
Investigating the Role of Gastrointestinal-Specific Anxiety and Perceived Disability in the Adjustment to Inflammatory Bowel Disease


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Measures
2.3. Procedures
2.4. Statistical Analyses
3. Results
3.1. Descriptive Statistics
3.2. Preliminary Analyses
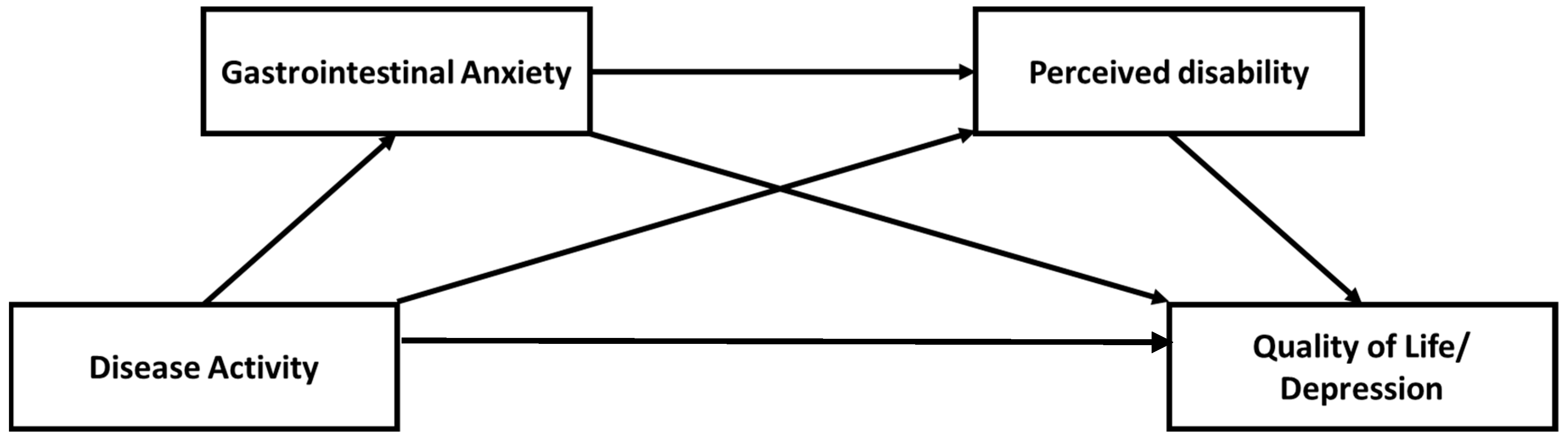
3.3. Serial Mediation
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, R.; Li, Z.; Liu, S.; Zhang, D. Global, regional and national burden of inflammatory bowel disease in 204 countries and territories from 1990 to 2019: A systematic analysis based on the Global Burden of Disease Study 2019. BMJ Open 2023, 13, e065186. [Google Scholar] [CrossRef]
- Sairenji, T.; Collins, K.L.; Evans, D.V. An Update on Inflammatory Bowel Disease. Prim. Care 2017, 44, 673–692. [Google Scholar] [CrossRef]
- Seyedian, S.S.; Nokhostin, F.; Malamir, M.D. A review of the diagnosis, prevention, and treatment methods of inflammatory bowel disease. J. Med. Life 2019, 12, 113–122. [Google Scholar] [CrossRef]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68, s1–s106. [Google Scholar] [CrossRef]
- Cai, Z.; Wang, S.; Li, J. Treatment of Inflammatory Bowel Disease: A Comprehensive Review. Front. Med. 2021, 8, 765474. [Google Scholar] [CrossRef]
- Knowles, S.R.; Graff, L.A.; Wilding, H.; Hewitt, C.; Keefer, L.; Mikocka-Walus, A. Quality of Life in Inflammatory Bowel Disease: A Systematic Review and Meta-analyses-Part I. Inflamm. Bowel Dis. 2018, 24, 742–751. [Google Scholar] [CrossRef]
- Knowles, S.R.; Keefer, L.; Wilding, H.; Hewitt, C.; Graff, L.A.; Mikocka-Walus, A. Quality of Life in Inflammatory Bowel Disease: A Systematic Review and Meta-analyses-Part II. Inflamm. Bowel Dis. 2018, 24, 966–976. [Google Scholar] [CrossRef] [PubMed]
- Larsson, K.; Lööf, L.; Rönnblom, A.; Nordin, K. Quality of life for patients with exacerbation in inflammatory bowel disease and how they cope with disease activity. J. Psychosom. Res. 2008, 64, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Adler, J.; Raju, S.; Beveridge, A.S.; Wang, S.; Zhu, J.; Zimmermann, E.M. College adjustment in University of Michigan students with Crohn’s and colitis. Inflamm. Bowel Dis. 2008, 14, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Kemp, K.; Griffiths, J.; Lovell, K. Understanding the health and social care needs of people living with IBD: A meta-synthesis of the evidence. World J. Gastroenterol. 2012, 18, 6240–6249. [Google Scholar] [CrossRef] [PubMed]
- Pittet, V.; Vaucher, C.; Froehlich, F.; Burnand, B.; Michetti, P.; Maillard, M.H.; Swiss IBD Cohort Study Group. Patient self-reported concerns in inflammatory bowel diseases: A gender-specific subjective quality-of-life indicator. PLoS ONE 2017, 12, e0171864. [Google Scholar] [CrossRef] [PubMed]
- Eugenicos, M.P.; Ferreira, N.B. Psychological factors associated with inflammatory bowel disease. Br. Med. Bull. 2021, 138, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Barberio, B.; Zamani, M.; Black, C.J.; Savarino, E.V.; Ford, A.C. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Mikocka-Walus, A.; Knowles, S.R.; Keefer, L.; Graff, L. Controversies Revisited: A Systematic Review of the Comorbidity of Depression and Anxiety with Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2016, 22, 752–762. [Google Scholar] [CrossRef]
- Martin-Subero, M.; Anderson, G.; Kanchanatawan, B.; Berk, M.; Maes, M. Comorbidity between depression and inflammatory bowel disease explained by immune-inflammatory, oxidative, and nitrosative stress; tryptophan catabolite; and gut-brain pathways. CNS Spectr. 2016, 21, 184–198. [Google Scholar] [CrossRef]
- Kredentser, M.S.; Graff, L.A.; Bernstein, C.N. Psychological Comorbidity and Intervention in Inflammatory Bowel Disease. J. Clin. Gastroenterol. 2021, 55, 30–35. [Google Scholar] [CrossRef]
- Szigethy, E.M.; Allen, J.I.; Reiss, M.; Cohen, W.; Perera, L.P.; Brillstein, L.; Cross, R.K.; Schwartz, D.A.; Kosinski, L.R.; Colton, J.B.; et al. White Paper AGA: The Impact of Mental and Psychosocial Factors on the Care of Patients with Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2017, 15, 986–997. [Google Scholar] [CrossRef]
- Moradkhani, A.; Beckman, L.J.; Tabibian, J.H. Health-related quality of life in inflammatory bowel disease: Psychosocial, clinical, socioeconomic, and demographic predictors. J. Crohns Colitis 2013, 7, 467–473. [Google Scholar] [CrossRef]
- Labus, J.S.; Bolus, R.; Chang, L.; Wiklund, I.; Naesdal, J.; Mayer, E.A.; Naliboff, B.D. The Visceral Sensitivity Index: Development and validation of a gastrointestinal symptom-specific anxiety scale. Aliment. Pharmacol. Ther. 2004, 20, 89–97. [Google Scholar] [CrossRef]
- Jerndal, P.; Ringström, G.; Agerforz, P.; Karpefors, M.; Akkermans, L.M.; Bayati, A.; Simrén, M. Gastrointestinal-specific anxiety: An important factor for severity of GI symptoms and quality of life in IBS. J. Neurogastroenterol. Motil. 2010, 22, 646-e179. [Google Scholar] [CrossRef] [PubMed]
- Bessissow, T.; Van Keerberghen, C.A.; Van Oudenhove, L.; Ferrante, M.; Vermeire, S.; Rutgeerts, P.; Van Assche, G. Anxiety is associated with impaired tolerance of colonoscopy preparation in inflammatory bowel disease and controls. J. Crohns Colitis 2013, 7, e580–e587. [Google Scholar] [CrossRef]
- Trieschmann, K.; Chang, L.; Park, S.; Naliboff, B.; Joshi, S.; Labus, J.S.; Sauk, J.S.; Limketkai, B.N.; Mayer, E.A. The visceral sensitivity index: A novel tool for measuring GI-symptom-specific anxiety in inflammatory bowel disease. J. Neurogastroenterol. Motil. 2022, 34, e14384. [Google Scholar] [CrossRef] [PubMed]
- Hunt, M.G.; Loftus, P.; Accardo, M.; Keenan, M.; Chen, L.; Osterman, M.T. Self-help Cognitive Behavioral Therapy Improves Health-Related Quality of Life for Inflammatory Bowel Disease Patients: A Randomized Controlled Effectiveness Trial. J. Clin. Psychol. Med. Settings 2020, 27, 467–479. [Google Scholar] [CrossRef] [PubMed]
- Kiebles, J.L.; Doerfler, B.; Keefer, L. Preliminary evidence supporting a framework of psychological adjustment to inflammatory bowel disease. Inflamm. Bowel Dis. 2010, 16, 1685–1695. [Google Scholar] [CrossRef] [PubMed]
- Argyriou, K.; Kapsoritakis, A.; Oikonomou, K.; Manolakis, A.; Tsakiridou, E.; Potamianos, S. Disability in Patients with Inflammatory Bowel Disease: Correlations with Quality of Life and Patient’s Characteristics. Can. J. Gastroenterol. Hepatol. 2017, 2017, 6138105. [Google Scholar] [CrossRef] [PubMed]
- Tse, C.S.; Hunt, M.G.; Brown, L.A.; Lewis, J.D. Inflammatory Bowel Diseases-related Disability: Risk Factors, Outcomes, and Interventions. Inflamm. Bowel Dis. 2023, izad182. [Google Scholar] [CrossRef] [PubMed]
- Israeli, E.; Graff, L.A.; Clara, I.; Walker, J.R.; Lix, L.M.; Targownik, L.E.; Bernstein, C.N. Low prevalence of disability among patients with inflammatory bowel diseases a decade after diagnosis. Clin. Gastroenterol. Hepatol. 2014, 12, 1330–1337. [Google Scholar] [CrossRef] [PubMed]
- van der Have, M.; Fidder, H.H.; Leenders, M.; Kaptein, A.A.; van der Valk, M.E.; van Bodegraven, A.A.; Dijkstra, G.; de Jong, D.J.; Pierik, M.; Ponsioen, C.Y.; et al. Self-reported disability in patients with inflammatory bowel disease largely determined by disease activity and illness perceptions. Inflamm. Bowel Dis. 2015, 21, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Beckman, N.; Turer, E.; Scherdell, T.; Dux, M.; Lofland, K. Long-term outcomes in chronic pain patients: The relationship between perceived disability, cognitive and affective factors, and adjustment. J. Pain 2008, 9 (Suppl. 2), 59. [Google Scholar] [CrossRef]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef]
- Cheung, W.Y.; Garratt, A.M.; Russell, I.T.; Williams, J.G. The UK IBDQ-a British version of the inflammatory bowel disease questionnaire. development and validation. J. Clin. Epidemiol. 2000, 53, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Cima, R.R.; Anderson, K.J.; Larson, D.W.; Dozois, E.J.; Hassan, I.; Sandborn, W.J.; Loftus, E.V.; Pemberton, J.H. Internet use by patients in an inflammatory bowel disease specialty clinic. Inflamm. Bowel Dis. 2007, 13, 1266–1270. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2018; ISBN 9781462534654. [Google Scholar]
- Turner, D.; Ricciuto, A.; Lewis, A.; D’Amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef]
- Bowers, H.; Gillanders, D.; Ferreira, N. Moderating effect of IBS acceptance on psychosocial mediators of Irritable Bowel Syndrome. J. Context. Behav. Sci. 2020, 16, 30–36. [Google Scholar] [CrossRef]
- Ferreira, N.B.; Gillanders, D.; Morris, P.G.; Eugenicos, M. Pilot study of acceptance and commitment therapy for irritable bowel syndrome: A preliminary analysis of treatment outcomes and processes of change. Clin. Psychol. (Aust. Psychol. Soc.) 2018, 22, 241–250. [Google Scholar] [CrossRef]
- Marrie, R.A.; Graff, L.A.; Fisk, J.D.; Patten, S.B.; Bernstein, C.N. The Relationship Between Symptoms of Depression and Anxiety and Disease Activity in IBD Over Time. Inflamm. Bowel Dis. 2021, 27, 1285–1293. [Google Scholar] [CrossRef]
- van den Brink, G.; Stapersma, L.; Vlug, L.E.; Rizopolous, D.; Bodelier, A.G.; van Wering, H.; Hurkmans, P.C.W.M.; Stuyt, R.J.L.; Hendriks, D.M.; van der Burg, J.A.T.; et al. Clinical disease activity is associated with anxiety and depressive symptoms in adolescents and young adults with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2018, 48, 358–369. [Google Scholar] [CrossRef]
- Trindade, I.A.; Ferreira, C.; Pinto-Gouveia, J. Chronic Illness-Related Shame: Development of a New Scale and Novel Approach for IBD Patients’ Depressive Symptomatology. Clin. Psyhcol. Psychot. 2017, 24, 255–263. [Google Scholar] [CrossRef]
- Trindade, I.A.; Ferreira, C.; Moura-Ramos, M.; Pinto-Gouveia, J. An 18-month study of the effects of IBD symptomatology and emotion regulation on depressed mood. Int. J. Colorectal Dis. 2017, 32, 651–660. [Google Scholar] [CrossRef]
- Timmer, A.; Preiss, J.C.; Motschall, E.; Rücker, G.; Jantschek, G.; Moser, G. Psychological interventions for treatment of inflammatory bowel disease. Cochrane Database Syst. Rev. 2011, CD006913. [Google Scholar] [CrossRef]
- Taft, T.H.; Ballou, S.; Bedell, A.; Lincenberg, D. Psychological Considerations and Interventions in Inflammatory Bowel Disease Patient Care. Gastroenterol. Clin. N. Am. 2017, 46, 847–858. [Google Scholar] [CrossRef] [PubMed]
- Wynne, B.; McHugh, L.; Gao, W.; Keegan, D.; Byrne, K.; Rowan, C.; Hartery, K.; Kirschbaum, C.; Doherty, G.; Cullen, G.; et al. Acceptance and Commitment Therapy Reduces Psychological Stress in Patients with Inflammatory Bowel Diseases. Gastroenterology 2019, 156, 935–945.e1. [Google Scholar] [CrossRef] [PubMed]
- Lavelle, J.; Storan, D.; Eswara Murthy, V.; De Dominicis, N.; Mulcahy, H.E.; McHugh, L. Brief and Telehealth Acceptance and Commitment Therapy (ACT) Interventions for Stress in Inflammatory Bowel Disease (IBD): A Series of Single Case Experimental Design (SCED) Studies. J. Clin. Med. 2022, 11, 2757. [Google Scholar] [CrossRef] [PubMed]
- Romano, D.; Chesterman, S.; Fuller-Tyszkiewicz, M.; Evans, S.; Dober, M.; Gearry, R.; Gibson, P.R.; Knowles, S.; McCombie, A.; Eric, O.; et al. Feasibility, Acceptability, and Preliminary Efficacy of Acceptance Commitment Therapy for Adults Living with Inflammatory Bowel Disease and Distress. Inflamm. Bowel Dis. 2023, izad122. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Number (N) | Percentage (%) | |
|---|---|---|---|
| Age (years) | 16–17 | 2 | 0.6 |
| 18–24 | 53 | 16.6 | |
| 25–34 | 98 | 30.6 | |
| 35–44 | 74 | 23.1 | |
| 45–54 | 56 | 17.5 | |
| 55–64 | 30 | 9.4 | |
| 55–64 | 6 | 1.9 | |
| 65–older | 1 | 0.3 | |
| Marital status | Married/domestic partnership | 161 | 50.3 |
| Single | 129 | 40.3 | |
| Divorced | 20 | 6.3 | |
| Separated | 4 | 1.3 | |
| Missing | 6 | 1.9 | |
| Diagnosis | CD | 195 | 60.9 |
| UC | 125 | 39.1 | |
| Time since diagnosis | <6 months–1 year ago | 35 | 10.9 |
| >1 years ago | 283 | 88.5 | |
| Missing | 2 | 0.6 | |
| Disease activity | Constantly or often active disease | 141 | 44.1 |
| Sometimes or occasionally active disease | 122 | 38.1 | |
| Rarely/in remission/absence of IBD symptoms | 57 | 17.8 |
| IBDQ | DASS Dep | Disease Activity | VSI | |
|---|---|---|---|---|
| DASS Dep | −0.56 | - | - | - |
| Disease Activity | −0.50 | 0.22 | - | - |
| VSI | −0.46 | 0.38 | 0.22 | - |
| PDS | −0.56 | 0.46 | 0.31 | 0.34 |
| Outcome | ||||||||
|---|---|---|---|---|---|---|---|---|
| Quality of Life | Depression | |||||||
| Coeff. | SE | p | 95% CI | Coeff. | SE | p | 95% CI | |
| Direct Effect | ||||||||
| DA→Outcome | −6.65 | 0.86 | <0.001 | −8.34; −4.96 | 0.80 | 0.75 | 0.29 | −0.68; 2.28 |
| Indirect Effect | ||||||||
| DA→GSA→Outcome | −1.15 | 0.39 | - | −1.99; −0.50 | 0.77 | 0.29 | - | 0.28; 1.42 |
| DA→PDS→Outcome | −1.42 | 0.48 | - | −2.81; −0.94 | 1.34 | 0.38 | - | 0.68; 2.17 |
| DA→GSA→PDS→Outcome | −0.46 | 0.16 | - | −0.80; −0.19 | 0.36 | 0.12 | - | 0.13; 0.59 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seaman, A.; Ferreira, N. Investigating the Role of Gastrointestinal-Specific Anxiety and Perceived Disability in the Adjustment to Inflammatory Bowel Disease. Gastrointest. Disord. 2024, 6, 191-201. https://doi.org/10.3390/gidisord6010014
Seaman A, Ferreira N. Investigating the Role of Gastrointestinal-Specific Anxiety and Perceived Disability in the Adjustment to Inflammatory Bowel Disease. Gastrointestinal Disorders. 2024; 6(1):191-201. https://doi.org/10.3390/gidisord6010014
Chicago/Turabian StyleSeaman, Angela, and Nuno Ferreira. 2024. "Investigating the Role of Gastrointestinal-Specific Anxiety and Perceived Disability in the Adjustment to Inflammatory Bowel Disease" Gastrointestinal Disorders 6, no. 1: 191-201. https://doi.org/10.3390/gidisord6010014
APA StyleSeaman, A., & Ferreira, N. (2024). Investigating the Role of Gastrointestinal-Specific Anxiety and Perceived Disability in the Adjustment to Inflammatory Bowel Disease. Gastrointestinal Disorders, 6(1), 191-201. https://doi.org/10.3390/gidisord6010014