Hadron Therapy Achievements and Challenges: The CNAO Experience


Abstract
:1. Introduction
Rationale and Diffusion of Hadron Therapy in the World
2. Experimental Part
- -
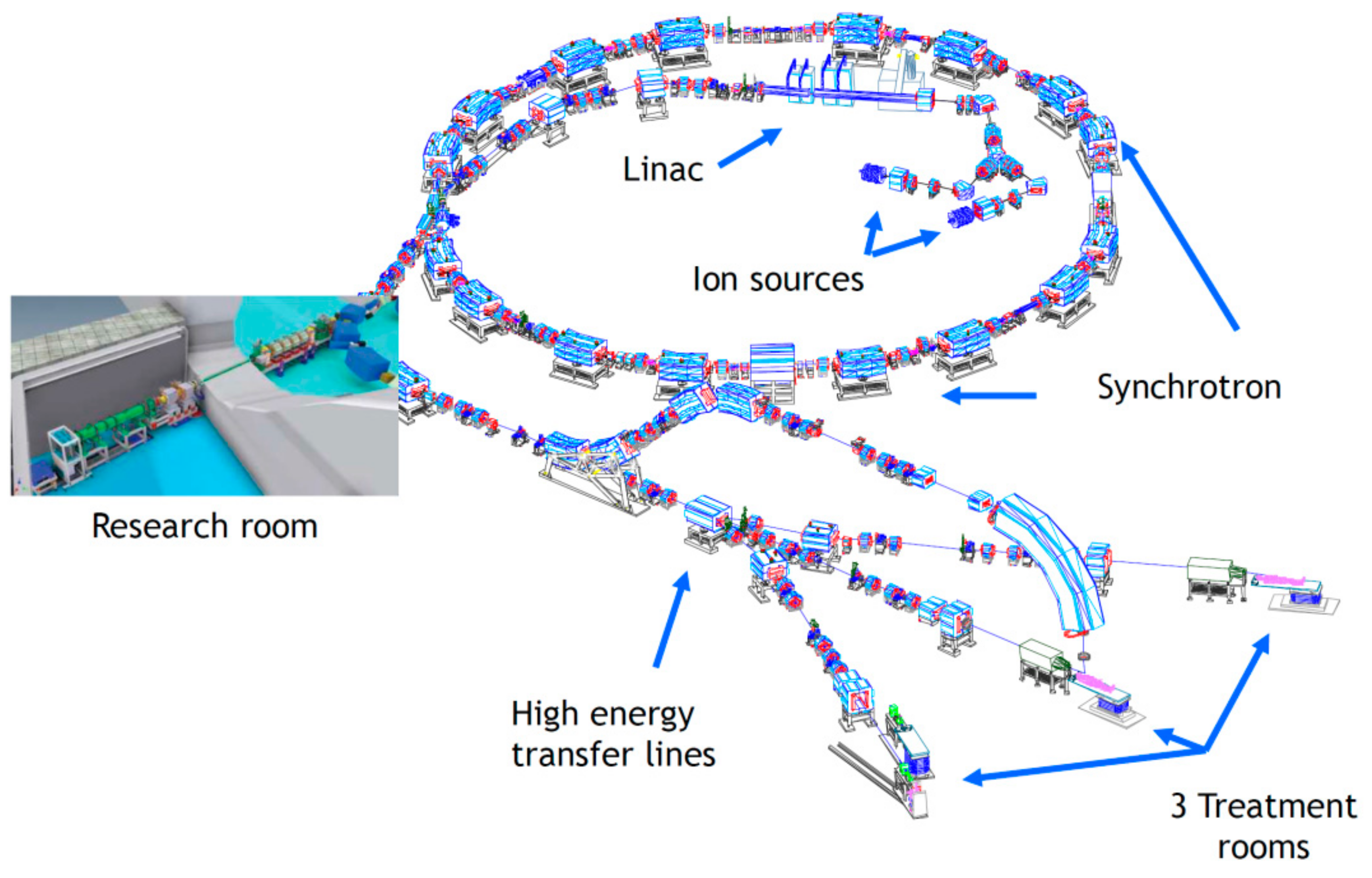
- two (or more) ion sources;
- -
- an injector linac;
- -
- a room-temperature synchrotron;
- -
- a high-energy beam transport line, made of magnets that steer and focus the beam; one or more horizontal beamlines and at least one vertical beamline, equipped with instruments that actively ‘paint’ the tumour and produce the dose distributions required by the Treatment Planning System;
- -
- in the case of HIT (Heidelberg) and NIRS (Chiba), a carbon ion gantry also rotates the beam around the patient couch;
- -
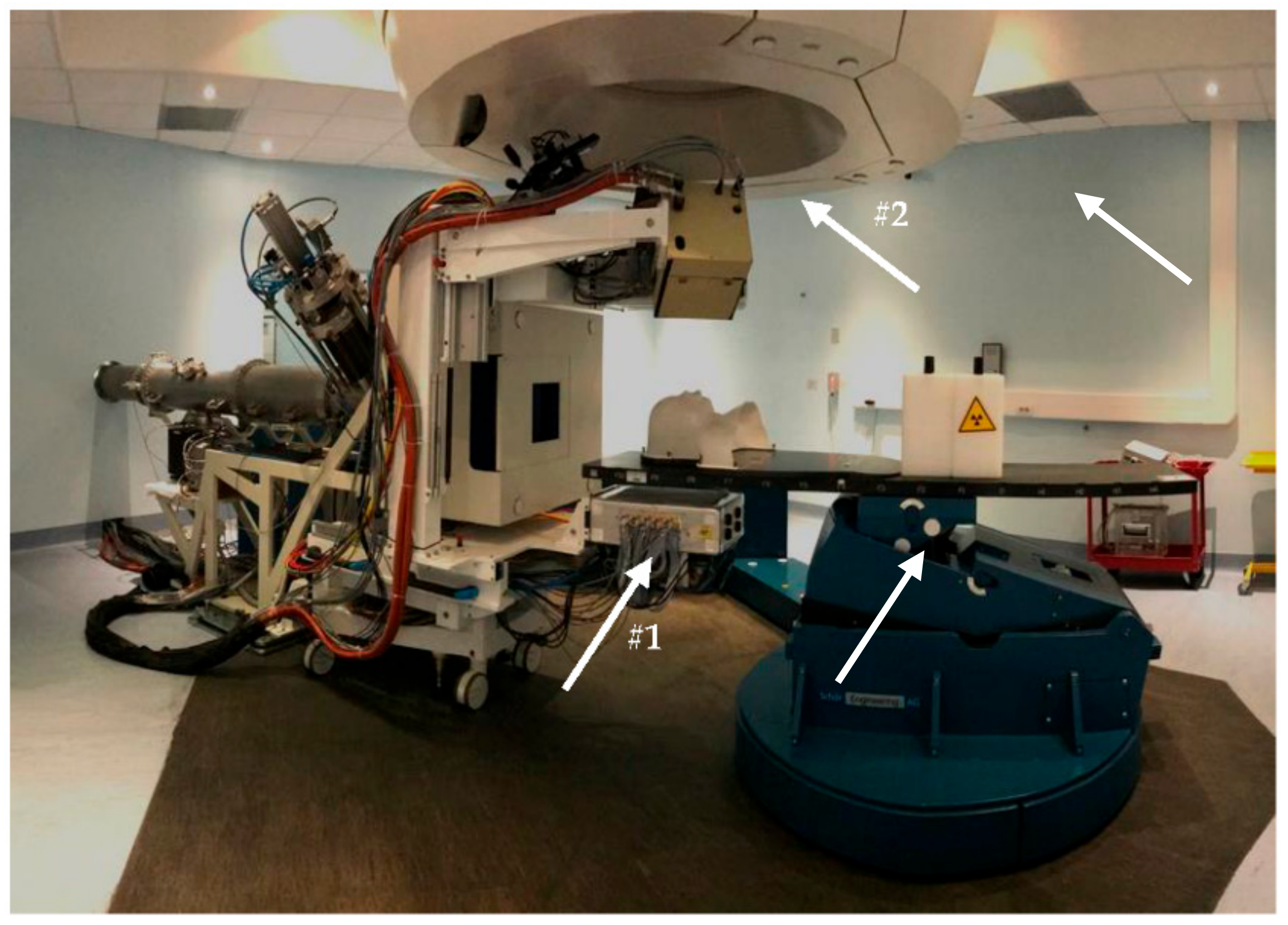
- robotic patient positioning devices and in-room imaging verification systems.
2.1. The National Centre for Oncological Hadron Therapy (CNAO)
2.2. Treatment Procedures at CNAO
2.3. CNAO Medical Device Operation and Performance
2.4. A New Ion Source at CNAO
2.5. In Vivo Range Verification
2.6. Improving Delivery Technology
2.7. Improving the System Efficiency
2.8. Single Room for Proton Therapy
2.9. BNCT, a Hope for the Cure of Metastatic Cancers
3. Theoretical Part
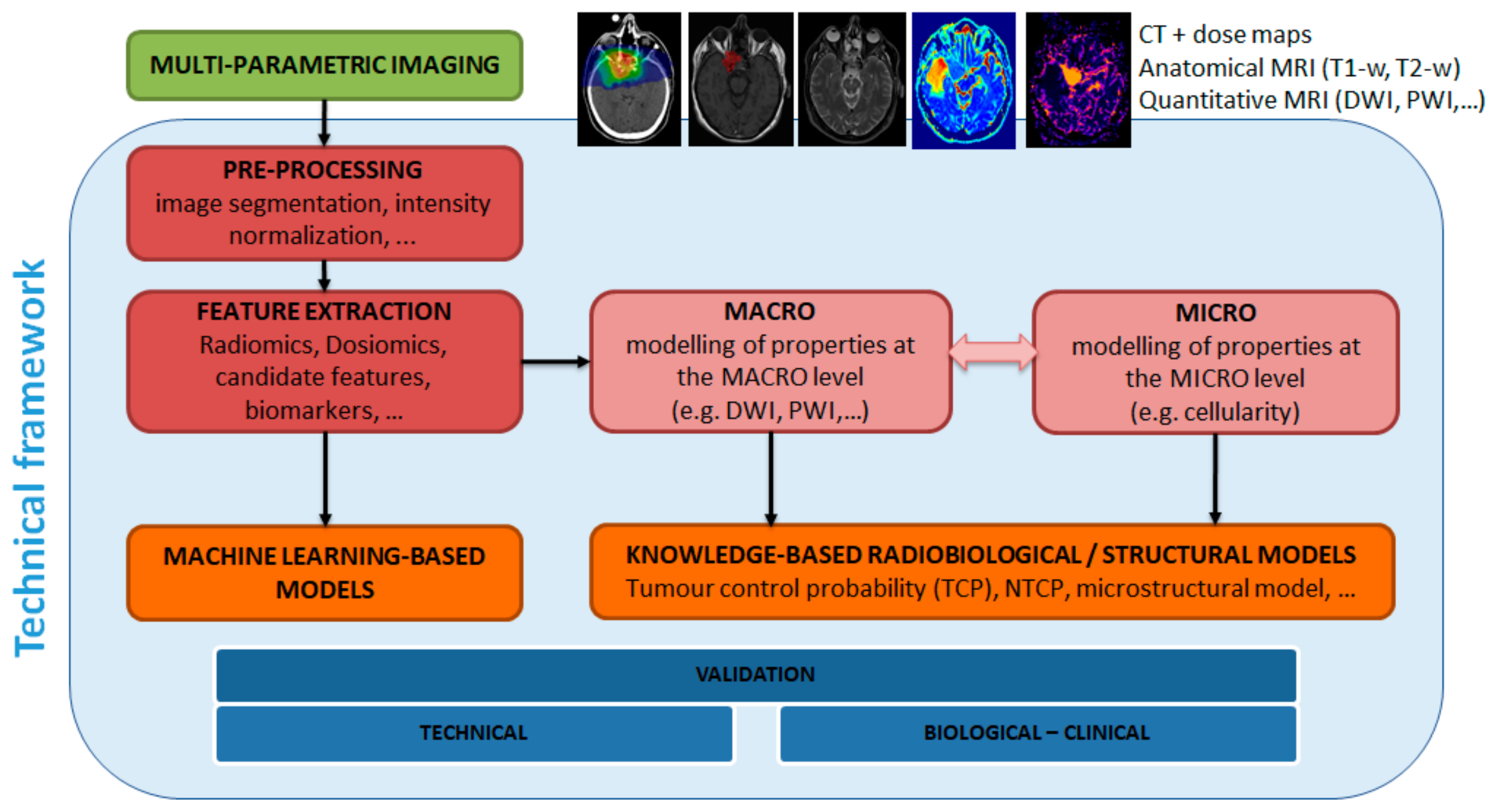
3.1. Modelling and Methodologies for a Patient Specific Therapy
3.2. Treatment Planning, Monte Carlo and Adaptive Protocols at CNAO
4. Results
4.1. Pre-Clinical Radiobiology Research
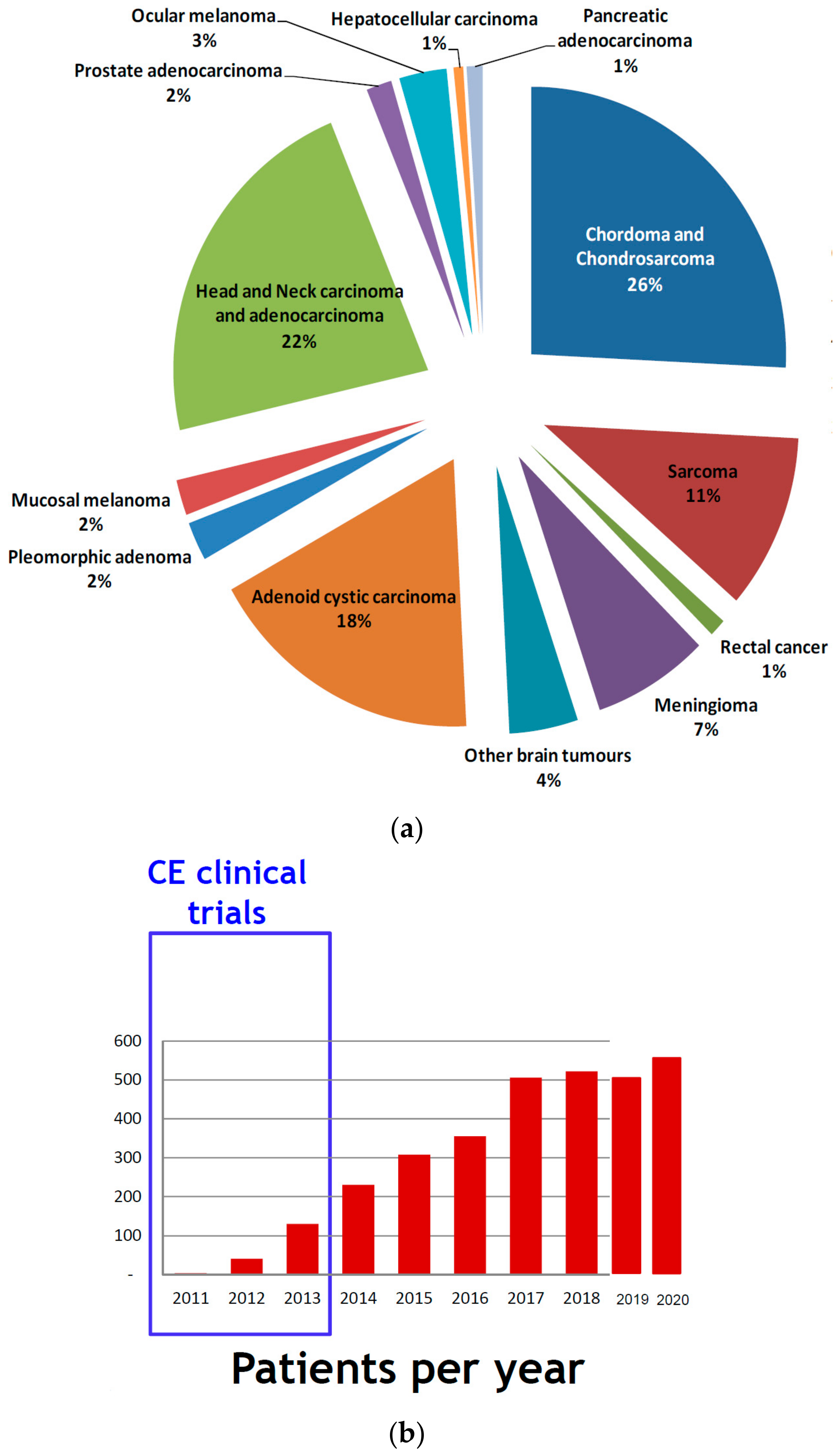
4.2. Clinical Activities: Pathologies and Results
- chordomas and chondrosarcomas (of the skull base and of the spine);
- meningioma;
- brain tumours (trunk);
- adenoid cystic carcinomas of the salivary glands;
- orbit tumours including eye melanoma;
- sino-nasal carcinomas;
- soft tissue and bone sarcomas (all sites);
- recurrent tumours (retreatment);
- patients with immunological disorders;
- paediatric solid tumours.
4.3. Skull Base Chordoma and Chondrosarcoma
4.4. Head-and-Neck Tumours
4.5. Malignant Mucosal Melanoma
4.6. Clinical Research Trials
- PIOPPO (preoperative treatment of borderline operable pancreatic adenocarcinomas with chemotherapy and radiotherapy with carbon ions) [96]: a phase 2 study, to evaluate the neo-adjuvant combination approach with chemotherapy followed by short-course carbon-ion radiotherapy for borderline pancreatic adenocarcinomas [97];
- CYCLE (carbon ion radiation therapy in the treatment of mucosal melanomas of the female lower genital tract): a phase 2 study to test the efficacy and the tolerability of carbon-ion treatments of unresectable gynaecological mucosal melanomas;
- CYCLOPS (Phase II clinical study on the re-irradiation of lateral pelvic recurrences of gynecological malignancies) a phase 2 study, to evaluate the efficacy and tolerability of carbon-ion re-irradiation for not central relapses of gynaecological neoplasms at the edge of the previous photon beam radiotherapy;
- 4D-MRI (guidance for organ motion management in particle treatments of thoraco-abdominal tumours): a clinical trial to study the organ motion of thoraco-abdominal neoplasms through 4D MRI;
- INSIDE: an experimental observational real-time live study of the particle range. This study is aimed at the early identification of potential morphological modifications of the target or of the adjacent areas, which might cause an anomaly in the dose distribution.
- STOPSTORM (a prospective European validation cohort for stereotactic therapy of Re-entrant tachycardia): aimed at the definition and harmonization of ventricular tachycardia radiation therapy treatment options (both medical and ablation therapy); to note that, at the end of 2019, in collaboration with Fondazione IRCSS Polyclinic San Matteo of Pave, for the first time in the literature, a patient affected by ventricular tachycardia (VT) has been successfully treated with proton beams at CNAO [98].
- PROTECT (PROton versus photon Therapy for Esophageal Cancer—a Trimodality strategy): a randomized clinical study aimed at building scientific evidence (in terms of efficacy and toxicity) on the proton pre-op treatment, combined with chemotherapy, for oesophageal cancer. This clinical trial is then compared to the current gold standard treatment, which is a combination of chemotherapy and IMRT.
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Haberer, T. Ion Beam Therapy at HIT: Options for Multi-Ion Treatment and Research. In Talk at the 3rd HITRIplus Seminar; Heidelberg University Hospital: Heidelberg, Germany, 13 October 2021; Available online: https://indico.cern.ch/event/1081649/ (accessed on 30 November 2021).
- Krämer, K.; Durante, M. Ion beam transport calculations and treatment plans in particle therapy. Eur. Phys. J. 2010, 60, 195–202. [Google Scholar] [CrossRef]
- Suit, H.; DeLaney, T.; Goldberg, S.; Paganetti, H.; Clasie, B.; Gerweck, L.; Niemierko, A.; Hall, E.; Flanz, J.; Hallman, J.; et al. Proton vs carbon ion beams in the definitive radiation treatment of cancer patients. Radiother. Oncol. 2010, 95, 3–22. [Google Scholar] [CrossRef] [PubMed]
- Durante, M.; Loeffler, J.S. Charged particles in radiation oncology. Pub. Med. 2009, 7, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Averbeck, N.B.; Topsch, J.; Scholz, M.; Kraft-Weyrather, W.; Durante, M.; Taucher-Scholz, G. Efficient Rejoining of DNA Double-strand breaks despite increased cell-killing effectiveness following spread-out bragg peak carbon-ion irradiation. Front. Oncol. 2016, 6, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Chiblak, S.; Tang, Z.; Campos, B.; Gal, Z.; Unterberg, A.; Debus, J.; Herold-Mendel, C.; Abdollahi, A. Radiosensitivity of patient-derived glioma stem cell 3-dimensional cultures to photon, proton, and carbon irradiation. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 112–119. [Google Scholar] [CrossRef]
- Peschke, P.; Debus, J. Relative biological effectiveness of carbon ions for local tumor control of a radioresistant prostate carcinoma in the rat. Int. J. Radiat. Oncol. Biol Phys. 2011, 79, 239–246. [Google Scholar] [CrossRef]
- Debus, J.; Abdollahi, A. For the next trick: New discoveries in radiobiology applied to glioblastoma. Am. Soc. Clin. Oncol. Educ. Book 2014, 34, e95–e99. [Google Scholar] [CrossRef] [Green Version]
- Klein, C.; Dokic, I.; Mairani, A.; Mein, S.; Brons, S.; Haring, P.; Haberer, T.; Jakel, O.; Zimmerman, A.; Zenke, F.; et al. Overcoming hypoxia-induced tumor radiore-sistance in non-small cell lung cancer by tar-geting DNA-dependent protein kinase in com-bination with carbon ion irradiation. Radiat. Oncol. 2017, 12, 208. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, Y.; Teshima, T.; Kawaguchi, N.; Hamada, Y.; Mori, S.; Madachi, A.; Ikeda, S.; Mizuno, H.; Ogata, T.; Nojima, K.; et al. Heavy ion irradiation inhibits in vitro angiogenesis even at sublethal dose. Cancer Res. 2003, 63, 4253–4257. [Google Scholar]
- Kamlah, F.; Hänze, J.; Arenz, A.; Seay, U.; Hasan, D.; Juricko, J.; Bischoff, B.; Gottschald, O.R.; Fournier, C.; Taucher-Scholz, G.; et al. Comparison of the effects of carbon ion and photon irradiation on the angiogenic response in human lung adenocarcinoma cells. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 1541–1549. [Google Scholar] [CrossRef]
- Ogata, T.; Teshima, T.; Kagawa, K.; Teshima, T.; Kagawa, K.; Hishikawa, Y.; Takahashi, Y.; Kawaguchi, A.; Suzumoto, Y.; Nojima, K.; et al. Particle irradiation suppresses metastatic potential of cancer cells. Cancer Res. 2005, 65, 113–120. [Google Scholar] [PubMed]
- Rieken, S.; Rieber, J.; Brons, S.; Rieber, J.; Brons, S.; Habermehl, D.; Rief, H.; Orschiedt, L.; Lindel, K.; Weber, K.J.; et al. Radiation-induced motility alterations in medulloblastoma cells. J. Radiat. Res. 2015, 56, 430–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durante, M.; Brenner, D.J.; Formenti, S.C. Does heavy ion therapy work through the immune system? Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 934–936. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.R. Radiological use of fast protons. Radiology 1946, 47, 487–491. [Google Scholar] [CrossRef]
- Slater, J.M.; Archambeau, J.O.; Dicello, J.F.; Slate, J.D. Proton beam irradiation: Toward routin clinical utilization. In Hadrontherapy in Oncology: Proceedings of the First International Symposium on Hadrontherapy, Como, Italy, 18–21 October 1993; Amaldi, U., Larsson, B., Eds.; Elsevier Science: Amsterdam, The Netherland, 1994; p. 130. [Google Scholar]
- Kawachi, K.; Yamada, S.; Sato, K.; Ogawa, H.; Soga, F.; Kanai, T.; Endo, M.; Hirao, Y. Heavy ion medical accelerator facility in Japan. In Hadrontherapy in Oncology: Proceedings of the First International Symposium on Hadrontherapy, Como, Italy, 18–21 October 1993; Amaldi, U., Larsson, B., Eds.; Elsevier Science: Amsterdam, The Netherlands, 1994; p. 229. [Google Scholar]
- ENLIGHT. ENLIGHT Coordination. Available online: https://enlight.web.cern.ch/enlight (accessed on 30 November 2021).
- An Organization for Those Interested in Proton, Light Ion and Heavy Charged Particle Radiotherapy. Particle Therapy Co-Operative Group. Available online: www.ptcog.ch (accessed on 30 November 2021).
- NIMMS—Next Ion Medical Machine Study. CERN. Available online: https://kt.cern/kt-fund/projects/nimms-next-ion-medical-machine-study (accessed on 30 November 2021).
- CERN. I.FAST. Available online: https://ifast-project.eu/home (accessed on 30 November 2021).
- Mizushima, K.; Shirai, T.; Iwata, Y.; Furukawa, T.; Noda, K. Design of a Superconducting Synchrotron for Heavy-Ion Radiotherapy. In Proceedings of the 14th Annual Meeting of Particle Accelerator Society of Japan, Sapporo, Japan, 1–3 August 2017; pp. 1243–1245. Available online: https://www.pasj.jp/web_publish/pasj2017/proceedings/PDF/WEP1/WEP131.pdf (accessed on 30 November 2021). (In Japanese).
- Benedetto, E.; Harbi, N.A.; Brouwer, L.; Tommasini, D.; Prestemon, S.; Riboni, P.; Amaldi, U. A carbon ion superconducting gantry and a synchrotron based on canted cosine-theta magnets. arXiv 2021, arXiv:2105.04205. [Google Scholar]
- Amaldi, U.; Alharbi, N.; Benedetto, E.; Riboni, P.; Vaziri, M.; Aguglia, D.; Ferrentino, V.; Le Godec, G.; Karppinen, M.; Perini, D.; et al. SIGRUM—A Superconducting Ion Gantry with Riboni’s Unconventional Mechamiics. CERN-ACC-NOTE-2021-0014 and NIMMS-Note-002. Available online: https://cds.cern.ch/record/2766876 (accessed on 30 November 2021).
- Badano, L.; Benedikt, M.; Bryant, P.J.; Crescenti, M.; Holy, P.; Maier, A.T.; Pullia, M.; Rossi, S.; Knaus, P. Proton-Ion Medical Machine Study (PIMMS). Part I; Report CERN/PS 99-010 (DI); CERN: Geneva, Switzerland, 1999; Available online: https://cds.cern.ch/record/385378 (accessed on 30 November 2021).
- Bryant, P.J.; Badano, L.; Benedikt, M.; Crescenti, M.; Holy, P.; Maier, A.T.; Pullia, M.; Reimoser, S.; Rossi, S.; Borri, G.; et al. Proton-Ion Medical Machine Study (PIMMS). Part II; Report CERN/PS 2000-007 (DR); CERN: Geneva, Switzerland, 2000; Available online: https://cds.cern.ch/record/449577 (accessed on 30 November 2021).
- Amaldi, U.; Magrin, G. (Eds.) The Path to the Italian National Centre for Ion Therapy; Edizioni Mercurio: Vercelli, Italy, 2005. [Google Scholar]
- Rossi, S. The status of CNAO. Eur. Phys. J. Plus 2011, 126, 78. [Google Scholar] [CrossRef]
- Fattori, G.; Riboldi, M.; Pella, A.; Peroni, M.; Cerveri, P.; Desplanques, M.; Fontana, G.; Tagaste, B.; Valvo, F.; Orecchia, R.; et al. Image guided particle therapy in CNAO room 2: Implementation and clinical validation. Phys. Med. 2015, 31, 9–15. [Google Scholar] [CrossRef]
- Fattori, G.; Seregni, M.; Pella, A.; Riboldi, M.; Capasso, L.; Donetti, M.; Ciocca, M.; Giordanengo, S.; Pullia, M.; Marchetto, F.; et al. Real-time optical tracking for motion compensated irradiation with scanned particle beams at CNAO. Nucl. Instrum. Meth. Phys. Res. A Accel. Spectrom. Detect. Assoc. Equip. 2016, 827, 39–45. [Google Scholar] [CrossRef]
- Via, R.; Fassi, A.; Fattori, G.; Fontana, G.; Pella, A.; Tagaste, B.; Riboldi, M.; Ciocca, M.; Orecchia, R.; Baroni, G. Optical eye tracking system for real-time noninvasive tumor localization in external beam radiotherapy. Med. Phys. 2015, 42, 2194–2202. [Google Scholar] [CrossRef]
- Seregni, M.; Paganelli, C.; Summers, P.; Bellomi, M.; Baroni, G.; Riboldi, M. A hybrid image registration and matching framework for real-time motion tracking in MRI-guided radiotherapy. IEEE Trans. Biomed. Eng. 2018, 65, 131–139. [Google Scholar] [CrossRef]
- Radiation Therapy. LEO Cancer Care. Available online: www.leocancercare.com (accessed on 30 November 2021).
- Molinelli, S.; Magro, G.; Mairani, A.; Matsufuji, N.; Kanematsu, N.; Inaniwa, T.; Mirandola, A.; Russo, S.; Mastella, E.; Hasegawa, A.; et al. Dose prescription in carbon ion radiotherapy: How to compare two different RBE-weighted dose calculation systems. Radiother. Oncol. 2016, 120, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Fossati, P.; Molinelli, S.; Matsufuji, N.; Ciocca, M.; Mirandola, A.; Mairani, A.; Mizoe, J.; Hasegawa, A.; Imai, R.; Kamada, T.; et al. Dose prescription in carbon ion radiotherapy: A planning study to compare NIRS and LEM approaches with a clinically-oriented strategy. Phys. Med. Biol. 2012, 57, 7543–7554. [Google Scholar] [CrossRef] [PubMed]
- Meschini, G.; Seregni, M.; Pella, A.; Ciocca, M.; Fossati, P.; Valvo, F.; Riboldi, M.; Baroni, G. Evaluation of residual abdominal tumour motion in carbon ion gated treatments through respiratory motion modelling. Phys. Med. 2017, 34, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Ciocca, M.; Mirandola, A.; Molinelli, S.; Russo, S.; Mastella, E.; Vai, A.; Mairani, A.; Magro, G.; Pella, A.; Donetti, M.; et al. Commissioning of the 4-D treatment delivery system for organ motion management in synchrotron-based scanning ion beams. Phys. Med. 2016, 32, 1667–1671. [Google Scholar] [CrossRef] [PubMed]
- Meschini, G.; Paganelli, C.; Vai, A.; Fontana, G.; Molinelli, S.; Pella, A.; Vitolo, V.; Barcellini, A.; Orlandi, E.; Ciocca, M.; et al. An MRI framework for respiratory motion modelling validation. J. Med. Imaging Radiat. Oncol. 2021, 65, 337–344. [Google Scholar] [CrossRef] [PubMed]
- PANTECHNIK. ECR ION SOURCES. Available online: https://www.pantechnik.com/ecr-ion-sources/ (accessed on 30 November 2021).
- Hub Research and Innovation, POR FESR 2014-2020, ID 1161908. Available online: https://home.infn.it/en/media-outreach/infn-newsletter/newsletter-interview/4680-interview-valerio-vercesi-2 (accessed on 30 November 2021).
- Celona, L.; Ciavola, G.; Gammino, S.; Andò, L.; Mascali, D. Design of the AISHA Ion Source for Hadrontherapy Facilities. In Proceedings of the 20th International Workshop on ECR Ion Sources, ECRIS2012, Sydney, Australia, 25–28 September 2012; pp. 54–56. Available online: https://accelconf.web.cern.ch/ECRIS2012/papers/tupp08.pdf (accessed on 30 November 2021).
- Bisogni, M.G. The INSIDE bimodal system for range monitoring in particle therapy toward clinical validation. Nucl. Instrum. Meth. Phys. Res. A Accel. Spectrom. Detect. Assoc. Equip. 2019, 936, 73–74. [Google Scholar] [CrossRef]
- Traini, G.; Mattei, I.; Battistoni, G.; Bisogni, M.; De Simoni, M.; Dong, Y.; Embriaco, A.; Fischetti, M.; Magi, M.; Mancini-Terracciano, C.; et al. Review and performance of the Dose Profiler, a particle therapy treatments online monitor. Phys. Med. 2019, 65, 84–93. [Google Scholar] [CrossRef]
- Ferrero, V.; Fiorina, E.; Morrocchi, M.; Pennazio, F.; Baroni, G.; Battistoni, G.; Belcari, N.; Camarlinghi, N.; Ciocca, M.; del Guerra, A.; et al. Online proton therapy monitoring: Clinical test of a Silicon-photodetectorbased in-beam PET. Sci. Rep. 2018, 8, 4100. [Google Scholar] [CrossRef]
- Fiorina, E.; Ferrero, V.; Pennazio, F.; Baroni, G.; Battistoni, G.; Belcari, N.; Cerello, P.; Camarlinghi, N.; Ciocca, M.; Del Guerra, A.; et al. Monte Carlo simulation tool for online treatment monitoring in hadrontherapy with in-beam PET: A patient study. Phys. Med. 2018, 51, 71–80. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. The U.S. National Library of Medicine. ID: NCT03662373. Available online: https://ClinicalTrials.gov (accessed on 30 November 2021).
- Fiorina, E.; Ferrero, V.; Baroni, G.; Battistoni, G.; Belcari, N.; Camarlinghi, N.; Cerello, P.; Ciocca, M.; De Simoni, M.; Donetti, M.; et al. Detection of interfractional morphological changes in proton therapy: A simulation and in vivo study with the INSIDE in-beam PET. Front. Phys. 2021, 8, 660. [Google Scholar] [CrossRef]
- Kraan, A.C.; Berti, A.; Retico, A.; Baroni, G.; Battistoni, G.; Belcari, N.; Cerello, P.; Ciocca, M.; de Simoni, M.; del Sarto, D.; et al. Localization of anatomical changes in patients during proton theraphy with in-beam PET monitoring: A Voxel Based Morphometry approach exploiting Monte Carlo simulations. Med. Phys. 2022, 49, 23–40. [Google Scholar] [CrossRef] [PubMed]
- Fischetti; Baroni, G.; Battistoni, G.; Bisogni, G.; Cerello, P.; Ciocca, M.; de Maria, P.; de Simoni, M.; di Lullo, B.; Donetti, M.; et al. Inter-fractional monitoring of 12C ions treatments: Results from a clinical trial at the CNAO facility. Sci. Rep. 2020, 10, 20735. [Google Scholar] [CrossRef] [PubMed]
- Toppi, M.; Baroni, G.; Battistoni, G.; Bisogni, M.G.; Cerello, P.; Ciocca, M.; De Maria, P.; De Simoni, M.; Donetti, M.; Dong, Y.; et al. Monitoring carbon ion beams transverse position detecting charged secondary fragments: Results from patient treatment performed at CNAO. Front. Oncol. 2021, 11, 601784. [Google Scholar] [CrossRef] [PubMed]
- Lis, M.; Newhauser, W.; Donetti, M.; Wolf, M.; Steinsberger, T.; Paz, A.; Graeff, C. Preliminary tests of dosimetric quality and projected therapeutic outcomes of multi-phase 4D radiotherapy with proton and carbon ion beams. Phys. Med. Biol. 2021, 66, 23. [Google Scholar] [CrossRef]
- Favaudon, V.; Caplier, L.; Monceau, V.; Pouzoulet, F.; Sayarath, M.; Fouillade, C.; Poupon, M.-F.; Brito, I.; Hupé, P.; Bourhis, J.; et al. Ultrahigh dose-rate FLASH irradiation increases the differential response between normal and tumor tissue in mice. Sci. Transl. Med. 2014, 6, 245ra93. [Google Scholar] [CrossRef]
- Haberer, T.; Becher, W.; Schardt, D.; Kraft, G. Magnetic scanning system for heavy ion therapy. Nucl. Instrum. Meth. Phys. Res. A Accel. Spectrom. Detect. Assoc. Equip. 1993, 330, 296–305. [Google Scholar] [CrossRef]
- Haberer, T.; Debus, J.; Eickhoff, H.; Jäkel, O.; Schulz-Ertner, D.; Weber, U. The Heidelberg Ion Therapy Center. Radiother. Oncol. 2004, 73 (Suppl. 2), S186–S190. [Google Scholar] [CrossRef]
- Schoemers, C.; Feldmeier, E.; Galonska, M.; Haberer, T.; Horn, J.; Peters, A. First tests of a re-accelerated beam at Heidelberg Ion-Beam Therapy Centre (HIT). In Proceedings of the 8th International Particle Accelerator Conference, IPAC2017, Copenhagen, Denmark, 14–19 May 2017; pp. 4647–4649. Available online: https://accelconf.web.cern.ch/ipac2017/papers/thpva083.pdf (accessed on 30 November 2021).
- Saverwein, W.; Wittig, A.; Moss, R.; Nakagawa, Y. Neutron Capture Therapy: Principles and Applications; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, M. Boron Neutron Capture Therapy (BNCT): A unique role in radiotherapy with a view to entering the accelerator-based BNCT era. Int. J. Clin. Oncol. 2020, 25, 43–50. [Google Scholar] [CrossRef]
- Buizza, G.; Paganelli, C.; D’ippolito, E.; Fontana, G.; Molinelli, S.; Preda, L.; Riva, G.; Iannalfi, A.; Valvo, F.; Orlandi, E.; et al. Radiomics and dosiomics for predicting local control after carbon-ion radiotherapy in skull-base chordoma. Cancers 2021, 13, 339. [Google Scholar] [CrossRef]
- Buizza, G.; Molinelli, S.; D’Ippolito, E.; Fontana, G.; Pella, A.; Valvo, F.; Preda, L.; Orecchia, R.; Baroni, G.; Paganelli, C. MRI-based tumour control probability in skull-base chordomas treated with carbon-ion therapy. Radiother. Oncol. 2019, 137, 32–37. [Google Scholar] [CrossRef]
- Zampini, M.; Buizza, G.; Paganelli, C.; Fontana, G.; D’Ippolito, E.; Valvo, F.; Preda, L.; Baroni, G. Perfusion and diffusion in meningioma tumors: A preliminary multiparametric analysis with Dynamic Susceptibility Contrast and IntraVoxel Incoherent Motion MRI. Magn. Reson. Imaging 2020, 67, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Monti, S.; Paganelli, C.; Buizza, G.; Preda, L.; Valvo, F.; Baroni, G.; Palma, G.; Cella, L. A novel framework for spatial normalization of dose distributions in voxel-based analyses of brain irradiation outcomes. Phys. Med. 2020, 69, 164–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buizza, G.; Zampini, M.A.; Riva, G.; Molinelli, S.; Fontana, G.; Imparato, S.; Ciocca, M.; Iannalfi, A.; Orlandi, E.; Baroni, G.; et al. Investigating DWI changes in white matter of meningioma patients treated with proton therapy. Phys. Med. 2021, 84, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Buizza, G.; Paganelli, C.; Ballati, F.; Sacco, S.; Preda, L.; Iannalfi, A.; Alexander, D.C.; Baroni, G.; Palombo, M. Improving the characterization of meningioma microstructure in proton therapy from conventional apparent diffusion coefficient measurements using Monte Carlo simulations of diffusion MRI. Phys. Med. 2021, 48, 1250–1261. [Google Scholar] [CrossRef] [PubMed]
- RaySearch Laboratories. ADVANCING CANCER TREATMENT. Available online: www.raysearchlabs.com (accessed on 30 November 2021).
- Molinelli, S.; Russo, S.; Magro, G.; Maestri, D.; Mairani, A.; Mastella, E.; Mirandola, A.; Vai, A.; Vischioni, B.; Valvo, F.; et al. Impact of TPS calculation algorithms on dose delivered to the patient in proton therapy treatments. Phys. Med. Biol. 2019, 64, 075016. [Google Scholar] [CrossRef] [PubMed]
- Molinelli, S.; Bonora, M.; Magro, G.; Casale, S.; Dale, J.E.; Fossati, P.; Hasegawa, A.; Mirandola, A.; Ronchi, S.; Russo, S.; et al. RBE-weighted dose in carbon ion therapy for ACC patients: Impact of the RBE model translation on treatment outcomes. Radiother. Oncol. 2019, 141, 227–233. [Google Scholar] [CrossRef]
- Molinelli, S.; Magro, G.; Mairani, A.; Allajbej, A.; Mirandola, A.; Chalaszczyk, A.; Imparato, S.; Ciocca, M.; Fiore, M.R.; Orlandi, E. How LEM-based RBE and dose-averaged LET affected clinical outcomes of sacral chordoma patients treated with carbon ion radiotherapy. Radiother. Oncol. 2021, 163, 209–214. [Google Scholar] [CrossRef]
- Russo, S.; Ricotti, R.; Molinelli, S.; Patti, F.; Barcellini, A.; Mastella, E.; Pella, A.; Paganelli, C.; Marvaso, G.; Pepa, M.; et al. Dosimetric impact of inter-fraction anatomical changes in carbon ion boost treatment for high-risk prostate cancer (AIRC IG 14300). Front. Oncol. 2021, 11, 740661. [Google Scholar] [CrossRef]
- Meschini, G.; Vai, A.; Paganelli, C.; Molinelli, S.; Maestri, D.; Fontana, G.; Pella, A.; Vitolo, V.; Valvo, F.; Ciocca, M.; et al. Investigating the use of virtual 4DCT from 4DMRI in gated carbon ion radiation therapy of abdominal tumors. Med. Phys. 2020, in press. [Google Scholar] [CrossRef]
- RAPTOR. ITN. Available online: https://raptor-consortium.com (accessed on 30 November 2021).
- Loap, P.; Mirandola, A.; De Marzi, L.; Vitolo, V.; Barcellini, A.; Iannalfi, A.; Dendale, R.; Kirova, Y.; Orlandi, E. Cardiac conduction system exposure with modern radiotherapy techniques for mediastinal Hodgkin lymphoma irradiation. Acta Oncol. 2022, 1–4. [Google Scholar] [CrossRef]
- Loeffler, J.S.; Durante, M. Charged particle therapy—optimization, challenges and future directions. Nat. Rev. Clin. Oncol. 2013, 10, 411–424. [Google Scholar] [CrossRef] [PubMed]
- Fujita, M.; Yamada, S.; Imai, T. Irradiation induces diverse changes in invasive potential in cancer cell lines. Semin. Cancer Biol. 2015, 35, 45–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Facoetti, A.; Di Gioia, C.; Pasi, F.; Di Liberto, R.; Corbella, F.; Nano, R.; Ciocca, M.; Valvo, F.; Orecchia, R. Morphological analysis of amoeboid-mesenchymal transition plasticity after low and high LET radiation on migrating and invading pancreatic cancer cells. Anticancer Res. 2018, 38, 4585–4591. [Google Scholar] [CrossRef] [PubMed]
- Croce, S.; Peloso, A.; Zoro, T.; Avanzini, M.A.; Cobianchi, L. A Hepatic scaffold from decellularized liver tissue: Food for thought. Biomolecules 2019, 9, 813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; Zhu, Z.-L.; Gao, X.-L.; Wu, J.-S.; Liang, X.-H.; Tang, Y.-L. Functions of chemokines in the perineural invasion of tumors (Review). Int. J. Oncol. 2018, 52, 1369–1379. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, M.F.; Corso, S. Patient-derived cancer models. Cancers 2020, 12, 3779. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, T.; Henthorn, N.; Durante, M. Modeling radioimmune response-current status and perspectives. Front. Oncol. 2021, 11, 647272. [Google Scholar] [CrossRef]
- Iannalfi, A.; D’Ippolito, E.; Riva, G.; Molinelli, S.; Gandini, S.; Viselner, G.; Fiore, M.R.; Vischioni, B.; Vitolo, V.; Bonora, M.; et al. Proton and carbon ion radiotherapy in skull base chordomas: A prospective study based on a dual particle and a patient-customized treatment strategy. Neurol. Oncol. 2020, 22, 1348–1358. [Google Scholar] [CrossRef]
- Van Dijk, B.A.; Gatta, G.; Capocaccia, R.; Pierannunzio, D.; Strojan, P.; Licitra, L.; The RARECARE Working Group. Rare cancers of the head and neck area in Europe. Eur. J. Cancer 2012, 48, 783–796. [Google Scholar] [CrossRef]
- El-Naggar, A.K.; Chan, J.F.K.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO Classification of Head and Neck Tumours, 4th ed.; World Health Organization: Geneva, Switzerland, 2017; Volume 9. [Google Scholar]
- Vischioni, B.; Dhanireddy, B.; Severo, C.; Bonora, M.; Ronchi, S.; Vitolo, V.; Fiore, M.R.; D’Ippolito, E.; Petrucci, R.; Barcellini, A.; et al. Reirradiation of salivary gland tumors with carbon ion radiotherapy at CNAO. Radiother. Oncol. 2020, 145, 172–177. [Google Scholar] [CrossRef]
- Loap, P.; Vischioni, B.; Bonora, M.; Ingargiola, R.; Ronchi, S.; Vitolo, V.; Barcellini, A.; Goanta, L.; De Marzi, L.; Dendale, R.; et al. Biological rationale and clinical evidence of carbon ion radiation therapy for adenoid cystic carcinoma: A narrative review. Front. Oncol. 2021, 11, 789079. [Google Scholar] [CrossRef] [PubMed]
- RARECAREnet. Information Network on Rare Cancers. 2017. Available online: http://www.rarecarenet.eu/rarecarenet/ (accessed on 30 November 2021).
- Kirchoff, D.D.; Deutsch, G.B.; Foshag, L.J.; Lee, J.H.; Sim, M.-S.; Faries, M.B. Evolving therapeutic strategies in mucosal melanoma have notiImproved survival over five decades. Am. Surg. 2016, 82, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Teterycz, P.; Czarnecka, A.M.; Indini, A.; Spałek, M.J.; Labianca, A.; Rogala, P.; Cybulska-Stopa, B.; Quaglino, P.; Ricardi, U.; Badellino, S.; et al. Multimodal treatment of advanced mucosal melanoma in the era of modern immunotherapy. Cancers 2020, 12, 3131. [Google Scholar] [CrossRef] [PubMed]
- Gadducci, A.; Carinelli, S.; Guerrieri, M.E.; Aletti, G.D. Melanoma of the lower genital tract: Prognostic factors and treatment modalities. Gynecol. Oncol. 2018, 150, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Penel, N.; Mallet, Y.; Mirabel, X.; Van, J.T.; Lefebvre, J.-L. Primary mucosal melanoma of head and neck: Prognostic value of clear margins. Laryngoscope 2006, 116, 993–995. [Google Scholar] [CrossRef]
- Shuman, A.G.; Light, E.; Olsen, S.H.; Pynnonen, M.A.; Taylor, J.M.; Johnson, T.M.; Bradford, C.R. Mucosal melanoma of the head and neck: Predictors of prognosis. Arch. Otolaryngol. Head Neck Surg. 2011, 137, 331–337. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.P.; Shimizu, K.T.; Tran, L.M.; Juillard, G.; Calcaterra, T.C. Mucosal melanoma of the head and neck: The impact of local control on survival. Laryngoscope 1994, 104, 121–126. [Google Scholar] [CrossRef]
- Ebner, D.K.; Malouff, T.D.; Frank, S.J.; Koto, M. The role of particle therapy in adenoid cystic carcinoma and mucosal melanoma of the head and neck. Int. J. Part Ther. 2021, 8, 273–284. [Google Scholar] [CrossRef]
- Murata, H.; Okonogi, N.; Wakatsuki, M.; Kato, S.; Kiyohara, H.; Karasawa, K.; Ohno, T.; Nakano, T.; Kamada, T.; Shozu, M.; et al. Long-term outcomes of carbon-ion radiotherapy for malignant gynecological melanoma. Cancers 2019, 11, 482. [Google Scholar] [CrossRef] [Green Version]
- Barcellini, A.; Vitolo, V.; Facoetti, A.; Fossati, P.; Preda, L.; Fiore, M.R.; Vischioni, B.; Iannalfi, A.; Bonora, M.; Ronchi, S.; et al. Feasibility of carbon ion radiotherapy in the treatment of gynecological melanoma. In Vivo 2019, 33, 473–476. [Google Scholar] [CrossRef] [Green Version]
- Takayasu, Y.; Kubo, N.; Shino, M.; Nikkuni, O.; Ida, S.; Musha, A.; Takahashi, K.; Hirato, J.; Shirai, K.; Saitoh, J.; et al. Working Group on Head and Neck Tumors. Carbon-ion radiotherapy combined with chemotherapy for head and neck mucosal melanoma: Prospective observational study. Cancer Med. 2019, 8, 7227–7235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalieri, S.; Ronchi, S.; Barcellini, A.; Bonora, M.; Vischioni, B.; Vitolo, V.; Villa, R.; Del Vecchio, M.; Licitra, L.; Orlandi, E. Toxicity of carbon ion radiotherapy and immune checkpoint inhibitors in advanced melanoma. Radiother. Oncol. 2021, 164, 1–5. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. The U.S. National Library of Medicine. ID: NCT03822936. Available online: https://ClinicalTrials.gov (accessed on 30 November 2021).
- Vitolo, V.; Cobianchi, L.; Brugnatelli, S.; Barcellini, A.; Peloso, A.; Facoetti, A.; Vanoli, A.; Delfanti, S.; Preda, L.; Molinelli, S.; et al. Preoperative chemotherapy and carbon ions therapy for treatment of resectable and borderline resectable pancreatic adenocarcinoma: A prospective, phase II, multicentre, single-arm study. BMC Cancer 2019, 19, 922. [Google Scholar] [CrossRef] [PubMed]
- Dusi, V.; Vitolo, V.; Frigerio, L.; Totaro, R.; Valentini, A.; Barcellini, A.; Mirandola, A.; Perego, G.B.; Coccia, M.; Greco, A.; et al. First-in-man case of non-invasive proton radiotherapy for the treatment of refractory ventricular tachycardia in advanced heart failure. Eur. J. Heart Fail. 2020, 23, 195–196. [Google Scholar] [CrossRef] [PubMed]
- Niemierko, A.; Goitein, M. Calculation of normal tissue complication probability and dose-volume histogram reduction schemes for tissues with a critical element architecture. Radiother. Oncol. 1991, 20, 166–176. [Google Scholar] [CrossRef]
- Langendijk, J.A.; Lambin, P.; De Ruysscher, D.; Widder, J.; Bos, M.; Verheij, M. Selection of patients for radiotherapy with protons aiming at reduction of side effects: The model-based approach. Radiother. Oncol. 2013, 107, 267–273. [Google Scholar] [CrossRef] [Green Version]
- Langendijk, J.A.; Hoebers, F.J.P.; de Jong, M.A.; Doornaert, P.; Terhaard, C.H.J.; Steenbakkers, R.J.H.M.; Hamming-Vrieze, O.; van de Kamer, J.B.; Verbakel, W.F.A.R.; Keskin-Cambay, F.; et al. National protocol for model-based selection for proton therapy in head and neck cancer. Int. J. Part Ther. 2021, 8, 354–365. [Google Scholar] [CrossRef]
- Tambas, M.; Steenbakkers, R.J.H.M.; van der Laan, H.P.; Wolters, A.M.; Kierkels, R.G.J.; Scandurra, D.; Korevaar, E.W.; Oldehinkel, E.; van Zon-Meijer, T.W.H.; Both, S.; et al. First experience with model-based selection of head and neck cancer patients for proton therapy. Radiother. Oncol. 2020, 151, 206–213. [Google Scholar] [CrossRef]
- Dionisi, F.; Widesott, L.; Van Vulpen, M.; Fuller, C.D.; Frondizi, R.; Meneguzzo, M.; Blanchard, P.; Amichetti, M.; Sanguineti, G. Methodologies to increase the level of evidence of real-life proton therapy in head and neck tumors. Int. J. Part Ther. 2021, 8, 328–338. [Google Scholar] [CrossRef]
- Orlandi, E.; Dal Mas, F.; Paoloni, P.; Band, H.; Fiore, M.R.; Vischioni, B.; Vitolo, V.; Campo, C.; Facoetti, A.; Necchi, M.; et al. A short reflection on COVID-19 and gender equality in healthcare. In Organizational Resilience and Female Entrepreneurship During Crises. Emerging Evidence and Future Agenda; Paoloni, P., Lombardi, R., Eds.; Springer: Berlin/Heidelberg, Germany, 2022. [Google Scholar] [CrossRef]
- Paoloni, P.; Dal Mas, F.; Massaro, M.; Barcellini, A.; Orlandi, E. An Organizational model for female leadership in healthcare. The National Centre of Oncological Hadrontherapy (CNAO Foundation) experience during the COVID-19 pandemic. In Proceedings of the 4th International Conference on Gender Research, ICGR 2021, Aveiro, Portugal, 21–22 June 2021; Pereira, E.T., Costa, C., Breda, Z., Eds.; Academic Conferences and Publishing International Limited: Reading, UK, 2021; pp. 228–237. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Beam particle species | p, He2+, Li3+, Be4+, B5+, C6+, O8+ |
| Beam particle switching time | ≤10 min |
| Beam range | 1.0 g/cm2 to 27 g/cm2 in one treatment room |
| 3.1 g/cm2 to 27 g/cm2 in two treatment rooms | |
| Up to 20 g/cm2 for O8+ ions | |
| Bragg peak modulation steps | 0.1 g/cm2 |
| Range adjustment | 0.1 g/cm2 |
| Adjustment/modulation accuracy | ≤±0.025 g/cm2 |
| Average dose rate | 2 Gy/min (for treatment volumes of 1000 cm3) |
| Delivery dose precision | ≤±2.5 % |
| Beam axis height (above floor) | 150 cm (head and neck beam line) |
| 120 cm (elsewhere) | |
| Beam size 1 | 4 to 10 mm FWHM for each direction independently |
| Beam size step 1 | 1 mm |
| Beam size accuracy 1 | ≤±0.25 mm |
| Beam position step 1 | 0.8 mm |
| Beam position accuracy 1 | ≤±0.2 mm |
| Field size 1 | 5 mm to 34 mm (diameter for ocular treatments) |
| 2 × 2 cm2 to 20 × 20 cm2 (for H and V fixed beams) | |
| Field position accuracy 1 | ≤±0.5 mm |
| Field dimensions accuracy 1 | 1 mm |
| Field size accuracy 1 | ≤±0.5 mm |
| Years from 2011 to 2021 | Years 2021 (Estimate) |
|---|---|
| 3401 running days | 329 dd |
| 2495 treatment days | 242 dd |
| 247 dd ordinary maintenance | 29 dd |
| 37 dd system breakdown | 0 dd |
| System availability: 90.6% | 90.1% |
| System reliability (dd): 98.5% | 100% |
| System reliability (sessions) | 99.4% 161 (32 + 129) vs. 10.034 |
| Ion | ECR Sources (eμA) | AISHa (eμA) |
|---|---|---|
| H+ | 2000 | 4000 |
| H2+ | 1200 | 2000 |
| H3+ | 1000 | 1500 |
| 3He+ | 800 | 2000 |
| 12C4+ | 250 | 800 |
| 6Li2+-7Li2+ | — | 800 |
| 10B3+-11B3+ | — | 600 |
| 16O6+ | 400 | 1200 |
| 21Ne7+ | 120 | 500 |
| 40Ar12+ | 20 | 140 |
| Item | Specification |
|---|---|
| Accelerator | Synchrotron |
| Species | Proton |
| Energy | 70–230 MeV |
| Maximum range | 32 g/cm2 |
| Minimum range | 4 g/cm2 |
| Maximum field size at isocentre | 40 cm × 30 cm |
| Dose rate | ≥1.4 Gy/min |
| Range modulation method | Energy stacking by energy change with accelerator or change of range shifter thickness |
| Gantry | 360 degrees rotating gantry |
| Robotic couch | 6 DOF swing robotic couch with error correction |
| Imaging | Orthogonal imaging device (radiography, fluoroscopy, CBCT with real time imaging capability) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, S. Hadron Therapy Achievements and Challenges: The CNAO Experience. Physics 2022, 4, 229-257. https://doi.org/10.3390/physics4010017
Rossi S. Hadron Therapy Achievements and Challenges: The CNAO Experience. Physics. 2022; 4(1):229-257. https://doi.org/10.3390/physics4010017
Chicago/Turabian StyleRossi, Sandro. 2022. "Hadron Therapy Achievements and Challenges: The CNAO Experience" Physics 4, no. 1: 229-257. https://doi.org/10.3390/physics4010017
APA StyleRossi, S. (2022). Hadron Therapy Achievements and Challenges: The CNAO Experience. Physics, 4(1), 229-257. https://doi.org/10.3390/physics4010017