
Diabot: Development of a Diabetic Foot Pressure Tracking Device

 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
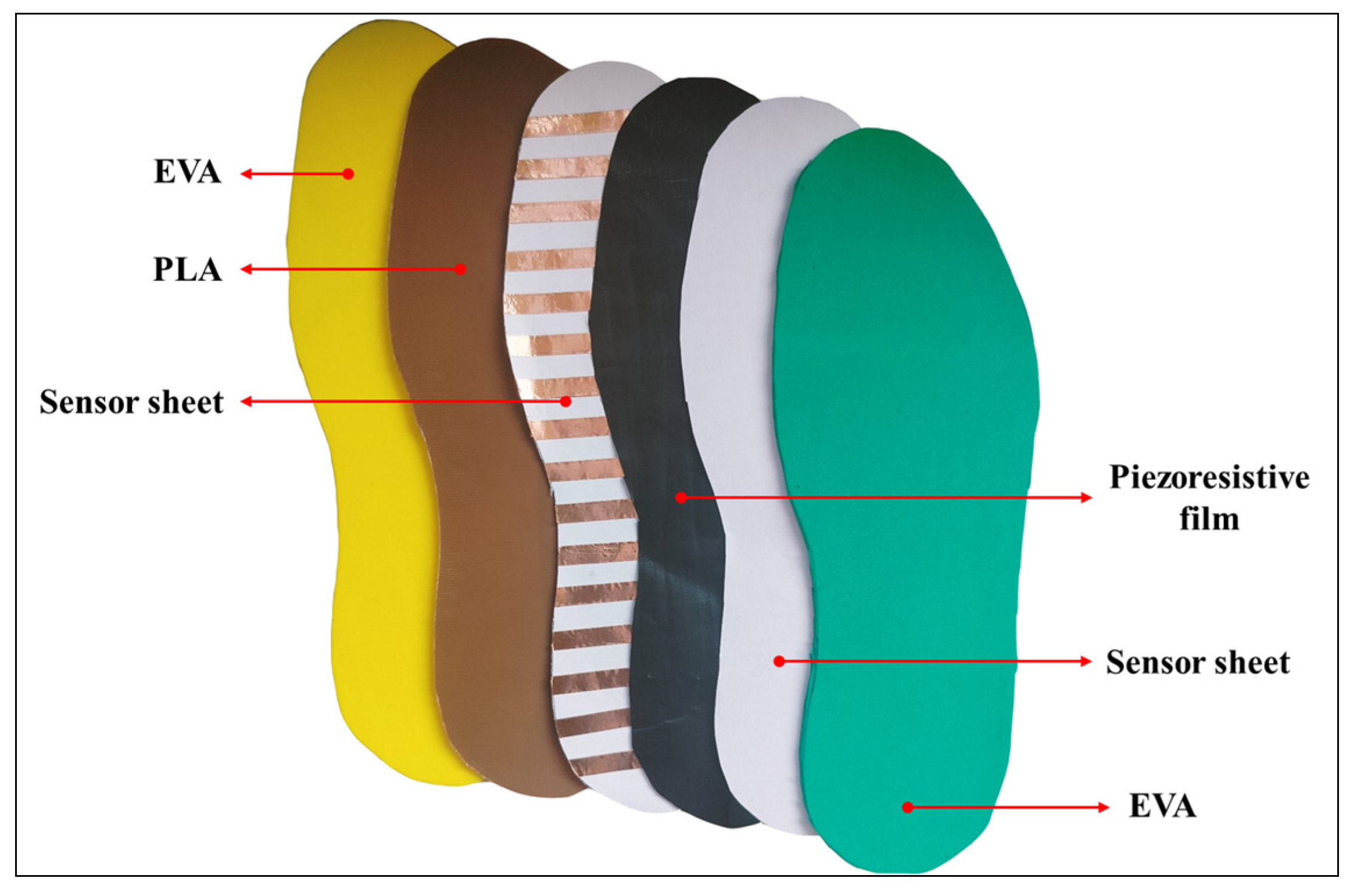
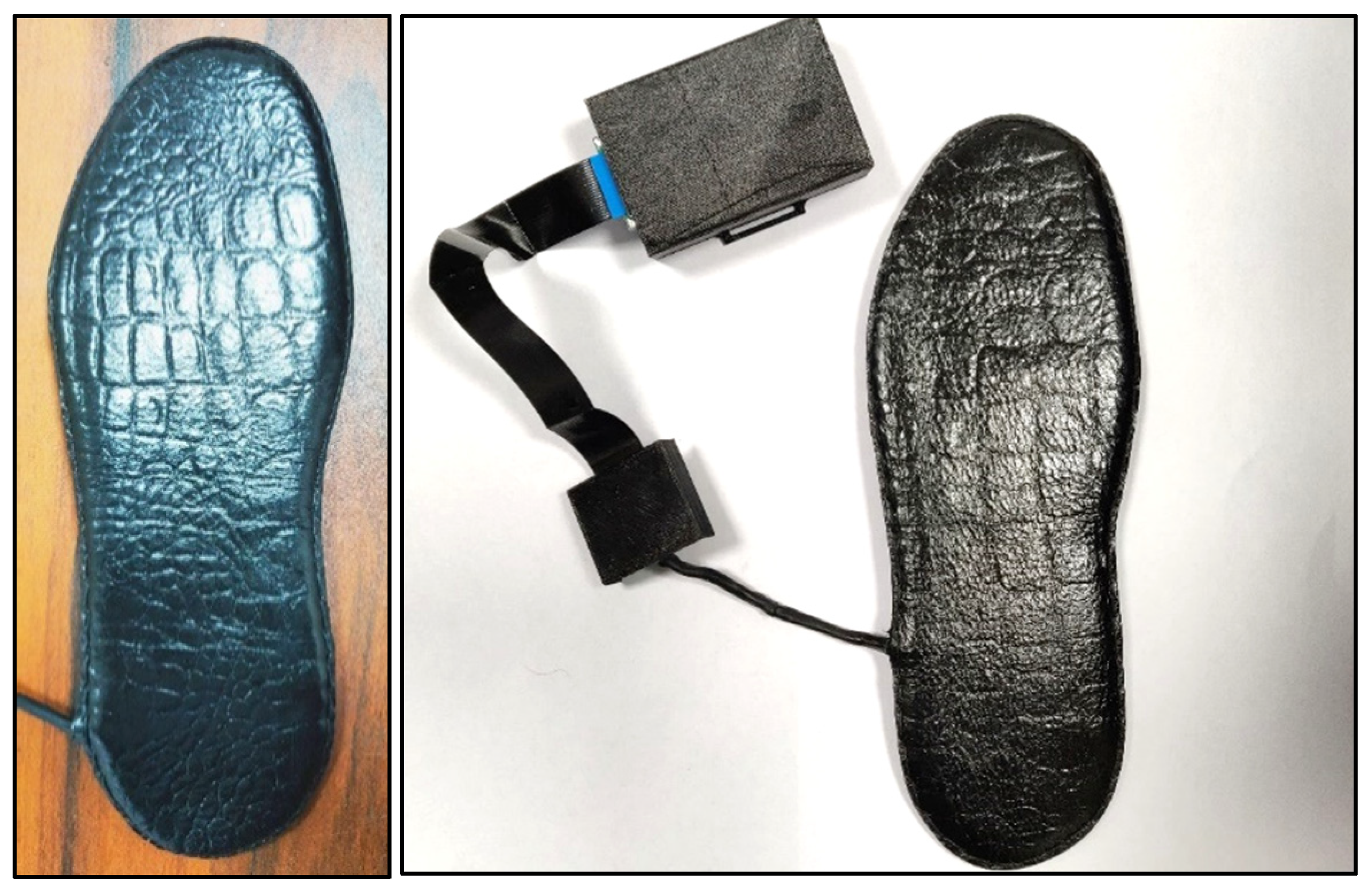
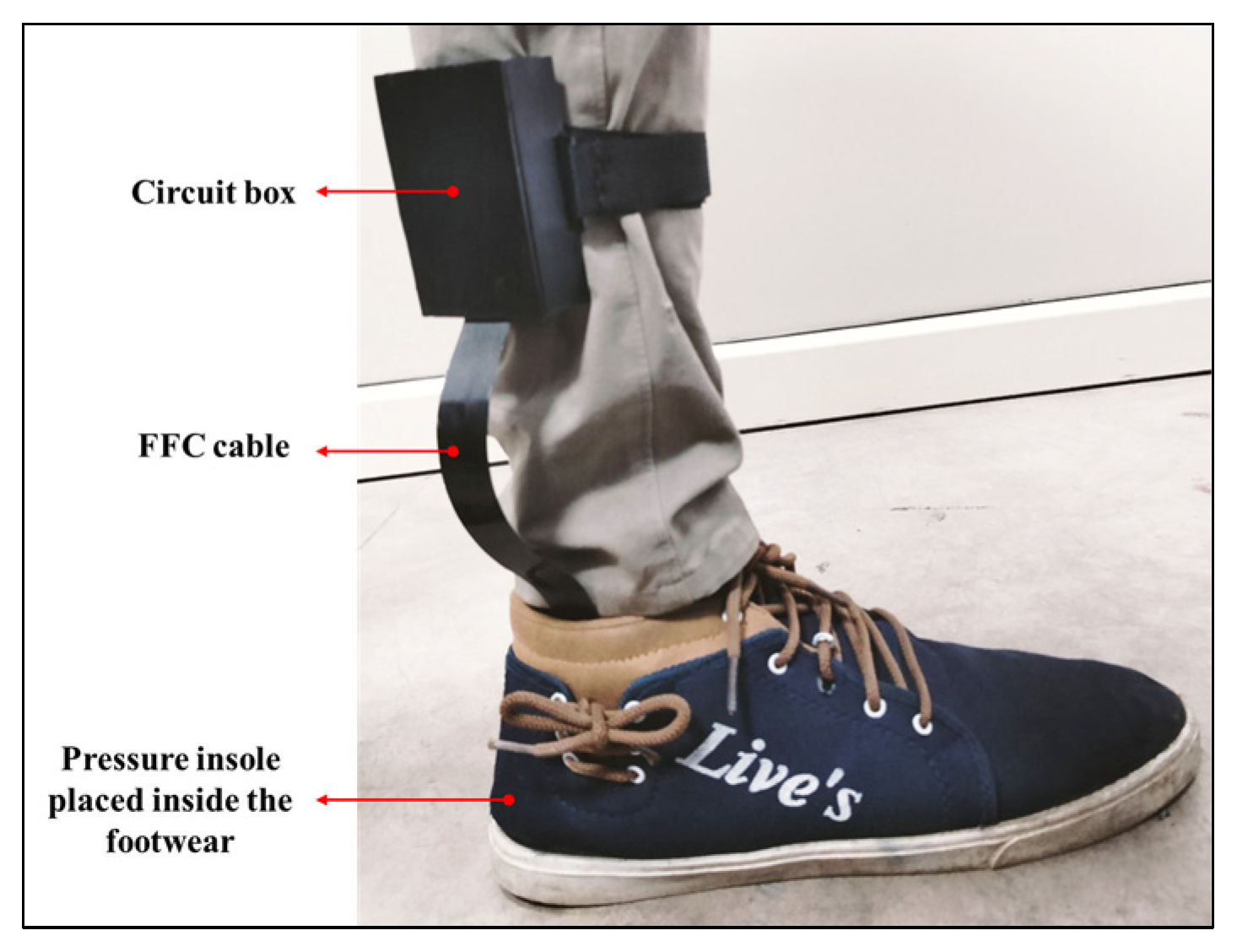
2. Materials and Methods
3. Results
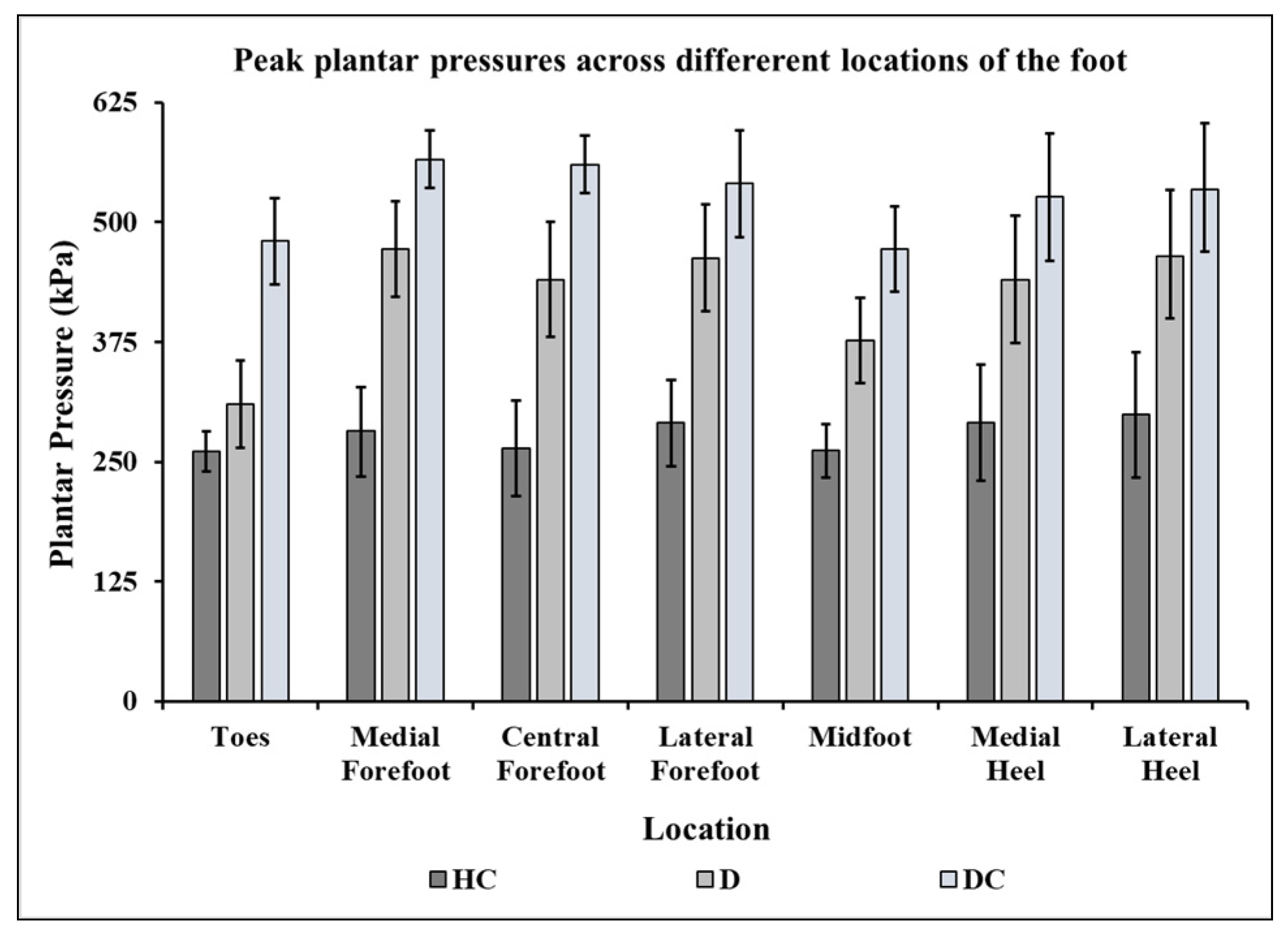
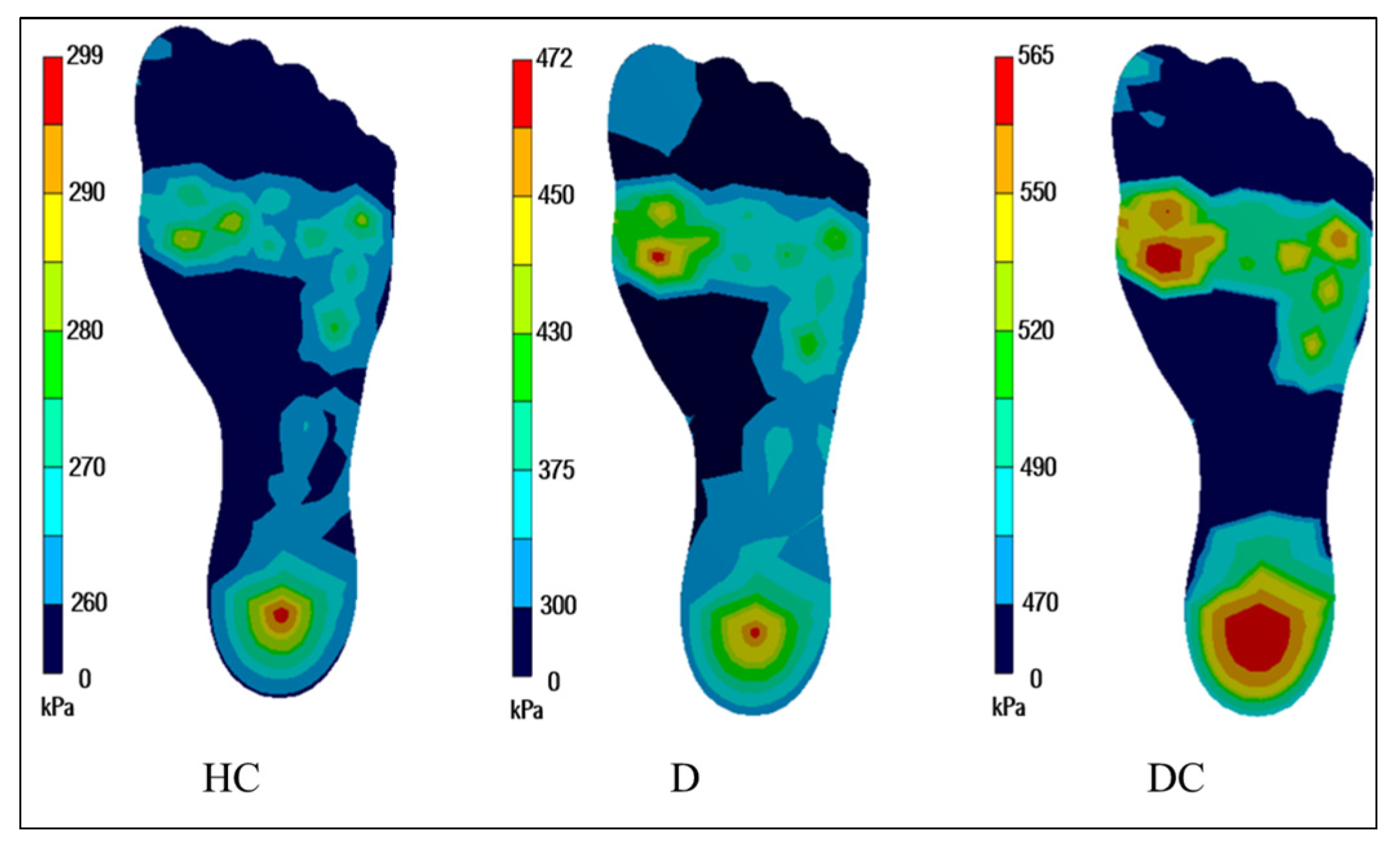
3.1. Plantar Pressure Distribution during Standing
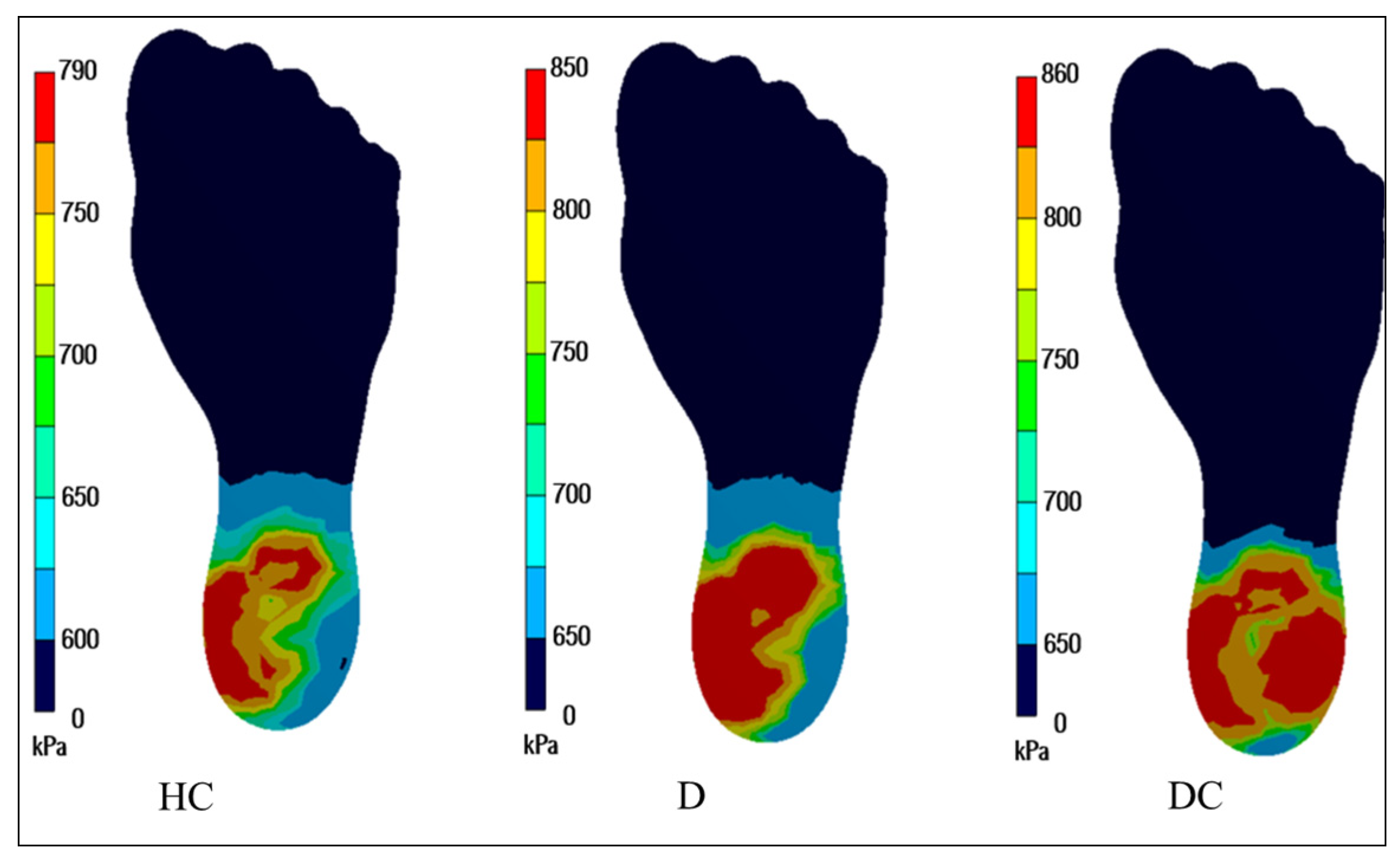
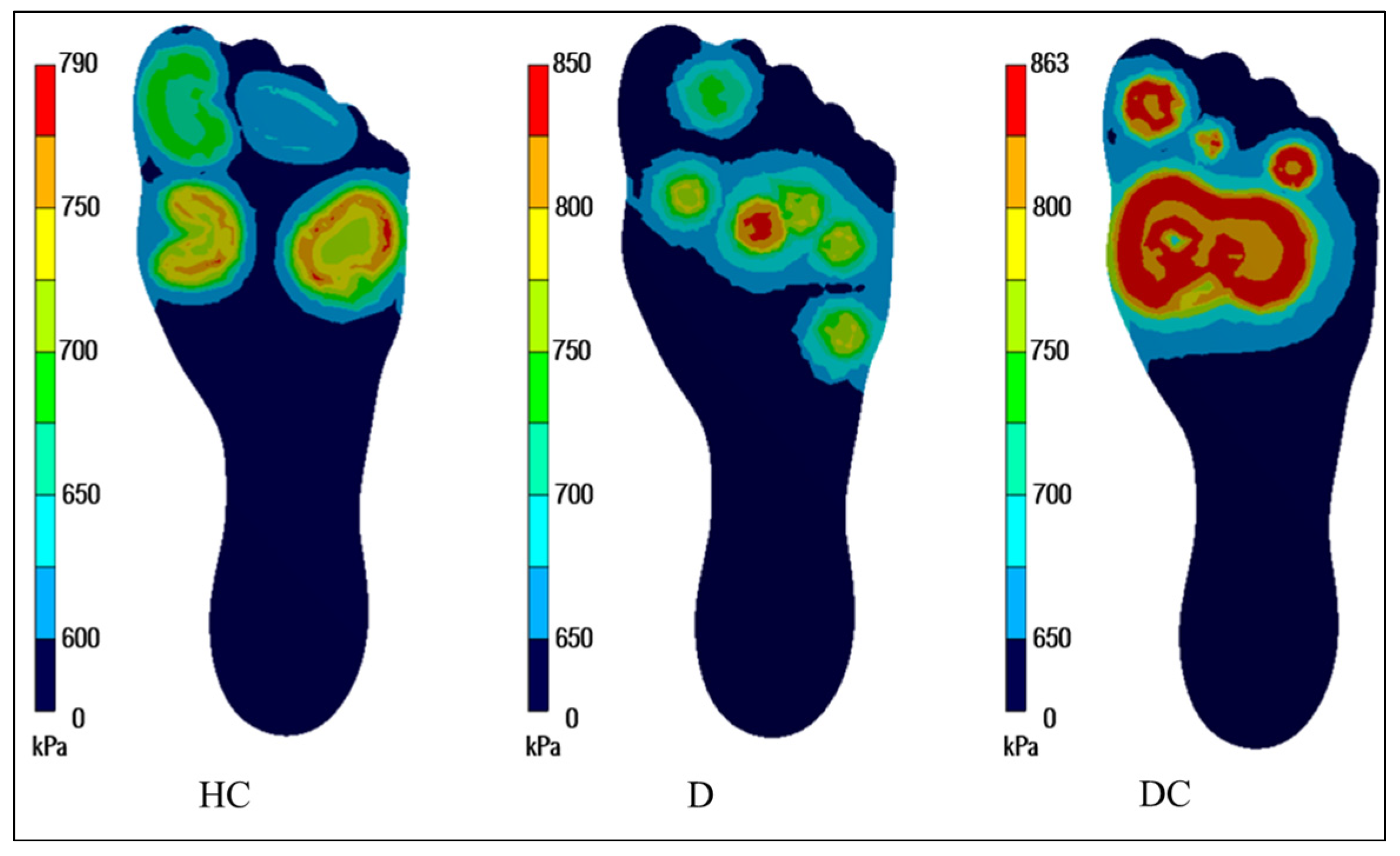
3.2. Plantar Pressure Distribution during Walking Loads
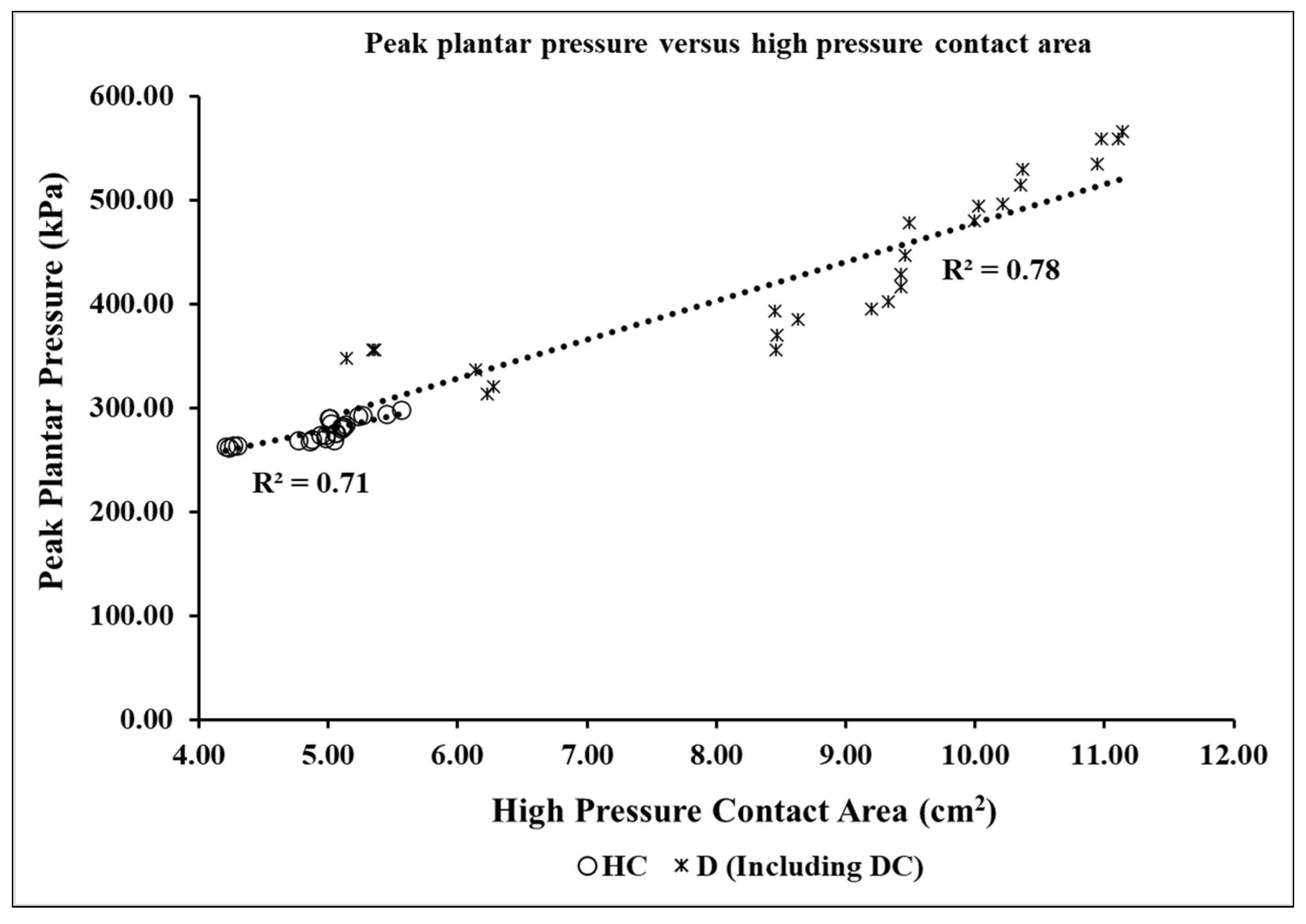
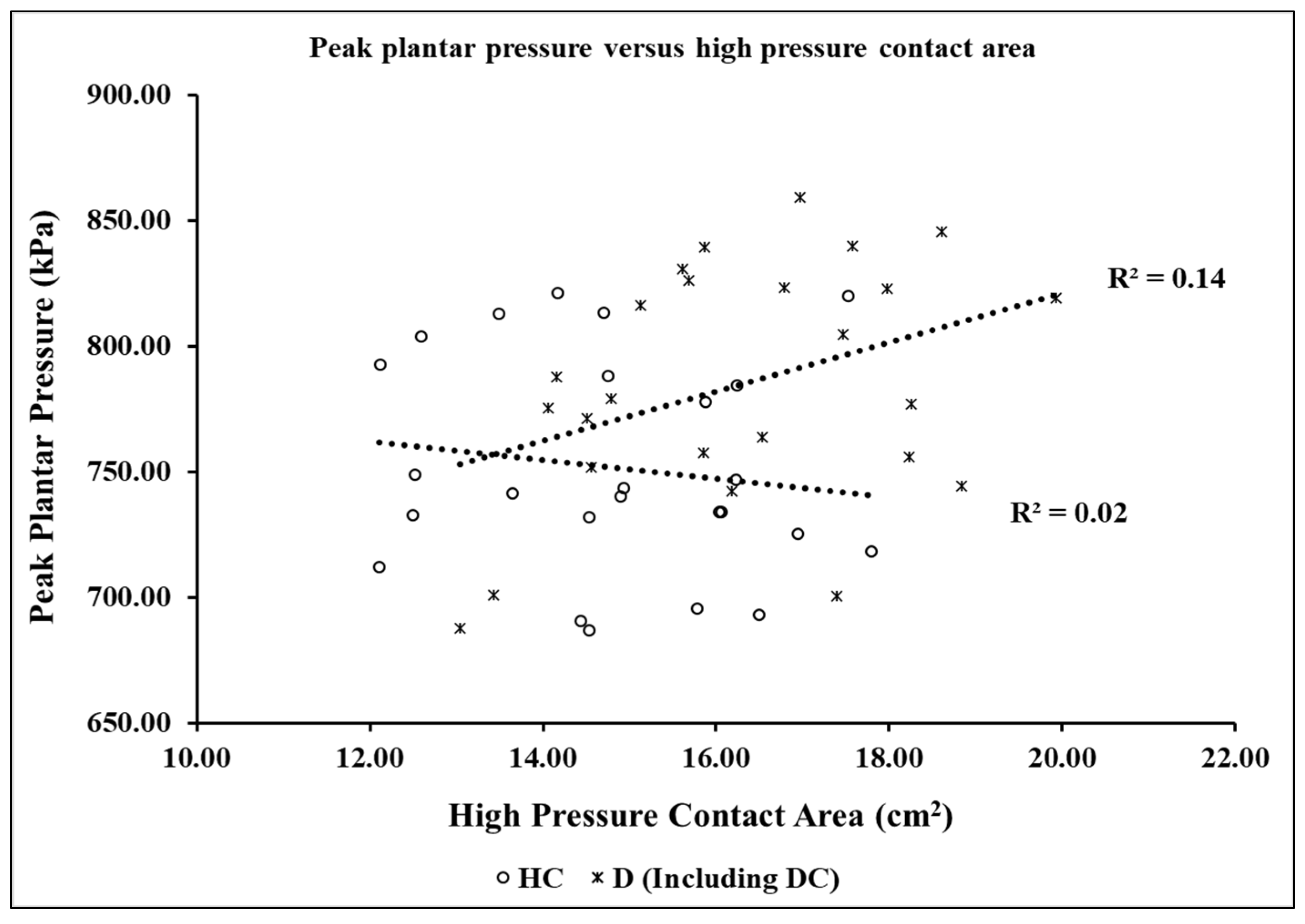
3.3. Effect of Peak Plantar Pressure on the High-Pressure Contact Area
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- López-López, D.; Pérez-Ríos, M.; Ruano-Ravina, A.; Losa-Iglesias, M.E.; Becerro-De-Bengoa-Vallejo, R.; Romero-Morales, C.; Calvo-Lobo, C.; Navarro-Flores, E. Impact of quality of life related to foot problems: A case–control study. Sci. Rep. 2021, 11, 14515. [Google Scholar] [CrossRef] [PubMed]
- Wright, W.G.; Ivanenko, Y.P.; Gurfinkel, V.S. Foot anatomy specialization for postural sensation and control. J. Neurophysiol. 2012, 107, 1513. [Google Scholar] [CrossRef] [Green Version]
- Lang, L.M.G. The anatomy of the foot. Baillieres Clin. Rheumatol. 1987, 1, 215–240. [Google Scholar] [CrossRef] [PubMed]
- Locke, J.; Baird, S.A.; Frankis, J. Preliminary observations of muscle fibre cross sectional area of flexor digitorum brevis in cadaver feet with and without claw toes. J. Foot Ankle Res. 2010, 3, 32–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghanem, I.; Massaad, A.; Assi, A.; Rizkallah, M.; Bizdikian, A.J.; El Abiad, R.; Seringe, R.; Mosca, V.; Wicart, P. Understanding the foot’s functional anatomy in physiological and pathological conditions: The calcaneopedal unit concept. J. Child. Orthop. 2019, 13, 134–146. [Google Scholar] [CrossRef]
- Pita-Fernandez, S.; Gonzalez-Martin, C.; Aalonso-Tajes, F.; Seoane-Pillado, T.; Pertega-Diaz, S.; Perez-Garcia, S.; Seijo-Bestilleiro, R.; Balboa-Barreiro, V. Flat Foot in a Random Population and its Impact on Quality of Life and Functionality. J. Clin. Diagn. Res. 2017, 11, 22–27. [Google Scholar] [CrossRef]
- Chhikara, K.; Singh, G.; Gupta, S.; Chanda, A. Progress of additive manufacturing in fabrication of foot orthoses for diabetic patients: A review. Ann. 3D Print Med. 2022, 8, 100085. [Google Scholar] [CrossRef]
- Hendry, G.J.; Fenocchi, L.; Woodburn, J.; Steultjens, M. Foot pain and foot health in an educated population of adults: Results from the Glasgow Caledonian University Alumni Foot Health Survey. J. Foot Ankle Res. 2018, 11, 48. [Google Scholar] [CrossRef]
- Garrow, A.P.; Silman, A.J.; Macfarlane, G.J. The cheshire foot pain and disability survey: A population survey assessing prevalence and associations. Pain 2004, 110, 378–384. [Google Scholar] [CrossRef]
- Dunn, J.E.; Link, C.L.; Felson, D.T.; Crincoli, M.G.; Keysor, J.J.; McKinlay, J.B. Prevalence of foot and ankle conditions in a multiethnic community sample of older adults. Am. J. Epidemiol. 2004, 159, 491–498. [Google Scholar] [CrossRef] [Green Version]
- Menz, H.B.; Jordan, K.P.; Roddy, E.; Croft, P.R. Characteristics of primary care consultations for musculoskeletal foot and ankle problems in the UK. Rheumatology 2010, 49, 1391–1398. [Google Scholar] [CrossRef] [Green Version]
- Chhikara, K.; Gupta, S.; Chanda, A. Development of a novel foot orthosis for plantar pain reduction. Mater. Today Proc. 2022, 62, 3532–3537. [Google Scholar] [CrossRef]
- Bakker, K.; Abbas, Z.G.; Pendsey, S. Step by Step, improving diabetic foot care in the developing world. Pract. Diabetes Int. 2006, 23, 365–369. [Google Scholar] [CrossRef]
- Moulik, P.K.; Mtonga, R.; Gill, G.V. Amputation and Mortality in New-Onset Diabetic Foot Ulcers Stratified by Etiology. Diabetes Care 2003, 26, 491–494. [Google Scholar] [CrossRef] [Green Version]
- Mohammed, Y.A.; Farouk, H.K.; Gbreel, M.I.; Ali, A.M.; Salah, A.A.; Nourelden, A.Z.; Gawad, M.M.A.-E. Human amniotic membrane products for patients with diabetic foot ulcers. Do they help? A systematic review and meta-analysis. J. Foot Ankle Res. 2022, 15, 71. [Google Scholar] [CrossRef]
- Fernando, M.E.; Crowther, R.G.; Lazzarini, P.A.; Sangla, K.S.; Wearing, S.; Buttner, P.; Golledge, J. Plantar pressures are higher in cases with diabetic foot ulcers compared to controls despite a longer stance phase duration. BMC Endocr. Disord. 2016, 16, 51. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Singh, G.; Chanda, A. Prediction of diabetic foot ulcer progression: A computational study. Biomed. Phys. Eng. Express 2021, 7, 065020. [Google Scholar] [CrossRef]
- Bus, S.A.; Armstrong, D.G.; van Deursen, R.W.; Lewis, J.E.A.; Caravaggi, C.F.; Cavanagh, P.R. IWGDF guidance on footwear and offloading interventions to prevent and heal foot ulcers in patients with diabetes. Diabetes Metab. Res. Rev. 2016, 32 (Suppl. S1), 25–36. [Google Scholar] [CrossRef] [Green Version]
- Sutkowska, E.; Sutkowski, K.; Sokołowski, M.; Franek, E.; Dragan, S. Distribution of the Highest Plantar Pressure Regions in Patients with Diabetes and Its Association with Peripheral Neuropathy, Gender, Age, and BMI: One Centre Study. J. Diabetes Res. 2019, 2019, 7395769. [Google Scholar] [CrossRef]
- Caselli, A.; Pham, H.; Giurini, J.M.; Armstrong, D.G.; Veves, A. The Forefoot-to-Rearfoot Plantar Pressure Ratio Is Increased in Severe Diabetic Neuropathy and Can Predict Foot Ulceration. Diabetes Care 2002, 25, 1066–1071. [Google Scholar] [CrossRef] [Green Version]
- De Cock, A.; Vanrenterghem, J.; Willems, T.; Witvrouw, E.; De Clercq, D. The trajectory of the centre of pressure during barefoot running as a potential measure for foot function. Gait Posture 2008, 27, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Pandey, S.; Sharma, V. World Diabetes Day 2018: Battling the Emerging Epidemic of Diabetic Retinopathy. Indian J. Ophthalmol. 2018, 66, 1652. [Google Scholar] [CrossRef] [PubMed]
- Di Rosa, M.; Hausdorff, J.M.; Stara, V.; Rossi, L.; Glynn, L.; Casey, M.; Burkard, S.; Cherubini, A. Concurrent validation of an index to estimate fall risk in community dwelling seniors through a wireless sensor insole system: A pilot study. Gait Posture 2017, 55, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Taborri, J.; Rossi, S.; Palermo, E.; Patanè, F.; Cappa, P. A Novel HMM Distributed Classifier for the Detection of Gait Phases by Means of a Wearable Inertial Sensor Network. Sensors 2014, 14, 16212–16234. [Google Scholar] [CrossRef] [PubMed]
- Shu, L.; Hua, T.; Wang, Y.; Li, Q.; Feng, D.D.; Tao, X. In-shoe plantar pressure measurement and analysis system based on fabric pressure sensing array. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 767–775. [Google Scholar] [CrossRef] [Green Version]
- Saito, M.; Nakajima, K.; Takano, C.; Ohta, Y.; Sugimoto, C.; Ezoe, R.; Sasaki, K.; Hosaka, H.; Ifukube, T.; Ino, S.; et al. An in-shoe device to measure plantar pressure during daily human activity. Med. Eng. Phys. 2011, 33, 638–645. [Google Scholar] [CrossRef]
- Cui, T.; Yang, L.; Han, X.; Xu, J.; Yang, Y.; Ren, T. A Low-Cost, Portable, and Wireless In-Shoe System Based on a Flexible Porous Graphene Pressure Sensor. Materials 2021, 14, 6475. [Google Scholar] [CrossRef]
- Tee, K.S.; Javahar, Y.S.H.; Saim, H.; Zakaria, W.N.W.; Khialdin, S.B.M.; Isa, H.; Awad, M.I.; Soon, C.F. A Portable Insole Pressure Mapping System. TELKOMNIKA Telecommun. Comput. Electron. Control 2017, 15, 1493–1500. [Google Scholar] [CrossRef]
- Skelly, M.M.; Chizeck, H.J. Real time gait event detection during FES paraplegic walking. Annu. Int. Conf. IEEE Eng. Med. Biol.-Proc. 1997, 5, 1934–1937. [Google Scholar] [CrossRef]
- Pappas, I.P.I.; Popovic, M.R.; Keller, T.; Dietz, V.; Morari, M. A reliable gait phase detection system. IEEE Trans. Neural Syst. Rehabil. Eng. 2001, 9, 113–125. [Google Scholar] [CrossRef]
- Pappas, I.P.I.; Keller, T.; Mangold, S. A Reliable, Gyroscope based Gait Phase Detection Sensor Embedded in a Shoe Insole. Proc. IEEE Sens. 2002, 1, 1085–1088. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, Y.L.; Xia, Y.; Wu, X.; Kirk, T.V.; Chen, X.D. A low-cost and highly integrated sensing insole for plantar pressure measurement. Sens. Bio-Sens. Res. 2019, 26, 100298. [Google Scholar] [CrossRef]
- ISO 9407:2019(en); Footwear Sizing—Mondopoint System of Sizing and Marking. International Organization for Standardization: Geneva, Switzerland, 2019. Available online: https://www.iso.org/obp/ui/#iso:std:iso:9407:ed-2:v1:en (accessed on 3 October 2022).
- Hunt, A.E.; Fahey, A.J.; Smith, R.M. Static measures of calcaneal deviation and arch angle as predictors of rearfoot motion during walking. Aust. J. Physiother. 2000, 46, 9–16. [Google Scholar] [CrossRef]
- Dzedzickis, A.; Sutinys, E.; Bucinskas, V.; Samukaite-Bubniene, U.; Jakstys, B.; Ramanavicius, A.; Morkvenaite-Vilkonciene, I. Polyethylene-Carbon Composite (Velostat®) Based Tactile Sensor. Polymers 2020, 12, 2905. [Google Scholar] [CrossRef]
- Standard Test Methods for Pressure-Sensitive Adhesive-Coated Tapes Used for Electrical and Electronic Applications. ASTM International: West Conshohocken, PA, USA, 2017. Available online: https://www.astm.org/d1000-17.html (accessed on 3 October 2022).
- Test Method Standard Electronic and Electrical Component Parts. Department of Defense: Arlington, VA, USA, 2002. Available online: https://nepp.nasa.gov/DocUploads/1F6AB74B-4517-4AD0-A34813268E75B8EB/MIL-STD-202.pdf (accessed on 3 October 2022).
- Hellstrand Tang, U.; Zügner, R.; Lisovskaja, V.; Karlsson, J.; Hagberg, K.; Tranberg, R. Comparison of plantar pressure in three types of insole given to patients with diabetes at risk of developing foot ulcers—A two-year, randomized trial. J. Clin. Transl. Endocrinol. 2014, 1, 121–132. [Google Scholar] [CrossRef] [Green Version]
- Viswanathan, V.; Madhavan, S.; Gnanasundaram, S.; Gopalakrishna, G.; Das, B.N.; Rajasekar, S.; Ramachandran, A. Effectiveness of Different Types of Footwear Insoles for the Diabetic Neuropathic FootA follow-up study. Diabetes Care 2004, 27, 474–477. [Google Scholar] [CrossRef] [Green Version]
- Tramonti, C.; Iacopi, E.; Cafalli, M.; Riitano, N.; Piaggesi, A.; Chisari, C. Type 2 diabetes mellitus and obesity: The synergistic effects on human locomotor function. Clin. Biomech. 2022, 100, 105759. [Google Scholar] [CrossRef]
- Hussein, M.K.; Saifalla, P.H. Estimation of insulin resistance and creatine kinase among Iraqi patients with type 2 diabetes mellitus. Eurasian Chem. Commun. 2022, 4, 1193–1200. [Google Scholar] [CrossRef]
- Puls, L.; Hauke, D.; Camathias, C.; Hügle, T.; Barg, A.; Valderrabano, V. Conservative Trio-Therapy for Varus Knee Osteoarthritis: A Prospective Case-Study. Medicina 2022, 58, 460. [Google Scholar] [CrossRef]
- Wang, Y.; Lu, Y.; Yao, J.; Yang, C.; Xu, W.; Wang, H. Differential analysis of plantar pressure parameters of lower limbs in stroke patients with different cerebral hemispheric injuries. Chin. J. Tissue Eng. Res. 2022, 26, 5646–5651. [Google Scholar] [CrossRef]
- Nemoto, K.I.; Gen-No, H.; Masuki, S.; Okazaki, K.; Nose, H. Effects of high-intensity interval walking training on physical fitness and blood pressure in middle-aged and older people. Mayo Clin. Proc. 2007, 82, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Baccelli, G.; Reggiani, P.; Mattioli, A.; Corbellini, E.; Garducci, S.; Catalano, M. The Exercise Pressor Reflex and Changes in Radial Arterial Pressure and Heart Rate During Walking in Patients with Arteriosclerosis Obliterans. Angiology 2016, 50, 361–374. [Google Scholar] [CrossRef]
- Basnet, S.; Maiya, A. Comparison of static plantar pressure in patients with diabetes and healthy individuals. J. Sci. Med. Sport. 2012, 15, S361. [Google Scholar] [CrossRef]
- Caravaggi, P.; Berti, L.; Leardini, A.; Lullini, G.; Marchesini, G.; Baccolini, L.; Giacomozzi, C. Biomechanical and functional alterations in the diabetic foot: Differences between type I and type II Diabetes. Gait Posture 2017, 57, 12–13. [Google Scholar] [CrossRef]
- Zimny, S.; Schatz, H.; Pfohl, M. The role of limited joint mobility in diabetic patients with an at-risk foot. Diabetes Care 2004, 27, 942–946. [Google Scholar] [CrossRef] [Green Version]
- Chanda, A.; Unnikrishnan, V. Novel insole design for diabetic foot ulcer management. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2018, 232, 1182–1195. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Mean | Standard Deviation | Standard Error Mean | |
|---|---|---|---|---|
| Age (years) | HC | 48.26 | 9.35 | 2.41 |
| D | 52.20 | 5.07 | 1.31 | |
| Weight (kg) | HC | 71.86 | 10.42 | 2.69 |
| D | 72.06 | 10.79 | 2.78 | |
| Pain Score | D | 5.92 | 0.89 | N/A |
| Duration of Diabetes (years) | D | 7.20 | 3.96 | N/A |
| Gait Phase | Group | Peak Plantar Pressure (kPa) during Walking | Location |
|---|---|---|---|
| Heel Strike | HC | 790.15 ± 35.45 | Medial Heel |
| 780.13 ± 15.77 | Lateral Heel | ||
| D | 850.46 ± 25.10 | Medial Heel | |
| 849.40 ± 15.85 | Lateral Heel | ||
| DC | 860.65 ± 18.47 | Lateral Heel | |
| 856.44 ± 17.56 | Medial Heel | ||
| Toe-off | HC | 790.00 ± 20.13 | Medial Forefoot |
| 788.70 ± 11.11 | Central Forefoot | ||
| 779.10 ± 10.47 | Lateral Forefoot | ||
| D | 850.14 ± 19.88 | Central Forefoot | |
| 850.00 ± 15.46 | Medial Forefoot | ||
| 849.14 ± 12.11 | Lateral Forefoot | ||
| DC | 863.64 ± 10.14 | Central Forefoot | |
| 860.00 ± 9.56 | Medial Forefoot | ||
| 859.00 ± 8.44 | Lateral Forefoot |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gupta, S.; Jayaraman, R.; Sidhu, S.S.; Malviya, A.; Chatterjee, S.; Chhikara, K.; Singh, G.; Chanda, A. Diabot: Development of a Diabetic Foot Pressure Tracking Device. J 2023, 6, 32-47. https://doi.org/10.3390/j6010003
Gupta S, Jayaraman R, Sidhu SS, Malviya A, Chatterjee S, Chhikara K, Singh G, Chanda A. Diabot: Development of a Diabetic Foot Pressure Tracking Device. J. 2023; 6(1):32-47. https://doi.org/10.3390/j6010003
Chicago/Turabian StyleGupta, Shubham, Rajan Jayaraman, Sarabjeet Singh Sidhu, Ayush Malviya, Subhodip Chatterjee, Komal Chhikara, Gurpreet Singh, and Arnab Chanda. 2023. "Diabot: Development of a Diabetic Foot Pressure Tracking Device" J 6, no. 1: 32-47. https://doi.org/10.3390/j6010003
APA StyleGupta, S., Jayaraman, R., Sidhu, S. S., Malviya, A., Chatterjee, S., Chhikara, K., Singh, G., & Chanda, A. (2023). Diabot: Development of a Diabetic Foot Pressure Tracking Device. J, 6(1), 32-47. https://doi.org/10.3390/j6010003