
Ethnobotanical Study of Traditional Medicinal Plants Used for the Treatment of Infectious Diseases by Local Communities in Traditional Authority (T/A) Mbelwa, Mzimba District, Northern Region, Malawi



Abstract
:1. Introduction
2. Materials and Methods
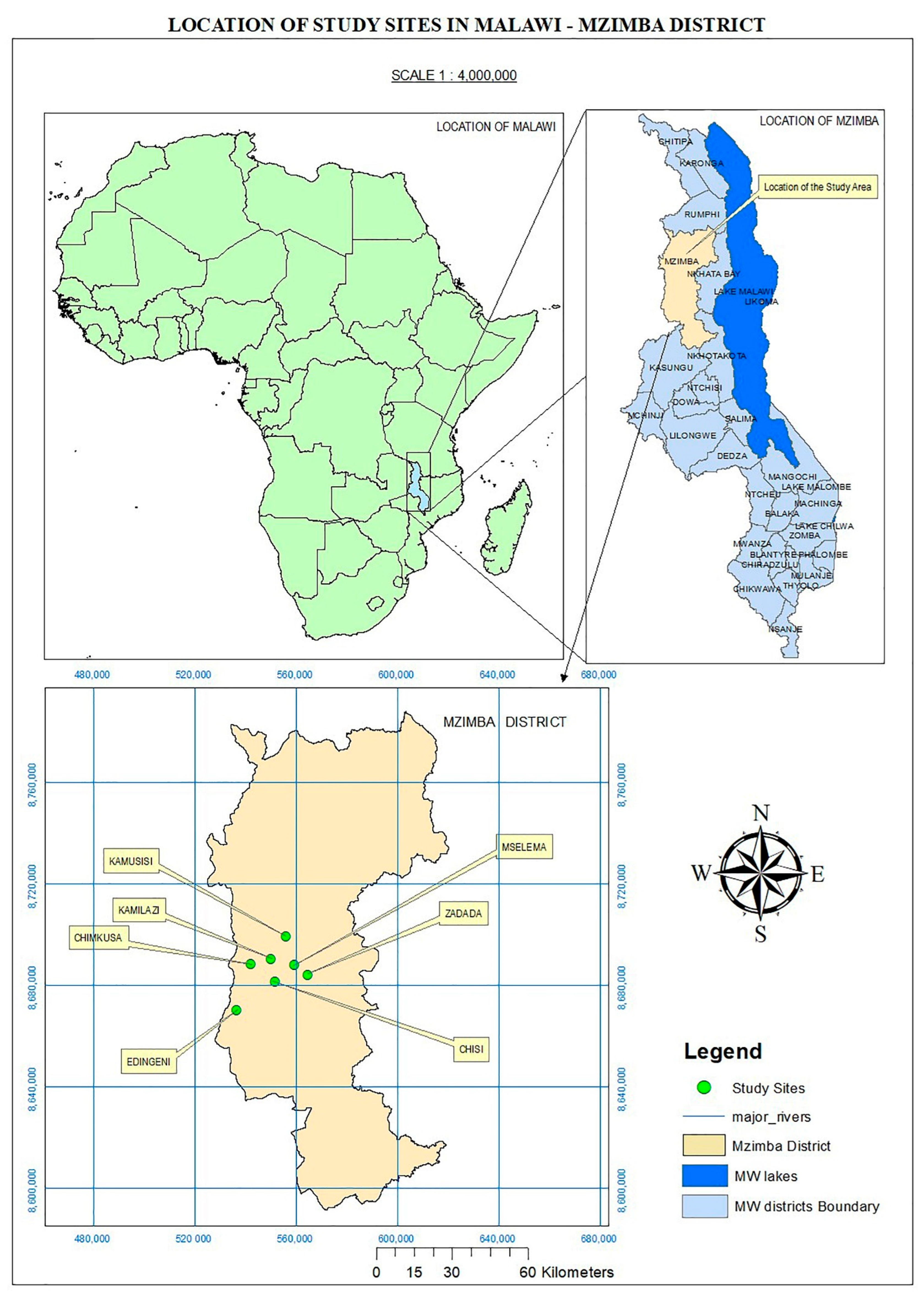
2.1. Study Area
2.2. Data Collection
Plant Collection
2.3. Statistical Analysis
2.3.1. Quantitative Ethnobotanical Indices
Use Value (UV)
Informant Consensus Factor (ICF)
Fidelity Level (FL)
Relative Frequency of Citation (RFC)
Relative Importance (RI) Value
3. Results
3.1. Demographic Data of the Respondents
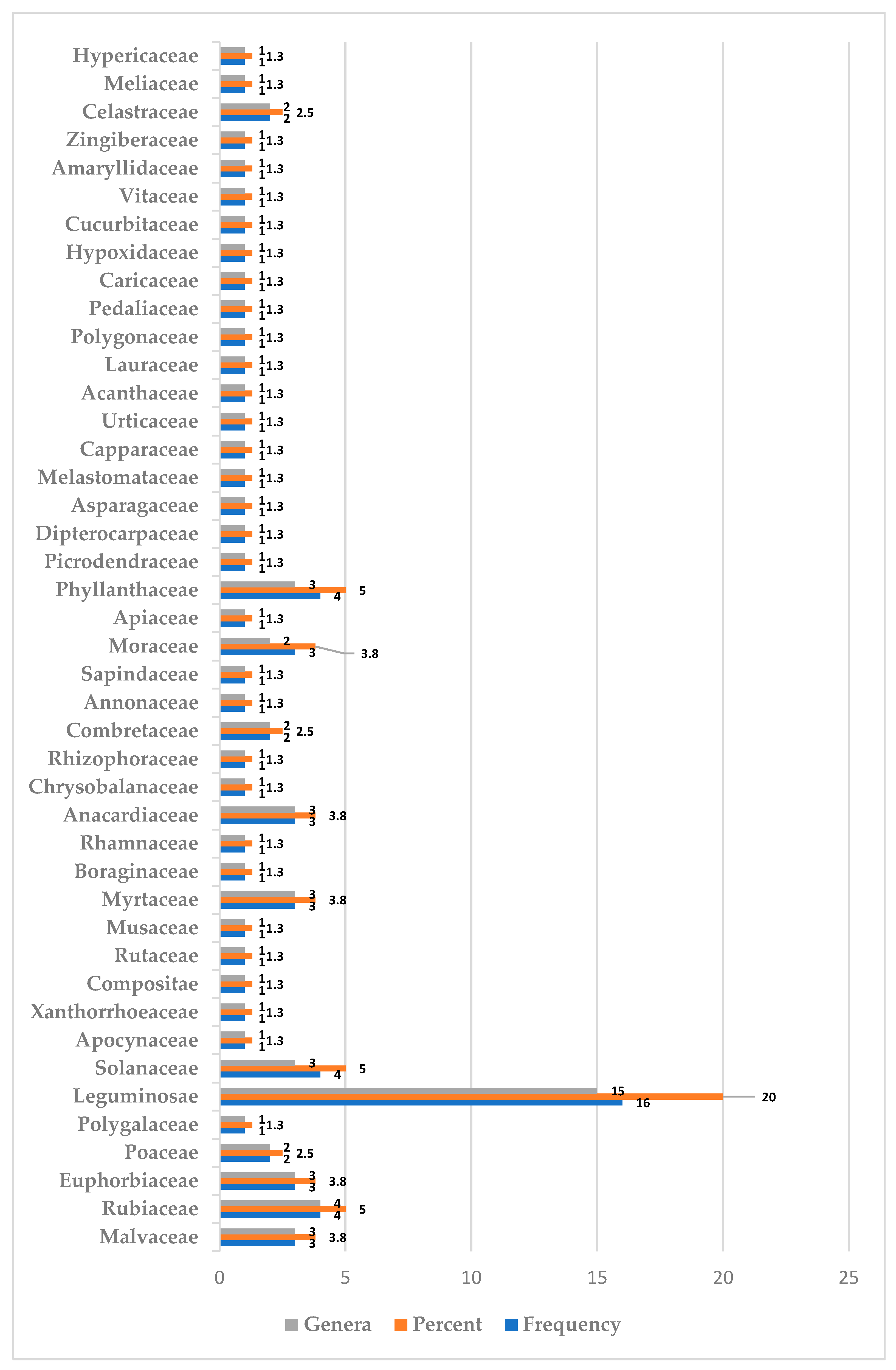
3.2. Diversity of Medicinal Plants in T/A Mbelwa, Mzimba District
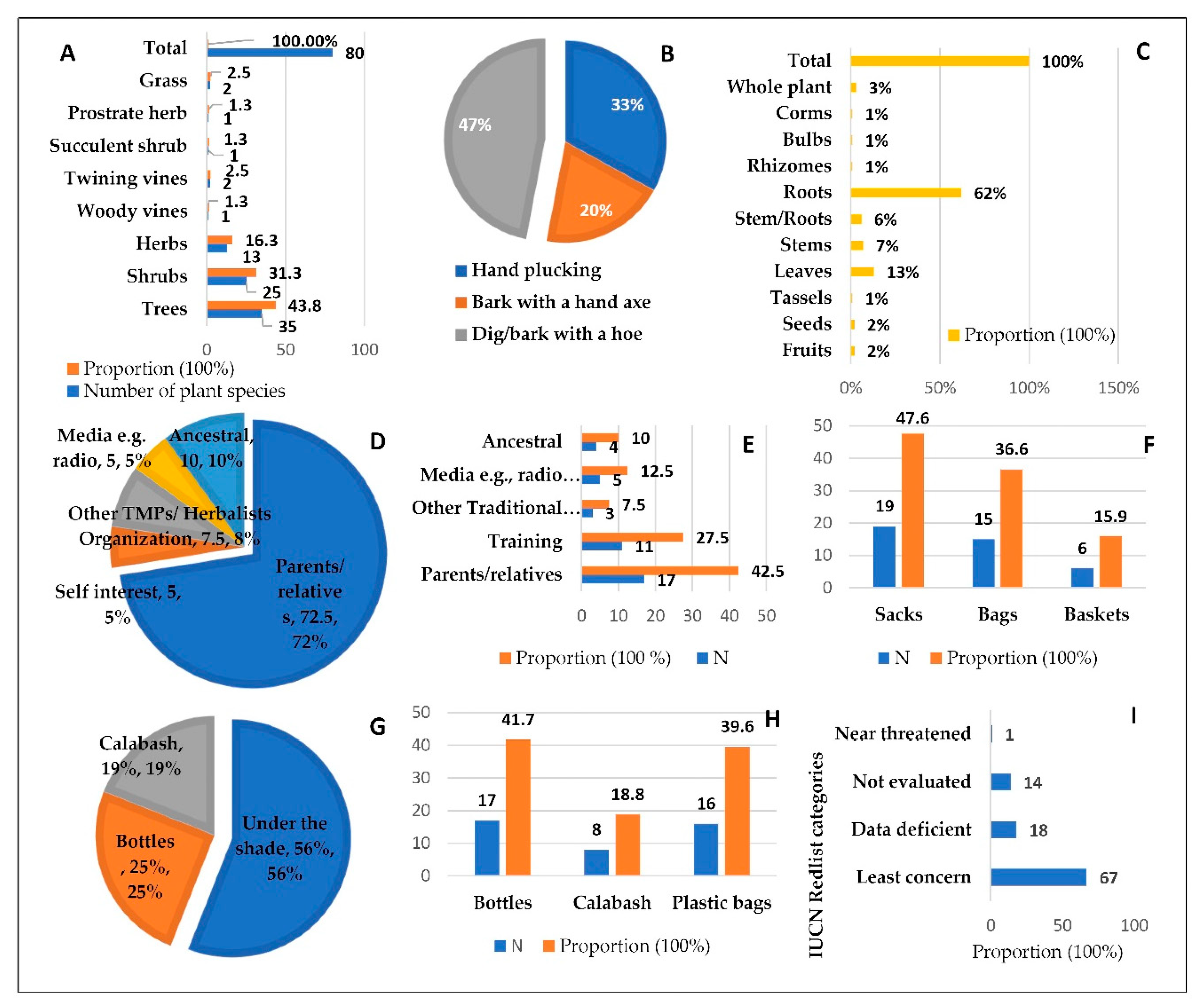
3.3. Medicinal Plants, Their Parts Used, and Collection/Harvesting Methods
3.4. Source of TK on Phytomedicines’ Use and Harvesting/Collection of Medicinal Plants
3.5. Transportation of Harvested/Collected MPs and Their Storage (Unprocessed and Processed)
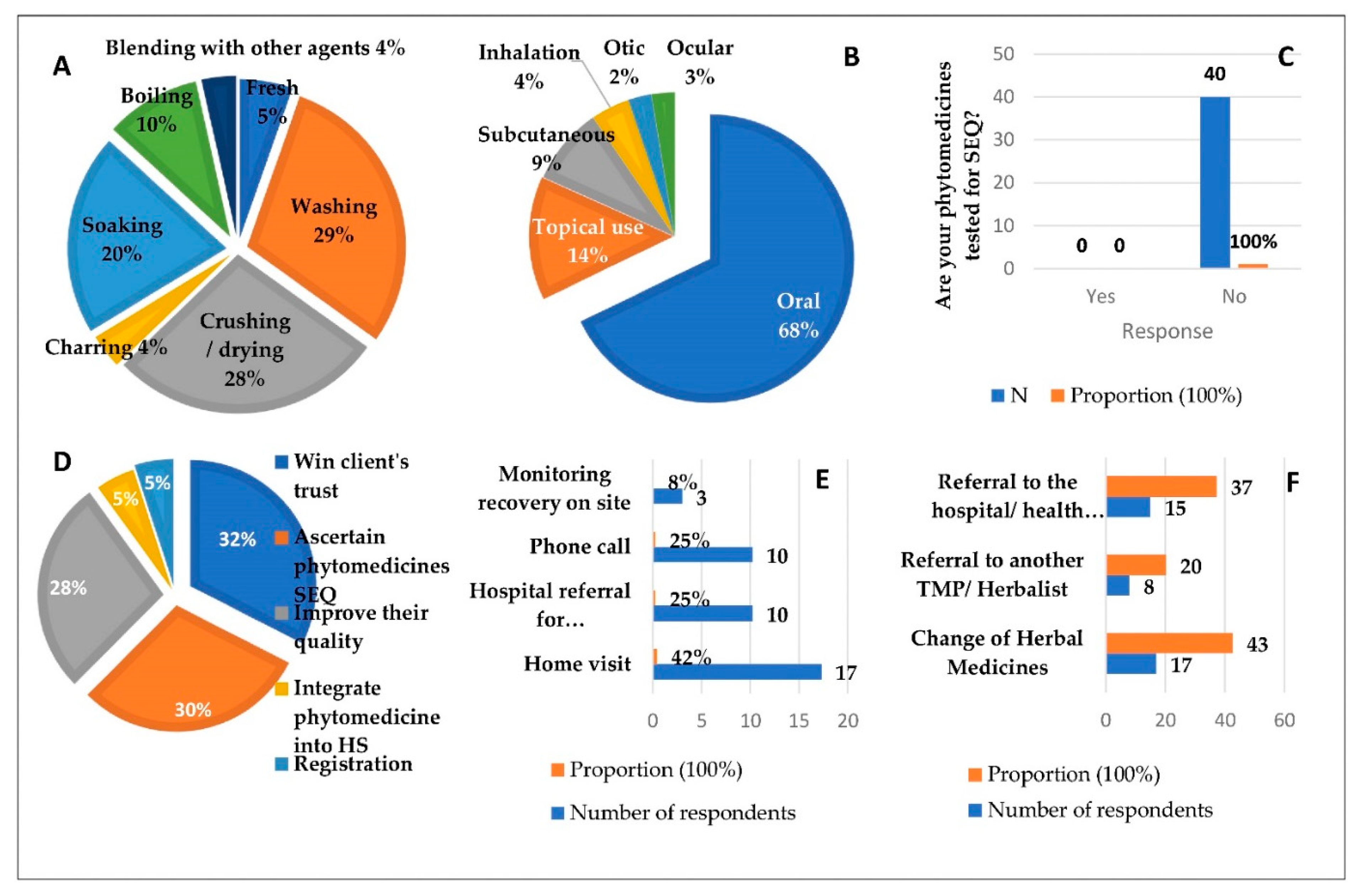
3.6. Method of Preparation of Medicinal Materials and Administration
3.7. Safety, Efficacy, and Quality (SEQ) Tests for Phytomedicines and Patient Recovery
3.8. Sources of Medicinal Plant Species and Their Conservation
3.9. Quantitative Indices
4. Discussion
4.1. Demographical Data of Participants
4.2. Diversity of Medicinal Plants in the T/A Mbelwa, Mzimba District
4.2.1. Medicinal Plant Parts Used and Collection/Harvesting Methods
4.2.2. Source of Traditional Knowledge (TK) on Phytomedicine Use and Harvesting/Collection of MPs
4.3. Preparation of Medicinal Materials and Administration
4.4. Transportation of Harvested/Collected MPs and Their Storage (Unprocessed and Processed)
4.5. Safety, Efficacy, and Quality (SEQ) Tests for Phytomedicines and Patient Recovery
4.6. Sources of Medicinal Plant Species and Their Threats
4.7. Quantitative Indices
4.7.1. Relative Frequency of Citation (RFC), Use Values (UVs), and Relative Importance (RI) Values
4.7.2. Informant Consensus Factors (ICFs) and Fidelity Levels (FLs)
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boutayeb, A. The Impact of Infectious Diseases on the Development of Africa. In Handbook of Disease Burdens and Quality of Life Measures; Springer: Berlin/Heidelberg, Germany, 2010; pp. 1171–1188. [Google Scholar] [CrossRef]
- World Health Organization. Mozambique Country Cooperation Strategy at a Glance, 3rd ed.; WHO: Geneva, Switzerland, 2008; pp. 154–196. Available online: http://apps.who.int/iris/bitstream/handle/10665/136935/ccsbrief_mwi_en.pdf?sequence=1 (accessed on 2 January 2021).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data WHO Coronavirus (COVID-19) Dashboard with Vaccination Data; World Health Organization: Geneva, Switzerland, 2021; Available online: https://covid19.who.int/%0Ahttps://covid19.who.int/region/searo/country/bd (accessed on 1 October 2021).
- WHO. Antimicrobial Resistance: Global Report on Surveillance. In WHO Library Cataloguing-in-Publication Data; WHO: Geneva, Switzerland, 2014; Available online: https://apps.who.int/iris/handle/10665/112642 (accessed on 15 January 2021).
- Makoka, M.H.; Miller, W.C.; Hoffman, I.F.; Cholera, R.; Gilligan, P.H.; Kamwendo, D.; Malunga, G.; Joaki, G.; Martinson, F.; Hosseinipour, M.C. Bacterial Infections in Lilongwe, Malawi: Aetiology and Antibiotic Resistance. BMC Infect. Dis. 2012, 12, 6–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musicha, P.; Cornick, J.E.; Bar-Zeev, N.; French, N.; Masesa, C.; Denis, B.; Kennedy, N.; Mallewa, J.; Gordon, M.A.; Msefula, C.L.; et al. Trends in Antimicrobial Resistance in Bloodstream Infection Isolates at a Large Urban Hospital in Malawi (1998–2016): A Surveillance Study. Lancet Infect. Dis. 2017, 17, 1042–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- M’Mbelwa District Council. M’Mbelwa District Council Socio Economic Profile 2017–2022; M’Mbelwa District Council: Mzimba, Malawi, 2017; pp. 1–211. Available online: https://global-uploads.webflow.com/6061a9d807f5368139d1c52c/610b12ffd09b837e524d4b18_Cleared-Mzimba-SEP-10-06-2018-v2.pdf (accessed on 2 January 2021).
- Doughari, J.H. Phytochemicals: Extraction Methods, Basic Structures and Mode of Action as Potential Chemotherapeutic Agents; INTECH Open Access Publisher: Rijeka, Croatia, 2014; pp. 1–32. [Google Scholar] [CrossRef] [Green Version]
- Ogbole, O.O.; Gbolade, A.A.; Ajaiyeoba, E.O. Ethnobotanical Survey of Plants Used in Treatment of Inflammatory Diseases in Ogun State of Nigeria. Eur. J. Sci. Res. 2010, 43, 183–191. Available online: https://www.researchgate.net/publication/288417018_Ethnobotanical_survey_of_plants_used_in_treatment_of_inflammatory_diseases_in_Ogun_State_of_Nigeria (accessed on 8 January 2023).
- Maliwichi-Nyirenda, C.P.; Maliwichi, L.L. Medicinal Plants Used for Contraception and Pregnancy-Related Cases in Malawi: A Case Study of Mulanje District. J. Med. Plants Res. 2010, 4, 2121–2127. [Google Scholar] [CrossRef]
- Chikowe, I.; Mnyenyembe, M.; Jere, S.; Mtewa, A.G.; Mponda, J.; Lampiao, F. An Ethnomedicinal Survey of Indigenous Knowledge on Medicinal Plants in the Traditional Authority Chikowi in Zomba, Malawi. Curr. Tradit. Med. 2019, 6, 225–241. [Google Scholar] [CrossRef]
- Maliwichi, C. The Conservation Biology of Berberis Hilstii Engl. in Nyika National Park, Malawi. Ph.D. Thesis, University of Plymouth, Plymouth, UK, 2008; pp. 1–259. Available online: https://pearl.plymouth.ac.uk/bitstream/handle/10026.1/1625/CECILIA%20PROMISE%20MALIWICHI%20NYIRENDA.PDF?sequence=1 (accessed on 17 January 2021).
- Neghabi-hajiagha, M.; Aliahmadi, A.; Taheri, M.R.; Ghassempour, A. A Bioassay-Guided Fractionation Scheme for Characterization of New Anti- Bacterial Compounds from Prosopis cineraria Aerial Parts. Iran. J. Microbiol. 2016, 8, 1. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4833735/pdf/IJM-8-1.pdf (accessed on 20 January 2021).
- Sonibare, M.A.; Abegunde, R.B. In Vitro Antimicrobial and Antioxidant Analysis of Dioscorea dumetorum (Kunth) Pax and Dioscorea hirtiflora (Linn.) and Their Bioactive Metabolites from Nigeria. J. Appl. Biosci. 2012, 51, 3583–3590. Available online: https://www.m.elewa.org/JABS/2012/51/4.pdf (accessed on 20 January 2021).
- Sonibare, M.; Abegunde, R. Ethnobotanical Study of Medicinal Plants Used by the Laniba Village People in South Western Nigeria. Afr. J. Microbiol. Res. 2012, 6, 1726–1732. [Google Scholar] [CrossRef]
- Oladele, A.T.; Alade, G.O.; Omobuwajo, O.R.; Medicine, H. Medicinal Plants Conservation and Cultivation by Traditional Medicine Practitioners (TMPs) in Aiyedaade Local Government Area of Osun State, Nigeria. Agric. Biol. J. N. Am. 2011, 2, 2151–7517. [Google Scholar] [CrossRef]
- Mwafongo, E.; Nordal, I.; Magombo, Z.; Stedje, B. Ethnobotanical Study of Hyacinthaceae and Geophytes in Selected Districts of Malawi. Ethnobot. Res. Appl. 2010, 8, 75–93. Available online: www.ethnobotanyjournal.org/vol8/i1547-3465-08-075.pdf (accessed on 21 January 2021). [CrossRef] [Green Version]
- Maliwichi, C.; Maliwichi, L.; Franco, M. Medicinal Uses of Berberis holstii Engl. (Berberidaceae) in Malawi, the Only African Endemic Barberry. J. Med. Plants Res. 2011, 5, 1367–1373. Available online: https://academicjournals.org/journal/JMPR/article-full-text-pdf/62F726C16697 (accessed on 2 February 2021).
- Bundschuh, T.V.; Hahn, K.; Wittig, R. The Medicinal Plants of the Woodlands in Northern Malawi (Karonga District). Flora Et Veg. Sudano-Sambesica 2011, 14, 3–8. Available online: https://d-nb.info/1097210375/34 (accessed on 22 January 2021). [CrossRef]
- Tembo, N.; Lampiao, F.; Mwakikunga, A.; Chikowe, I. Ethnobotanical Survey of Medicinal Plants Used for Cervical Cancer Management in Zomba District, Malawi. Sci. Afr. 2021, 13, e00941. [Google Scholar] [CrossRef]
- Mng’omba, S.A.; Akinnifesi, F.K.; Mkonda, A.; Mhango, J.; Chilanga, T.; Sileshi, G.; Ajayi, O.C. Ethnoecological Knowledge for Identifying Elite Phenotypes of the Indigenous Fruit Tree, Uapaca kirkiana in the Miombo Woodlands of Southern Africa. Agroecol. Sustain. Food Syst. 2015, 39, 399–415. [Google Scholar] [CrossRef]
- Manda, L. Status and Uses of Oldfieldia dactylophylla (Euphorbiaceae) in Malawi CBM MASTER THESES SERIES. Master’s Thesis, International Master Programme at the Swedish Biodiversity Centre, Uppsala, Sweden, 2007. No. 38. pp. 1–51. Available online: https://www.slu.se/globalassets/ew/org/centrb/cbm/dokument/publikationer-cbm/masteruppsatser/leonard-manda-thesis.pdf (accessed on 18 March 2022).
- Li, H.; Li, Z.; Zhang, X.; Yang, S.; Chen, C.; Yang, Q.; He, C. Ethnobiological Study on Traditional Medicinal Plants and Fungi Recorded in the Naxi Dongba Sutras. J. Ethnobiol. Ethnomed. 2021, 8, 32. [Google Scholar] [CrossRef]
- World Organization of Family Doctors (WONCA): International Classification of Primary Care. Available online: https://www.globalfamilydoctor.com/site/DefaultSite/filesystem/documents/Groups/WICC/International%20Classification%20of%20Primary%20Care%20Dec16.pdf (accessed on 18 April 2022).
- Mesfin, A.; Giday, M.; Animut, A.; Teklehaymanot, T. Ethnobotanical Study of Antimalarial Plants in Shinile District, Somali Region, Ethiopia, and in Vivo Evaluation of Selected Ones against Plasmodium berghei. J. Ethnopharmacol. 2012, 139, 221–227. [Google Scholar] [CrossRef]
- Al-Fatimi, M. Wild Edible Plants Traditionally Collected and Used in Southern Yemen. J. Ethnobiol. Ethnomed. 2021, 17, 49. [Google Scholar] [CrossRef]
- Hosseini, S.H.; Bibak, H.; Ghara, A.R.; Sahebkar, A.; Shakeri, A. Ethnobotany of the Medicinal Plants Used by the Ethnic Communities of Kerman Province, Southeast Iran. J. Ethnobiol. Ethnomed. 2021, 17, 31. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8082778/ (accessed on 18 November 2021). [CrossRef]
- Mootoosamy, A.; Fawzi Mahomoodally, M. Ethnomedicinal Application of Native Remedies Used against Diabetes and Related Complications in Mauritius. J. Ethnopharmacol. 2014, 151, 413–444. [Google Scholar] [CrossRef]
- Kayani, S.; Ahmad, M.; Sultana, S.; Khan, Z. Ethnobotany of Medicinal Plants among the Communities of Alpine and Sub- Alpine Regions of Pakistan Ethnobotany of Medicinal Plants among the Communities of Alpine and Sub-Alpine Regions of Pakistan. J. Ethnopharmacol. 2015, 164, 186–202. [Google Scholar] [CrossRef]
- Connelly, M.P.E.; Fabiano, E.; Patel, I.H.; Kinyanjui, S.M.; Mberu, E.K.; Watkins, W.M. Antimalarial Activity in Crude Extracts of Malawian Medicinal Plants. Ann. Trop. Med. Parasitol. 1996, 90, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Mongalo, N.I.; Mafoko, B.J. Cassia abbreviata Oliv. A Review of Its Ethnomedicinal Uses, Toxicology, Phytochemistry, Possible Propagation Techniques and Pharmacology. Afr. J. Pharm. Pharmacol. 2013, 7, 2901–2906. [Google Scholar] [CrossRef]
- Erasto, P.; Majinda, R. Bioactive Proanthocyanidins from the Root Bark of Cassia abbreviata. Int. J. Biol. Chem. Sci. 2011, 5, 2170. [Google Scholar] [CrossRef] [Green Version]
- Musila, M.F.; Dossaji, S.F.; Nguta, J.M.; Lukhoba, C.W.; Munyao, J.M. In Vivo Antimalarial Activity, Toxicity and Phytochemical Screening of Selected Antimalarial Plants. J. Ethnopharmacol. 2013, 146, 557–561. [Google Scholar] [CrossRef]
- Koudouvo, K.; Karou, D.S.; Kokou, K.; Essien, K.; Aklikokou, K.; Glitho, I.A.; Simpore, J.; Sanogo, R.; De Souza, C.; Gbeassor, M. An Ethnobotanical Study of Antimalarial Plants in Togo Maritime Region. J. Ethnopharmacol. 2011, 134, 183–190. [Google Scholar] [CrossRef]
- Stangeland, T.; Wangensteen, H.; Katuura, E.; Lye, K.A.; Paulsen, B.S. Antioxidant and Anti-Plasmodial Activity of Extracts from Three Ugandan Medicinal Plants. J. Med. Plants Res. 2010, 4, 1916–1923. [Google Scholar] [CrossRef]
- Nalule, S. In Vitro Anthelmintic Potential and Phytochemical Composition of Ethanolic and Aqueous Crude Extracts of Zanthoxylum chalybeum Engl. Afr. J. Pharm. Pharmacol. 2013, 7, 1604–1614. [Google Scholar] [CrossRef] [Green Version]
- Kiplagat, D.M.; Akala, H.M.; Liyala, P.O.; Wangui, J.M.; Odhiambo, R.A.O.; Omolo, J.O. Antiplasmodial Activity of Flavan Derivatives from Rootbark of Cassia abbreviata Oliv. J. Saudi Chem. Soc. 2016, 20, S140–S144. [Google Scholar] [CrossRef] [Green Version]
- Kiraithe, M.N.; Nguta, J.M.; Mbaria, J.M.; Kiama, S.G. Evaluation of the Use of Ocimum suave Willd. (Lamiaceae), Plectranthus barbatus Andrews (Lamiaceae) and Zanthoxylum chalybeum Engl. (Rutaceae) as Antimalarial Remedies in Kenyan Folk Medicine. J. Ethnopharmacol. 2016, 178, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Okagu, I.U.; Ndefo, J.C.; Aham, E.C.; Teodor, E. Zanthoxylum Species: A Review of Traditional Uses, Phytochemistry and Pharmacology in Relation to Cancer, Infectious Diseases and Sickle Cell Anemia. Front. Pharmacol. 2021, 12, 713090. [Google Scholar] [CrossRef] [PubMed]
- Anza, M. A Coniferyl Alcohol Derivative from the Roots of Zanthoxylum chalybeum. J. Coast. Life Med. 2014, 2, 970–974. [Google Scholar] [CrossRef]
- Nguta, J.; Kiraithe, M. In Vitro Antimicrobial Activity of Aqueous Extracts of Ocimum willd, Plectranthus barbatus Andrews and Zanthoxylum chalybeum Engl. against Selected Pathogenic Bacteria. Biomed. Biotechnol. Res. J. 2019, 3, 30. [Google Scholar] [CrossRef]
- Chikowe, I.; Mtewa, A.G.; Tembo, D.; Smith, D.; Ibrahim, E.; Mwamatope, B.; Nkhungulu, J.; Kumpalume, P.; Maroyi, A. Potential of Malawi’s Medicinal Plants in Covid-19 Disease Management: A Review. Malawi Med. J. 2021, 33, 85–107. [Google Scholar] [CrossRef] [PubMed]
- Priyadarshi, A.; Ram, B. A Review on Pharmacognosy and Pharmacological Activity of Carica papaya (Linn.) Leaf. Int. J. Pharm. Sci. Res. 2018, 9, 4071–4078. [Google Scholar] [CrossRef]
- Saeed, F.; Arshad, M.U.; Pasha, I.; Naz, R.; Batool, R.; Khan, A.A.; Nasir, M.A.; Shafique, B. Nutritional and Phyto-Therapeutic Potential of Papaya (Carica papaya Linn.): An Overview. Int. J. Food. Prop. 2014, 17, 1637–1653. [Google Scholar] [CrossRef]
- Semenya, S.S.; Maroyi, A. Ethnobotanical Survey of Plants Used by Bapedi Traditional Healers to Treat Tuberculosis and Its Opportunistic Infections in the Limpopo Province, South Africa. S. Afr. J. Bot. 2019, 122, 401–421. [Google Scholar] [CrossRef]
- Khadka, D.; Dhamala, M.K.; Li, F.; Aryal, P.C.; Magar, P.R.; Bhatta, S.; Thakur, M.S.; Basnet, A.; Cui, D.; Shi, S. The Use of Medicinal Plants to Prevent COVID-19 in Nepal. J. Ethnobiol. Ethnomed. 2021, 17, 26. [Google Scholar] [CrossRef]
- Mongalo, N.I.; Mashele, S.S.; Makhafola, T.J. Ziziphus mucronata Willd. (Rhamnaceae): It’s Botany, Toxicity, Phytochemistry and Pharmacological Activities. Heliyon 2020, 6, e03708. [Google Scholar] [CrossRef] [PubMed]
- Chinsembu, K.C. Ethnobotanical Study of Plants Used in the Management of HIV/AIDS-Related Diseases in Livingstone, Southern Province, Zambia. Evid.-Based Complement. Altern. Med. 2016, 2016, 4238625. [Google Scholar] [CrossRef] [Green Version]
- Kumar, G.; Karthik, L.; Bhaskara Rao, K.V. A Review on Pharmacological and Phytochemical Properties of Zingiber officinale Roscoe (Zingiberaceae). J. Pharm. Res. 2011, 4, 2963–2966. Available online: https://nupo.com/en/wp-content/uploads/sites/37/2020/03/A-review-on-Pharmacological-and-Phytochemical-properties-of-Zingiber-officinale-Roscoe.pdf (accessed on 20 June 2022).
- Raja, W.; Pandey, S.; Hanfi, S.; Khan, A.; Author, C. Evaluation of Antibacterial and Anticough Forming Effects of Zingiber officinale Extract. Int. J. Chem. Pharm. Res. 2012, 1, 141–147. Available online: https://www.researchgate.net/publication/265339103_Evaluation_of_Antibacterial_and_Anticough_Forming_Effects_of_Zingiber_officinale_Extract/link/540961830cf2718acd3d0966/download (accessed on 24 June 2022).
- Ghareeb, M.A.; Habib, M.R.; Mossalem, H.S.; Abdel-Aziz, M.S. Phytochemical Analysis of Eucalyptus camaldulensis Leaves Extracts and Testing Its Antimicrobial and Schistosomicidal Activities. Bull. Natl. Res. Cent. 2018, 42, 16. [Google Scholar] [CrossRef] [Green Version]
- El Maaiden, E.; El Kharrassi, Y.; Qarah, N.A.S.; Essamadi, A.K.; Moustaid, K.; Nasser, B. Genus Ziziphus: A Comprehensive Review on Ethnopharmacological, Phytochemical and Pharmacological Properties; Elsevier B.V.: Amsterdam, The Netherlands, 2020; Volume 259. [Google Scholar] [CrossRef]
- Nyaberi, M.O.; Onyango, C.A.; Mathooko, F.M.; Maina, J.M.; Makobe, M.; Mwaura, F. Evaluation of Phytochemical, Antioxidant and Antibacterial Activity of Edible Fruit Extracts of Ziziphus abyssinica A. Rich. J. Anim. Plant Sci. 2010, 6, 623–629. Available online: https://www.m.elewa.org/JAPS/2010/6.2/2.pdf (accessed on 8 January 2023).
- Ncube, B.; Ndhlala, A.R.; Okem, A.; Van Staden, J. Hypoxis (Hypoxidaceae) in African Traditional Medicine. J. Ethnopharmacol. 2013, 150, 818–827. [Google Scholar] [CrossRef]
- Msonthi, J.; Hostettmann, K.; Maillard, M. Phytochemical Studies of Medicinal Plants from Malawi. In Chemistry, Biological and Pharmacological Properties of African Medicinal Plants; University of Zimbabwe Publications: Harare, Zimbabwe, 1996; Available online: https://opendocs.ids.ac.uk/opendocs/bitstream/handle/20.500.12413/10199/Msonthi%2C%20JD%2C%20Hostettman%2CK%26Millard%2CM%20Phytochemical%20studies%20of%20medicinal%20plants%20%28book%20chapter%29.pdf?sequence=1 (accessed on 15 July 2022).
- Nicoletti, M.; Galeffi, C.; Messana, L.; Marini-Bettolo, G.B. Hypoxidaceae. Medicinal Uses and the Norlignan Constituents. J. Ethnopharmacol. 1992, 36, 95–101. [Google Scholar] [CrossRef]
- Betto, P.; Gabriele, R.; Galeffi, C. Determination of the Norlignan Glucosides of Hypoxidaceae by High-Performance Liquid Chromatography. J. Chromatogr. A 1992, 594, 131–135. [Google Scholar] [CrossRef]
- Maroyi, A. Review of Pharmacological Properties, Phytochemistry and Medicinal Uses of Baccharoides adoensis. J. Pharm. Nutr. Sci. 2020, 10, 205–212. [Google Scholar] [CrossRef]
- Liu, Y.; Abreu, P.J.M. Long Chain Alkyl and Alkenyl Phenols from the Roots of Ozoroa insignis. J. Braz. Chem. Soc. 2006, 17, 527–532. [Google Scholar] [CrossRef]
- Ahmed, A.S.; Mcgaw, L.J.; Moodley, N.; Naidoo, V.; Eloff, J.N. Cytotoxic, Antimicrobial, Antioxidant, Antilipoxygenase Activities and Phenolic Composition of Ozoroa and Searsia Species (Anacardiaceae) Used in South African Traditional Medicine for Treating Diarrhoea. S. Afr. J. Bot. 2014, 95, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Pare, D.; Hilou, A.; Ouedraogo, N.; Guenne, S. Ethnobotanical Study of Medicinal Plants Used as Anti-Obesity Remedies in the Nomad and Hunter Communities of Burkina Faso. Medicines 2016, 3, 9. [Google Scholar] [CrossRef] [Green Version]
- Subhan, N.; Burrows, G.E.; Kerr, P.G.; Obied, H.K. Phytochemistry, Ethnomedicine, and Pharmacology of Acacia, 1st ed.; Elsevier B.V.: Amsterdam, The Netherlands, 2018; Volume 57. [Google Scholar] [CrossRef]
- Adamu, H.M.; Ushie, O.A.; Lawal, D.S.; Oga, I.A. Phytochemical Screening of Fruit of Azanza garckeana and Root of Acacia macrothyrsa. Int. J. Tradit. Nat. Med. 2013, 3, 19–25. Available online: https://modernscientificpress.com/journals/ViewArticle.aspx?+Mc3krJiu0rRKsgS85dvRbjjVupRxbkOBBaFWBeQCaDDZP55j7kEct9b27jrJ0/RLDn1CTXtpaJ8A30t9u0bcw== (accessed on 2 August 2022).
- Coulibaly, A.Y.; Alexandre, P.; Djifaby, E.; Hashim, R.; Sulaiman, S.F.; Sulaiman, O.; Zuin, L.; Ang, P.; Kiendrebéogo, M.; Nacoulma, O.G. GC-MS Analysis and Antibacterial Activities of Feretia apodanthera Del. (Rubiaceae) and Ozoroa insignis Del. J. Dis. Med. Plants 2019, 5, 52–59. [Google Scholar] [CrossRef]
- Moshi, M.J.; Mbwambo, Z.H. Experience of Tanzanian Traditional Healers in the Management of Non-Insulin Dependent Diabetes Mellitus Experience of Tanzanian Traditional Healers in the Management of Non-Insulin Dependent Diabetes Mellitus. Pharm. Biol. 2002, 40, 552–560. [Google Scholar] [CrossRef]
- Omwenga, E.O.; Hensel, A.; Shitandi, A.; Goycoolea, F.M. Ethnobotanical Survey of Traditionally Used Medicinal Plants for Infections of Skin, Gastrointestinal Tract, Urinary Tract and the Oral Cavity in Borabu Sub-County, Nyamira County, Kenya. J. Ethnopharmacol. 2015, 176, 508–514. [Google Scholar] [CrossRef]
- Machaba, T.C.; Mahlo, S.M. Antifungal Activity of Medicinal Plants Used Traditionally for the Treatment of Fungal Infections and Related Ailments in South Africa. Int. J. Pharmacol. Pharm. Sci. 2017, 11, 395–400. [Google Scholar] [CrossRef]
- El-Seedi, H.R.; El-Shabasy, R.; Sakr, H.; Zayed, M.; El-Said, A.M.A.; Helmy, K.M.H.; Gaara, A.H.M.; Turki, Z.; Azeem, M.; Ahmed, A.M.; et al. Anti-Schistosomiasis Triterpene Glycoside from the Egyptian Medicinal Plant Asparagus Stipularis. Rev. Bras. Farmacogn. 2012, 22, 314–318. [Google Scholar] [CrossRef] [Green Version]
- Okello, S.V.; Nyunja, R.O.; Netondo, G.W.; Onyango, J.C. Ethnobotanical Study of Medicinal Plants Used by Sabaots of Mt. Elgon Kenya. Afr. J. Tradit. Complement. Altern. Med. 2010, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Maroyi, A. Zanha africana (Radlk.) Exell: Review of Its Botany, Medicinal Uses and Biological Activities. J. Pharm. Sci. Res. 2019, 11, 2980–2985. Available online: https://www.jpsr.pharmainfo.in/Documents/Volumes/vol11issue08/jpsr11081933.pdf (accessed on 23 August 2022).
- Stevenson, P.C.; Green, P.W.C.; Veitch, N.C.; Farrell, I.W.; Kusolwa, P.; Belmain, S.R. Nor-Hopanes from Zanha africana Root Bark with Toxicity to Bruchid Beetles. Phytochemistry 2016, 123, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Lans, C.A. Ethnomedicines Used in Trinidad and Tobago for Urinary Problems and Diabetes Mellitus. J. Ethnobiol. Ethnomed. 2006, 2, 45. [Google Scholar] [CrossRef] [Green Version]
- Solihah, M.A.; Rosli, W.W.I.; Nurhanan, A.R. Phytochemicals Screening and Total Phenolic Content of Malaysian Zea mays Hair Extracts. Int. Food Res. J. 2012, 19, 1533–1538. Available online: https://core.ac.uk/download/pdf/83541532.pdf (accessed on 26 August 2022).
- Wang, Q.; Zhao, L.; Gao, C.; Zhao, J.; Ren, Z.; Shen, Y.; Yao, R.; Yin, H. Ethnobotanical Study on Herbal Market at the Dragon Boat Festival of Chuanqing People in China. J. Ethnobiol. Ethnomed. 2021, 17, 19. [Google Scholar] [CrossRef]
- Novotna, B.; Polesny, Z.; Pinto-Basto, M.F.; Van Damme, P.; Pudil, P.; Mazancova, J.; Duarte, M.C. Medicinal Plants Used by ‘Root Doctors’, Local Traditional Healers in Bié Province, Angola. J. Ethnopharmacol. 2020, 260, 112662. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Guidelines on Good Agricultural and Collection Practices (GACP) for Medicinal Plants; WHO: Geneva, Switzerland, 2003; 80p, Available online: https://apps.who.int/iris/bitstream/handle/10665/42783/9241546271.pdf?sequence=1 (accessed on 8 January 2023).
- Chen, S.L.; Yu, H.; Luo, H.M.; Wu, Q.; Li, C.F.; Steinmetz, A. Conservation and Sustainable Use of Medicinal Plants: Problems, Progress, and Prospects. Chin. Med. 2016, 11, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozioma, J.E.; Chinwe, N.O. Herbal Medicines in African Traditional Medicine; Intech Open: London, UK, 2019; pp. 191–214. [Google Scholar] [CrossRef] [Green Version]
- CTA Technical Centre for Agricultural and Rural Co-operation. Medicinal Plants. WRENmedia 2007, 3, 1–43. Available online: https://core.ac.uk/download/pdf/132675062.pdf (accessed on 13 September 2022).
- Mozhui, L.; Kakati, L.N.; Meyer-Rochow, V.B. Entomotherapy: A Study of Medicinal Insects of Seven Ethnic Groups in Nagaland, North-East India. J. Ethnobiol. Ethnomed. 2021, 17, 17. [Google Scholar] [CrossRef] [PubMed]
- Das, K.; Tiwari, R.K.S.; Shrivastava, D.K. Techniques for Evaluation of Medicinal Plant Products as Antimicrobial Agent: Current Methods and Future Trends. J. Med. Plants 2010, 4, 104–111. [Google Scholar] [CrossRef]
- Nahashon, M. Conservation of Wild-Harvested Medicinal Plant Species in Tanzania. Exam. I Hållbar Utveckl. Master Thesis E, in Sustainable Development, Uppsala, Sweden. 2013, 24, 1–55. Available online: http://www.diva-portal.org/smash/get/diva2:615493/FULLTEXT01.pdf (accessed on 14 September 2022).
- WHO. WHO Expert Committee on Specifications for Pharmaceutical Preparations. In WHO Guidelines on Good Herbal Processing Practices for Herbal Medicines; WHO: Hong Kong, China, 2017; pp. 83–149. Available online: https://apps.who.int/iris/bitstream/handle/10665/272452/9789241210195-eng.pdf (accessed on 15 September 2022).
- WHO-AFRO. The African Health Monitor: African Traditional Medicine Day, 31 August; WHO-AFRO: Kano, Nigeria, 2010; pp. 1–104. Available online: https://www.afro.who.int/sites/default/files/2017-06/ahm-special-issue-14.pdf (accessed on 20 September 2022).
- Simwaka, A.; Peltzer, K.; Maluwa-Banda, D. Indigenous Healing Practices in Malawi. J. Psychol. Afr. 2007, 17, 155–161. [Google Scholar] [CrossRef]
- Meke, G.S.; Mumba, R.F.E.; Bwanali, R.J.; Williams, V.L. The Trade and Marketing of Traditional Medicines in Southern and Central Malawi. Int. J. Sustain. Dev. World Ecol. 2017, 24, 73–87. [Google Scholar] [CrossRef]
- Musa, M.S.; Abdelrasool, F.E.; Elsheikh, E.A.; Ahmed, L.A.M.N. Ethnobotanical Study of Medicinal Plants in the Blue Nile State, South-Eastern Sudan. J. Med. Plants Res. 2011, 5, 4287–4297. Available online: http://www.ethnopharmacologia.org/prelude2020/pdf/biblio-hm-52-musa.pdf (accessed on 27 September 2022).
- Anza, M.; Endale, M.; Cardona, L.; Cortes, D.; Eswaramoorthy, R.; Cabedo, N.; Abarca, B.; Zueco, J.; Rico, H.; Domingo-Ortí, I.; et al. Cytotoxicity, Antimicrobial Activity, Molecular Docking, Drug Likeness and Dft Analysis of Benzo[c]Phenanthridine Alkaloids from Roots of Zanthoxylum chalybeum. Biointerface Res. Appl. Chem. 2022, 12, 1569–1586. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Feature | Number (40) | Proportion (100%) |
|---|---|---|
| Age (years) | ||
| 30–39 | 6 | 15 |
| 40–49 | 10 | 25 |
| 50–59 | 3 | 7.5 |
| 60–69 | 14 | 35 |
| 70–79 | 4 | 10 |
| 80–89 | 3 | 7.5 |
| Gender | ||
| Male | 24 | 60 |
| Female | 16 | 40 |
| Marital status | ||
| Married | 35 | 87.5 |
| Divorced | 3 | 7.5 |
| Widowed | 2 | 5 |
| Education level | ||
| Primary | 37 | 92.5 |
| Secondary | 3 | 7.5 |
| Occupation | ||
| Traditional healers | 24 | 60 |
| Herbalists | 12 | 30 |
| Farmers | 4 | 10 |
| Years of experience | ||
| 0–4 | 2 | 5 |
| 5–9 | 7 | 17.5 |
| 10–14 | 5 | 12.5 |
| 15–19 | 8 | 20 |
| 20–24 | 2 | 5 |
| 25–29 | 2 | 5 |
| 30–34 | 5 | 12.5 |
| 35–39 | 2 | 5 |
| 40–44 | 4 | 10 |
| 45–49 | 2 | 5 |
| 50–54 | 1 | 2.5 |
| Monthly net income (MWK) | ||
| 0–10,000 | 7 | 17.5 |
| 10,001–20,000 | 5 | 12.5 |
| 20,001–30,000 | 4 | 10.0 |
| 30,001–40,000 | 1 | 2.5 |
| 40,001–50,000 | 1 | 2.5 |
| 50,001–60,000 | 9 | 22.5 |
| 60,001–70,000 | 2 | 5.0 |
| 70,001–80,000 | 1 | 2.5 |
| 80,001–90,000 | 4 | 10.0 |
| 90,001–10,000 | 2 | 5.0 |
| Over 100,000 | 4 | 10.0 |
| Family size (persons) | ||
| 1–10 | 33 | 82.5 |
| 11–20 | 6 | 15 |
| 21–30 | 1 | 2.5 |
| Location | Group village head | Village head |
| Chimkusa | Chanunkha (5) | Nehemiya (2) |
| Kasoti | ||
| Kadulila | ||
| Maolezimba | ||
| Kafoteka (7) | Kamatundu (5) | |
| Mgezuru | ||
| Mugeme | ||
| Chisi | Kazezani (5) | Zebediya (5) |
| Makamo | Mutajiri | |
| Zikoti | Muzgezge | |
| Zadada | Ndawandawa (2) | Nkuna (2) |
| Chunga | Mateyo | |
| Kamilazi | Yesaya (5) | Msimuko (5) |
| Edingeni | Jere (2) | Bascor |
| Phiri | ||
| Mselema | Mungoni (7) | Mungoni (7) |
| Kamusisi | Maluzu (3) | Sambo (2) |
| Ginyi | ||
| Kamzoli | Pandamayere | |
| Conservation Efforts of MPs | If Yes, A Conservation Effort by Govt/NGOs | N | Proportion |
|---|---|---|---|
| Yes (N = 17, 43%) | Provision of tree seedlings | 10 | 59 |
| Civic education/training on sustainable use of forest and their products | 7 | 41 | |
| If no, suggested MP conservation efforts | |||
| No (N = 23, 58%) | Afforestation and re-afforestation | 6 | 26 |
| Training local people on sustainable utilization of forests and their products | 6 | 26 | |
| Enforcing local laws through stiff punishments/fines | 6 | 26 | |
| Provision of incentives/alternative livelihood sources | 5 | 22 |
| Disease Category | ICF | Ailment | Preferred Species | FL (%) | Previous Citations | Pharmacological Activity | Phytochemistry |
|---|---|---|---|---|---|---|---|
| General and unspecified | 0.31 | Malaria | Cassia abbreviata Oliv. Zanthoxylum chalybeum Engl. | 100 100 | [30,31,32] [33,34,35,36] | Antiplasmodial, antioxidant, antimicrobial, and laxative activities [32,37] Antimalarial, trypanocidal, antimicrobial, and anti-helminthic activities [38,39] | 2,4-trans-7,40- dihydroxymethoxyflavan, flavan 2 derivative, and Cassinidin A and B [32,37] 2, 3-epoxy- 6,7-methylenedioxyconiferyl alcohol, dihydrochelerythrine, alkaloids, flavonoids, terpenoids, tannins, and anthraquinones [40,41] |
| Respiratory disorder | 0.53 | COVID-19 | Carica papaya L. | 94 | [42,43,44] | Antioxidant, immune-stimulating, expectorant, carminative, antimicrobial, and diuretic activities [44] | Phenolic compounds, carotenoids, alkaloids, quercetin, kaempferol, cyanogenic compounds, and benzyl glucosinolate [44] |
| Pneumonia | Zingiber officinale Roscoe Eucalyptus camaldulensis Dehnh Ziziphus abyssinica Hochnst. ex A. Rich. | 92 68 80 | [42,45,46] [42,45] [47,48] | Antioxidant, anticough, antimicrobial, anti-inflammatory, antidiabetic, and hepatoprotective activities [49,50] Antioxidant, antimicrobial, larvicidal, cytotoxic, -- pesticidal, and anti-dermatophyte [51] Antioxidant, antimicrobial, anti-inflammatory, antidiabetic, and antinociceptive [52,53] | Phenolic compounds, flavonoids, carbohydrates, proteins, alkaloids, glycosides, saponins, steroids, terpenoids, and tannins [49,50] Eucalyptanoic acid, flavonoids, acylated pentacyclic triterpenoids, and essential oils [51] Alkaloids, saponins, flavonoids and polyphenolics, tannins, sterols, and steroids [52,53] | ||
| Male or female genital/blood/blood-forming organs/immune mechanism | 0.02 | Syphilis | Cassia abbreviata Oliv | 85 | [31] | Antibacterial, antifungal, antioxidant, antimalarial, and anti-helminthic [31] | Anthocyanins, anthraquinones, polyphenols, tannins, and proanthocyanidins (Cassinidin A and Cassinidin B) [31] |
| Candidiasis | Hypoxis nyasica Baker | 80 | [54,55,56,57] | Antimicrobial, antioxidant, antiviral, and antidiabetic [55,56,57] | Mononyasines A and B, hypoxoside, nyasoside, nyasicoside, nyaside, and hypoxoside [55,56,57] | ||
| Skin | 0.20 | Ringworms | Hypoxis nyasica Baker | 86 | [35,58] | Antimicrobial, antioxidant, antiplasmodial, antitrypanosomal, antileishmanial, and anti-ulcer [58] | Alkaloids, flavonoids, free sugars, glycosides, phenols, proanthocyanidin, saponins, steroids, tannins, and terpenoids [35,58] |
| Digestive disorders | 0.19 | Diarrhoea Dysentery Helminths | Baccharoides adoensis (Sch.Bip. ex Walp.) H. Rob Ozoroa insignis Delile Cassia abbreviata Oliv. Oldfieldia dactylophylla (Welw. ex Oliv.) J.Léonard Acacia amythethophylla Steud.ex A.Rich | 95 96 85 100 90 | [35,58] [59,60,61] [31,32] [22] [62,63] | Antimicrobial, antioxidant, antiplasmodial, antitrypanosomal, antileishmanial, and anti-ulcer [58] Antimicrobial, anti-helminthic, antioxidant, cytotoxic, and anti-lipoxygenase [59,60,64] Antifungal, antibacterial, antioxidant, and antiplasmodial [31,32] - Anti-helminthic, antimicrobial, antioxidant, antiulcer, and hypoglycemic activities [62,63] | Alkaloids, flavonoids, free sugars, glycosides, phenols, proanthocyanidin, saponins, steroids, tannins, and terpenoids [35,58] Alkyl, alkenylphenols, essential oils, anacardic acid, and ginkgolic acid [59] 4-trans-7,40- dihydroxymethoxyflavan, flavan 2 derivative, Cassinidin A and B, and chelerythrine [31,32] - Flavonoids, terpenoids, tannins, cardiac glycosides, and saponins [62,63] |
| Eye | 0.25 | Conjunctivitis | Asparagus buchananii Baker | 75 | [65,66,67] | Antibacterial and anti-plasmodial activities [65,66,67] | Alkaloids, isoflavonoids, steroidal glycosides, triterpene saponin, and asparagalin A [68] |
| Musculoskeletal disorder/neurological disorder | 0.25 | Polio | Ziziphus abyssinica Hochst.ex A. Rich. | 85 | [47,69] | Antibacterial, antifungal, antiviral, antioxidant, and anti-mycobacterial [47] | Phenolic acids, flavonoids terpenoids, quinones, and peptide alkaloids [47] |
| Zanha africana (Raslk.) Exell | 86 | [70,71] | Anti-inflammatory, antimicrobial, antidiabetic, insecticidal, antitrypanosomal, and cytotoxic activities [70,71] | Zanhasaponins A, B, and C and nor-hopanes [70,71] | |||
| Urological disorders | 0.17 | Bilharzia | Zea mays L. | 90 | [72,73] | Antioxidant, anti-prostatitis, and anti-inflammatory activities [73] | Saponins, phlobatannins, phenols, proteins, vitamins, flavonoids, steroids, carbohydrates, and volatile components [73] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chisamile, W.A.; Sonibare, M.A.; Kamanula, J.F. Ethnobotanical Study of Traditional Medicinal Plants Used for the Treatment of Infectious Diseases by Local Communities in Traditional Authority (T/A) Mbelwa, Mzimba District, Northern Region, Malawi. J 2023, 6, 115-139. https://doi.org/10.3390/j6010009
Chisamile WA, Sonibare MA, Kamanula JF. Ethnobotanical Study of Traditional Medicinal Plants Used for the Treatment of Infectious Diseases by Local Communities in Traditional Authority (T/A) Mbelwa, Mzimba District, Northern Region, Malawi. J. 2023; 6(1):115-139. https://doi.org/10.3390/j6010009
Chicago/Turabian StyleChisamile, Wilfred A., Mubo A. Sonibare, and John F. Kamanula. 2023. "Ethnobotanical Study of Traditional Medicinal Plants Used for the Treatment of Infectious Diseases by Local Communities in Traditional Authority (T/A) Mbelwa, Mzimba District, Northern Region, Malawi" J 6, no. 1: 115-139. https://doi.org/10.3390/j6010009
APA StyleChisamile, W. A., Sonibare, M. A., & Kamanula, J. F. (2023). Ethnobotanical Study of Traditional Medicinal Plants Used for the Treatment of Infectious Diseases by Local Communities in Traditional Authority (T/A) Mbelwa, Mzimba District, Northern Region, Malawi. J, 6(1), 115-139. https://doi.org/10.3390/j6010009