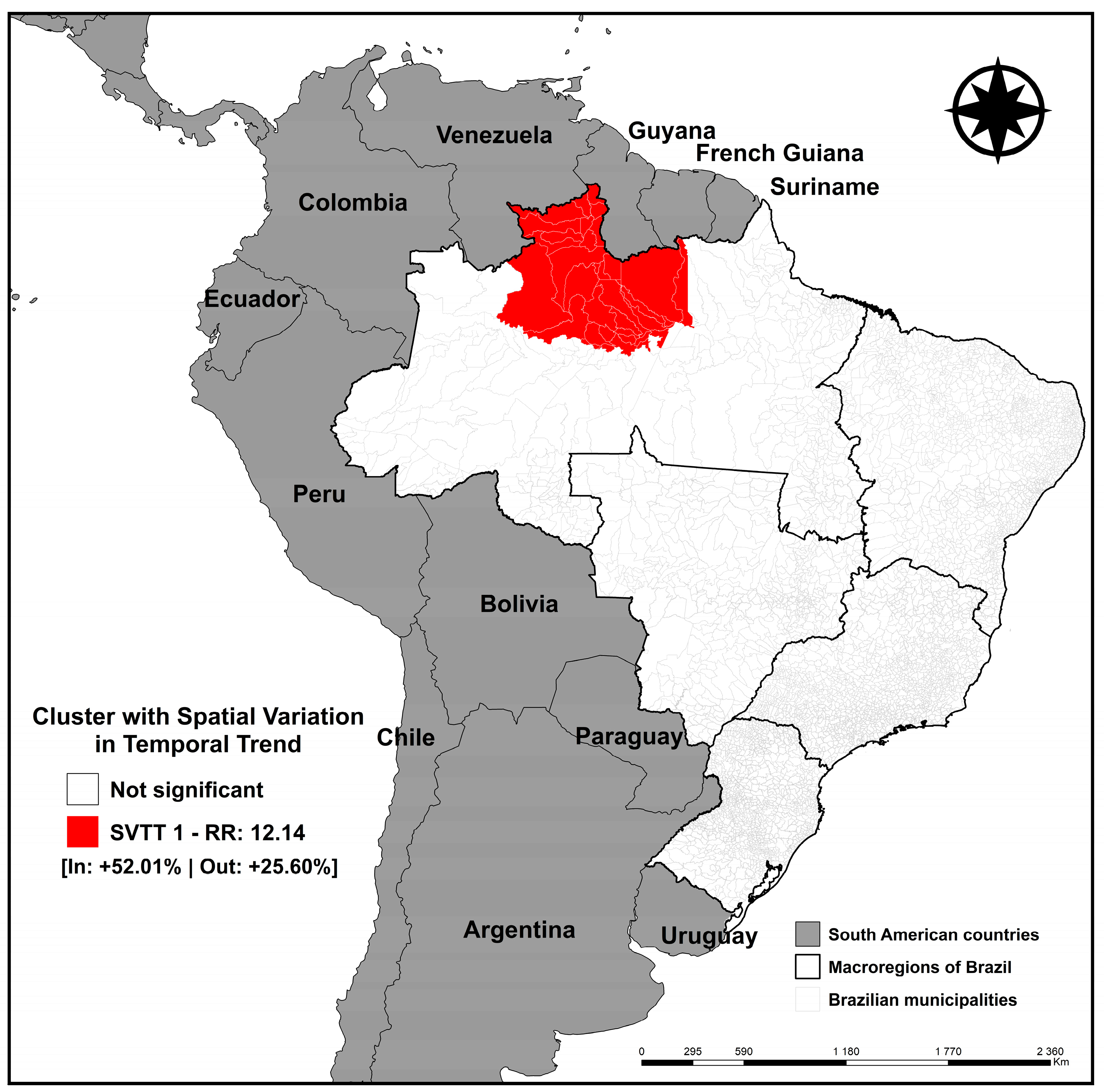
2.2.2. Identification of Clusters
2.2.3. Logistic Regression
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Jezus, S.V.; Sales, C.M.M.; Rissino, S.d.D.; Mocelin, H.J.S.; Araújo, M.P.d.S.; Arcêncio, R.A.; Araújo, V.M.S.; Terena, N.d.F.M.; Freitas, P.d.S.S.; Maciel, E.L.N. Prevalence of tuberculosis, COVID-19, chronic conditions and vulnerabilities among migrants and refugees: An electronic survey. Rev. Lat.-Am. Enferm. 2023, 31, e3690. [Google Scholar] [CrossRef] [PubMed]
- Abubakar, I.; Aldridge, R.W.; Devakumar, D.; Orcutt, M.; Burns, R.; Barreto, M.L.; Dhavan, P.; Fouad, F.M.; Groce, N.; Guo, Y.; et al. The UCL–Lancet Commission on Migration and Health: The health of a world on the move. Lancet 2018, 392, 2606–2654. [Google Scholar] [CrossRef]
- Dhavan, P.; Dias, H.M.; Creswell, J.; Weil, D. An overview of tuberculosis and migration. Int. J. Tuberc. Lung Dis. 2017, 21, 610–623. [Google Scholar] [CrossRef] [PubMed]
- Alto Comissariado das Nações Unidas para Refugiados (ACNUR). Protegendo Refugiados no Brasil e no Mundo. 2018. Available online: https://www.acnur.org/portugues/wp-content/uploads/2018/02/Protegendo-Refugiados-no-Brasil-e-no-Mundo_ACNUR-2018.pdf (accessed on 25 February 2023).
- OIM; International Organization for Migration. World Migration Report 2022; IOM: Geneva, Switzerland, 2022; ISBN 978-92-9268-076-3. Available online: https://publications.iom.int/system/files/pdf/WMR-2022.pdf (accessed on 3 March 2023).
- Cavalcanti, L.; Oliveira, T.; Silva, B.G. Relatório Anual 2021—2011–2020: Uma Década de Desafios Para a Imigração e o Refúgio no Brasil; Série Migrações; Observatório das Migrações Internacionais; Ministério da Justiça e Segurança Pública/Conselho Nacional de Imigração e Coordenação Geral de Imigração Laboral. OBMigra: Brasília, Brazil, 2021. Available online: https://portaldeimigracao.mj.gov.br/images/Obmigra_2020/Relat%C3%B3rio_Anual/Relato%CC%81rio_Anual_-_Completo.pdf (accessed on 3 March 2023).
- United Kingdom Health Security Agency (UKHSA). WHO Estimates of Tuberculosis Incidence by Country and Territory. 2020. Available online: https://www.gov.uk/government/publications/tuberculosis-tb-by-country-rates-per-100000-people/who-estimates-of-tuberculosis-incidence-by-country-and-territory-2020-accessible-text-version (accessed on 27 February 2023).
- Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde e Ambiente|Ministério da Saúde. Boletim Epidemiológico. Tuberculose. 2023. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/especiais/2023/boletim-epidemiologico-de-tuberculose-numero-especial-mar.2023/view (accessed on 27 February 2023).
- Pavli, A.; Maltezou, H. Health problems of newly arrived migrants and refugees in Europe. J. Travel Med. 2017, 24. [Google Scholar] [CrossRef] [PubMed]
- Meaza, A.; Tola, H.H.; Eshetu, K.; Mindaye, T.; Medhin, G.; Gumi, B. Tuberculosis among refugees and migrant populations: Systematic review. PLoS ONE 2022, 17, e0268696. [Google Scholar] [CrossRef]
- Dasgupta, K.; Menzies, D. Cost-effectiveness of tuberculosis control strategies among immigrants and refugees. Eur. Respir. J. 2005, 25, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.R.; Mello, F.C.d.Q.; Johansen, F.D.C.; Centis, R.; D’Ambrosio, L.; Migliori, G.B. Migration and medical screening for tuberculosis. J. Bras. Pneumol. 2023, 49, e20230051. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Tuberculosis Report. 2022. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022 (accessed on 10 March 2023).
- MPareek, M.; Greenaway, C.; Noori, T.; Munoz, J.; Zenner, D. The impact of migration on tuberculosis epidemiology and control in high-income countries: A review. BMC Med. 2016, 14, 48. [Google Scholar] [CrossRef]
- Arcêncio, R.A.; Berra, T.Z.; Terena, N.d.F.M.; Rocha, M.P.; Alecrim, T.F.d.A.; Kihara, F.M.d.S.; Mascarello, K.C.; Sales, C.M.M.; Maciel, E.L.N. Spatial clustering and temporal trend analysis of international migrants diagnosed with tuberculosis in Brazil. PLoS ONE 2021, 16, e0252712. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Municípios da Faixa de Fronteira [Internet]. 2023. Available online: https://www.ibge.gov.br/geociencias/organizacao-do-territorio/estrutura-territorial/24073-municipios-da-faixa-de-fronteira.html?=&t=sobre (accessed on 22 February 2023).
- Gonçalves, D. Tuberculose em Imigrantes: Identificação e Análise das Características Associadas. Tese de Doutorado. Universidade de São Paulo. 2019. Available online: https://teses.usp.br/teses/disponiveis/17/17139/tde-12072019-105117/pt-br.php (accessed on 8 March 2023).
- Santo, K.d.S.G.D.; Paste, A.A.; Maturino, H.S.d.A.; Rocha, V.O.; Junior, G.S.O.; Coelho, G.M.; Oliveira, M.S.S.; Torres, L.M. Desfecho de Pacientes com Tuberculose Pertencentes a Populações Vulneráveis no Brasil, em 2020. Braz. J. Infect. Dis. 2022, 26, 102303. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística. Brasil em Síntese [Internet]. 2020. Available online: https://www.ibge.gov.br/geociencias (accessed on 22 February 2023).
- Cleveland, R.; Cleveland, W.; McRee, J.E. Seasonal-trend decomposition procedure based on LOESS. J. Off. Stat. 1990, 6, 3–73. Available online: http://www.nniiem.ru/file/news/2016/stl-statistical-model.pdf (accessed on 1 March 2023).
- Hyndman, R.; Athanasopoulos, G.; Bergmeir, C.; Caceres, G.; Chhay, L.; Kuroptev, K.; O’Hara-Wild, M.; Petropoulos, F.; Razbash, S.; Wang, E.; et al. Forecasting: Forecasting Functions for Time Series and Linear Models. 2023. Available online: https://cran.r-project.org/web/packages/forecast/forecast.pdf (accessed on 6 March 2023).
- Box, G.E.; Jenkins, G.M.; Reinsel, G.C.; Ljung, G.M. Time Series Analysis: Forecasting and Control, 5th ed.; Wiley: Hoboken, NJ, USA, 2015; Available online: https://books.google.com.br/books?hl=pt-BR&lr=&id=rNt5CgAAQBAJ&oi=fnd&pg=PR7&dq=Time+Series+Analysis:+Forecasting+and+Control.+Wiley,+5+edition,+2015.&ots=DL18AVoXRz&sig=yp7bsP6bjzMh2mP07NRY2URl5UA#v=onepage&q=Time%20Series%20Analysis%3A%20Forecasting%20and%20Control.%20Wiley%2C%205%20edition%2C%202015.&f=false (accessed on 5 March 2023).
- Camelo, H.D.N.; Lucio, P.S.; Junior, J.B.V.L.; de Carvalho, P.C.M. Métodos de previsão de séries temporais e modelagem híbrida ambos aplicados em médias mensais de velocidade do vento para regiões do nordeste do Brasil. Rev. Bras. Meteorol. 2017, 32, 565–574. [Google Scholar] [CrossRef]
- Kulldorff, M.; Nagarwalla, N. Spatial disease clusters: Detection and inference. Stat. Med. 1995, 14, 799–810. [Google Scholar] [CrossRef] [PubMed]
- Kulldorff, M. SaTScan User Guide V9.4. 2015. Available online: https://edisciplinas.usp.br/pluginfile.php/7199540/mod_resource/content/2/SaTScan_TM_Manual_do_Usuario_v9.4_Portugues_2016_05.pdf (accessed on 5 March 2023).
- Moraga, P.; Kulldorff, M. Detection of spatial variations in temporal trends with a quadratic function. Stat. Methods Med Res. 2016, 25, 1422–1437. [Google Scholar] [CrossRef]
- Jaisankar, R.; Kesavan, J. A study on spatial variations in temporal trends of dengue incidences in Tamil Nadu, India. Int. J. Sci. Technol. Res. 2019, 8, 788–792. Available online: https://www.researchgate.net/profile/Kesavan-Janarthanan/publication/335978484_A_Study_On_Spatial_Variations_In_Temporal_Trends_Of_Dengue_Incidences_In_Tamil_Nadu_India/links/5e58a0b6a6fdccbeba07b149/A-Study-On-Spatial-Variations-In-Temporal-Trends-Of-Dengue-Incidences-In-Tamil-Nadu-India.pdf (accessed on 13 March 2023).
- Han, J.; Zhu, L.; Kulldorff, M.; Hostovich, S.; Stinchcomb, D.G.; Tatalovich, Z.; Lewis, D.R.; Feuer, E.J. Using Gini coefficient to determining optimal cluster reporting sizes for spatial scan statistics. J. Health Geogr. 2016, 15, 27. [Google Scholar] [CrossRef] [PubMed]
- Zuur, A.F.; Ieno, E.N.; Elphick, C.S. A protocol for data exploration to avoid common statistical problems. Methods Ecol. Evol. 2010, 1, 3–14. [Google Scholar] [CrossRef]
- Šimundić, A.M. Medidas de acurácia diagnóstica: Definições básicas. Electron. J. Int. Fed. Clin. Chem. Lab. Med. 2009, 19, 203–211. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4975285/ (accessed on 9 March 2023).
- Cavalcanti, L.; Oliveira, T.; Macedo, M. Imigração e Refúgio no Brasil. Relatório Anual 2019; Série Migrações; Observatório das Migrações Internacionais; Ministério da Justiça e Segurança Pública/Conselho Nacional de Imigração e Coordenação Geral de Imigração Laboral. OBMigra: Brasília, Brazil, 2019. Available online: https://portaldeimigracao.mj.gov.br/images/relatorio-anual/RELAT%C3%93RIO%20ANUAL%20OBMigra%202019.pdf (accessed on 22 March 2023).
- Cavalcanti, L.; Oliveira, T.; Silva, B.G. Relatório Anual OBMigra 2022; Série Migrações; Observatório das Migrações Internacionais; Ministério da Justiça e Segurança Pública/Conselho Nacional de Imigração e Coordenação Geral de Imigração Laboral. OBMigra: Brasília, Brazil, 2022. Available online: https://portaldeimigracao.mj.gov.br/images/Obmigra_2020/OBMigra_2022/RELAT%C3%93RIO_ANUAL/Relat%C3%B3rio_Anual_2022_-_Vers%C3%A3o_completa_01.pdf (accessed on 6 March 2023).
- Mamed, L.H.; De Lima, E.O. Trabalho, precarização e migração: O processo de recrutamento de haitianos na Amazônia acreana pela agroindústria brasileira. Novos Cad. NAEA 2015, 18, 33–64. [Google Scholar] [CrossRef]
- Barreto-Duarte, B.; Araújo-Pereira, M.; Nogueira, B.M.F.; Sobral, L.; Rodrigues, M.M.S.; Queiroz, A.T.L.; Rocha, M.S.; Nascimento, V.; Souza, A.B.; Cordeiro-Santos, M.; et al. Tuberculosis Burden and Determinants of Treatment Outcomes According to Age in Brazil: A Nationwide Study of 896,314 Cases Reported Between 2010 and 2019. Front. Med. 2021, 8, 706689. [Google Scholar] [CrossRef]
- Hertz, D.; Schneider, B. Sex differences in tuberculosis. Semin. Immunopathol. 2018, 41, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, L.; Tonhati, T.; Dutra, D.; De Oliveira, M. A Imigração Haitiana no Brasil: Características Sociodemográficas e Laborais na Região Sul e no Distrito Federal; OBMIGRA: Brasília, Brazil, 2016. Available online: https://portaldeimigracao.mj.gov.br/images/publicacoes/A_imigra%C3%A7%C3%A3o_Haitiana_no_Brasil_Caracter%C3%ADsticas_Demogr%C3%A1ficas_na_regi%C3%A3o_Sul_e_no_Distrito_Federal.pdf (accessed on 5 March 2023).
- Gómez, C.; Herrera, G. (Eds.) State and ‘Mixed Migrations’: Migration Policies towards Haitians, Colombians and Venezuelans in Ecuador. In Migration in South America; IMISCOE Regional Reader: Quito, Ecuador, 2022; pp. 77–95. [Google Scholar]
- Díaz-Quijano, F.A.; Rodríguez-Morales, A.J.; Waldman, E.A. Migration, public health and infectious diseases in South America. PLoS ONE 2018, 13, e0194114. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Coefficient | p-Value | OR | 95% CI |
|---|---|---|---|---|
| TB incidence rate (median: 14.40) | 1.1262 | <0.01 * | 3.08 | 2.42–3.94 |
| International migrant population | 19.0827 | 0.94983 | NA | NA |
| Municipality population (median: 11042) | 1.1726 | <0.01 * | 3.23 | 2.49–4.22 |
| Mean household income per capita (median: 456.43) | −0.4335 | <0.01 * | 0.64 | 0.47–0.87 |
| Gini index 2010 (median: 0.49) | 0.2125 | 0.04 * | 1.23 | 1.01–1.52 |
| Illiteracy rate—15 years or older (median: 13.12) | 0.2529 | 0.02 * | 1.77 | 1.62–1.96 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alves, Y.M.; Berra, T.Z.; Tavares, R.B.V.; Popolin, M.A.P.; da Costa, F.B.P.; de Jezus, S.V.; Ferezin, L.P.; Tártaro, A.F.; Serrano-Gallardo, M.D.P.; Pinto, I.C.; et al. International Migration, Refugees, and Spread of Tuberculosis in Brazil: Analysis of Clusters, Trends, and Associated Factors (2010–2021). Trop. Med. Infect. Dis. 2024, 9, 82. https://doi.org/10.3390/tropicalmed9040082
Alves YM, Berra TZ, Tavares RBV, Popolin MAP, da Costa FBP, de Jezus SV, Ferezin LP, Tártaro AF, Serrano-Gallardo MDP, Pinto IC, et al. International Migration, Refugees, and Spread of Tuberculosis in Brazil: Analysis of Clusters, Trends, and Associated Factors (2010–2021). Tropical Medicine and Infectious Disease. 2024; 9(4):82. https://doi.org/10.3390/tropicalmed9040082
Chicago/Turabian StyleAlves, Yan Mathias, Thaís Zamboni Berra, Reginaldo Bazon Vaz Tavares, Marcela Antunes Paschoal Popolin, Fernanda Bruzadelli Paulino da Costa, Sonia Vivian de Jezus, Letícia Perticarrara Ferezin, Ariela Fehr Tártaro, Maria Del Pilar Serrano-Gallardo, Ione Carvalho Pinto, and et al. 2024. "International Migration, Refugees, and Spread of Tuberculosis in Brazil: Analysis of Clusters, Trends, and Associated Factors (2010–2021)" Tropical Medicine and Infectious Disease 9, no. 4: 82. https://doi.org/10.3390/tropicalmed9040082
APA StyleAlves, Y. M., Berra, T. Z., Tavares, R. B. V., Popolin, M. A. P., da Costa, F. B. P., de Jezus, S. V., Ferezin, L. P., Tártaro, A. F., Serrano-Gallardo, M. D. P., Pinto, I. C., Maciel, E. L. N., & Arcêncio, R. A. (2024). International Migration, Refugees, and Spread of Tuberculosis in Brazil: Analysis of Clusters, Trends, and Associated Factors (2010–2021). Tropical Medicine and Infectious Disease, 9(4), 82. https://doi.org/10.3390/tropicalmed9040082