
Prevalence of Multiple Sclerosis in Patients with Inflammatory Bowel Disease

 ,
,  ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Results
2.1. General Characteristics
- -
- For one of the fourteen patients with MS, no data on previous and current treatment were available.
- -
- For two of the fourteen patients with MS, only biographical data were available, including year of death, smoking status, type of IBD diagnosed, and date and age of IBD diagnosis and behavior, while all other elements analyzed were missing.
2.2. Case–Control Study
3. Discussion
4. Materials and Methods
Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Molodecky, N.A.; Soon, I.S.; Rabi, D.M.; Ghali, W.A.; Ferris, M.; Chernoff, G.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Barkema, H.W.; et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology 2012, 142, 46–54.e42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Actis, G.C.; Pellicano, R.; Fagoonee, S.; Ribaldone, D.G. History of Inflammatory Bowel Diseases. J. Clin. Med. 2019, 8, 1970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thurgate, L.E.; Lemberg, D.A.; Day, A.S.; Leach, S.T. An Overview of Inflammatory Bowel Disease Unclassified in Children. Inflamm. Intest. Dis. 2019, 4, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Alatab, S.; Sepanlou, S.G.; Ikuta, K.; Vahedi, H.; Bisignano, C.; Safiri, S.; Sadeghi, A.; Nixon, M.R.; Abdoli, A.; Abolhassani, H.; et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 17–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fornari, C.; Madotto, F.; Fiorino, G.; Ardizzone, S.; Bortoli, A.; Caprioli, F.; Cestari, R.; Conti, S.; Cortelezzi, C.; Mantovani, L.; et al. Inflammatory bowel diseases in Italy: Incidence trends and patients’ characteristics. Value Health 2013, 16, A501. [Google Scholar] [CrossRef] [Green Version]
- Caviglia, G.P.; Garrone, A.; Bertolino, C.; Vanni, R.; Bretto, E.; Poshnjari, A.; Tribocco, E.; Frara, S.; Armandi, A.; Astegiano, M.; et al. Epidemiology of Inflammatory Bowel Diseases: A Population Study in a Healthcare District of North-West Italy. J. Clin. Med. 2023, 12, 641. [Google Scholar] [CrossRef]
- Kuenzig, M.E.; Nguyen, G.C.; Benchimol, E.I. Rural and Urban Differences in the Risk of Inflammatory Bowel Disease and Subsequent Health Services Utilization in Ontario. Healthc. Q. 2019, 22, 6–9. [Google Scholar] [CrossRef]
- Cosnes, J.; Gower-Rousseau, C.; Seksik, P.; Cortot, A. Epidemiology and natural history of inflammatory bowel diseases. Gastroenterology 2011, 140, 1785–1794. [Google Scholar] [CrossRef]
- Rustgi, S.D.; Kayal, M.; Shah, S.C. Sex-based differences in inflammatory bowel diseases: A review. Ther. Adv. Gastroenterol. 2020, 13, 1756284820915043. [Google Scholar] [CrossRef]
- Ribaldone, D.G.; Pellicano, R.; Actis, G.C. The gut and the inflammatory bowel diseases inside-out: Extra-intestinal manifestations. Minerva Gastroenterol. Dietol. 2019, 65, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Kosmidou, M.; Katsanos, A.H.; Katsanos, K.H.; Kyritsis, A.P.; Tsivgoulis, G.; Christodoulou, D.; Giannopoulos, S. Multiple sclerosis and inflammatory bowel diseases: A systematic review and meta-analysis. J. Neurol. 2017, 264, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Vidal-Jordana, A.; Montalban, X. Multiple sclerosis: Clinical aspects. Curr. Opin. Neurol. 2018, 31, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Alfredsson, L.; Olsson, T. Lifestyle and Environmental Factors in Multiple Sclerosis. Cold Spring Harb. Perspect. Med. 2019, 9, a028944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broadley, S.A.; Deans, J.; Sawcer, S.J.; Clayton, D.; Compston, D.A. Autoimmune disease in first-degree relatives of patients with multiple sclerosis. A UK survey. Brain 2000, 123 Pt 6, 1102–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobson, R.; Giovannoni, G. Autoimmune disease in people with multiple sclerosis and their relatives: A systematic review and meta-analysis. J. Neurol. 2013, 260, 1272–1285. [Google Scholar] [CrossRef]
- Sonnenberg, A.; Ajdacic-Gross, V. Similar birth-cohort patterns in Crohn’s disease and multiple sclerosis. Mult. Scler. 2018, 24, 140–149. [Google Scholar] [CrossRef]
- Yang, Y.; Musco, H.; Simpson-Yap, S.; Zhu, Z.; Wang, Y.; Lin, X.; Zhang, J.; Taylor, B.; Gratten, J.; Zhou, Y. Investigating the shared genetic architecture between multiple sclerosis and inflammatory bowel diseases. Nat. Commun. 2021, 12, 5641. [Google Scholar] [CrossRef]
- Wang, X.; Wan, J.; Wang, M.; Zhang, Y.; Wu, K.; Yang, F. Multiple sclerosis and inflammatory bowel disease: A systematic review and meta-analysis. Ann. Clin. Transl. Neurol. 2022, 9, 132–140. [Google Scholar] [CrossRef]
- Istat.it Malattie. Available online: https://www.istat.it/it/archivio/malattie (accessed on 19 June 2023).
- Rang, E.H.; Brooke, B.N.; Hermon-Taylor, J. Association of ulcerative colitis with multiple sclerosis. Lancet 1982, 2, 555. [Google Scholar] [CrossRef]
- Pokorny, C.S.; Beran, R.G.; Pokorny, M.J. Association between ulcerative colitis and multiple sclerosis. Intern. Med. J. 2007, 37, 721–724. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.M.; Frisch, M.; Rostgaard, K.; Wohlfahrt, J.; Hjalgrim, H.; Koch-Henriksen, N.; Melbye, M.; Westergaard, T. Autoimmune diseases in patients with multiple sclerosis and their first-degree relatives: A nationwide cohort study in Denmark. Mult. Scler. 2008, 14, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Fernández, O.; Fernández, V.; De Ramón, E. Azathioprine and methotrexate in multiple sclerosis. J. Neurol. Sci. 2004, 223, 29–34. [Google Scholar] [CrossRef]
- Avasarala, J.; Guduru, Z.; McLouth, C.J.; Wilburn, A.; Talbert, J.; Sutton, P.; Sokola, B.S. Use of anti-TNF-α therapy in Crohn’s disease is associated with increased incidence of multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 51, 102942. [Google Scholar] [CrossRef] [PubMed]
- Koch-Henriksen, N.; Sørensen, P.S. The changing demographic pattern of multiple sclerosis epidemiology. Lancet Neurol. 2010, 9, 520–532. [Google Scholar] [CrossRef]
- Maaser, C.; Sturm, A.; Vavricka, S.R.; Kucharzik, T.; Fiorino, G.; Annese, V.; Calabrese, E.; Baumgart, D.C.; Bettenworth, D.; Borralho Nunes, P.; et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J. Crohns Colitis 2019, 13, 144–164. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Risk Factors | Case (n = 14) | Control (n = 342) | p-Value |
|---|---|---|---|
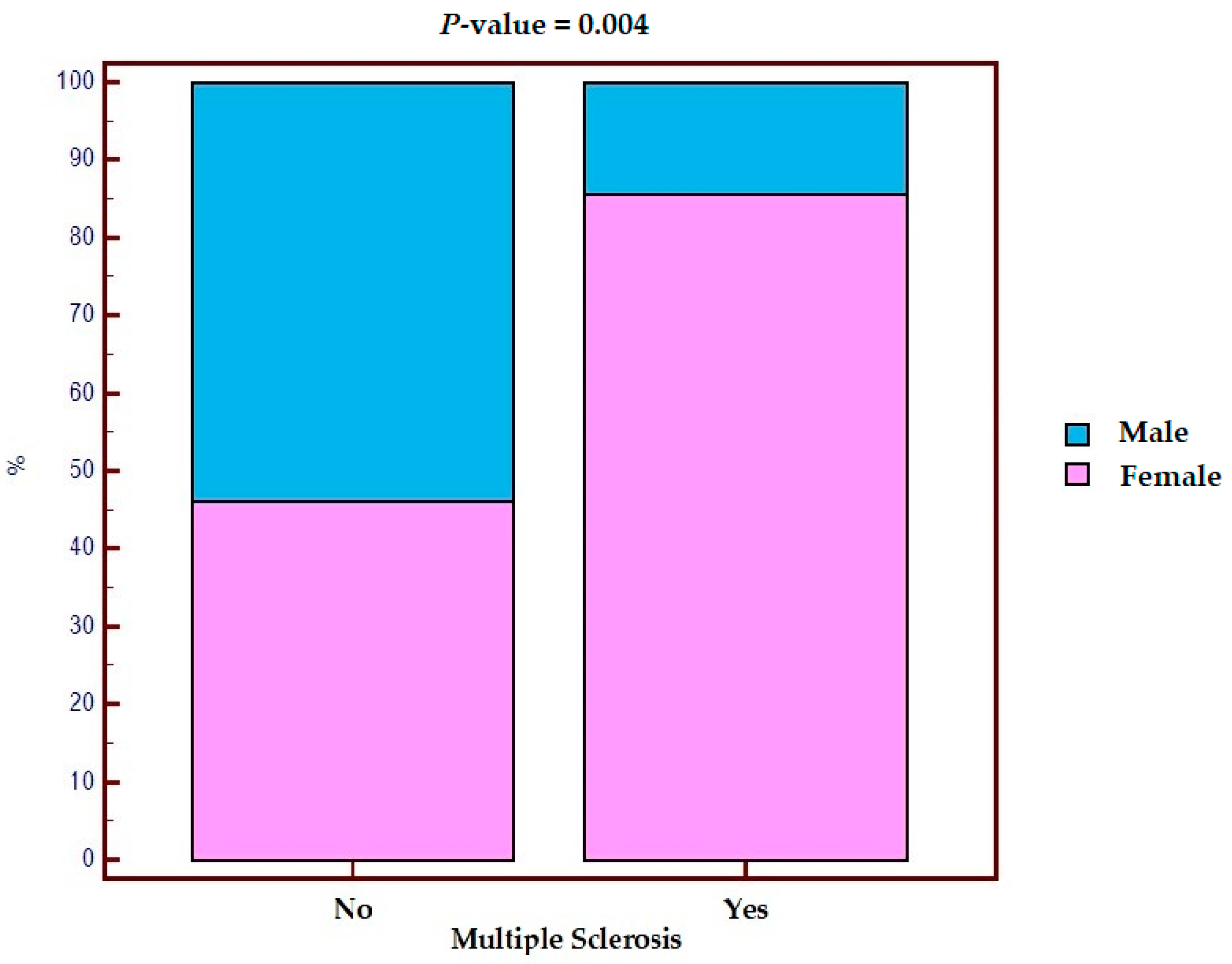
| Sex, n (%) | |||
| Female | 12 (85.7%) | 158 (46.2%) | 0.004 |
| Male | 2 (14.3%) | 184 (53.8%) | |
| Smoking habit, n (%) | |||
| Active smokers | 3 (21.4%) | 82 (23.9%) | 0.980 |
| Former smokers | 5 (35.7%) | 114 (33.3%) | |
| Never smokers | 6 (42.8%) | 142 (41.5%) | |
| IBD type, n (%) | |||
| Chrohn’s disease | 8 (57.1%) | 210 (61.4%) | 0.190 |
| Ulcerative colitis | 4 (28.5%) | 120 (35.1%) | |
| IBD-U | 2 (14.3%) | 12 (3.5%) | |
| Age at diagnosis of IBD, years | 31.5 (27.0–40.0) | 33.0 (24.0–48.0) | 0.930 |
| Mesalazine, n (%) | |||
| Yes | 5 * (41.7%) | 317 ° (92.7%) | <0.001 |
| No | 7 * (58.3%) | 25 ° (7.3%) | |
| Thiopurine, n (%) | |||
| Yes | 1/12 * (8.3%) | 91 ° (26.6%) | 0.160 |
| No | 11/12 * (91.7%) | 251 ° (73.4%) | |
| Anti-TNF, n (%) | |||
| Yes | 0 * (0%) | 91 ° (26.6%) | 0.030 |
| No | 14 * (100%) | 251 ° (73.4%) | |
| Anti-Integrin, n (%) | |||
| Yes | 1 * (7.1%) | 23 ° (6.7%) | 0.950 |
| No | 13 * (92.8%) | 319 ° (93.3%) | |
| Ustekinumab, n (%) | |||
| Yes | 0 * (0%) | 5 ° (1.5%) | 0.650 |
| No | 14 * (100%) | 337 ° (98.5%) | |
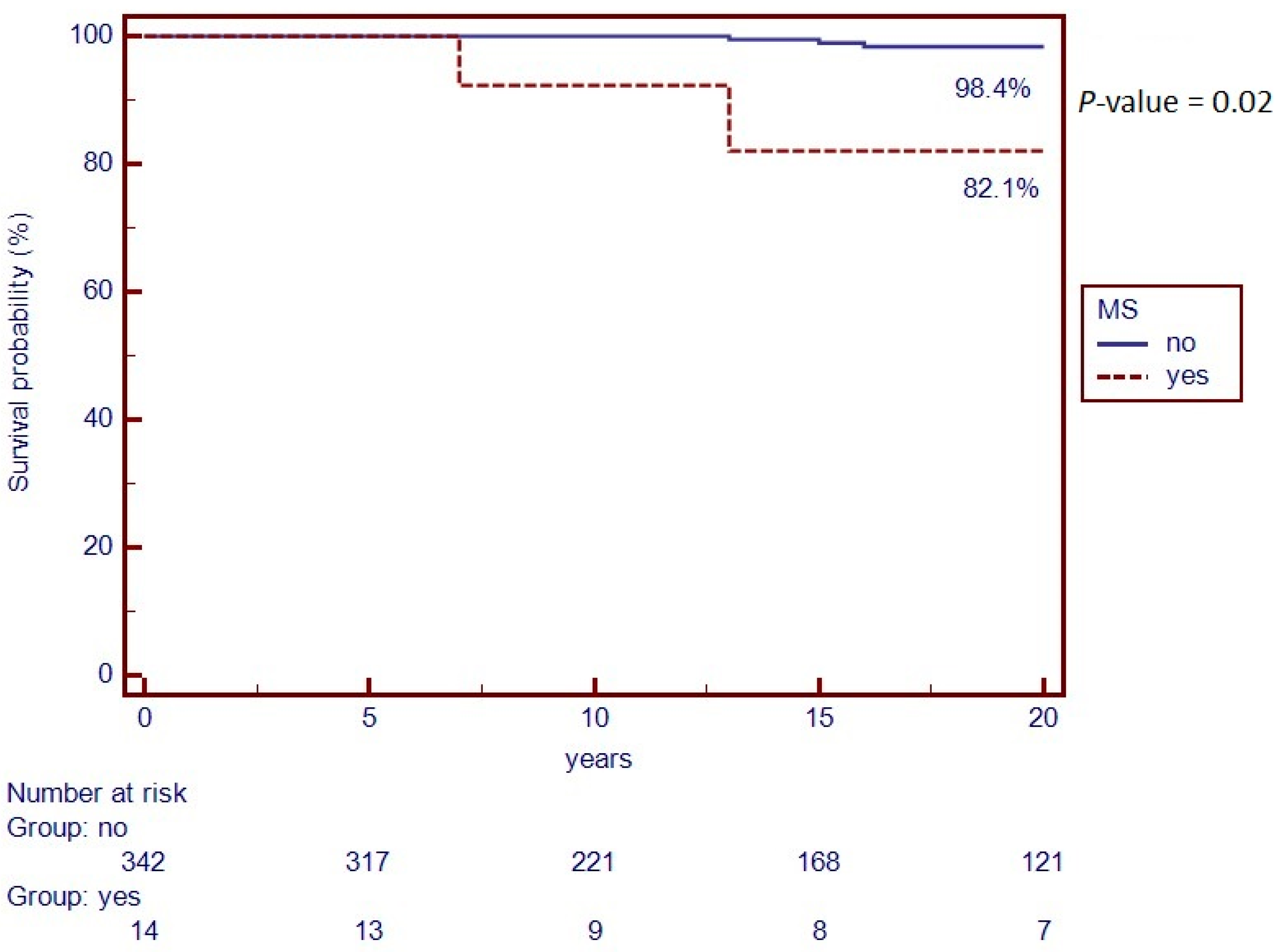
| Death, n (%) | |||
| Yes | 2 (14.3%) | 7 (2.1%) | 0.020 |
| No | 12 (85.7%) | 335 (97.9%) | |
| Surgical resection, n (%) | |||
| Yes | 2 ° (14.3%) | 107 ° (31.3%) | 0.180 |
| No | 12 ° (85.7%) | 235 ° (68.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perez-Diaz-del-Campo, N.; Caviglia, G.P.; Piana, G.L.; Vernero, M.; Schillaci, V.; Armandi, A.; Stalla, F.; Pitoni, D.; Bugianesi, E.; Ciancio, A.; et al. Prevalence of Multiple Sclerosis in Patients with Inflammatory Bowel Disease. Gastrointest. Disord. 2023, 5, 287-295. https://doi.org/10.3390/gidisord5030023
Perez-Diaz-del-Campo N, Caviglia GP, Piana GL, Vernero M, Schillaci V, Armandi A, Stalla F, Pitoni D, Bugianesi E, Ciancio A, et al. Prevalence of Multiple Sclerosis in Patients with Inflammatory Bowel Disease. Gastrointestinal Disorders. 2023; 5(3):287-295. https://doi.org/10.3390/gidisord5030023
Chicago/Turabian StylePerez-Diaz-del-Campo, Nuria, Gian Paolo Caviglia, Giorgia La Piana, Marta Vernero, Valentina Schillaci, Angelo Armandi, Francesco Stalla, Demis Pitoni, Elisabetta Bugianesi, Alessia Ciancio, and et al. 2023. "Prevalence of Multiple Sclerosis in Patients with Inflammatory Bowel Disease" Gastrointestinal Disorders 5, no. 3: 287-295. https://doi.org/10.3390/gidisord5030023
APA StylePerez-Diaz-del-Campo, N., Caviglia, G. P., Piana, G. L., Vernero, M., Schillaci, V., Armandi, A., Stalla, F., Pitoni, D., Bugianesi, E., Ciancio, A., Cavalla, P., & Ribaldone, D. G. (2023). Prevalence of Multiple Sclerosis in Patients with Inflammatory Bowel Disease. Gastrointestinal Disorders, 5(3), 287-295. https://doi.org/10.3390/gidisord5030023