
On the Efficacy of a CBT-I-Based Online Program for Sleep Problems: A Randomized Controlled Trial



{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Subjective Sleep Parameters
2.1.1. Insomnia Severity
2.1.2. Subjective Sleep Quality
2.2. Objective Sleep Parameters
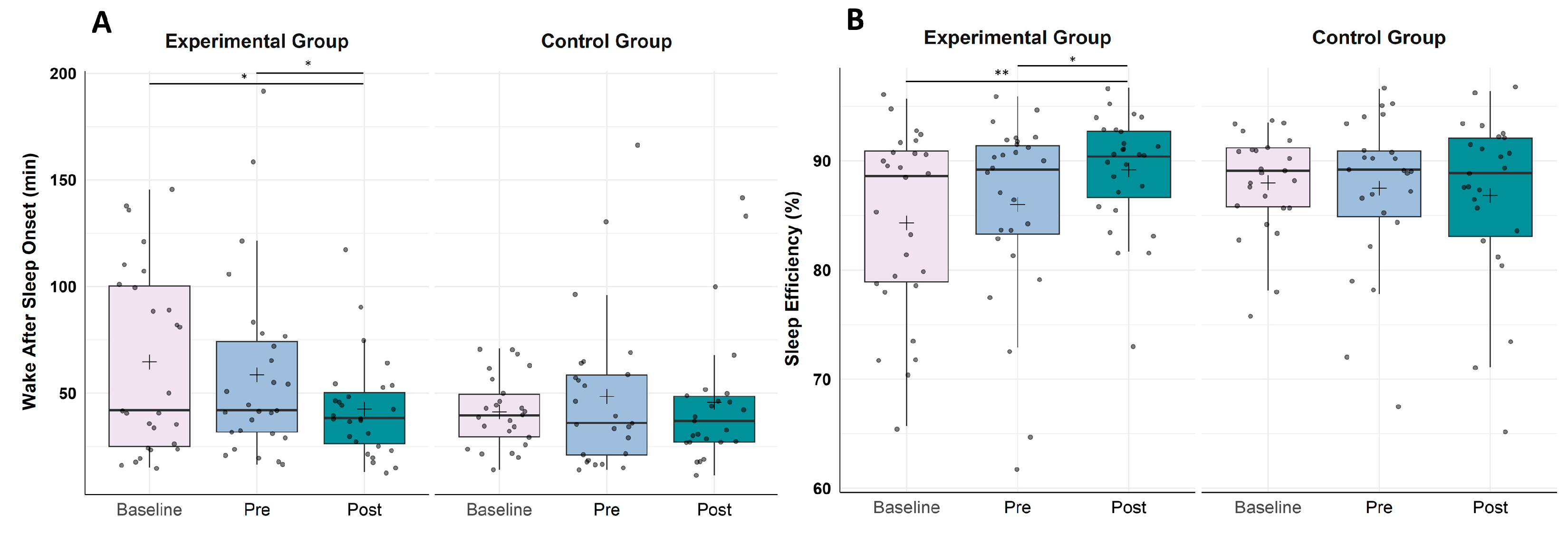
2.2.1. Wake after Sleep Onset
2.2.2. Sleep Efficiency
2.2.3. Total Sleep Time
3. Discussion
3.1. Changes in Subjective Measures of Sleep (Questionnaires)
3.2. Changes in Objective Measures of Sleep (PSG)
3.3. Limitations and Future Directions
4. Materials and Methods
4.1. Participants
4.2. Study Design and Procedure
4.2.1. Intervention Program “GesunderSchlaf.Coach”
4.2.2. Active Control Group
4.3. Materials and Measures
4.3.1. Subjective Sleep Assessment
Insomnia Severity
Sleep Quality
Sleep Diary
4.3.2. Objective Sleep Assessment
Ambulatory Polysomnography
4.4. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Penzel, T.; Peter, J.H.; Peter, H.; Becker, H.F.; Fietze, I.; Fischer, J.; Mayer, G.; Podszus, T.; Raschke, F.; Riemann, D.; et al. Themenheft 27 “Schlafstörungen”; Robert Koch Institute: Berlin, Germany, 2005; p. 49. [Google Scholar]
- Grandner, M.A. Sleep, Health, and Society. Sleep Med. Clin. 2017, 12, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Hajak, G. Insomnia in primary care. Sleep 2000, 23 (Suppl. 3), S54–S63. [Google Scholar]
- Ohayon, M.M. Epidemiological Overview of sleep Disorders in the General Population. Sleep Med. Res. 2011, 2, 1–9. [Google Scholar] [CrossRef]
- Morin, C.M.; Benca, R. Chronic insomnia. Lancet 2012, 379, 1129–1141. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Schlack, R.; Hapke, U.; Maske, U.; Busch, M.; Cohrs, S. Häufigkeit und Verteilung von Schlafproblemen und Insomnie in der deutschen Erwachsenenbevölkerung. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 2013, 56, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Kyle, S.D.; Morgan, K.; Espie, C.A. Insomnia and health-related quality of life. Sleep Med. Rev. 2010, 14, 69–82. [Google Scholar] [CrossRef]
- Riemann, D.; Benz, F.; Dressle, R.J.; Espie, C.A.; Johann, A.F.; Blanken, T.F.; Leerssen, J.; Wassing, R.; Henry, A.L.; Kyle, S.D.; et al. Insomnia disorder: State of the science and challenges for the future. J. Sleep Res. 2022, 31, e13604. [Google Scholar] [CrossRef]
- Li, M.; Zhang, X.W.; Hou, W.S.; Tang, Z.Y. Insomnia and risk of cardiovascular disease: A meta-analysis of cohort studies. Int. J. Cardiol. 2014, 176, 1044–1047. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Quantity and quality of sleep and incidence of type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2010, 33, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Hertenstein, E.; Feige, B.; Gmeiner, T.; Kienzler, C.; Spiegelhalder, K.; Johann, A.; Jansson-Frojmark, M.; Palagini, L.; Rucker, G.; Riemann, D.; et al. Insomnia as a predictor of mental disorders: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 43, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Palagini, L.; Hertenstein, E.; Riemann, D.; Nissen, C. Sleep, insomnia and mental health. J. Sleep Res. 2022, 31, e13628. [Google Scholar] [CrossRef] [PubMed]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef]
- Weissman, M.M.; Greenwald, S.; Niño-Murcia, G.; Dement, W.C. The morbidity of insomnia uncomplicated by psychiatric disorders. Gen. Hosp. Psychiatry 1997, 19, 245–250. [Google Scholar] [CrossRef]
- Pigeon, W.R.; Pinquart, M.; Conner, K. Meta-analysis of sleep disturbance and suicidal thoughts and behaviors. J. Clin. Psychiatry 2012, 73, e1160–e1167. [Google Scholar] [CrossRef]
- Besedovsky, L.; Lange, T.; Haack, M. The Sleep-Immune Crosstalk in Health and Disease. Physiol. Rev. 2019, 99, 1325–1380. [Google Scholar] [CrossRef]
- Fortier-Brochu, E.; Beaulieu-Bonneau, S.; Ivers, H.; Morin, C.M. Insomnia and daytime cognitive performance: A meta-analysis. Sleep Med. Rev. 2012, 16, 83–94. [Google Scholar] [CrossRef]
- Wardle-Pinkston, S.; Slavish, D.C.; Taylor, D.J. Insomnia and cognitive performance: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 48, 101205. [Google Scholar] [CrossRef]
- Daley, M.; Morin, C.M.; LeBlanc, M.; Gregoire, J.P.; Savard, J.; Baillargeon, L. Insomnia and its relationship to health-care utilization, work absenteeism, productivity and accidents. Sleep Med. 2009, 10, 427–438. [Google Scholar] [CrossRef]
- Thiart, H.; Ebert, D.D.; Lehr, D.; Nobis, S.; Buntrock, C.; Berking, M.; Smit, F.; Riper, H. Internet-Based Cognitive Behavioral Therapy for Insomnia: A Health Economic Evaluation. Sleep 2016, 39, 1769–1778. [Google Scholar] [CrossRef] [PubMed]
- Qaseem, A.; Kansagara, D.; Forciea, M.A.; Cooke, M.; Denberg, T.D. and Clinical Guidelines Committee of the American College of, P. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline from the American College of Physicians. Ann. Intern. Med. 2016, 165, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Riemann, D.; Baglioni, C.; Bassetti, C.; Bjorvatn, B.; Groselj, L.C.; Ellis, J.G.; Espie, C.A.; Garcia-Borreguero, D.; Gjerstad, M.; Gonçalves, M.; et al. European guideline for the diagnosis and treatment of insomnia. J. Sleep Res. 2017, 26, 675–700. [Google Scholar] [CrossRef] [PubMed]
- Riemann, D.; Baum, E.; Cohrs, S.; Crönlein, T.; Hajak, G.; Hertenstein, E.; Klose, P.; Langhorst, J.; Mayer, G.; Nissen, C. S3-Leitlinie nicht erholsamer Schlaf/Schlafstörungen. Somnologie-Schlafforschung Schlafmed. 2017, 21, 2–44. [Google Scholar] [CrossRef]
- van der Zweerde, T.; Bisdounis, L.; Kyle, S.D.; Lancee, J.; van Straten, A. Cognitive behavioral therapy for insomnia: A meta-analysis of long-term effects in controlled studies. Sleep Med. Rev. 2019, 48, 101208. [Google Scholar] [CrossRef]
- Morin, C.M.; Colecchi, C.; Stone, J.; Sood, R.; Brink, D. Behavioral and pharmacological therapies for late-life insomnia: A randomized controlled trial. JAMA 1999, 281, 991–999. [Google Scholar] [CrossRef]
- Okajima, I.; Komada, Y.; Inoue, Y. A meta-analysis on the treatment effectiveness of cognitive behavioral therapy for primary insomnia. Sleep Biol. Rhythm. 2011, 9, 24–34. [Google Scholar] [CrossRef]
- Mitchell, M.D.; Gehrman, P.; Perlis, M.; Umscheid, C.A. Comparative effectiveness of cognitive behavioral therapy for insomnia: A systematic review. BMC Fam. Pract. 2012, 13, 40. [Google Scholar] [CrossRef]
- Zachariae, R.; Lyby, M.S.; Ritterband, L.M.; O’Toole, M.S. Efficacy of internet-delivered cognitive-behavioral therapy for insomnia—A systematic review and meta-analysis of randomized controlled trials. Sleep Med. Rev. 2016, 30, 1–10. [Google Scholar] [CrossRef]
- Grobe, T.G.; Steinmann, S.; Gerr, J. Gesundheitsreport 2019; Schlafstörungen: Berlin, Germany, 2019; p. 10837. [Google Scholar]
- Leger, D.; Poursain, B. An international survey of insomnia: Under-recognition and under-treatment of a polysymptomatic condition. Curr. Med. Res. Opin. 2005, 21, 1785–1792. [Google Scholar] [CrossRef]
- Morin, C.M.; LeBlanc, M.; Daley, M.; Gregoire, J.P.; Merette, C. Epidemiology of insomnia: Prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors. Sleep Med. 2006, 7, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Claßen, M.; Dreimann, S.; Gelhaus, L.; Schulte, M.; Werner, A.; Schlarb, A.A. Glücklich schlafen: Einfluss positiver Kognitionen auf die Schlafqualität und das Wohlbefinden. Somnologie-Schlafforschung Schlafmed. 2017, 21, 173–179. [Google Scholar] [CrossRef]
- Luik, A.I.; Kyle, S.D.; Espie, C.A. Digital Cognitive Behavioral Therapy (dCBT) for Insomnia: A State-of-the-Science Review. Curr. Sleep Med. Rep. 2017, 3, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Espie, C.A.; Kyle, S.D.; Williams, C.; Ong, J.C.; Douglas, N.J.; Hames, P.; Brown, J.S. A randomized, placebo-controlled trial of online cognitive behavioral therapy for chronic insomnia disorder delivered via an automated media-rich web application. Sleep 2012, 35, 769–781. [Google Scholar] [CrossRef]
- Ritterband, L.M.; Thorndike, F.P.; Ingersoll, K.S.; Lord, H.R.; Gonder-Frederick, L.; Frederick, C.; Quigg, M.S.; Cohn, W.F.; Morin, C.M. Effect of a Web-Based Cognitive Behavior Therapy for Insomnia Intervention With 1-Year Follow-up: A Randomized Clinical Trial. JAMA Psychiatry 2017, 74, 68–75. [Google Scholar] [CrossRef]
- Vedaa, Ø.; Hagatun, S.; Kallestad, H.; Pallesen, S.; Smith, O.R.; Thorndike, F.P.; Ritterband, L.M.; Sivertsen, B. Long-term effects of an unguided online cognitive behavioral therapy for chronic insomnia. J. Clin. Sleep Med. 2019, 15, 101–110. [Google Scholar] [CrossRef]
- Soh, H.L.; Ho, R.C.; Ho, C.S.; Tam, W.W. Efficacy of digital cognitive behavioural therapy for insomnia: A meta-analysis of randomised controlled trials. Sleep Med. 2020, 75, 315–325. [Google Scholar] [CrossRef]
- Simon, L.; Steinmetz, L.; Feige, B.; Benz, F.; Spiegelhalder, K.; Baumeister, H. Comparative efficacy of onsite, digital, and other settings for cognitive behavioral therapy for insomnia: A systematic review and network meta-analysis. Sci. Rep. 2023, 13, 1929. [Google Scholar] [CrossRef]
- Baglioni, C.; Regen, W.; Teghen, A.; Spiegelhalder, K.; Feige, B.; Nissen, C.; Riemann, D. Sleep changes in the disorder of insomnia: A meta-analysis of polysomnographic studies. Sleep Med. Rev. 2014, 18, 195–213. [Google Scholar] [CrossRef]
- Geiger-Brown, J.M.; Rogers, V.E.; Liu, W.; Ludeman, E.M.; Downton, K.D.; Diaz-Abad, M. Cognitive behavioral therapy in persons with comorbid insomnia: A meta-analysis. Sleep Med. Rev. 2015, 23, 54–67. [Google Scholar] [CrossRef]
- Krystal, A.D.; Edinger, J.D. Sleep EEG predictors and correlates of the response to cognitive behavioral therapy for insomnia. Sleep 2010, 33, 669–677. [Google Scholar] [CrossRef] [PubMed]
- Cervena, K.; Dauvilliers, Y.; Espa, F.; Touchon, J.; Matousek, M.; Billiard, M.; Besset, A. Effect of cognitive behavioural therapy for insomnia on sleep architecture and sleep EEG power spectra in psychophysiological insomnia. J. Sleep Res. 2004, 13, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Dressle, R.J.; Riemann, D. Hyperarousal in insomnia disorder: Current evidence and potential mechanisms. J. Sleep Res. 2023, e13928. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, M.H.; Arand, D.L. Hyperarousal and insomnia: State of the science. Sleep Med. Rev. 2010, 14, 9–15. [Google Scholar] [CrossRef]
- Crönlein, T.; Lehner, A.; Schussler, P.; Geisler, P.; Rupprecht, R.; Wetter, T.C. Changes in Subjective-Objective Sleep Discrepancy Following Inpatient Cognitive Behavior Therapy for Insomnia. Behav. Ther. 2019, 50, 994–1001. [Google Scholar] [CrossRef]
- Nishikawa, K.; Kuriyama, K.; Yoshiike, T.; Yoshimura, A.; Okawa, M.; Kadotani, H.; Yamada, N. Effects of Cognitive Behavioral Therapy for Insomnia on Subjective-Objective Sleep Discrepancy in Patients with Primary Insomnia: A Small-Scale Cohort Pilot Study. Int. J. Behav. Med. 2021, 28, 715–726. [Google Scholar] [CrossRef]
- Harvey, A.G.; Tang, N.K. (Mis)perception of sleep in insomnia: A puzzle and a resolution. Psychol. Bull. 2012, 138, 77–101. [Google Scholar] [CrossRef]
- Koffel, E.; Kuhn, E.; Petsoulis, N.; Erbes, C.R.; Anders, S.; Hoffman, J.E.; Ruzek, J.I.; Polusny, M.A. A randomized controlled pilot study of CBT-I Coach: Feasibility, acceptability, and potential impact of a mobile phone application for patients in cognitive behavioral therapy for insomnia. Health Inform. J. 2018, 24, 3–13. [Google Scholar] [CrossRef]
- Hartescu, I.; Morgan, K.; Stevinson, C.D. Increased physical activity improves sleep and mood outcomes in inactive people with insomnia: A randomized controlled trial. J. Sleep Res. 2015, 24, 526–534. [Google Scholar] [CrossRef]
- Lowe, H.; Haddock, G.; Mulligan, L.D.; Gregg, L.; Fuzellier-Hart, A.; Carter, L.-A.; Kyle, S.D. Does exercise improve sleep for adults with insomnia? A systematic review with quality appraisal. Clin. Psychol. Rev. 2019, 68, 1–12. [Google Scholar] [CrossRef]
- van Maanen, A.; Meijer, A.M.; van der Heijden, K.B.; Oort, F.J. The effects of light therapy on sleep problems: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 29, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Morin, C.M.; Schaefer, K.; Wallenstein, G.V. Interpreting score differences in the Insomnia Severity Index: Using health-related outcomes to define the minimally important difference. Curr. Med. Res. Opin. 2009, 25, 2487–2494. [Google Scholar] [CrossRef] [PubMed]
- Spiegelhalder, K.; Acker, J.; Baumeister, H.; Büttner-Teleaga, A.; Danker-Hopfe, H.; Ebert, D.D.; Fietze, I.; Frase, L.; Klein, S.; Lehr, D.; et al. Digitale Behandlungsangebote für Insomnie—Eine Übersichtsarbeit. Somnologie 2020, 24, 106–114. [Google Scholar] [CrossRef]
- Ohayon, M.; Wickwire, E.M.; Hirshkowitz, M.; Albert, S.M.; Avidan, A.; Daly, F.J.; Dauvilliers, Y.; Ferri, R.; Fung, C.; Gozal, D.; et al. National Sleep Foundation’s sleep quality recommendations: First report. Sleep Health 2017, 3, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Reilly, E.D.; Robinson, S.A.; Petrakis, B.A.; Gardner, M.M.; Wiener, R.S.; Castaneda-Sceppa, C.; Quigley, K.S. Mobile Intervention to Improve Sleep and Functional Health of Veterans with Insomnia: Randomized Controlled Trial. JMIR Form. Res. 2021, 5, e29573. [Google Scholar] [CrossRef]
- Florea, C.; Topalidis, P.; Hauser, T.; Angerer, M.; Kurapov, A.; Beltran Leon, C.A.; Soares Brandao, D.; Schabus, M. Sleep during COVID-19 lockdown: A cross-cultural study investigating job system relevance. Biochem. Pharmacol. 2021, 191, 114463. [Google Scholar] [CrossRef]
- Blume, C.; Schmidt, M.H.; Cajochen, C. Effects of the COVID-19 lockdown on human sleep and rest-activity rhythms. Curr. Biol. 2020, 30, R795–R797. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Dieck, A.; Morin, C.M.; Backhaus, J. A German version of the Insomnia Severity Index. Somnologie 2018, 22, 27–35. [Google Scholar] [CrossRef]
- Weingartz, S.; Pillmann, F. Meinungen-zum-Schlaf-Fragebogen: Deutsche Version der DBAS-16 zur Erfassung Dysfunktionaler Überzeugungen und Einstellungen zum Schlaf (ORIGINALARBEIT); Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- World Health Organization. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol. Med. 1996, 28, 551–559. [Google Scholar]
- Scharfenstein, A.; Basler, H.-D. Schlafstörungen: Auf Dem Weg Zu Einem Besseren Schlaf. Trainerhandbuch. Psychologisches Trainingsprogramm Für Gruppen-Und Einzelbehandlung; Vandenhoeck & Ruprecht: Göttingen, Germany, 2004. [Google Scholar]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Riemann, D.; Backhaus, J. Behandlung von Schlafstörungen. Ein Psychologisches Gruppenprogramm; Beltz Psychologie Verlags Union: Weinheim, Germany, 1996. [Google Scholar]
- AAST Standards; Guidelines Committee. AAST Technical Guideline. Standard Polysomongraphy; American Association for Sleep Technologists (AAST): Chicago, IL, USA, 2021. [Google Scholar]
- Bakker, J.P.; Ross, M.; Cerny, A.; Vasko, R.; Shaw, E.; Kuna, S.; Magalang, U.J.; Punjabi, N.M.; Anderer, P. Scoring sleep with artificial intelligence enables quantification of sleep stage ambiguity: Hypnodensity based on multiple expert scorers and auto-scoring. Sleep 2023, 46, zsac154. [Google Scholar] [CrossRef] [PubMed]
- Wasserstein, R.L.; Schirm, A.L.; Lazar, N.A. Moving to a World Beyond “p < 0.05”. Am. Stat. 2019, 73, 1–19. [Google Scholar] [CrossRef]
- Mitchell, L.J.; Bisdounis, L.; Ballesio, A.; Omlin, X. and Kyle, S.D. The impact of cognitive behavioural therapy for insomnia on objective sleep parameters: A meta-analysis and systematic review. Sleep Med. Rev. 2019, 47, 90–102. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eigl, E.-S.; Hauser, T.; Topalidis, P.I.; Schabus, M. On the Efficacy of a CBT-I-Based Online Program for Sleep Problems: A Randomized Controlled Trial. Clocks & Sleep 2023, 5, 590-603. https://doi.org/10.3390/clockssleep5040039
Eigl E-S, Hauser T, Topalidis PI, Schabus M. On the Efficacy of a CBT-I-Based Online Program for Sleep Problems: A Randomized Controlled Trial. Clocks & Sleep. 2023; 5(4):590-603. https://doi.org/10.3390/clockssleep5040039
Chicago/Turabian StyleEigl, Esther-Sevil, Theresa Hauser, Pavlos I. Topalidis, and Manuel Schabus. 2023. "On the Efficacy of a CBT-I-Based Online Program for Sleep Problems: A Randomized Controlled Trial" Clocks & Sleep 5, no. 4: 590-603. https://doi.org/10.3390/clockssleep5040039
APA StyleEigl, E. -S., Hauser, T., Topalidis, P. I., & Schabus, M. (2023). On the Efficacy of a CBT-I-Based Online Program for Sleep Problems: A Randomized Controlled Trial. Clocks & Sleep, 5(4), 590-603. https://doi.org/10.3390/clockssleep5040039