
Optimizing Healthcare Delivery: A Model for Staffing, Patient Assignment, and Resource Allocation



Abstract
:1. Introduction
1.1. Challenges Confronting the Current Healthcare System
1.2. Research Context and Significance
2. Related Work
Healthcare Scheduling and Resource Optimization
3. Model Mathematical Formulation
3.1. Problem Description
3.2. Variables and Parameters
- : Binary decision variable indicating whether staff member i is assigned to time slot t.
- : Binary decision variable indicating whether patient p is assigned to time slot t.
- : Binary decision variable indicating whether resource r is allocated at time slot t.
- : Binary decision variable indicating whether staff member i works overtime.
- : Binary decision variable indicating whether staff member i serves patient p.
- : The weight associated with assigning staff member i to time slot t. This could represent the cost or importance of this assignment.
- : The interaction weight between staff members i and j at time slot t when both are assigned to work. This could reflect the benefit or cost of having these two staff members work together.
- : The cost associated with assigning patient p to time slot t. This could represent the cost of providing service to this patient at this time.
- : The cost associated with allocating resource r at time slot t. This could represent the cost of using this resource at this time.
- : The penalty associated with patient p not receiving service during time slot t. This could reflect the negative impact of not serving this patient at this time.
- : The overtime weight for staff member i when they work overtime. This could represent the extra cost or penalty for having this staff member work beyond their regular hours.
- : The weight associated with patient p not receiving service when staff member i serves them. This could reflect the negative impact of not serving this patient when this staff member is working.
- : The skill level of staff member i required for serving patients during time slot t. This could represent the ability of this staff member to provide service.
- : The demand for staff at time slot t. This could represent the number of staff members needed at this time.
- : The maximum working hours for staff member i. This could represent the maximum number of time slots this staff member can be assigned to.
- : The minimum skill level of staff member i required for serving patient p in task k during time slot t. This could represent the minimum ability needed to provide this service.
- B: The budget constraint. This could represent the maximum total cost of staff assignments and resource allocations.
- : The maximum allowed difference in working hours between staff members i and j. This could represent the maximum disparity in workload between these two staff members.
3.3. Objective Function
Objective Function Terms
- 1
- : This term represents the weight associated with assigning staff member i to time slot t.
- 2
- : This term represents the interaction weight between staff members i and j at time slot t when both are assigned to work.
- 3
- : This term represents the cost associated with assigning patient p to time slot t.
- 4
- : This term represents the cost associated with allocating resource r at time slot t.
- 5
- : This term represents the penalty associated with patient p not receiving service during time slot t.
- 6
- : This term represents the overtime weight for staff member i when they work overtime.
- 7
- : This term represents the weight associated with patient p not receiving service when staff member i serves them.
- 8
- : This term represents the skill level of staff member i required for serving patients during time slot t.
3.4. Constraints
- 1
- Staff Availability: The total number of staff members assigned to each time slot must equal the demand for staff at that time.
- 2
- Maximum Working Hours: The total number of time slots each staff member can be assigned to is limited by their maximum working hours.
- 3
- Patient Scheduling: Each patient is assigned to exactly one time slot.
- 4
- Resource Allocation: Each resource is allocated to exactly one time slot.
- 5
- Skill Level: The skill level of each staff member assigned to serve a patient in a task during a time slot must be at least equal to the minimum skill level required for that task.
- 6
- Overtime: If a staff member works overtime, the sum of their assigned time slots must exceed their maximum working hours.
- 7
- Budget Constraint: The total cost of staff assignments and resource allocations must not exceed the budget constraint.
- 8
- Workload Balance: The difference in working hours between any two staff members must be within the maximum allowed difference.
3.5. Model Algorithm
| Algorithm 1 Healthcare Scheduling Optimization |
|
4. Methodology
4.1. Research Input Data
4.2. Flexibility and Optimization Capabilities of the Proposed Healthcare Scheduling Model
4.3. Use of Simulated Data: Overcoming Challenges in Obtaining Real-World Data
Data Selection for Real-World Healthcare Simulation
- Realistic Assumptions: The chosen values for parameters such as working hours, resource utilization, patient demand, and capacity are aligned with typical healthcare practices, regulations, and operational constraints.
- Expert Consultation: Inputs from healthcare practitioners and administrators play a pivotal role. Moreover, experts have informed the selection of initial values, ensuring that they mirror the complexities and nuances of real-world healthcare delivery.
- Sensitivity Analysis: The model’s responsiveness to variations in the initial values have been tested, confirming that the chosen values provide a robust and representative simulation of real-world scenarios.
4.4. Research Materials and System Configuration
5. Results and Discussions
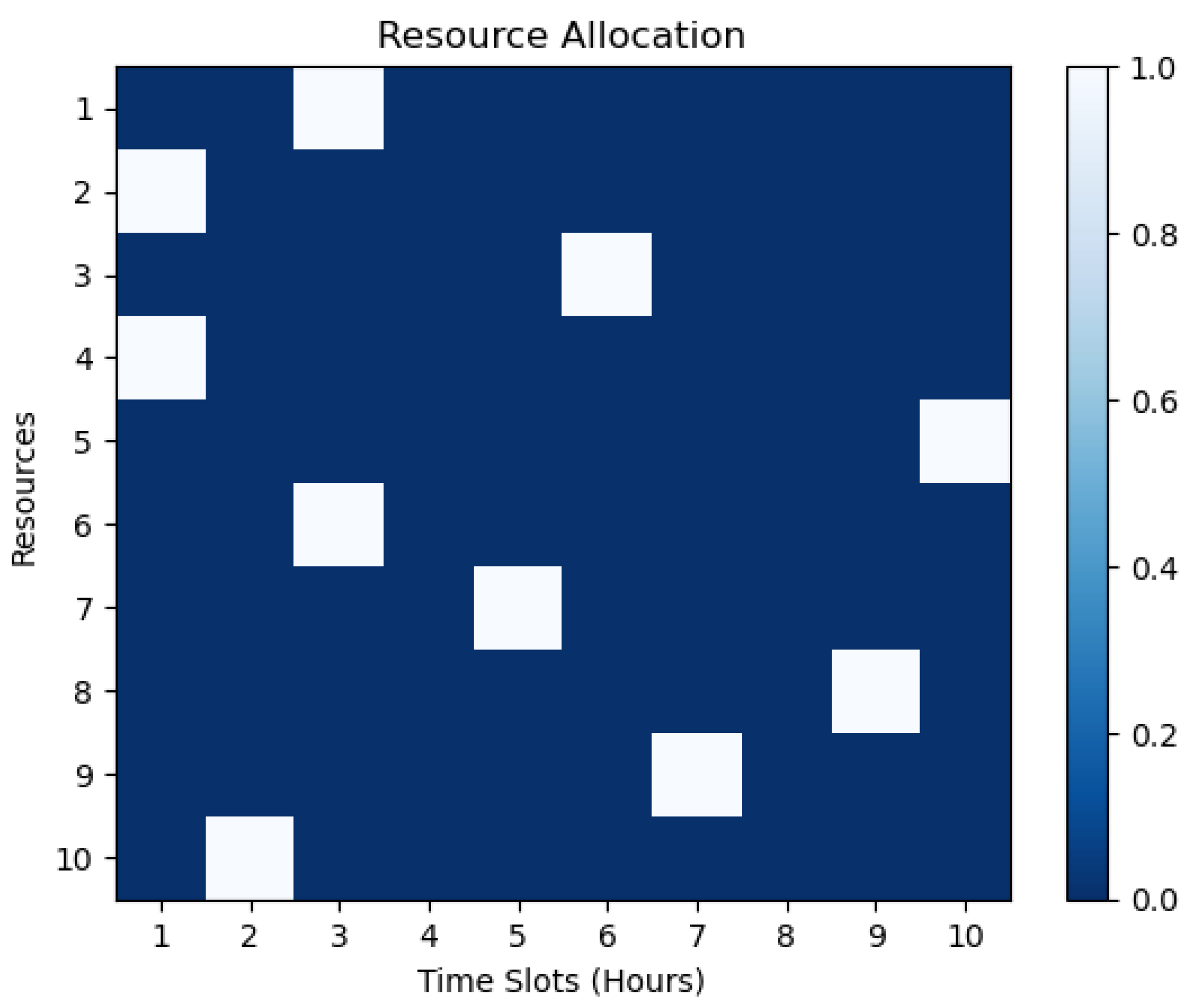
5.1. Resource Allocations
- T is the set of time slots;
- R is the set of resources;
- r is a resource from R;
- t is a time slot from T;
- denotes the allocation of resource r at time slot t.
5.2. Patient Distribution
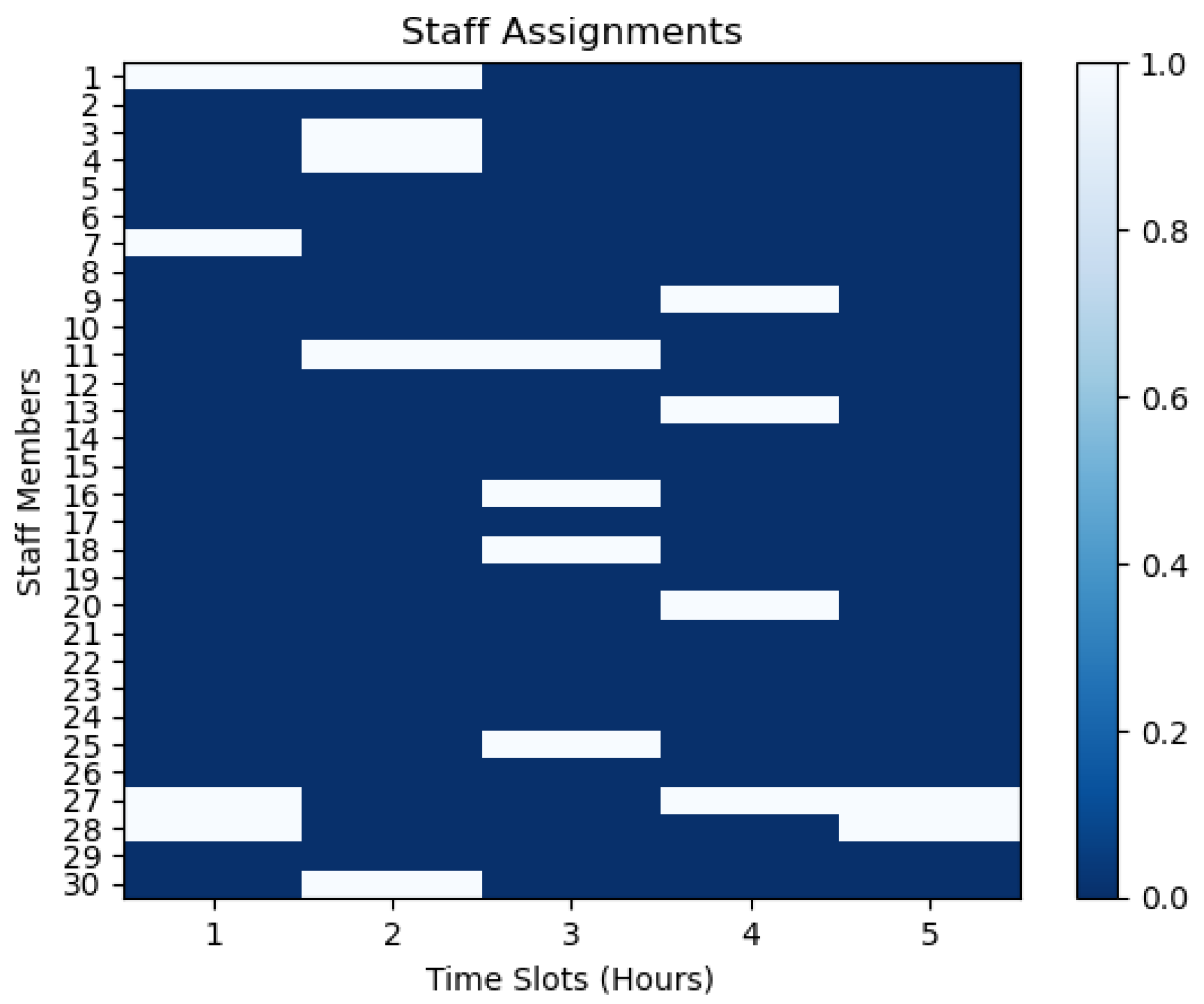
5.3. Staff Assignment
5.4. Patient Assignment
5.5. Actual and Maximum Allowed Working Hours
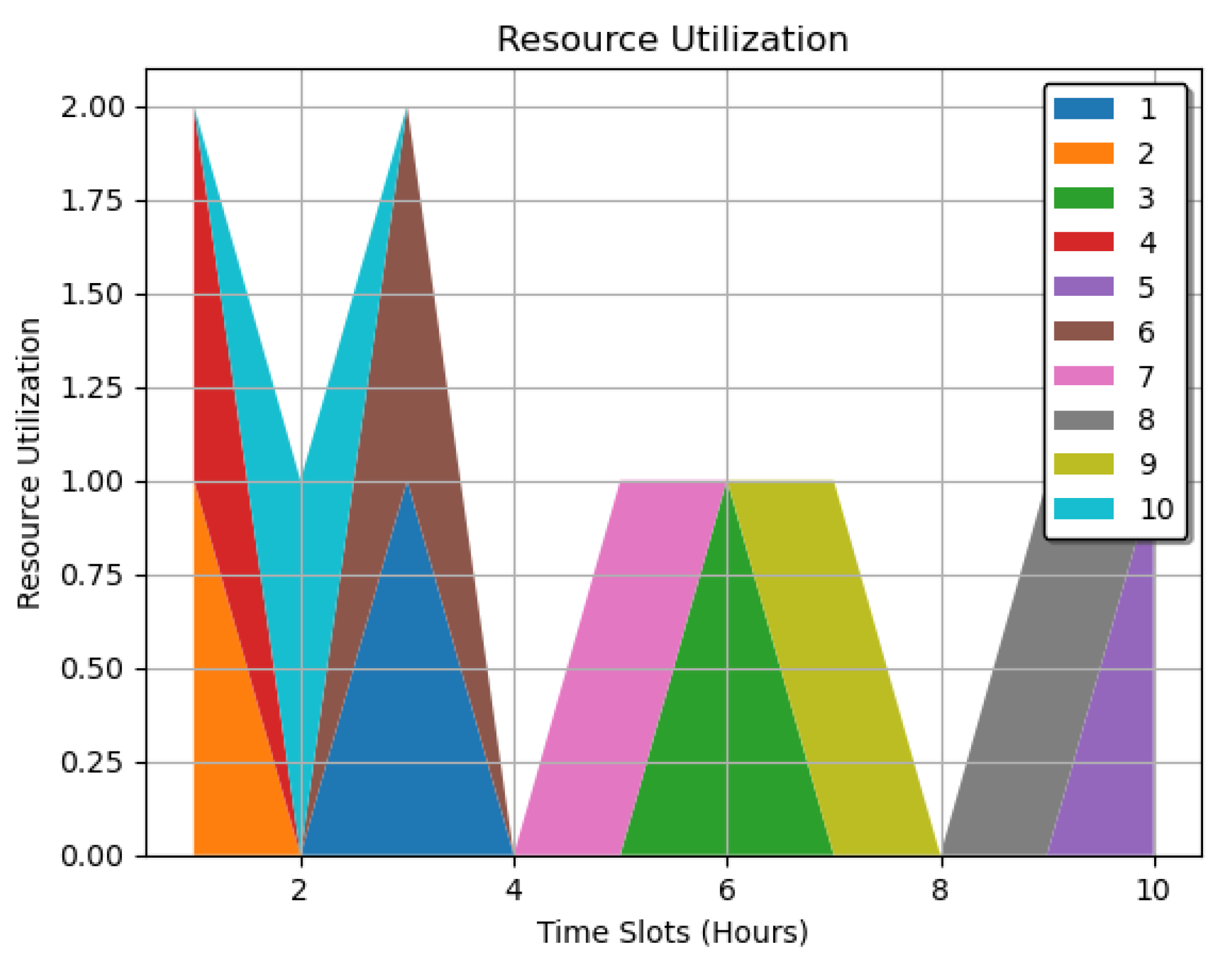
5.6. Resource Utilization
- : A mapping of each resource to its utilization across all time slots.
- R: The set of resources, .
- T: The set of time slots.
- r: A specific resource from the set R.
- t: A specific time slot from the set T.
- : The utilization of resource r at time slot t, representing how much of that resource is being used or allocated at that specific time.
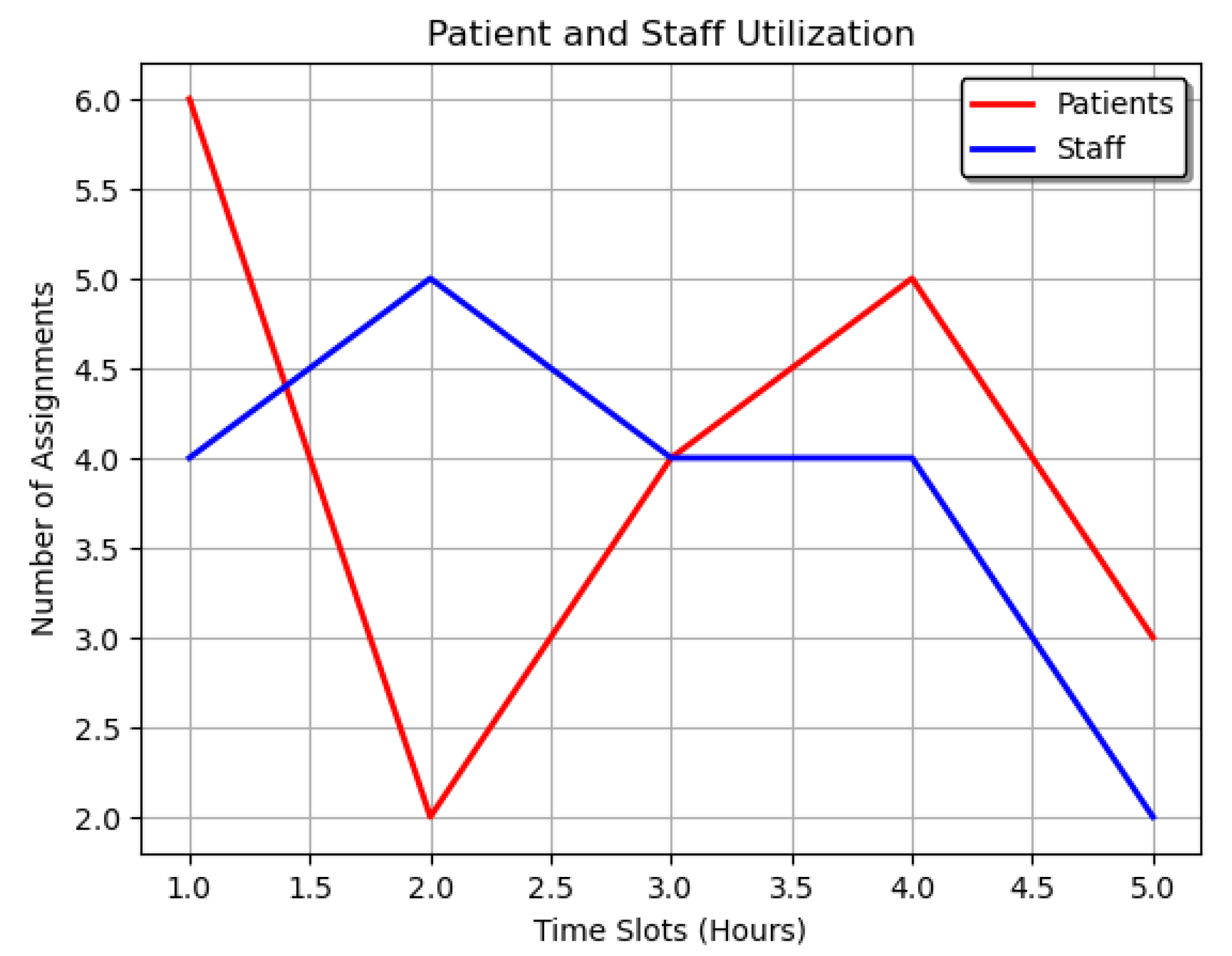
5.7. Patient and Staff Utilization
- : Total number of assignments for all patients at each time slot.
- p: A specific patient within the set P.
- P: Refers to the collection of all patients.
- t: A specific time interval or slot within the set T.
- : Number of assignments for a particular patient at a given time slot.
- T: The collection of all time intervals or slots considered.
- : Total number of assignments for all staff members at each time slot.
- i: A specific staff member within the set N.
- t: A specific time interval or slot within the set T.
- : Number of assignments for a particular staff member at a given time slot.
- N: The collection of all staff members.
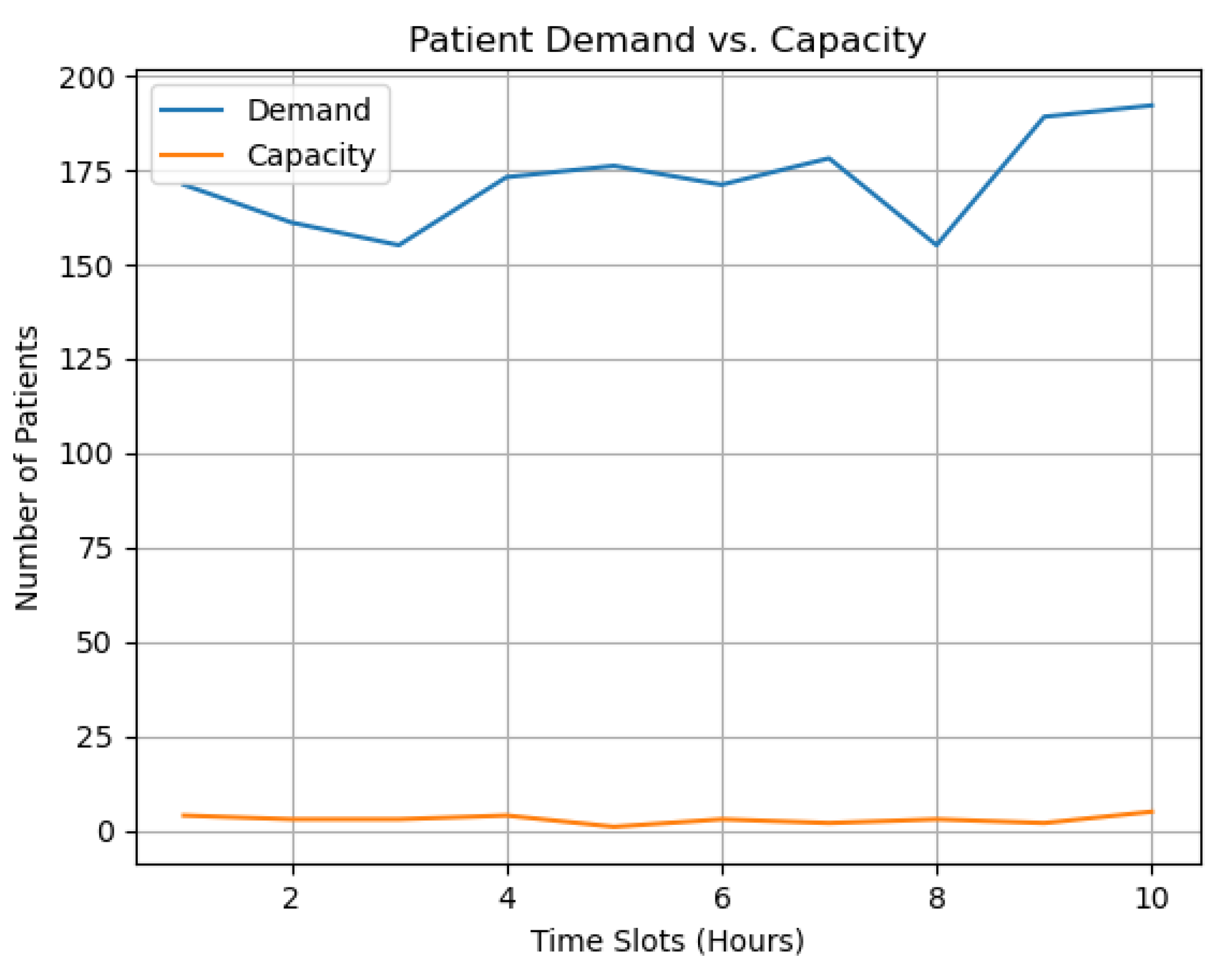
5.8. Demand and Capacity Analysis in Scheduling
- Period’s Total Demand and Capacity: This refers to the overall demand and capacity for a specific period. It is calculated for scheduling patients based on available resources and demands.
- Patients P: This represents the set of all patients considered in the scheduling.
- Set of Periods T: This refers to the specific periods for which demand and capacity are calculated and scheduled.
- Demand at Time t, demandt: This is the total demand at a specific time t, calculated as the sum of the demand for all patients at that time. The demand for each patient p at time t is represented by .
- Capacity at Time t, capacityt: This is the total capacity at time t, calculated as the sum of a capacity-related variable for all patients at that time. The capacity-related variable for each patient p at time t is represented by .
- : This corresponds to the demand for a specific patient p at time t. It represents the patient’s required resources, treatment, or service.
- : This represents the value of a capacity-related variable for a specific patient p at time t. It may signify how much of a certain resource is allocated or available for that patient, possibly weighted by some variable x.
- (For All t in T): This notation signifies that the given equations for demand and capacity are applicable for all periods t in the set of periods T.
5.9. Patient Satisfaction
- Patient Satisfaction at Time t: satisfaction_t: This is the target variable representing the satisfaction level of patients at time t.
- Summation Over Patients and Staff: : This summation indicates that the calculation is done over all patients p in a set P and all staff members i in a set N.
- Conditional Part: : This condition implies that the summation is calculated only when the product of the capacity-related variable and some variable x is more significant than 0.5. This could be a threshold for considering only specific assignments or capacities.
- Utility of Patient p: : This represents the utility or benefit of a specific patient p, which may be based on their needs or preferences.
- Assignment Variable: : This term denotes the assignment of patient p to staff member i, possibly weighted by variable x. It might represent how well the staff member fits the patient’s needs.
- Denominator Summation: : This part sums up the capacity-related variable for all patients p in set P at time t. It likely represents the total capacity or availability at time t and is the normalizing factor for patient satisfaction.
- Main Equation: Putting all the parts together, the equation calculates patient satisfaction at time t as a weighted sum of utilities and assignments normalized by the total capacity-related variable.
6. Conclusions
7. Future Research Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MILP | Mixed-Integer Linear Programming |
| LP | Linear Programming |
References
- Hughes, R.G. Tools and strategies for quality improvement and patient safety. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008. [Google Scholar]
- Yen, P.Y.; Kellye, M.; Lopetegui, M.; Saha, A.; Loversidge, J.; Chipps, E.M.; Gallagher-Ford, L.; Buck, J. Nurses’ time allocation and multitasking of nursing activities: A time motion study. In AMIA Annual Symposium Proceedings; American Medical Informatics Association: Bethesda, MD, USA, 2018; Volume 2018, p. 1137. [Google Scholar]
- Dugdale, D.C.; Epstein, R.; Pantilat, S.Z. Time and the patient-physician relationship. J. Gen. Intern. Med. 1999, 14, S34. [Google Scholar] [CrossRef] [PubMed]
- Mosadeghrad, A.M. Factors influencing healthcare service quality. Int. J. Health Policy Manag. 2014, 3, 77. [Google Scholar] [CrossRef] [PubMed]
- How to Ease the Nursing Shortage in America. Available online: https://www.americanprogress.org/article/how-to-ease-the-nursing-shortage-in-america/ (accessed on 24 August 2023).
- Haleem, A.; Javaid, M.; Singh, R.P.; Suman, R. Telemedicine for healthcare: Capabilities, features, barriers, and applications. Sens. Int. 2021, 2, 100117. [Google Scholar] [CrossRef] [PubMed]
- Holmér, S.; Nedlund, A.C.; Thomas, K.; Krevers, B. How health care professionals handle limited resources in primary care–an interview study. BMC Health Serv. Res. 2023, 23, 1–12. [Google Scholar] [CrossRef]
- Rahardja, U.; Andriyani, F.; Triyono, T. Model Scheduling Optimization Workforce Management Marketing. APTISI Trans. Manag. (ATM) 2020, 4, 92–100. [Google Scholar] [CrossRef]
- Moussavi, S.E.; Mahdjoub, M.; Grunder, O. A matheuristic approach to the integration of worker assignment and vehicle routing problems: Application to home healthcare scheduling. Expert Syst. Appl. 2019, 125, 317–332. [Google Scholar] [CrossRef]
- Afshar-Nadjafi, B. Multi-skilling in scheduling problems: A review on models, methods and applications. Comput. Ind. Eng. 2021, 151, 107004. [Google Scholar] [CrossRef]
- Abdalkareem, Z.A.; Amir, A.; Al-Betar, M.A.; Ekhan, P.; Hammouri, A.I. Healthcare scheduling in optimization context: A review. Health Technol. 2021, 11, 445–469. [Google Scholar] [CrossRef]
- García-Nieves, J.D.; Ponz-Tienda, J.L.; Ospina-Alvarado, A.; Bonilla-Palacios, M. Multipurpose linear programming optimization model for repetitive activities scheduling in construction projects. Autom. Constr. 2019, 105, 102799. [Google Scholar] [CrossRef]
- Ghannam, L. Development of a Mathematical Model for Optimal Scheduling of Patients and Resource Management in Healthcare in Palestine during the Pandemic. Ph.D. Thesis, An-Najah National University, Nablus, Palestine, 2022. [Google Scholar]
- Ala, A.; Goli, A.; Nejad Attari, M.Y. Scheduling and routing of dispatching medical staff to homes healthcare from different medical centers with considering fairness policy. Math. Probl. Eng. 2022, 2022, 3189574. [Google Scholar] [CrossRef]
- Guastalla, A.; Sulis, E.; Aringhieri, R.; Branchi, S.; Di Francescomarino, C.; Ghidini, C. Workshift scheduling using optimization and process mining techniques: An application in healthcare. In Proceedings of the 2022 Winter Simulation Conference (WSC), Singapore, 11–14 December 2022; IEEE: Piscataway, NJ, USA, 2022; pp. 1116–1127. [Google Scholar]
- Maghzi, P.; Roohnavazfar, M.; Mohammadi, M.; Naderi, B. A Mathematical Model for Operating Room Scheduling Considering Limitations on Human Resources Access and Patient Prioritization. J. Qual. Eng. Prod. Optim. 2019, 4, 67–82. [Google Scholar]
- Mielczarek, B. Review of modelling approaches for healthcare simulation. Oper. Res. Decis. 2016, 26. [Google Scholar]
- Yinusa, A.; Faezipour, M.; Faezipour, M. A Study on CKD Progression and Health Disparities Using System Dynamics Modeling. Healthcare 2022, 10, 1628. [Google Scholar] [CrossRef] [PubMed]
- Maenhout, B.; Vanhoucke, M. An integrated nurse staffing and scheduling analysis for longer-term nursing staff allocation problems. Omega 2013, 41, 485–499. [Google Scholar] [CrossRef]
- Restrepo, M.I.; Rousseau, L.M.; Vallée, J. Home healthcare integrated staffing and scheduling. Omega 2020, 95, 102057. [Google Scholar] [CrossRef]
- Granja, C.; Almada-Lobo, B.; Janela, F.; Seabra, J.; Mendes, A. An optimization based on simulation approach to the patient admission scheduling problem using a linear programing algorithm. J. Biomed. Inform. 2014, 52, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Ala, A.; Alsaadi, F.E.; Ahmadi, M.; Mirjalili, S. Optimization of an appointment scheduling problem for healthcare systems based on the quality of fairness service using whale optimization algorithm and NSGA-II. Sci. Rep. 2021, 11, 19816. [Google Scholar] [CrossRef]
- Bennett, A.R.; Erera, A.L. Dynamic periodic fixed appointment scheduling for home health. IIE Trans. Healthc. Syst. Eng. 2011, 1, 6–19. [Google Scholar] [CrossRef]
- Leksakul, K.; Phetsawat, S. Nurse scheduling using genetic algorithm. Math. Probl. Eng. 2014, 2014. [Google Scholar] [CrossRef]
- Turhan, A.M.; Bilgen, B. Mixed integer programming based heuristics for the patient admission scheduling problem. Comput. Oper. Res. 2017, 80, 38–49. [Google Scholar] [CrossRef]
- Bolaji, A.L.; Bamigbola, A.F.; Adewole, L.B.; Shola, P.B.; Afolorunso, A.; Obayomi, A.A.; Aremu, D.R.; Almazroi, A.A.A. A room-oriented artificial bee colony algorithm for optimizing the patient admission scheduling problem. Comput. Biol. Med. 2022, 148, 105850. [Google Scholar] [CrossRef] [PubMed]
- Bastos, L.S.; Marchesi, J.F.; Hamacher, S.; Fleck, J.L. A mixed integer programming approach to the patient admission scheduling problem. Eur. J. Oper. Res. 2019, 273, 831–840. [Google Scholar] [CrossRef]
- Gocgun, Y.; Bresnahan, B.W.; Ghate, A.; Gunn, M.L. A Markov decision process approach to multi-category patient scheduling in a diagnostic facility. Artif. Intell. Med. 2011, 53, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Li, X.; Gao, L. A discrete artificial bee colony algorithm for the distributed heterogeneous no-wait flowshop scheduling problem. Appl. Soft Comput. 2021, 100, 106946. [Google Scholar] [CrossRef]
- Gurobi Optimization. Available online: https://www.gurobi.com (accessed on 24 August 2023).



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| CPU model | Intel® Core™ i5-6200U CPU @ 2.30GHz |
| Instruction set | [SSE2|AVX|AVX2] |
| Thread count | 2 physical cores, 4 logical processors, using up to 4 threads |
| First Output | Second Output | ||
|---|---|---|---|
| Term | Value | Term | Value |
| Objective value | 844.0 | Objective value | 539.0 |
| Solution count | 5 | Solution count | 3 |
| Best objective | 844.0 | Best objective | 539.0 |
| Best bound | 844.0 | Best bound | 539.0 |
| Gap | 0.0% | Gap | 0.0% |
| Term | First Output | Second Output | Description |
|---|---|---|---|
| Objective Value | 844.0 | 539.0 | Optimized value of the objective function. Represents key measures like total cost or profit. |
| Solution Count | 5 | 3 | Number of feasible solutions satisfying all constraints. |
| Best Objective, Bound | 844.0 | 539.0 | Best value and lowest value found for the function during optimization. |
| Gap | 0.0% | 0.0% | Difference between best bound and best objective. |
| Staff Assignments | 20 | 30 | Allocation of staff members to specific time slots for effective scheduling. |
| Patient Assignments | 30 | 20 | Allocation of patients to specific time slots for ensuring timely care. |
| Resource Allocations | 10 | 15 | Allocation of resources to specific time slots for effective resource management. |
| Staff Overtime Hours | 10 | 7 | Extra hours required by staff beyond regular hours for monitoring workload distribution. |
| First Output | Second Output | ||
|---|---|---|---|
| Staff Member | Time Slot | Staff Member | Time Slot |
| 1 | 1, 8 | 1 | 4 |
| 2 | 5, 6 | 3 | 5 |
| 4 | 1, 4, 10 | 4 | 5 |
| 6 | 3, 10 | 7 | 1 |
| 7 | 3 | 9 | 5 |
| 8 | 6, 8 | 10 | 3 |
| 11 | 5, 6, 8 | 16 | 2 |
| 13 | 2, 7 | 18 | 1, 2 |
| 15 | 2, 3, 5 | 20 | 1, 2, 3, 4 |
| 16 | 5, 8, 9 | 25 | 4, 5 |
| 17 | 8 | 26 | 3 |
| 18 | 2, 7 | 27 | 4, 5 |
| 19 | 1, 2, 5, 9 | 29 | 2 |
| 20 | 3, 4, 6, 7, 9 | ||
| First Output | Second Output | ||
|---|---|---|---|
| Patient | Time Slot | Patient | Time Slot |
| 1 | 3 | 1, 2, 3 | 2 |
| 2 | 1 | 4 | 3 |
| 3 | 7 | 5 | 1 |
| 4 | 4 | 6 | 5 |
| 5 | 10 | 7, 11, 12 | 2 |
| 6 | 10 | 8 | 4 |
| 7 | 10 | 9 | 5 |
| 8 | 1 | 10, 13 | 3 |
| 9 | 2 | 14, 16, 18 | 4 |
| 10 | 7 | 15 | 5 |
| 11 | 6 | 17, 20 | 1 |
| 12 | 5 | 19 | 4 |
| 13 | 8 | - | - |
| 14 | 4 | - | - |
| 15 | 2 | - | - |
| 16 | 8 | - | - |
| 17 | 10 | - | - |
| 18 | 10 | - | - |
| 19 | 1 | - | - |
| 20 | 9 | - | - |
| 21 | 4 | - | - |
| 22 | 2 | - | - |
| 23 | 4 | - | - |
| 24 | 6 | - | - |
| 25 | 3 | - | - |
| 26 | 1 | - | - |
| 27 | 9 | - | - |
| 28 | 8 | - | - |
| 29 | 3 | - | - |
| 30 | 6 | - | - |
| First Output | Second Output | ||
|---|---|---|---|
| Resource | Time Slot | Resource | Time Slot |
| 1 | 3 | 1 | 3 |
| 2 | 1 | 2, 3, 6 | 1 |
| 3 | 6 | 4, 7 | 2 |
| 4 | 1 | 5 | 5 |
| 5 | 10 | 8 | 1 |
| 6 | 3 | 9 | 4 |
| 7 | 5 | 10 | 3 |
| 8 | 9 | 11 | 4 |
| 9 | 7 | 12, 13, 15 | 1 |
| 10 | 2 | 14 | 4 |
| First Output | Second Output | ||
|---|---|---|---|
| Staff Member | Overtime Hours | Staff Member | Overtime Hours |
| 1 | 0 | 1–30 | 0 |
| 2 | 1 | 20 | 7 |
| 3 | 0 | - | - |
| 4 | 0 | - | - |
| 5 | 0 | - | - |
| 6 | 0 | - | - |
| 7 | 0 | - | - |
| 8 | 1 | - | - |
| 9 | 0 | - | - |
| 10 | 0 | - | - |
| 11 | 5 | - | - |
| 12 | 0 | - | - |
| 13 | 0 | - | - |
| 14 | 0 | - | - |
| 15 | 0 | - | - |
| 16 | 3 | - | - |
| 17 | 0 | - | - |
| 18 | 0 | - | - |
| 19 | 0 | - | - |
| 20 | 0 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yinusa, A.; Faezipour, M. Optimizing Healthcare Delivery: A Model for Staffing, Patient Assignment, and Resource Allocation. Appl. Syst. Innov. 2023, 6, 78. https://doi.org/10.3390/asi6050078
Yinusa A, Faezipour M. Optimizing Healthcare Delivery: A Model for Staffing, Patient Assignment, and Resource Allocation. Applied System Innovation. 2023; 6(5):78. https://doi.org/10.3390/asi6050078
Chicago/Turabian StyleYinusa, Ahmeed, and Misagh Faezipour. 2023. "Optimizing Healthcare Delivery: A Model for Staffing, Patient Assignment, and Resource Allocation" Applied System Innovation 6, no. 5: 78. https://doi.org/10.3390/asi6050078
APA StyleYinusa, A., & Faezipour, M. (2023). Optimizing Healthcare Delivery: A Model for Staffing, Patient Assignment, and Resource Allocation. Applied System Innovation, 6(5), 78. https://doi.org/10.3390/asi6050078