
Trait Interindividual Differences in the Magnitude of Subjective Sleepiness from Sleep Inertia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
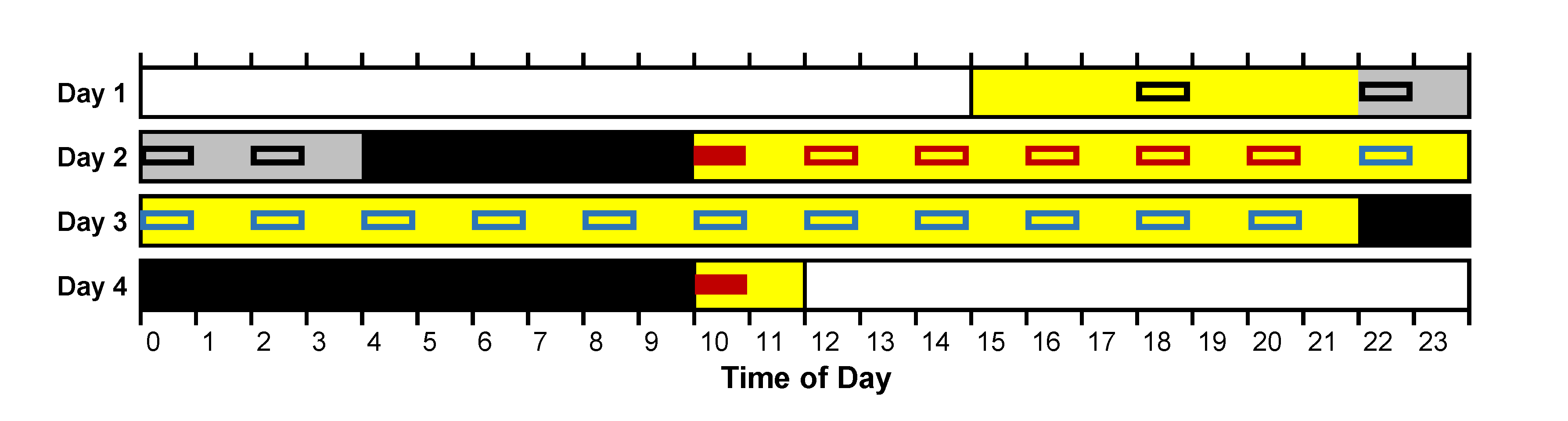
2.2. Experimental Design
2.3. Statistical Analyses
3. Results
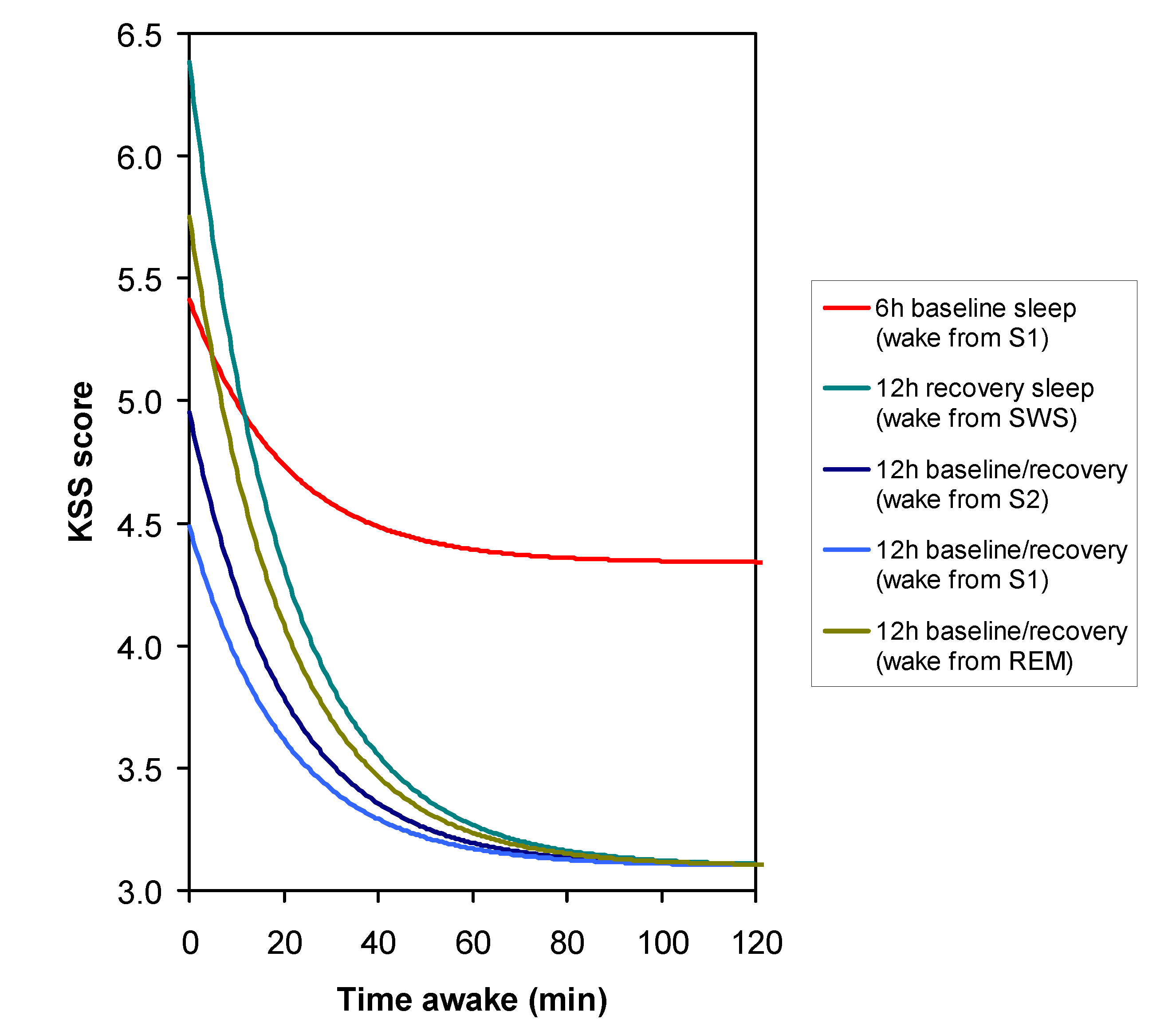
3.1. Sleep Stage at Awakening
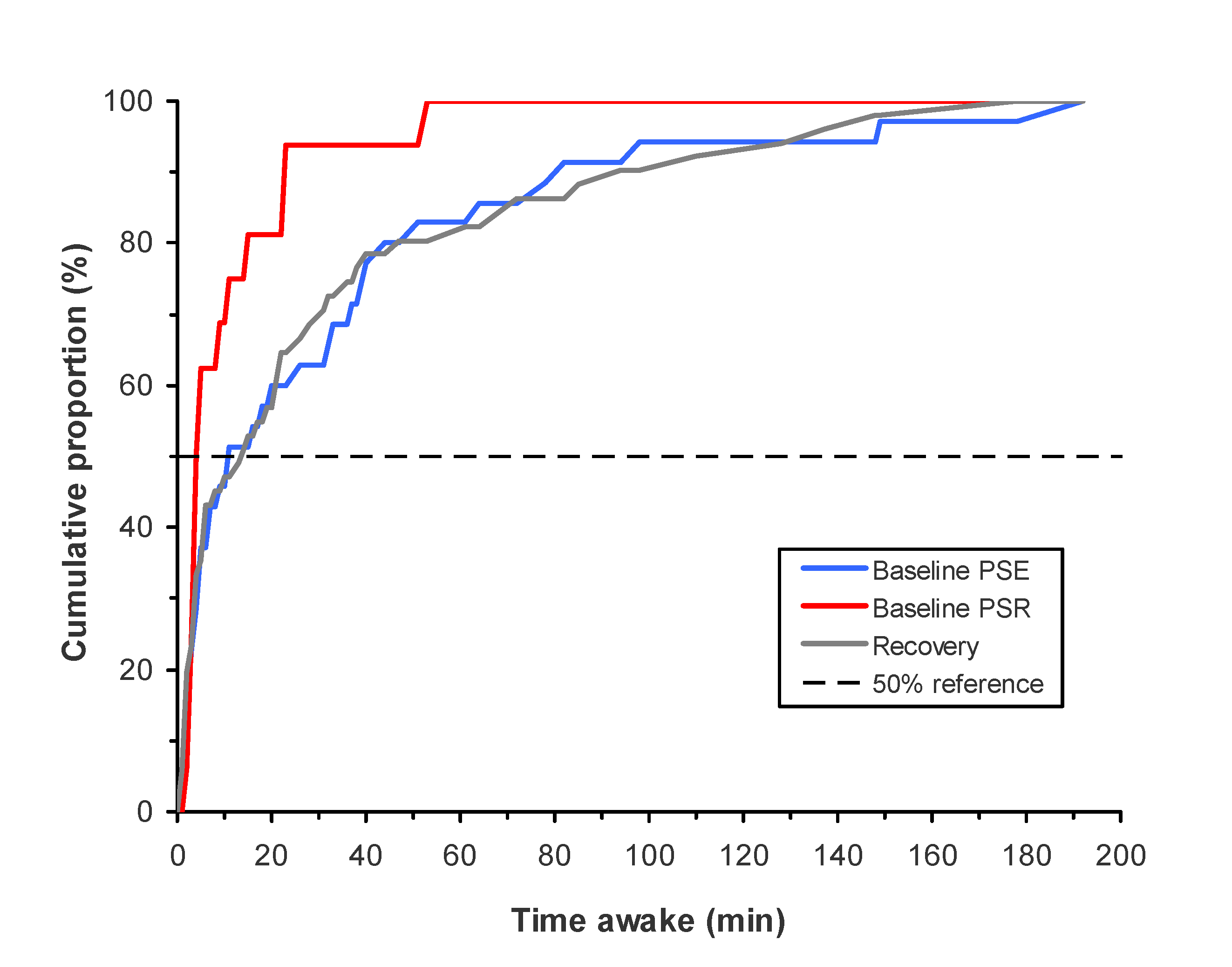
3.2. Time Awake at First KSS Administration
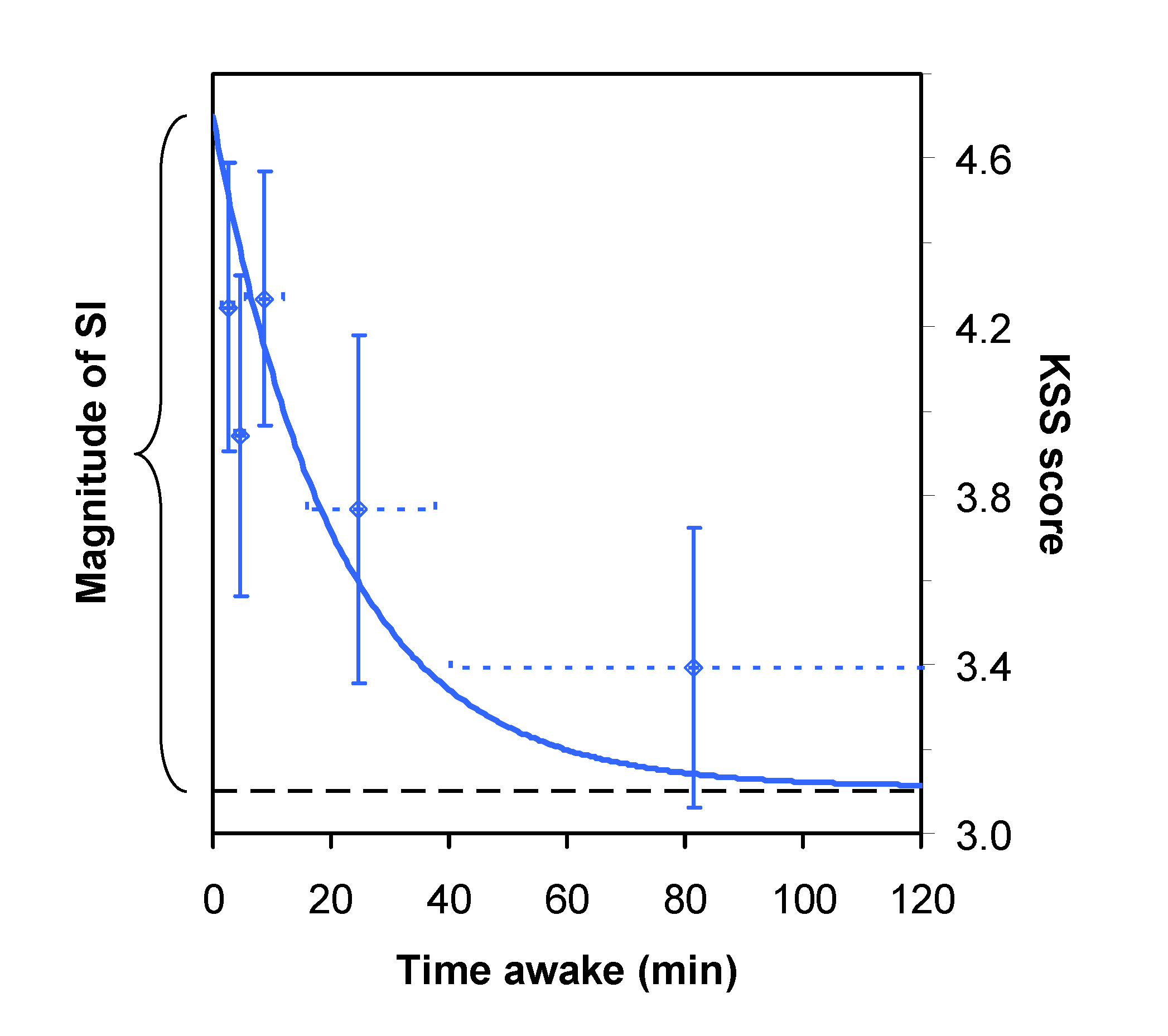
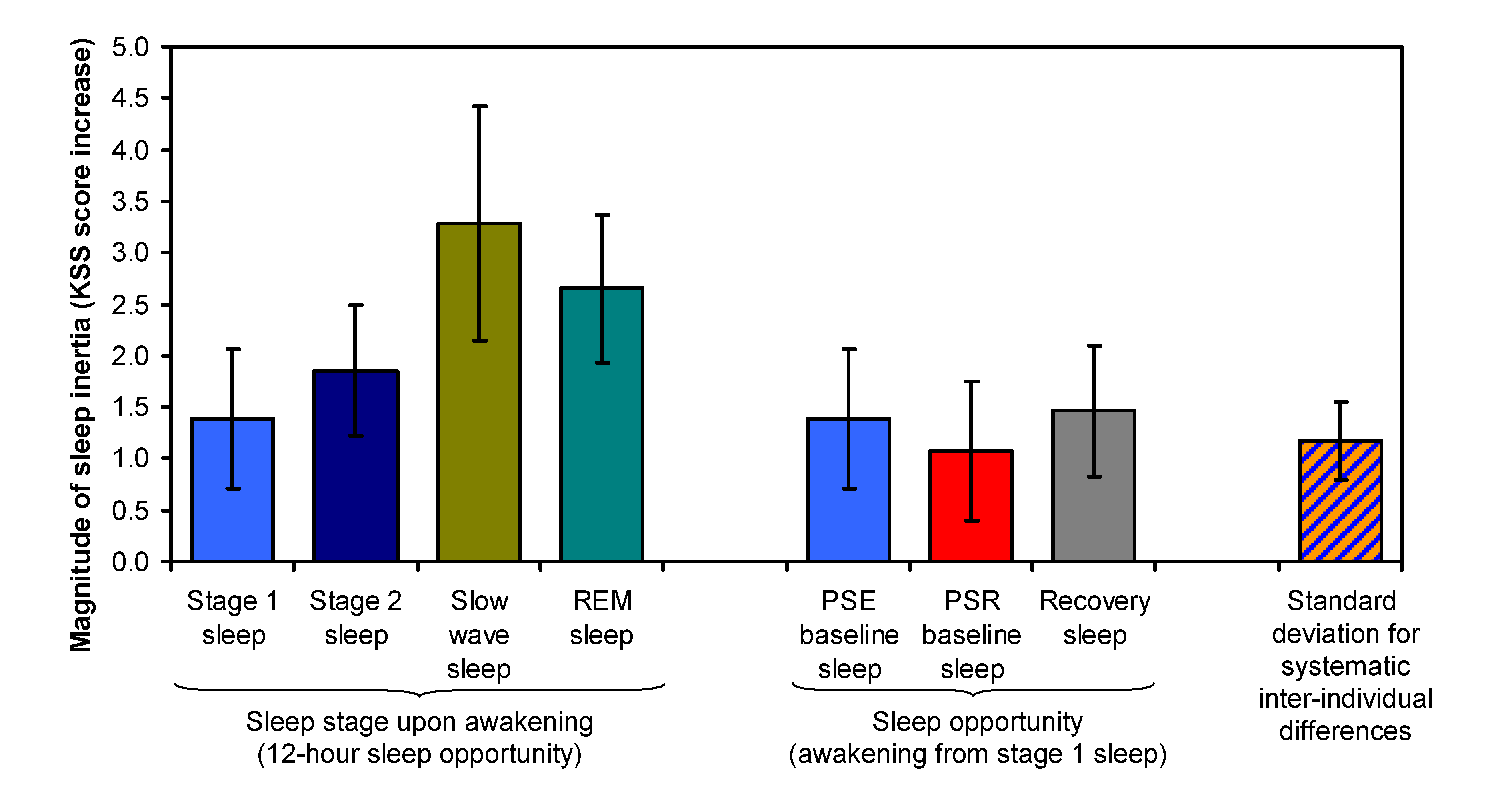
3.3. Magnitude of Sleep Inertia
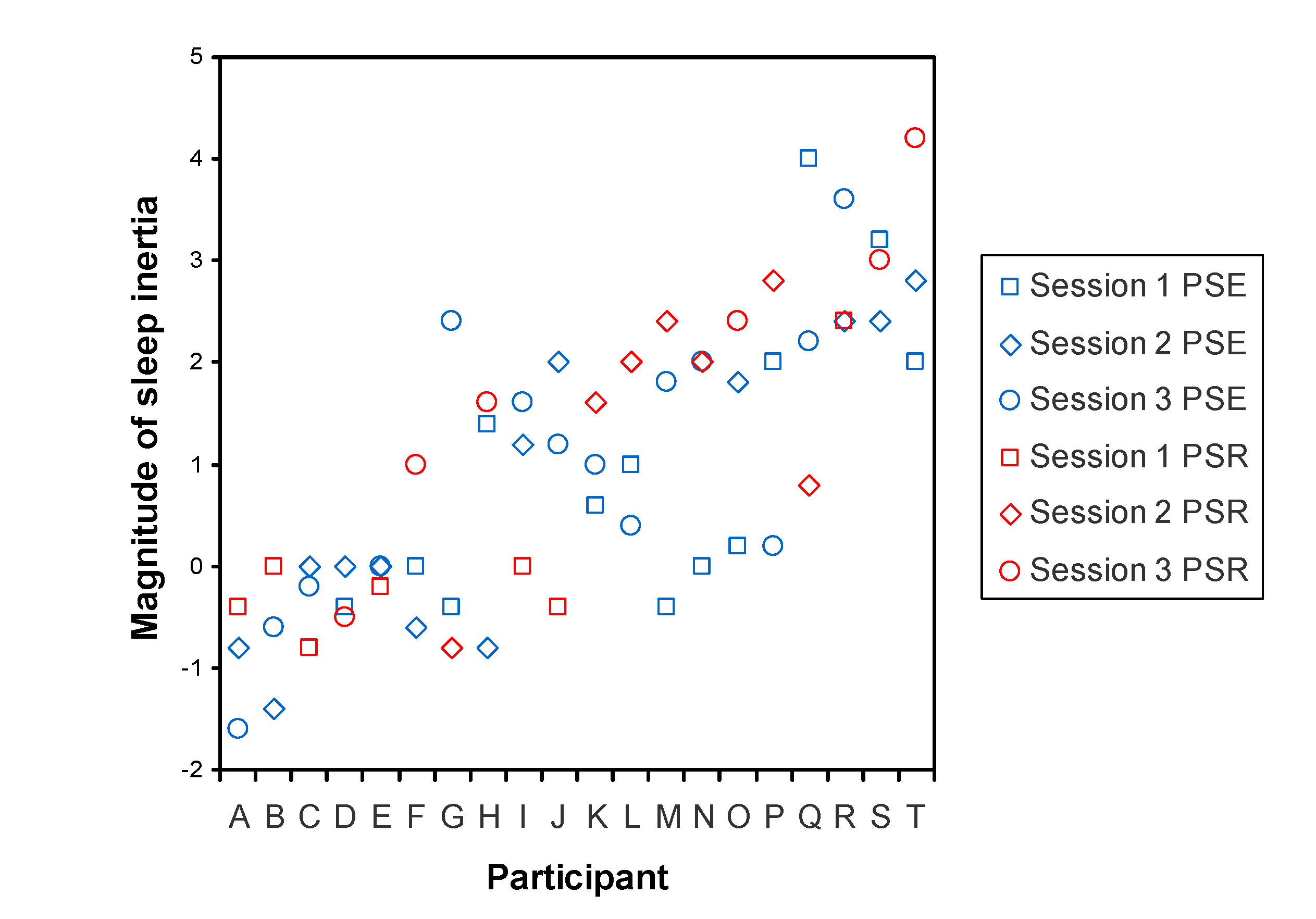
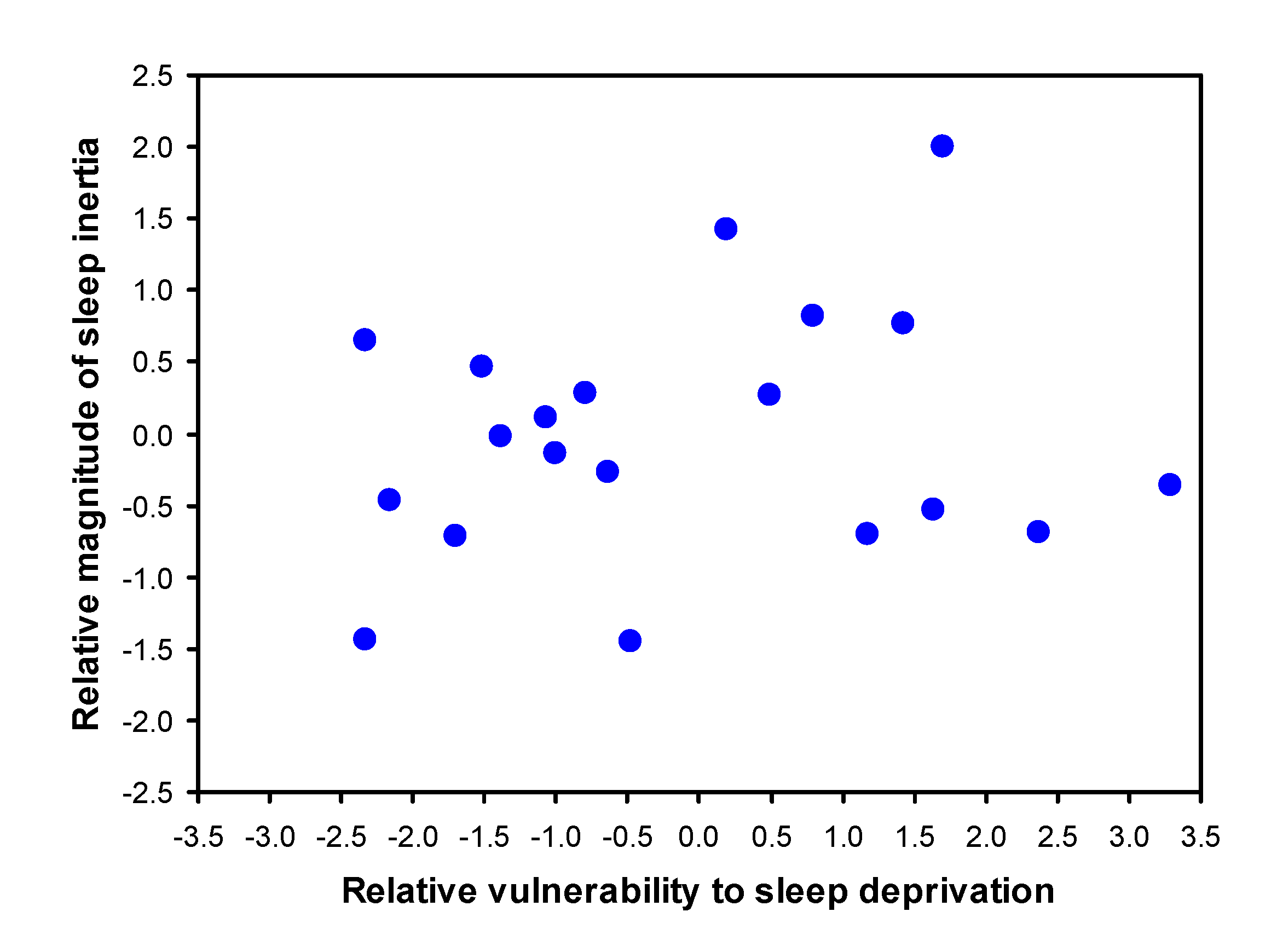
3.4. Trait Interindividual Differences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Åkerstedt, T. Sleepiness as a consequence of shift work. Sleep 1988, 11, 17–34. [Google Scholar] [CrossRef]
- Sallinen, M.; Härmä, M.; Mutanen, P.; Ranta, R.; Virkkala, J.; Müller, K. Sleepiness in various shift combinations of irregular shift systems. Ind. Health 2005, 43, 114–122. [Google Scholar] [CrossRef] [Green Version]
- Härmä, M. Individual differences in tolerance to shiftwork: A review. Ergonomics 1993, 36, 101–109. [Google Scholar] [CrossRef]
- Van Dongen, H.P.A. Shift work and inter-individual differences in sleep and sleepiness. Chronobiol. Int. 2006, 23, 1139–1147. [Google Scholar] [CrossRef]
- Kovac, K.; Vincent, G.E.; Jay, S.M.; Sprajcer, M.; Aisbett, B.; Lack, L.; Ferguson, S.A. The impact of anticipating a stressful task on sleep inertia when on-call. Appl. Ergon. 2020, 82, 102942. [Google Scholar] [CrossRef]
- Patterson, P.D.; Higgins, J.S.; Van Dongen, H.P.A.; Buysse, D.J.; Thackery, R.W.; Kupas, D.F.; Becker, D.S.; Dean, B.E.; Lindbeck, G.H.; Guyette, F.X.; et al. Evidence-based guidelines for fatigue risk management in emergency medical services. Prehospital Emerg. Care 2018, 22 (Suppl. 1), 89–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, M.; Riedy, S.M.; Himmel, M.; English, A.; Burton, J.; Albritton, S.; Johnson, K.; Morgan, P.; Van Dongen, H.P.A. Sleep quality, sleepiness and the influence of workplace breaks: A cross-sectional survey of health-care workers in two US hospitals. Chronobiol. Int. 2018, 35, 849–852. [Google Scholar] [CrossRef]
- Hilditch, C.J.; Short, M.; Van Dongen, H.P.A.; Centofanti, S.A.; Dorrian, J.; Kohler, M.; Banks, S. Sleep inertia during a simulated 6-h on/6-h off fixed split duty schedule. Chronobiol. Int. 2016, 33, 685–696. [Google Scholar] [CrossRef] [PubMed]
- Dinges, D.F. Are you awake? Cognitive performance and reverie during the hypnopompic state. In Sleep and Cognition; Bootzin, R.R., Kihlstrom, J.F., Schacter, D.L., Eds.; American Psychological Association: Washington, DC, USA, 2004; pp. 159–175. [Google Scholar]
- Ritchie, H.K.; Burke, T.M.; Dear, T.B.; McHill, A.W.; Axelsson, J.; Wright, K.P., Jr. Impact of sleep inertia on visual selective attention for rare targets and the influence of chronotype. J. Sleep Res. 2017, 26, 551–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tassi, P.; Muzet, A. Sleep inertia. Sleep Med. Rev. 2000, 4, 341–353. [Google Scholar] [CrossRef]
- Trotti, L.M. Waking up is the hardest thing I do all day: Sleep inertia and sleep drunkenness. Sleep Med. Rev. 2017, 35, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Hilditch, C.J.; McHill, A.W. Sleep inertia: Current insights. Nat. Sci. Sleep 2019, 11, 155–165. [Google Scholar] [CrossRef] [Green Version]
- Achermann, P.; Werth, E.; Dijk, D.J.; Borbély, A.A. Time course of sleep inertia after nighttime and daytime sleep episodes. Arch. Ital. Biol. 1995, 134, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Jewett, M.E.; Wyatt, J.K.; Ritz-De Cecco, A.; Khalsa, S.B.S.; Dijk, D.J.; Czeisler, C.A. Time course of sleep inertia dissipation in human performance and alertness. J. Sleep Res. 1999, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Dinges, D.F.; Orne, M.T.; Orne, E.C. Assessing performance upon abrupt awakening from naps during quasi-continuous operations. Behav. Res. Methods, Instrum. Comput. 1985, 17, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Burke, T.M.; Scheer, F.A.J.L.; Ronda, J.M.; Czeisler, C.A.; Wright, K.P., Jr. Sleep inertia, sleep homeostatic and circadian influences on higher-order cognitive functions. J. Sleep Res. 2015, 24, 364–371. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, J.M.; Van Dongen, H.P.A.; Dinges, D.F. Time of day and sleep inertia effects on cognitive performance and sleepiness during chronic sleep restriction. Sleep-Wake Res. Neth. 2005, 16, 75–78. [Google Scholar]
- McHill, A.W.; Hull, J.T.; Cohen, D.A.; Wang, W.; Czeisler, C.A.; Klerman, E.B. Chronic sleep restriction greatly magnifies performance decrements immediately after awakening. Sleep 2019, 42, zsz032. [Google Scholar] [CrossRef]
- Scheer, F.A.J.L.; Shea, T.J.; Hilton, M.F.; Shea, S.A. An endogenous circadian rhythm in sleep inertia results in greatest cognitive impairment upon awakening during the biological night. J. Biol. Rhythms 2008, 23, 353–361. [Google Scholar] [CrossRef] [Green Version]
- Rosa, R.R.; Bonnet, M.H. Sleep stages, auditory arousal threshold, and body temperature as predictors of behavior upon awakening. Int. J. Neurosci. 1985, 27, 73–83. [Google Scholar] [CrossRef]
- Cavallero, C.; Versace, F. Stage at awakening, sleep inertia, and performance. Sleep Res. Online 2003, 5, 89–97. [Google Scholar]
- Van Dongen, H.P.A.; Price, N.J.; Mullington, J.M.; Szuba, M.P.; Kapoor, S.C.; Dinges, D.F. Caffeine eliminates psychomotor vigilance deficits from sleep inertia. Sleep 2001, 24, 813–819. [Google Scholar] [CrossRef]
- Newman, R.A.; Kamimori, G.H.; Wesensten, N.J.; Picchioni, D.; Balkin, T.J. Caffeine gum minimizes sleep inertia. Percept. Mot. Ski. 2013, 116, 280–293. [Google Scholar] [CrossRef]
- Benington, J.H.; Heller, H.C. Restoration of brain energy metabolism as the function of sleep. Prog. Neurobiol. 1995, 45, 347–360. [Google Scholar] [CrossRef]
- Aeschbach, D.; Cajochen, C.; Landolt, H.P.; Borbély, A.A. Homeostatic sleep regulation in habitual short sleepers and long sleepers. Am. J. Physiol. Integr. Comp. Physiol. 1996, 270, R41–R53. [Google Scholar] [CrossRef]
- Tucker, A.M.; Dinges, D.F.; Van Dongen, H.P.A. Trait interindividual differences in the sleep physiology of healthy young adults. J. Sleep Res. 2007, 16, 170–180. [Google Scholar] [CrossRef]
- Van Dongen, H.P.A.; Baynard, M.D.; Maislin, G.; Dinges, D.F. Systematic interindividual differences in neurobehavioral impairment from sleep loss: Evidence of trait-like differential vulnerability. Sleep 2004, 27, 423–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Åkerstedt, T.; Anund, A.; Axelsson, J.; Kecklund, G. Subjective sleepiness is a sensitive indicator of insufficient sleep and impaired waking function. J. Sleep Res. 2014, 23, 240–252. [Google Scholar] [CrossRef] [PubMed]
- Van Dongen, H.P.A.; Maislin, G.; Dinges, D.F. Dealing with inter-individual differences in the temporal dynamics of fatigue and performance: Importance and techniques. Aviat. Space Environ. Med. 2004, 75, A147–A154. [Google Scholar] [PubMed]
- Smith, C.S.; Reilly, C.; Midkiff, K. Evaluation of three circadian rhythm questionnaires with suggestions for an improved measure of morningness. J. Appl. Psychol. 1989, 74, 728–738. [Google Scholar] [CrossRef]
- Rechtschaffen, A.; Kales, A. A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects; UCLA Brain Information Service: Los Angeles, CA, USA, 1968. [Google Scholar]
- Åkerstedt, T.; Gillberg, M. Subjective and objective sleepiness in the active individual. Int. J. Neurosci. 1990, 52, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Olofsen, E.; Dinges, D.F.; Van Dongen, H.P.A. Nonlinear mixed-effects modeling: Individualization and prediction. Aviat. Space Environ. Med. 2004, 75, A134–A140. [Google Scholar]
- Van Dongen, H.P.A.; Olofsen, E.; Dinges, D.F.; Maislin, G. Mixed-model regression analysis and dealing with interindividual differences. Methods Enzymol. 2004, 384, 139–171. [Google Scholar] [CrossRef]
- Rao, P.S.R.S. Variance Components Estimation: Mixed Models, Methodologies and Applications; Chapman and Hall/CRC: London, UK, 1997. [Google Scholar]
- Satterfield, B.C.; Stucky, B.; Landolt, H.P.; Van Dongen, H.P.A. Unraveling the genetic underpinnings of sleep deprivation-induced impairments in human cognition. Prog. Brain Res. 2019, 246, 127–158. [Google Scholar] [CrossRef]
- Arnal, P.J.; Sauvet, F.; Leger, D.; Van Beers, P.; Bayon, V.; Bougard, C.; Rabat, A.; Millet, G.Y.; Chennaoui, M. Benefits of sleep extension on sustained attention and sleep pressure before and during total sleep deprivation and recovery. Sleep 2015, 38, 1935–1943. [Google Scholar] [CrossRef]
- Watson, N.F.; Badr, M.S.; Belenky, G.; Bliwise, D.L.; Buxton, O.M.; Buysse, D.; Dinges, D.F.; Gangwisch, J.; Grandner, M.A.; Kushida, C.; et al. Recommended amount of sleep for a healthy adult: A joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep 2015, 38, 843–844. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, I.; Floyd, T.C. Systematic trends across the night in human sleep cycles. Psychophysiology 1979, 16, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Borbély, A.A.; Baumann, F.; Brandeis, D.; Strauch, I.; Lehmann, D. Sleep deprivation: Effect on sleep stages and EEG power density in man. Electroencephalogr. Clin. Neurophysiol. 1981, 51, 483–495. [Google Scholar] [CrossRef]
- Dijk, D.J.; Cajochen, C.; Tobler, I.; Borbély, A.A. Sleep extension in humans: Sleep stages, EEG power spectra and body temperature. Sleep 1991, 14, 294–306. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, S.A.; Smith, B.P.; Browne, M.; Rockloff, M.J. Fatigue in emergency services operations: Assessment of the optimal objective and subjective measures using a simulated wildfire deployment. Int. J. Environ. Res. Public Health 2016, 13, 171. [Google Scholar] [CrossRef] [PubMed]
- Dawson, D.; Ferguson, S.A.; Vincent, G.E. Safety implications of fatigue and sleep inertia for emergency services personnel. Sleep Med. Rev. 2021, 55, 101386. [Google Scholar] [CrossRef] [PubMed]
- Muzet, A.; Nicolas, A.; Tassi, P.; Dewasmes, G.; Bonneau, A. Implementation of napping in industry and the problem of sleep inertia. J. Sleep Res. 1995, 4, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Wörle, J.; Metz, B.; Baumann, M. Sleep inertia in automated driving: Post-sleep take-over and driving performance. Accid. Anal. Prev. 2021, 150, 105918. [Google Scholar] [CrossRef]
- Hilditch, C.J.; Dorrian, J.; Banks, S. Time to wake up: Reactive countermeasures to sleep inertia. Ind. Health 2016, 54, 528–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilditch, C.J.; Dorrian, J.; Banks, S. A review of short naps and sleep inertia: Do naps of 30 min or less really avoid sleep inertia and slow-wave sleep? Sleep Med. 2017, 32, 176–190. [Google Scholar] [CrossRef] [PubMed]
- Centofanti, S.; Banks, S.; Coussens, S.; Gray, D.; Munro, E.; Nielsen, J.; Dorrian, J. A pilot study investigating the impact of a caffeine-nap on alertness during a simulated night shift. Chronobiol. Int. 2020, 37, 1469–1473. [Google Scholar] [CrossRef] [PubMed]
- Santhi, N.; Groeger, J.A.; Archer, S.N.; Gimenez, M.; Schlangen, L.J.M.; Dijk, D.J. Morning sleep inertia in alertness and performance: Effect of cognitive domain and white light conditions. PLoS ONE 2013, 8, e79688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueiro, M.G.; Sahin, L.; Roohan, C.; Kalsher, M.; Plitnick, B.; Rea, M.S. Effects of red light on sleep inertia. Nat. Sci. Sleep 2019, 11, 45–57. [Google Scholar] [CrossRef] [Green Version]
- Thompson, A.; Jones, H.; Gregson, W.; Atkinson, G. Effects of dawn simulation on markers of sleep inertia and post-waking performance in humans. Eur. J. Appl. Physiol. 2014, 114, 1049–1056. [Google Scholar] [CrossRef]
- McFarlane, S.J.; Garcia, J.E.; Verhagen, D.S.; Dyer, A.G. Auditory countermeasures for sleep inertia: Exploring the effect of melody and rhythm in an ecological context. Clocks Sleep 2020, 2, 208–224. [Google Scholar] [CrossRef]
- Kovac, K.; Vincent, G.E.; Paterson, J.L.; Aisbett, B.; Reynolds, A.C.; Ferguson, S.A. Can an increase in noradrenaline induced by brief exercise counteract sleep inertia? Chronobiol. Int. 2020, 37, 1474–1478. [Google Scholar] [CrossRef] [PubMed]
- Rangan, S.; Riedy, S.M.; Bassett, R.; Klinck, Z.A.; Hagerty, P.; Schek, E.; Zhang, Y.; Hursh, S.R.; Van Dongen, H.P.A. Predictive and proactive fatigue risk management approaches in commercial aviation. Chronobiol. Int. 2020, 37, 1479–1482. [Google Scholar] [CrossRef] [PubMed]
- Dawson, D.; Chapman, J.; Thomas, M.J. Fatigue-proofing: A new approach to reducing fatigue-related risk using the principles of error management. Sleep Med. Rev. 2012, 16, 167–175. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sleep Stage at Awakening | 12-h Baseline (PSE Condition) | 6-h Baseline (PSR Condition) | 12-h Recovery | ICC |
|---|---|---|---|---|
| Stage 1 sleep | 28.6% (10) | 25.0% (4) | 41.2% (21) | 0.024 (0.000–0.207) |
| Stage 2 sleep | 48.6% (17) | 56.3% (9) | 29.4% (15) | 0.116 (0.000–0.333) |
| Slow wave sleep | 0% (0) | 0% (0) | 5.9% (3) | 0.000 (0.000–0.171) |
| REM sleep | 22.8% (8) | 18.7% (3) | 23.5% (12) | 0.113 (0.000–0.329) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lundholm, K.R.; Honn, K.A.; Skeiky, L.; Muck, R.A.; Van Dongen, H.P.A. Trait Interindividual Differences in the Magnitude of Subjective Sleepiness from Sleep Inertia. Clocks & Sleep 2021, 3, 298-311. https://doi.org/10.3390/clockssleep3020019
Lundholm KR, Honn KA, Skeiky L, Muck RA, Van Dongen HPA. Trait Interindividual Differences in the Magnitude of Subjective Sleepiness from Sleep Inertia. Clocks & Sleep. 2021; 3(2):298-311. https://doi.org/10.3390/clockssleep3020019
Chicago/Turabian StyleLundholm, Kirsie R., Kimberly A. Honn, Lillian Skeiky, Rachael A. Muck, and Hans P. A. Van Dongen. 2021. "Trait Interindividual Differences in the Magnitude of Subjective Sleepiness from Sleep Inertia" Clocks & Sleep 3, no. 2: 298-311. https://doi.org/10.3390/clockssleep3020019
APA StyleLundholm, K. R., Honn, K. A., Skeiky, L., Muck, R. A., & Van Dongen, H. P. A. (2021). Trait Interindividual Differences in the Magnitude of Subjective Sleepiness from Sleep Inertia. Clocks & Sleep, 3(2), 298-311. https://doi.org/10.3390/clockssleep3020019