1. Introduction
Thyroid ultrasonography has become a routine tool for the endocrinologist in the diagnosis and management of thyroid and parathyroid disorders [
1,
2]. However, it is now clear that the thyroid specialist (“thyroidologist”) with a portable ultrasound machine is in the best position to correlate the features of thyroid nodules and other thyroid disorders with the clinical findings and blood test results. In addition, the thyroid specialist can provide “one stop shopping” for their patients as they also perform their own fine needle aspiration biopsies (FNAB) of suspicious nodules.
In this review we describe the ultrasound features of the common types of thyroid disorders, how to correctly interpret what is seen, when to repeat the imaging and when to carry out FNAB of suspicious nodules. We will describe some newly recognised features of thyroid sonograms and briefly discuss the sonographic appearances of parathyroid adenomas, the usual cause of primary hyperparathyroidism. The purpose of the review is to provide an understanding of the utility of real time thyroid, parathyroid and neck ultrasound for the aspiring thyroid specialist, its scope in the office and how can it help in the patient’s management. All figures are derived from one of the authors’ (JW) own patients and were obtained using his M-Tubo Sonosite portable ultrasound machine and a 5 MHZ small parts transducer.
2. The Normal Thyroid Gland
Critical to being able to recognize ultrasonographic abnormalities in patients with thyroid disorders, it is necessary to fully understand the sonographic characteristics of the normal thyroid gland, an example of which is shown in
Figure 1. The overall size of the thyroid gland is determined by measuring its width, depth and length, from which the volume of each lobe can be calculated. With experience, the user can develop their own reference ranges for adult males and adult females, and for pregnancy (the volume of the thyroid gland increases by approx. 30% during pregnancy). While there is a big variation in the size of the normal gland which reflects both genetic and environmental factors, such as local iodine availability and the effect of pregnancy, each lobe of the normal gland measures approx. 50 × 30 × 10 mm with a thin isthmus connecting the two lobes [
3]. Some euthyroid subjects have an enlarged gland that otherwise looks normal, reflecting either a normal variation, rare abnormalities of thyroid hormone metabolism or iodine deficiency goitre, which is presumed to be rare in Australia. An extra small lobe arising from the top of the left lobe, called the pyramidal lobe, is present in approximately 20% of people. This can be misdiagnosed as a nodule and even biopsied. The overall shape of the normal thyroid also varies, and some subjects have one or two thin and elongated lobes that extend laterally into the neck. Finally, a transverse view of the oesophagus can often be seen to the medial side of the left lobe, that to the uninitiated could also be mistaken for a nodule.
The texture of the normal thyroid texture, or echogenicity, as determined using the ultrasound grey scale, is described as isogenous or isoechoic. Features of an abnormal gland, such as cysts or nodules, that are less white than normal, ranging from grey through to black, are described as being variably hypoechoic. Some nodules and areas of inflammation that are whiter than normal are described as being hyperechoic. Thyroid cysts, which are fluid-containing sacs, and the “black holes” of end stage Hashimoto thyroiditis, are uniformly black. Benign colloid nodules are usually isoechoic or slightly hypoechoic, whilst more cellular follicular nodules may be slightly hyperechoic. The ability to recognize variations in the echogenicity of the thyroid gland itself and nodules, cysts or infiltrations within the gland can only be obtained by extensive, long term experience, even surpassing that of the general radiologist.
Another feature of the thyroid gland to be assessed is its vascularity. The normal vascularity of the thyroid reflects the distribution of the thyroid arteries and veins, which will vary from subject to subject and include several anatomical variations, all of which are “normal”, and the overall blood flow into and out of the gland.
In Graves’ hyperthyroidism, the overall blood supply is greatly increased due to the diffuse and intense inflammatory reaction, whereas in Hashimoto thyroiditis, the blood supply to the thyroid is initially increased when the inflammatory reaction is active, then decreases as the gland is progressively destroyed over time and replaced by fibrosis and scarring. Abnormalities of the blood supply in the various thyroid disorders will be discussed in more detail below.
3. Nodules
Thyroid nodules are very common, increasing to a prevalence of about 60% in adult women aged 60 or more. Most benign nodules are “colloid” according to the dominant presence of fluid and few cells (low cell:fluid ratio), i.e., the nodule comprises scattered normal thyroid follicular cells within a background of thick, viscous fluid [
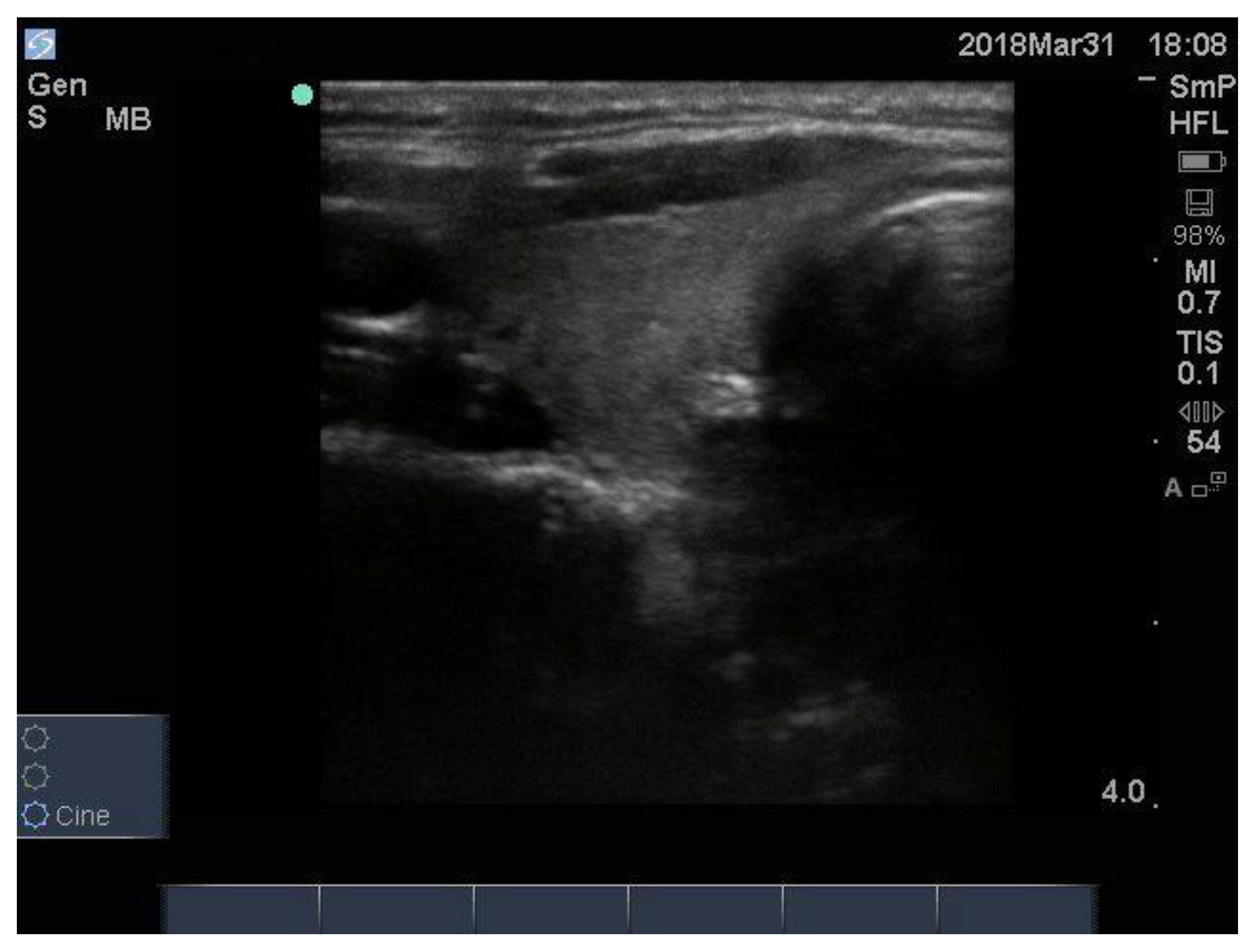
4]. Although the prevalence of cancer is about 8% in patients with one or more nodules, the risk of cancer is greater in patients with a single nodule since multi nodular, or colloid, goitre is a benign disease and all of the nodules are expected to be the same, differing only in size. A micro cancer incidentally found in a multi nodular can be considered to be an incidentaloma that would not have harmed the patient if left alone. An example of a benign colloid nodule with a sharp edge, halo (a black ring thought to represent compressed blood vessels) and isogenic texture, which is <3 cm and wider than tall, is shown in
Figure 2.
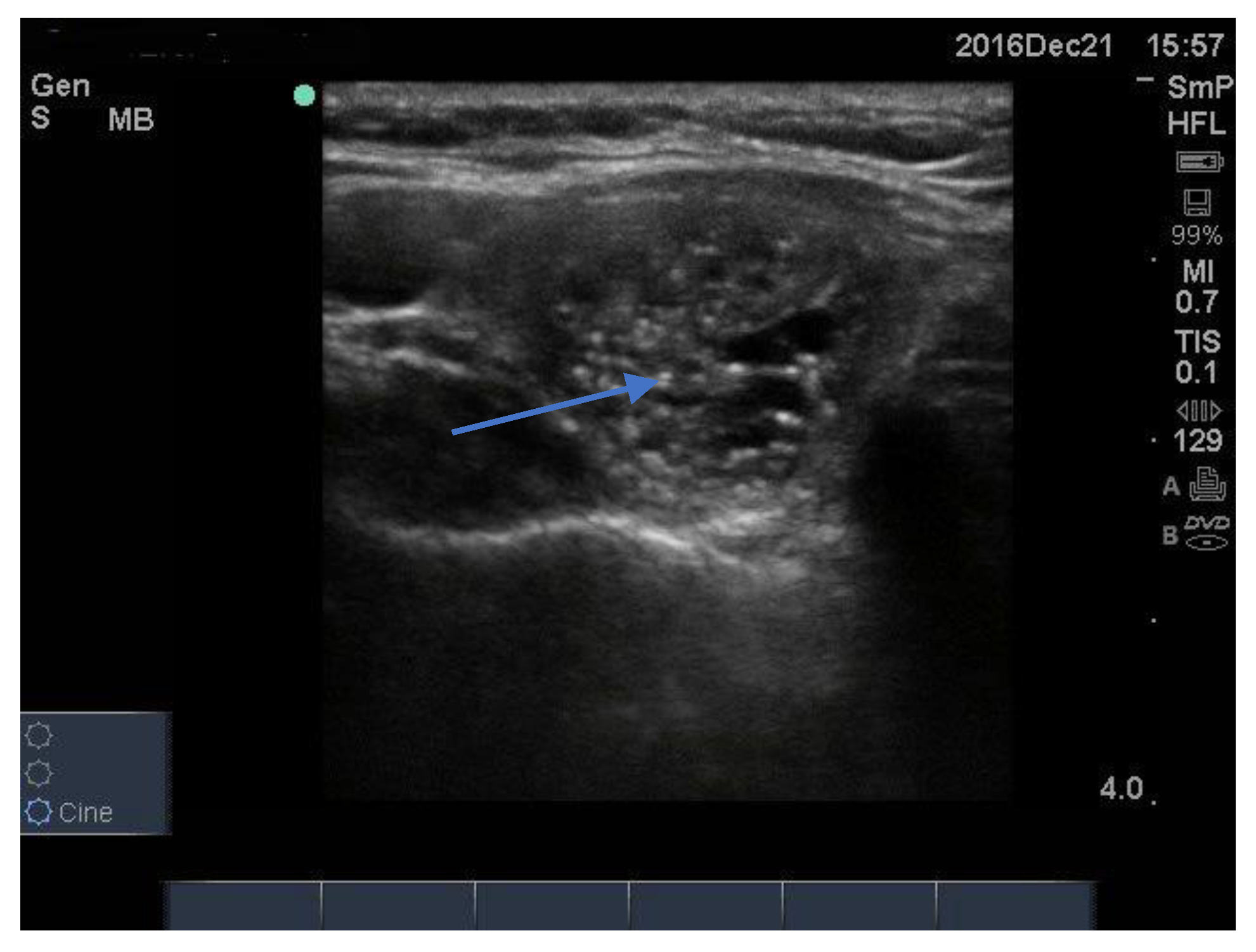
Some intra nodular “microcalcifications” are actually colloid, which may be lined up like a comet tail or dispersed around the inner edge of the nodule (
Figure 3). Others, brighter and sharper, are probably colloid crystals. In many nodules there is a single bright spot, often at one side of the nodule, like a nucleus of a cell, that might be the source of the colloid fluid, that could be called a “colloidoma”. Although radiologists describe these as “microcalcifications”—implying suspicion for papillary thyroid cancer—this is probably not correct as, in the authors’ experience, they are quite different from the microcalcifications of papillary thyroid cancer. Finally, some of these colloid bright spots may represent what has been called “the ring down resonance artifact”. Overall, our experience suggests that colloid bright spots are mislabelled as microcalcifications in approximately 30% of cases.
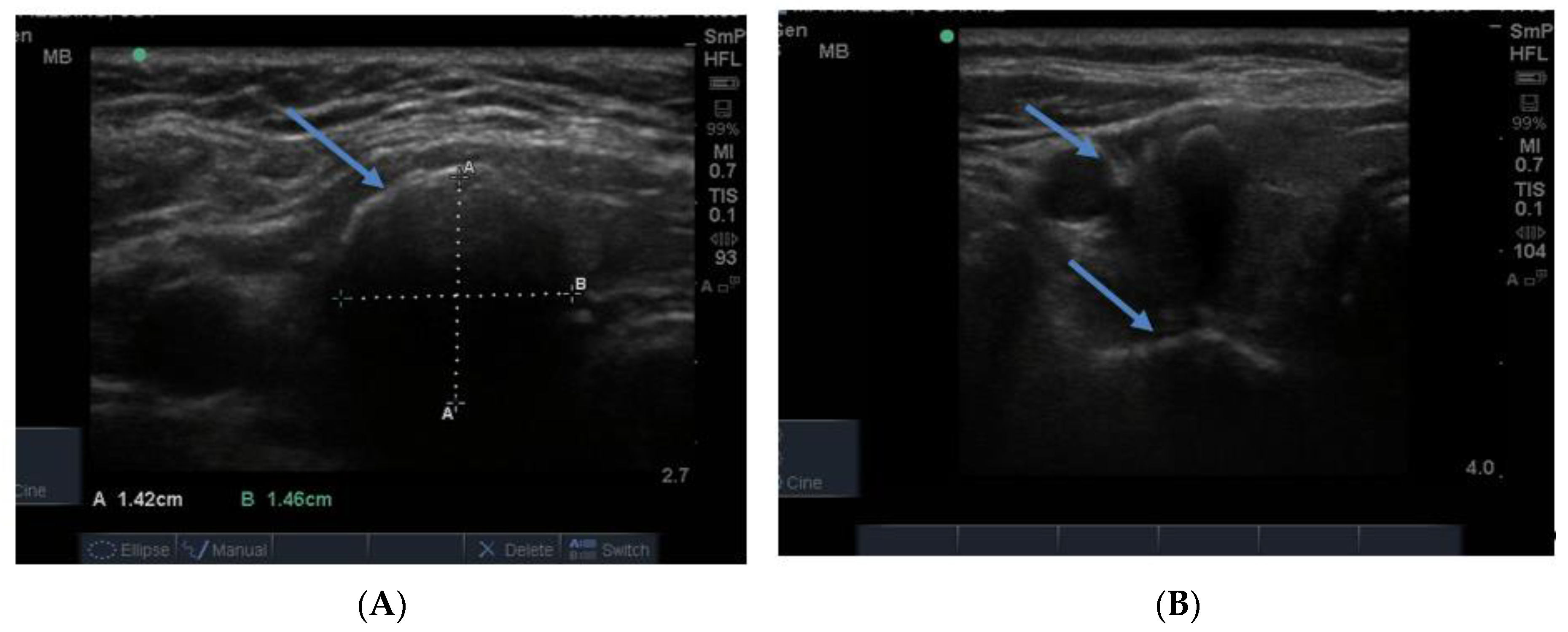
4. Follicular Nodules
Follicular nodules are much less common than colloid nodules with a different appearance on ultrasound; they are more cellular, giving a solid appearance, with a whitish colour, i.e., less hypoechoic. They too have a sharp edge and halo and grow slowly over time [
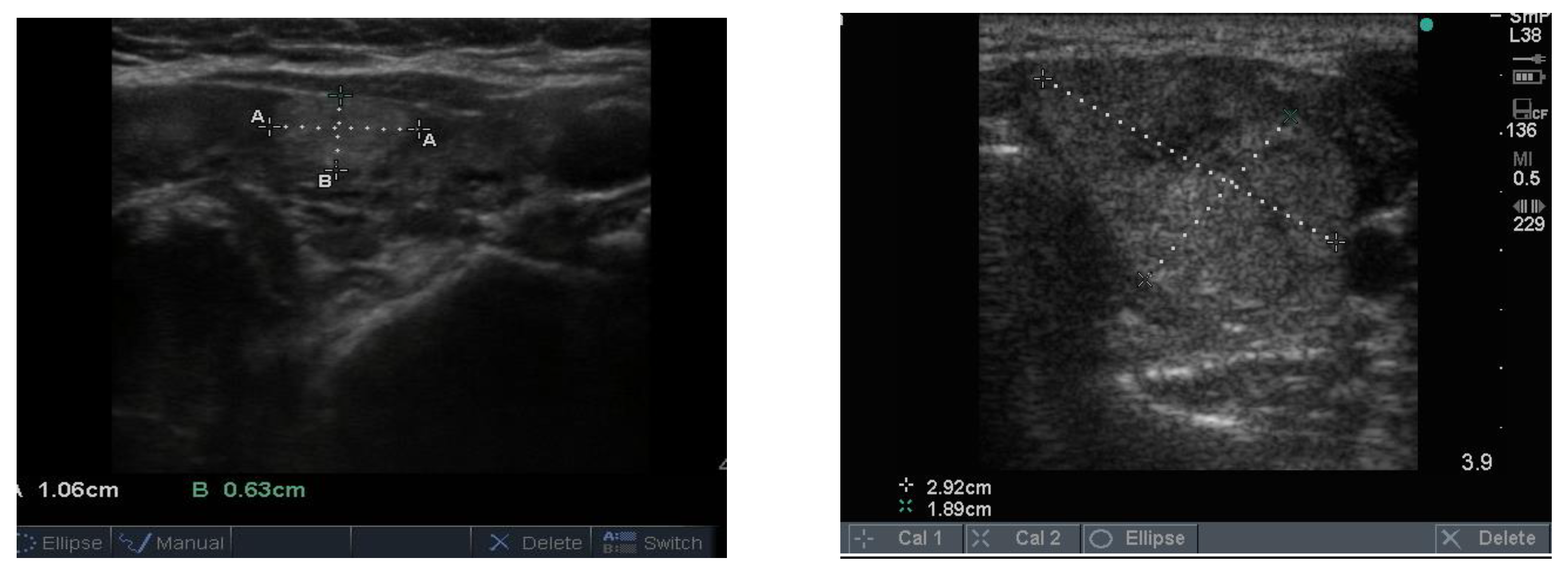
5]. The problem with these lesions is that FNAB is unable to differentiate between a benign follicular adenoma and follicular cancer, and if the latter is suspected, thyroid surgery is the final arbitrator. About 10% of benign thyroid nodules are follicular, and most of them end up being removed. Two examples of follicular nodules that were finally proven to be benign are shown in
Figure 4. On follow-up ultrasound (US), 6–12 months later, repeat biopsy might be indicated if a nodule has grown by 20% or more in two or more dimensions; benign nodules also grow, but less quickly.
5. Hot Nodules
Nodules shown to be “hot” or “toxic” on technetium scan are “never” cancerous as they are at least partially differentiated, in other words, producing thyroid hormones. It is however sometimes appropriate to carry out FNAB in order to reassure the patient and confirm the benign nature of the nodule. On occasion, hot nodules may contain fluid on biopsy, but on needling the nodule, a cellular specimen is obtained, as in the case of the example shown in
Figure 5. The appearance of toxic nodules varies, but they are usually similar to the colloid nodules. Occasionally they are markedly hypoechoic, or cystic, as in this case.
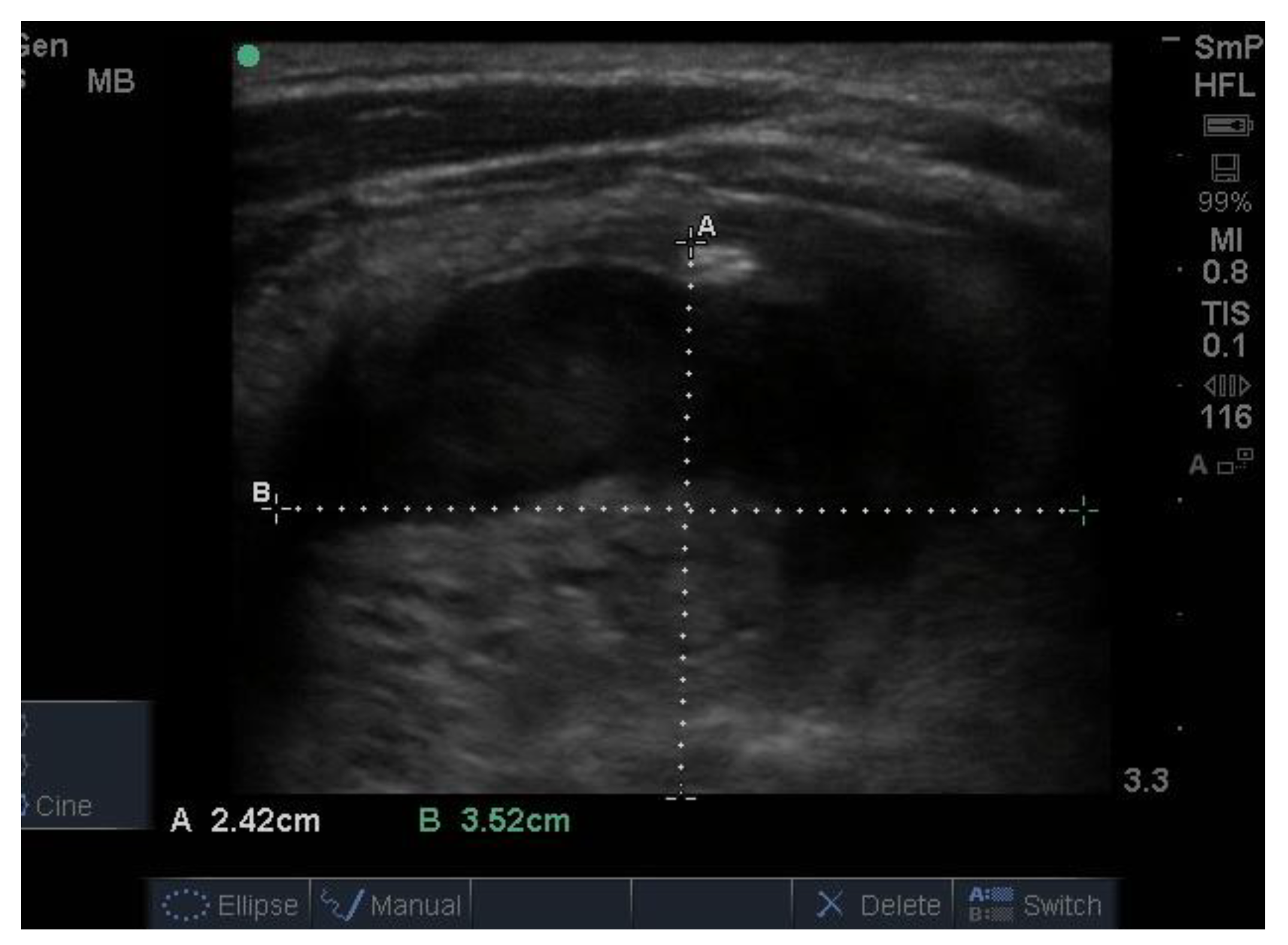
6. Thyroid Cysts
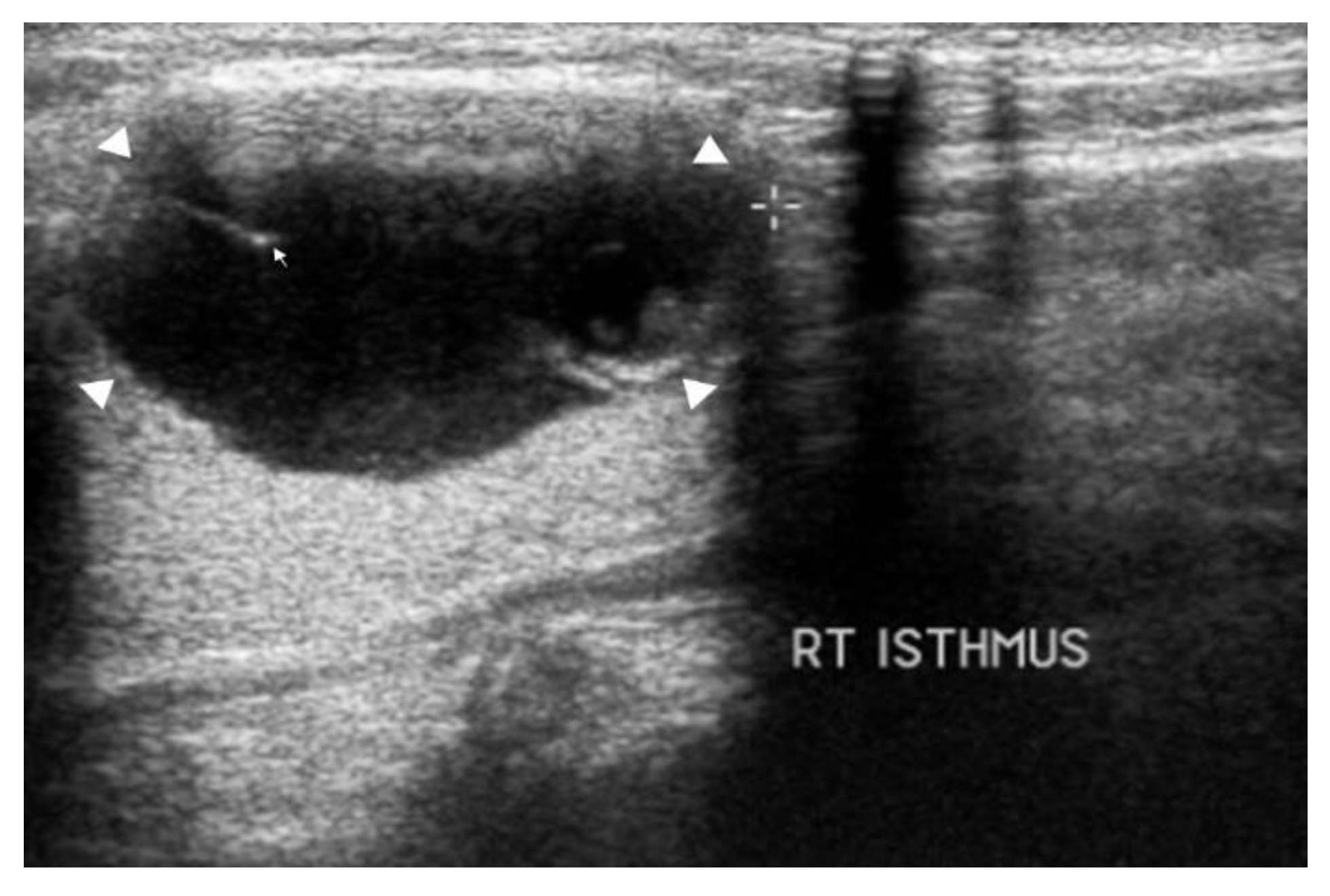
Thyroid cysts are important because it may be possible to relieve the patient’s neck symptoms by removing the fluid. However, a cyst tends to refill, which can be a sign that it has a solid component which, in about 10% of cases, is cancerous [
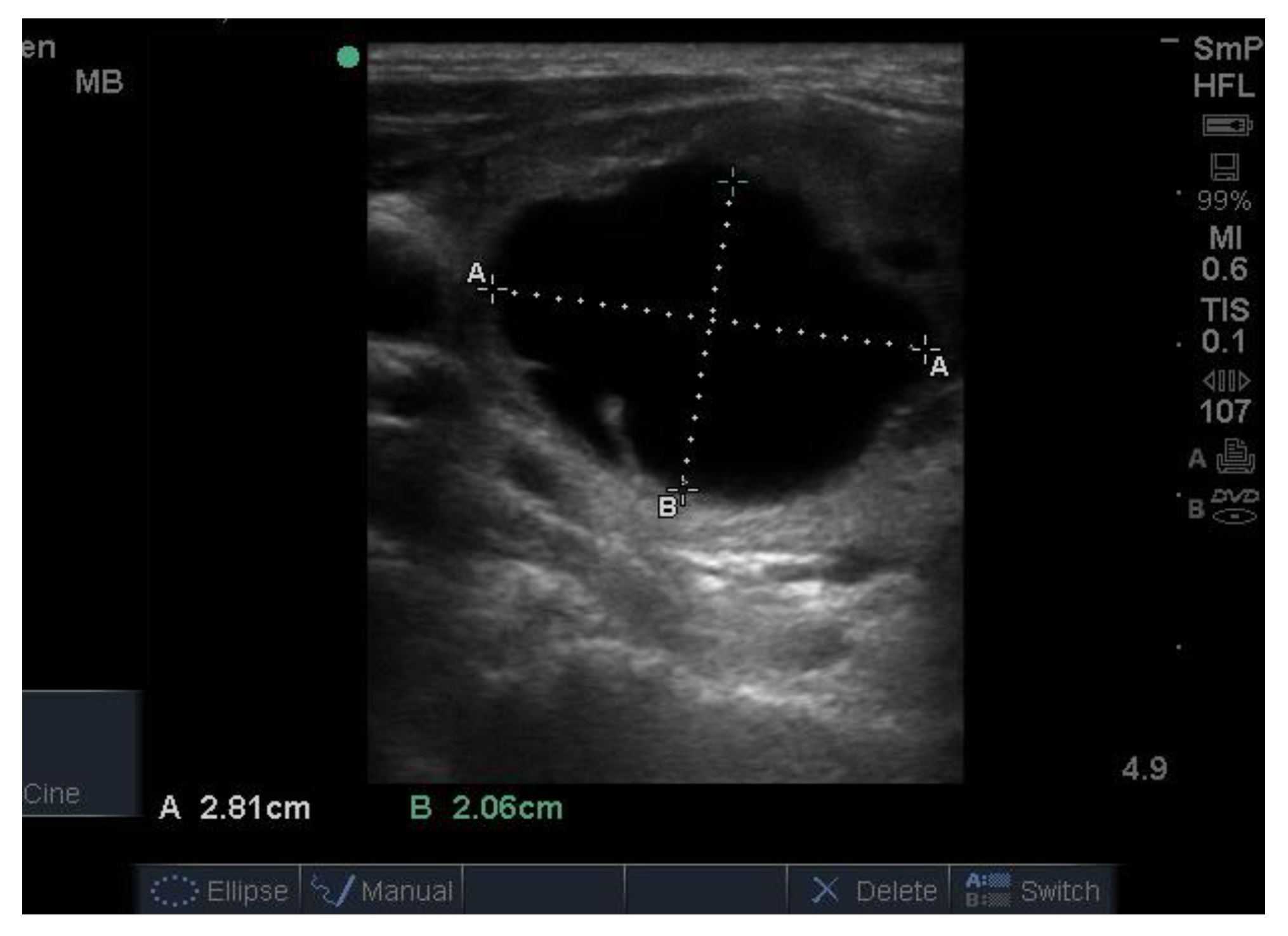
6]. Sometimes it is difficult to differentiate a cyst from a hyperechoic colloid or “toxic” nodule, even after biopsy, since fluid may be drawn off from both lesions. Both may look hypoechoic (black) but a cyst is usually larger and more round, somewhat blacker and has a thin, sharp edge, as shown in
Figure 6. The cyst has a specific feel on palpation (whereas a colloid nodule, where palpable, feels firm, even hard) and, if tested for, is translucent. Cysts may have a solid component whose echogenicity may be hypo or hyper echoic, sometimes only seen after removal of the fluid.
7. Oncocytic Nodules
About 10% of thyroid nodules contain a predominance of oncocytes, or Hürthle cells, which are characterised from their eosinophilic granular cytoplasm, vesicular nucleus and large nucleolus. A Hürthle cell is larger than a follicular cell, and its cellular material stains pink with ethanol fixed haematoxylin–eosin stain. These cells can also be identified and enumerated in Papanicolaou-stained smears or with air-dried Romanowsky stain. Hürthle cells are also seen in Hashimoto thyroiditis and in association with benign nodules. An oncocytic tumour comprises 70% or more oncocytes and is shown at surgery to be benign in 90% of cases and malignant in 10% of cases. An example of a benign oncocytic adenoma is seen in
Figure 7.
8. Calcification
The normal gland does not contain any calcification. The presence of calcification in association with nodules generally indicates that the nodules are long standing and therefore likely to be benign. However, breaks in the wall of a calcified nodule suggest that the nodule is a cancer which has invaded into the surrounding thyroid tissue and is considered a suspicious feature of a nodule [
7]. Calcification is sometimes seen as spots or sheets scattered throughout the thyroid. Calcification surrounding a thyroid nodule, giving it the appearance of a “bone ball”, can be felt as a hard, mobile lump on neck palpation that is crunchy on biopsy. Chronic linear or egg shell calcification is associated with shadowing because the ultrasound waves are unable to pass through calcified tissue (
Figure 8A,B). Calcification is also seen in the thyroid of patients with chronic Hashimoto thyroiditis and Graves’ disease.
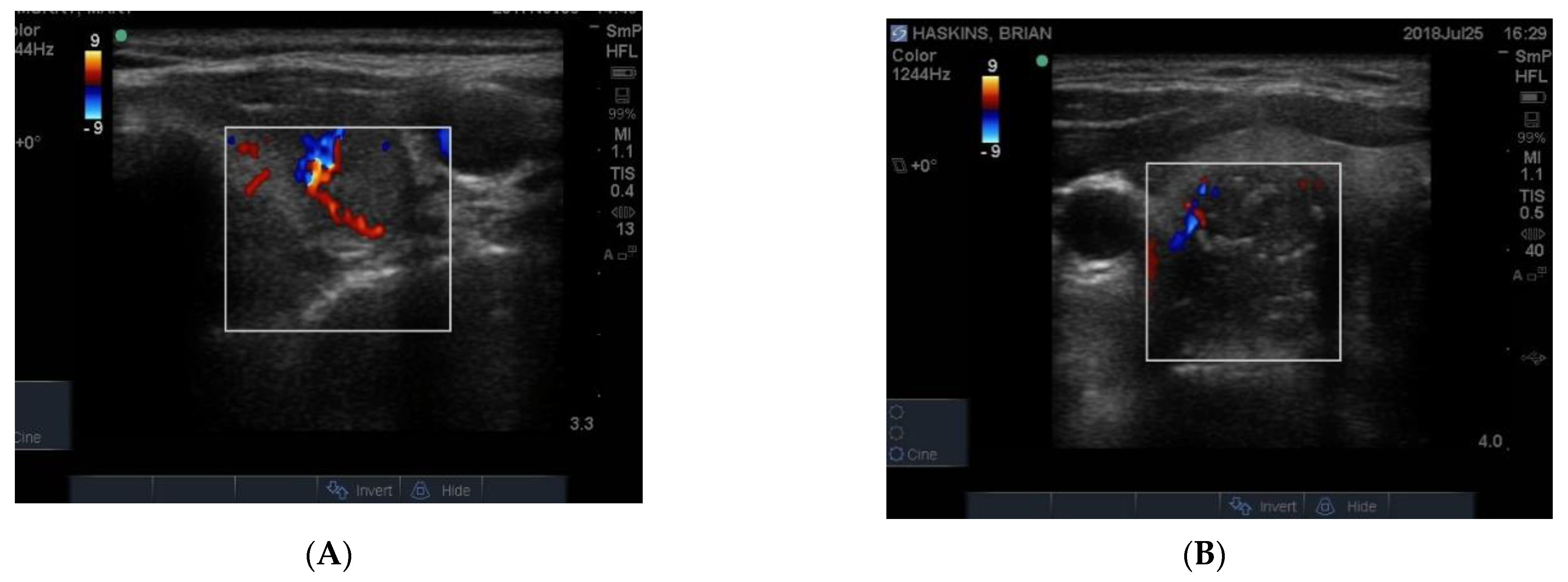
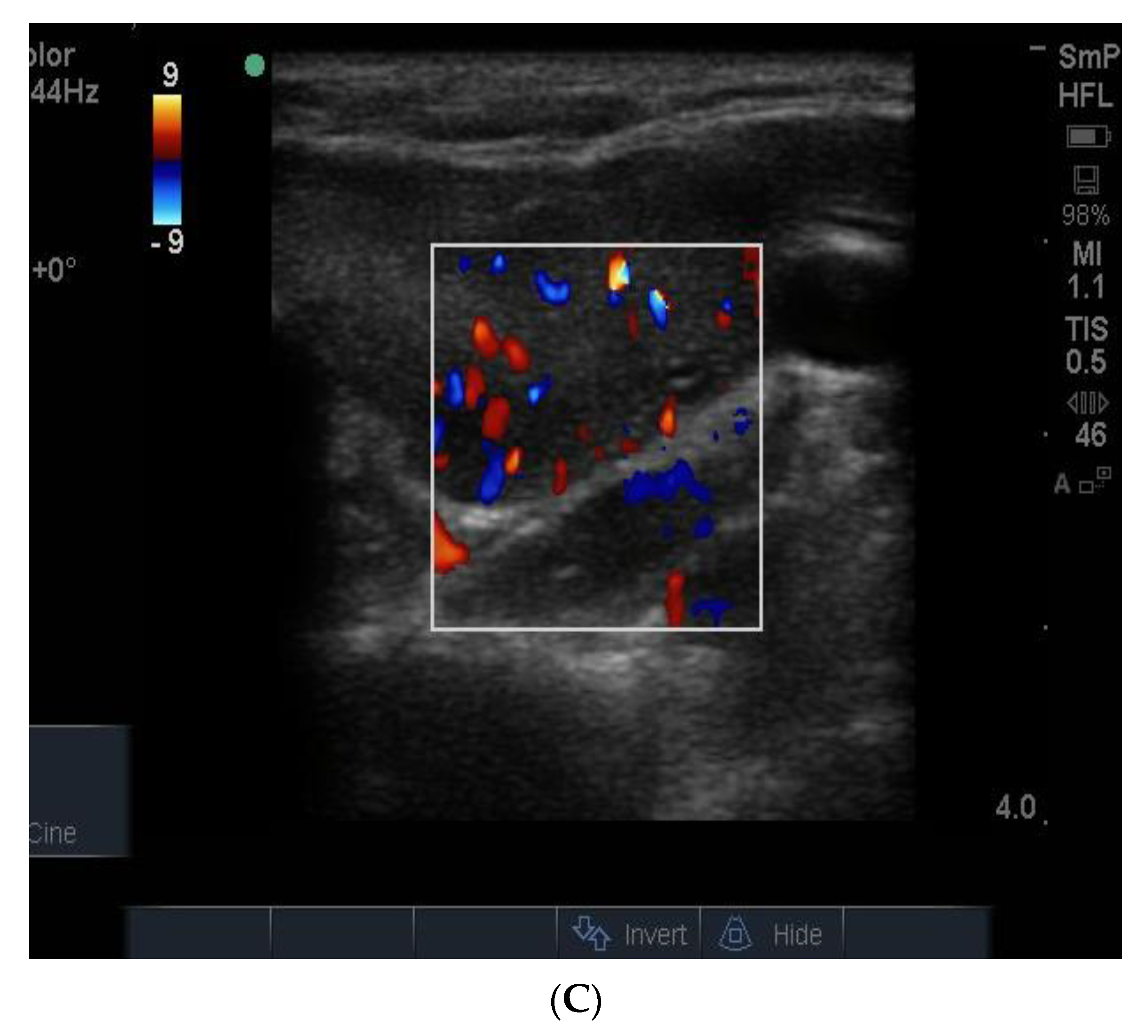
9. Vascularity
The blood supply to thyroid nodules is an important feature to be documented in the course of real time ultrasonography. There are three types of vascularity to be discussed. Firstly, the so-called hypoechoic halo surrounding a benign nodule is caused by compressed blood vessels which can be seen when the “colour” button is engaged. An example of this is seen in
Figure 9A. Secondly, the degree of vascularity around the outside of a nodule is reflective of its activity and prominent blood supply around a nodule maybe a sign of thyroid cancer (
Figure 9B) [
8] but can also be present around nodules shown by biopsy to be benign. It has recently been shown that blood vessels within a nodule, especially if it has other suspicious features (
Figure 9B), may be a reliable sign of cancer [
9].
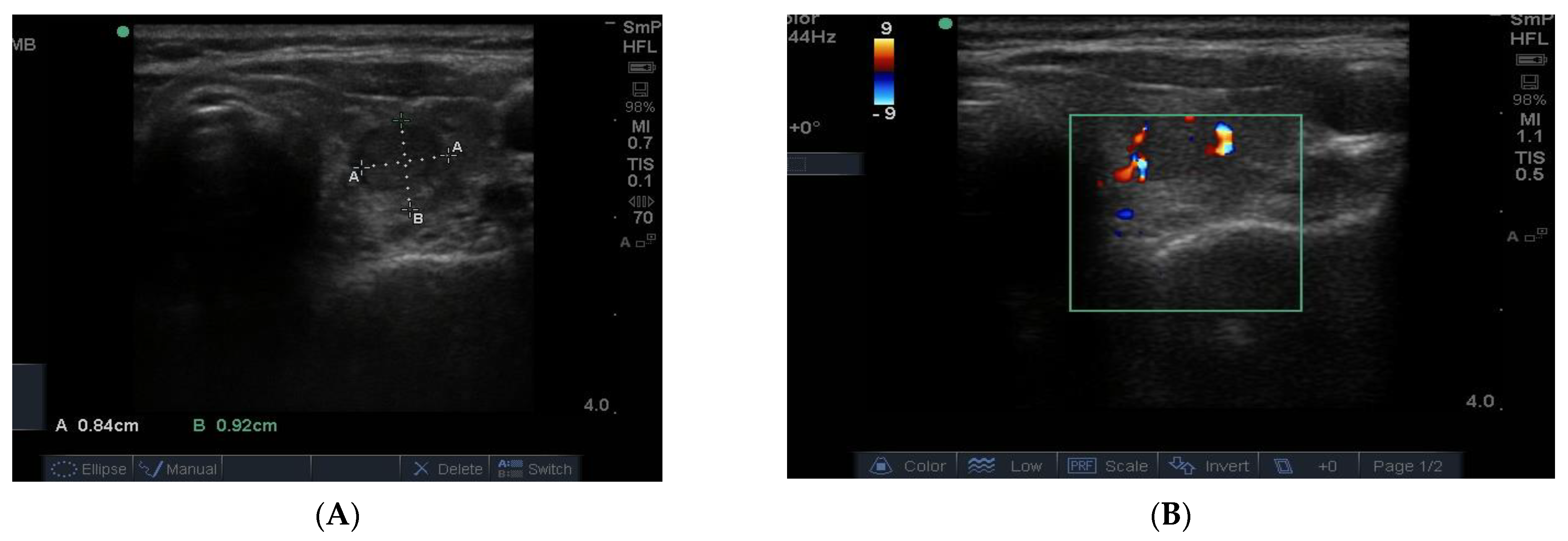
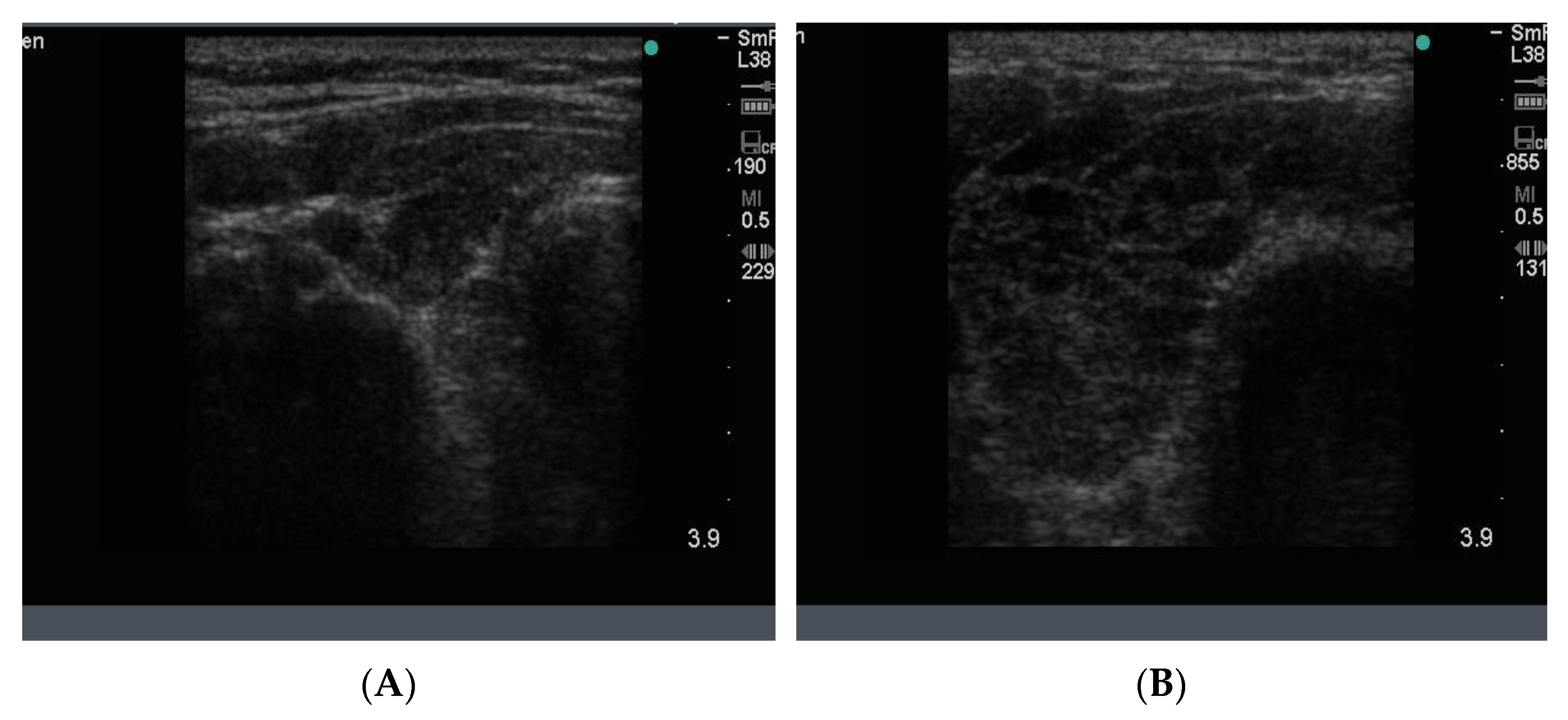
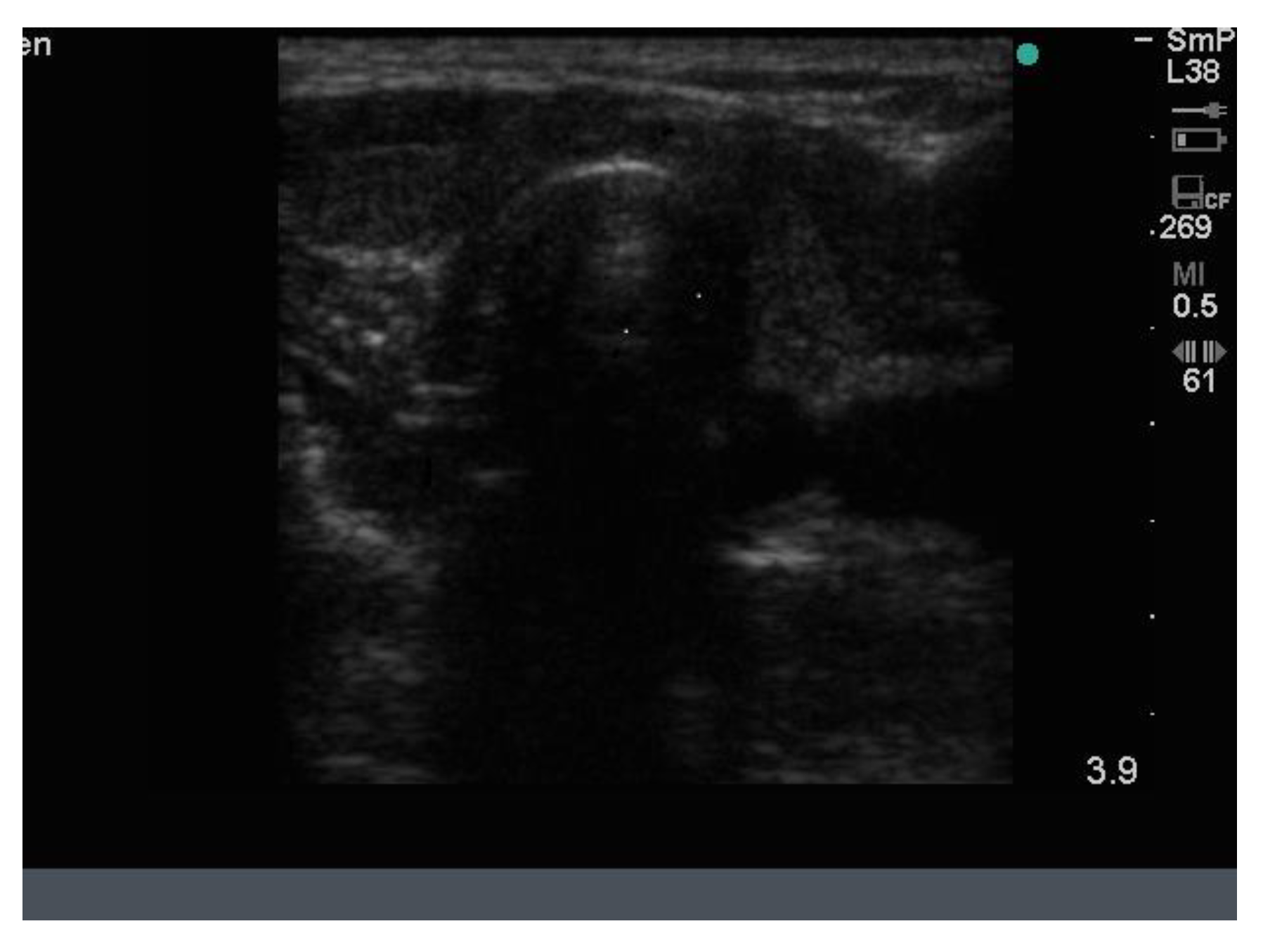
In
Figure 10 is shown matching images of a benign nodule without (A) and with (B) blood flow in the halo around the nodule.
10. Thyroid Cancer
The thyroid specialist using their own portable US machine will, with experience, learn to recognize those characteristics of nodules which are suspicious for malignancy. These include taller than wide, indicating that the tumour is growing through, rather than along, the tissue planes; absence of a peripheral halo (compressed blood vessels in a benign nodule), the 3–4 mm “fluffy” intra nodular microcalcifications (actually psamoma bodies rather than true calcification), which are 90% specific for papillary cancer [
1,
2,
10]; intra nodular hypervascularity, which is presumed to be feeding the cancer; and size > 3 cm.
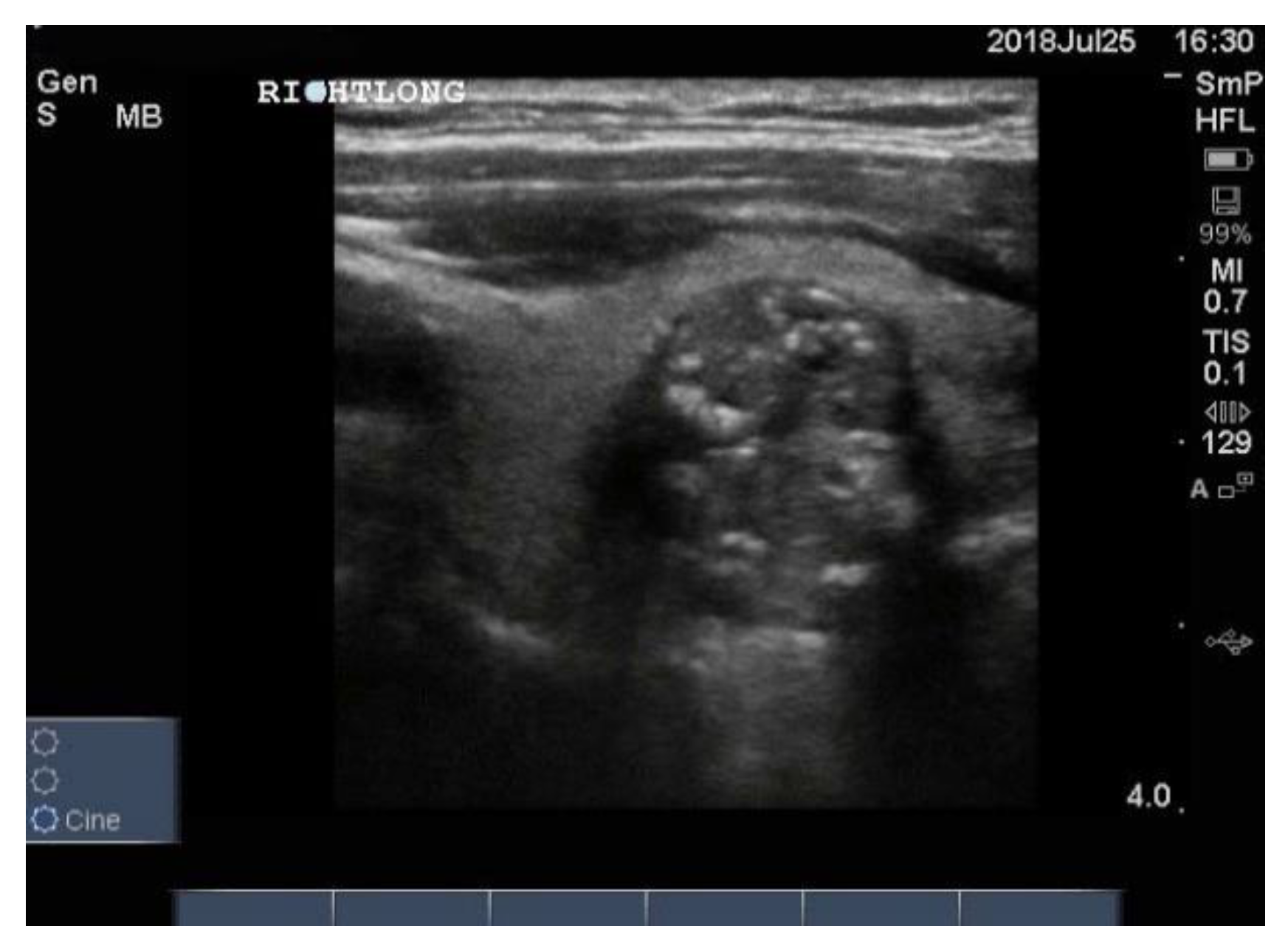
Three examples of papillary thyroid cancer are shown here. Firstly, a large typical papillary cancer with the characteristic microcalcifications is seen in
Figure 11.
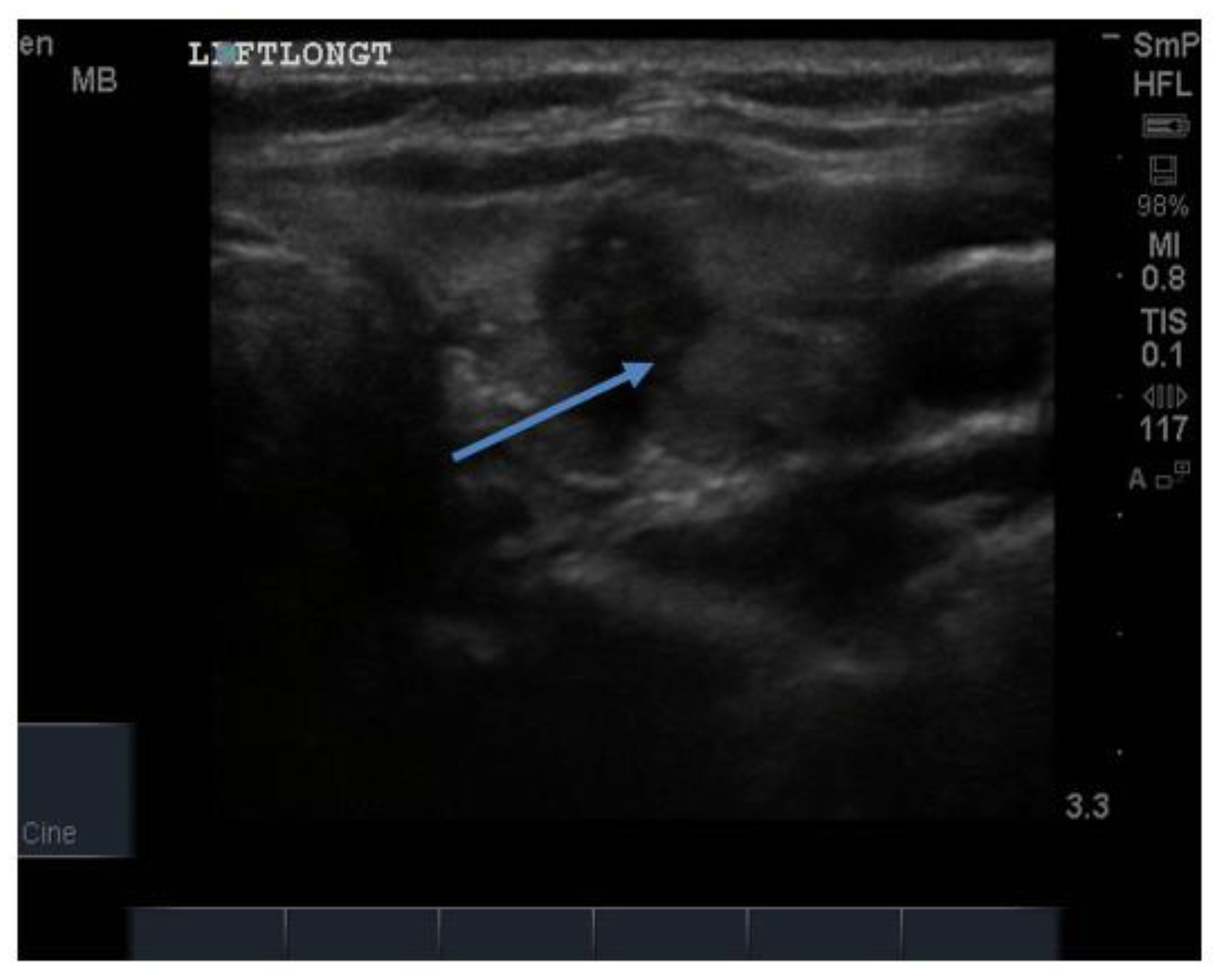
Secondly, a smaller but more hypoechoic lesion with obvious and larger soft microcalcifications and an irregular edge is shown in
Figure 12. These two nodules are typical for papillary cancer and are reported from FNAB as “suspicious for papillary thyroid cancer”. In both cases this was confirmed at thyroidectomy
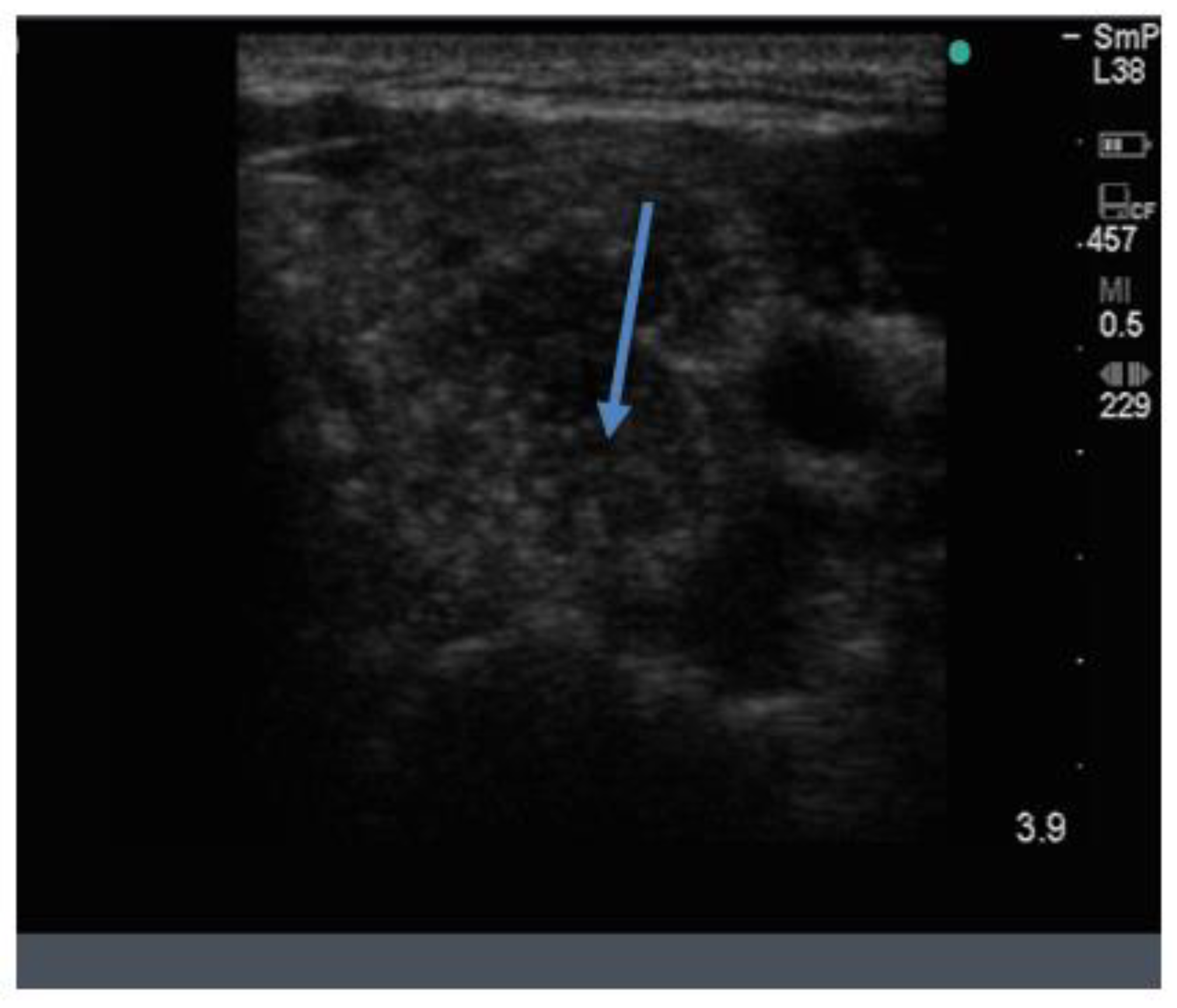
Thirdly, an example of a much smaller lesion that turned out to be papillary cancer is shown in
Figure 13. The nodule is only 10–12 mm in size, hypoechoic and has an unusual and irregular edge. Three years earlier the same lesion was seen on ultrasound, and its size then was 8 × 9 mm with no other suspicious features and no microcalcifications nor feeding vessels or blood vessels, indicating that it had grown very little over the intervening 3 years. It was considered suspicious on ultrasound because of its shape and edge. The lesion was shown to be suspicious for papillary cancer at FNAB and confirmed at hemi thyroidectomy.
It is not possible to differentiate the more common papillary cancer from the very much less common follicular neoplasms by ultrasound, although follicular lesions are more cellular and less hypoechoic and do not usually contain microcalcifications, the diagnosis being made at open biopsy.
On follow up after treatment, usually total thyroidectomy followed by radioiodine, one looks for abnormal lymph nodes in the neck, indicating local relapse. In the case of papillary carcinoma, involved nodes are round, hypo echoic and may contain microcalcifications (
Figure 14). They may have a cystic structure with posterior enhancement. It is recommended that the cervical lymph nodes be examined in all patients who undergo ultrasonography for whatever reason.
11. Graves’ Hyperthyroidism
In Graves’ hyperthyroidism, the gland is typically diffusely enlarged to a degree that reflects the severity of the hyperthyroidism. Its vascularity is increased, often dramatically, and is generalised. As the disease becomes chronic, e.g., after one or more relapses post ant thyroid medication, the gland shrinks and becomes scarred and nodular, so called “nodular Graves’ disease”. However, it is not uncommon for patients with Graves’ disease to have incidental nodules, in which case the differential diagnosis is as follows: (1) Graves’ disease which has become thickened and nodular due to its chronicity; (2) Graves’ disease with distinct nodules; and (3) Graves’ disease with one or more hot (toxic) nodules, i.e., two different diseases.
The blood supply in typical Graves’ disease is diffusely increased (and associated with a murmur), sometime up to 100 times normal, and the gland texture on ultrasound is usually heterogeneous (patchy) with a fine cystic appearance throughout, which reflects the diffuse nature of the inflammatory process (
Figure 15). Following radio iodine treatment, the normal gland architecture is disrupted because the follicles are destroyed, and scar tissue predominates.
12. Hashimoto Thyroiditis
Hashimoto thyroiditis is common, especially when diagnosed cytologically from biopsy of thyroid nodules, as an incidental finding, being demonstrated in 13.4% of a group of 811 patients [
11]. The disease is approximately 10 times more common in females than males. Ultrasonography should be performed in all patients with Hashimoto thyroiditis to identify any nodules. Although not clearly established, it seems likely that there is an increased prevalence of cancer in patients with this chronic inflammatory condition compared to patients without nodules Ultrasonography is also useful in following individual patients with Hashimoto thyroiditis as an aid to management with thyroxine replacement [
12] and to recognize the uncommon, but not rare, situation where Graves’ hyperthyroidism changes (“flips”) to Hashimoto thyroiditis [
13].
As a result of the senior author’s (JW) extensive experience of the ultrasound appearances of Hashimoto thyroiditis, he and his colleagues have developed a 5-stage classification of the inflammatory changes from early (stages 1, 2) through later (stages 3, 4, 5), as follows: Stage 1 is characterised by mild inflammatory changes manifest as small cystic lesions representing the lymphoid nodules and inflammatory infiltrations in a normal or slightly enlarged thyroid. In stage 2, the gland is enlarged and the cystic areas are better defined, more frequent and larger; the blood supply to the gland is increased in stages 1 and 2. In stage 3, the thyroid is generally bigger and the signs of inflammation increased with larger inflammatory nodules, and the blood supply is now patchy. In stage 4 the gland is becoming avascular, and the nodules are replaced by hypoechoic (black) spaces with scar tissue (fibrosis), and there are increased sheets of fibrosis, giving the appearance of pseudo nodules. In the final stage the gland is shrunken and scarred with absent blood supply and devoid of thyroid tissue [
14]. Further uses of this classification system, such as the correlation between inflammation stage and the need for thyroxin replacement, are currently being addressed by the authors.
In Hashimoto thyroiditis the blood supply to the gland increases during the early inflammatory stages, but later, when the inflammation has burnt out and the gland is scarred and empty, the overall blood supply is markedly reduced. Examples of the two types of end stage disease are seen in
Figure 16.
13. Transient Thyroiditis
The sonographic appearance of the various forms of transient thyroiditis, namely subacute thyroiditis, silent thyroiditis and post-partum thyroiditis, is worthy of mention as this has not been described in detail by others. Taking subacute thyroiditis as a model for the changes that occur during inflammation and on recovery, we see that the gland appears very abnormal when the patient is hyperthyroid with hypoechoic “streaks” infiltrating the gland, as seen in
Figure 17. On recovery, the gland returns to normal as the thyroid follicular cells recover. Even though the tissue damage in subacute thyroiditis reflects virus infection, or a post viral reaction, and that in the latter two disorders, an immunological process, the ultrasound changes seen in all three disorders are similar.
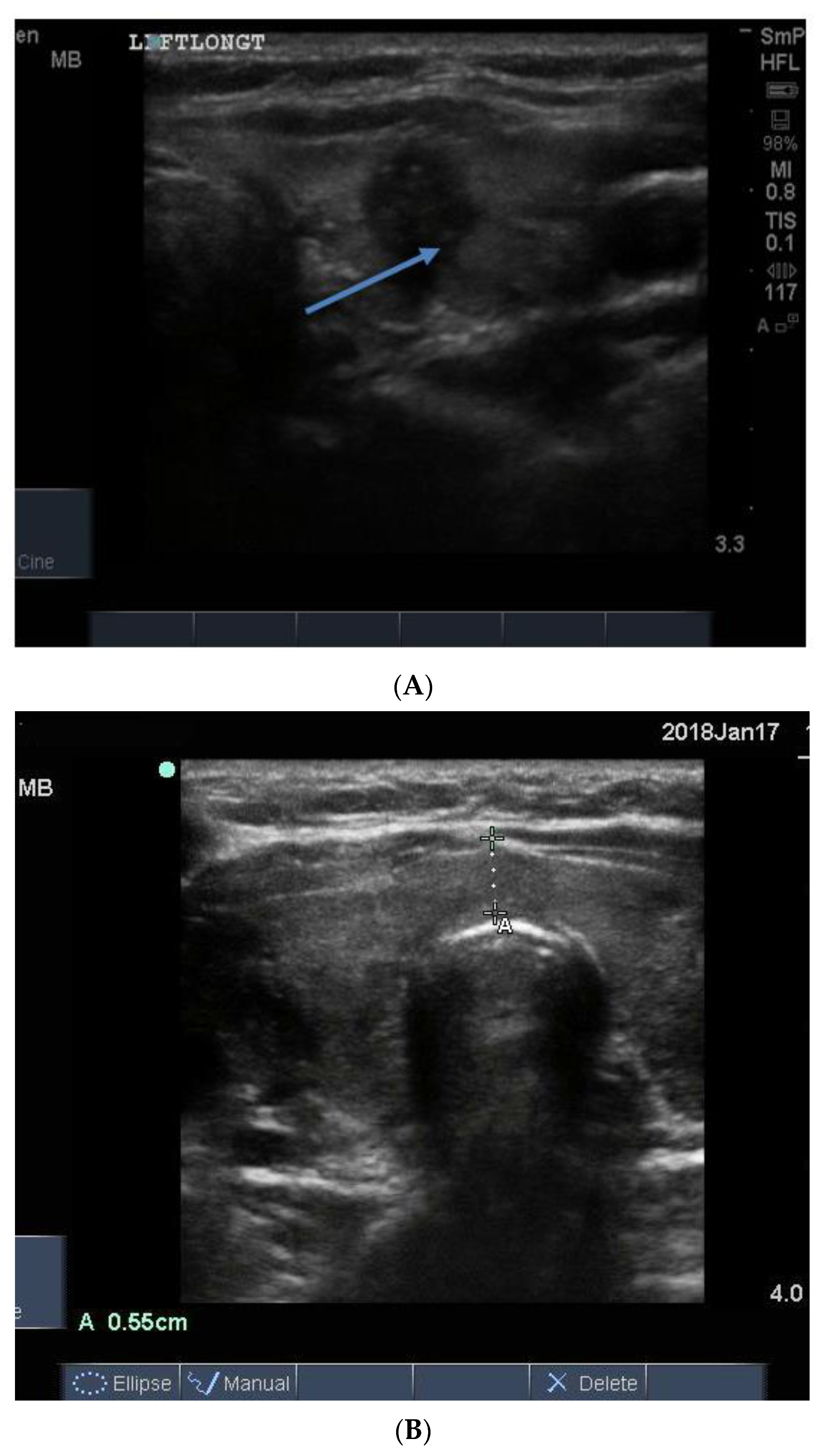
14. Parathyroid Disease
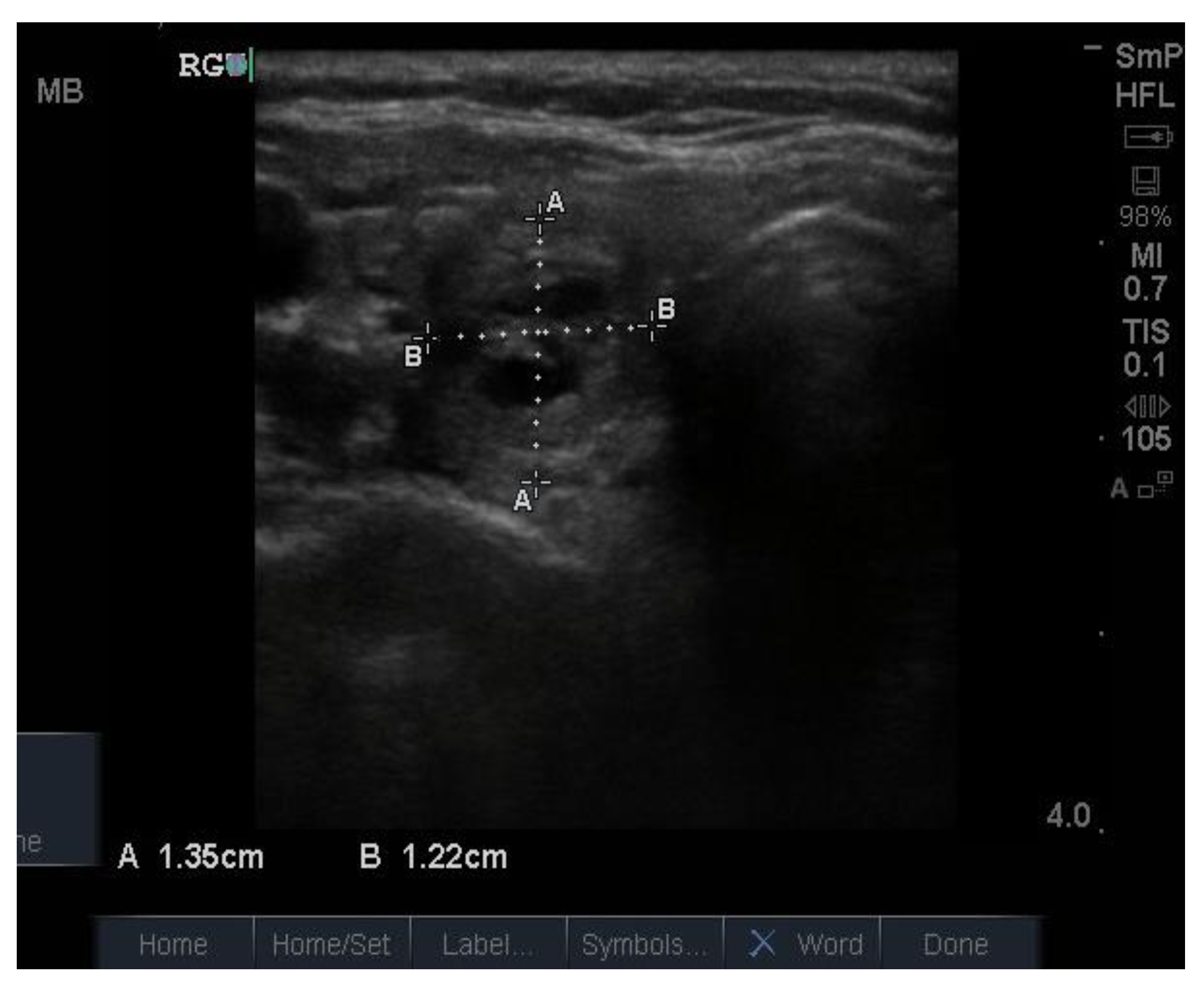
Because the senior author (JW) routinely measures serum calcium, parathyroid hormone (PTH) and vitamin D in his patients, hyperparathyroidism due to a benign adenoma of one of the parathyroid glands appears to be much more common than previously thought. The parathyroid glands are hidden behind the thyroid and so may be obscured by thyroid nodules, although they can often be seen in the longitudinal view below the lobes, as a hypoechoic lesion of around 1 cm in diameter (
Figure 18).
The parathyroid adenoma is typically hypoechoic by comparison to the nearby thyroid tissue, which is consistent with the author’s experience. However, only about 50% of subsequently proven parathyroid adenomas are seen on ultrasound and even the Sestamibi nuclear scan fails to pick them up in about 30% of cases.
15. Does the Thyroid Specialist have Advantages over the Consultant Radiologist?
The consultant radiologist does not always report on those features of thyroid lesions that are essential to interpreting the clinical and other findings. For example, in the senior author’s (JW) experience, the diffuse familial fibrotic variant of papillary thyroid cancer has been described as “localised Hashimoto thyroiditis”, which does not exist, and the inflammatory lesions of Hashimoto thyroiditis and Graves’ hyperthyroidism are often referred to as “nodules” and are counted and measured. Recommending biopsy of a thyroid nodule based on its size only—rather than the presence or not of suspicious features—is problematic, since it wrongly assumes that small nodules are never cancerous.
More recently, the emphasis has shifted to classifying nodules according to their degree of suspicion for cancer, regardless of their size. In the context of this changing approach to assessing thyroid nodules, a new scoring system, known as TI-RADS [
15,
16], has been developed to allow everyone who carries out thyroid ultrasonography, whether technician, radiologist or endocrinologist, to be consistent in how they characterise and report features of thyroid nodules. As a result of the now almost universal use of TI-RADS, the tendency is to carry out more ultrasounds and fewer biopsies. This seems logical because we should remember that only about 5% of patients with one or more thyroid nodules turn out to have thyroid cancer. Finally, in respect to who is best qualified to carry out thyroid ultrasonography, we recommend that the role of clinician practiced ultrasound in either confirming of changing ultrasound/radiology findings of patients presenting with imaging performed before referral be addressed in a prospective study.
16. Vocal Cord Assessment
Recently, the thyroid specialist has found a new use for their portable ultrasound machine. Although thyroid surgeons generally send their patients to an ENT specialist for direct laryngoscopic assessment of the vocal cords to identify any problem that was present before surgery, the thyroid specialist can learn to recognize and quantify normal abduction and adduction of the true vocal cord, especially in female patients. They do this by placing the small parts probe in a transverse plane across the anterior wall of the larynx just below the thyroid notch, with the patient speaking or humming (preferably in tune).
17. The Future
New approaches to the use of ultrasound to assess thyroid nodules including shear wave elastography, which measures tissue stiffness, are being developed in order to help identify those nodules that need to be biopsied. Thyroid specialists in Europe often treat thyroid cysts by injecting 90% alcohol to replace the fluid removed, and some solid nodules are treated by laser ablation. These procedures are rarely used in North America and Australia, countries where the senior author (JW) has worked, and it is unlikely that this approach will ever become mainstream outside of Europe.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}


















