

Socket Shield Technique to Improve the Outcomes of Immediate Implant: A Systematic Review and Meta-Analysis

 ,
,  , ,
, ,  ,
, 
 and
and 
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
- Population: Adult healthy patients (≥18 years) who indicated immediate dental implantation after tooth extraction in the aesthetic area (i.e., incisors, canines, or premolars).
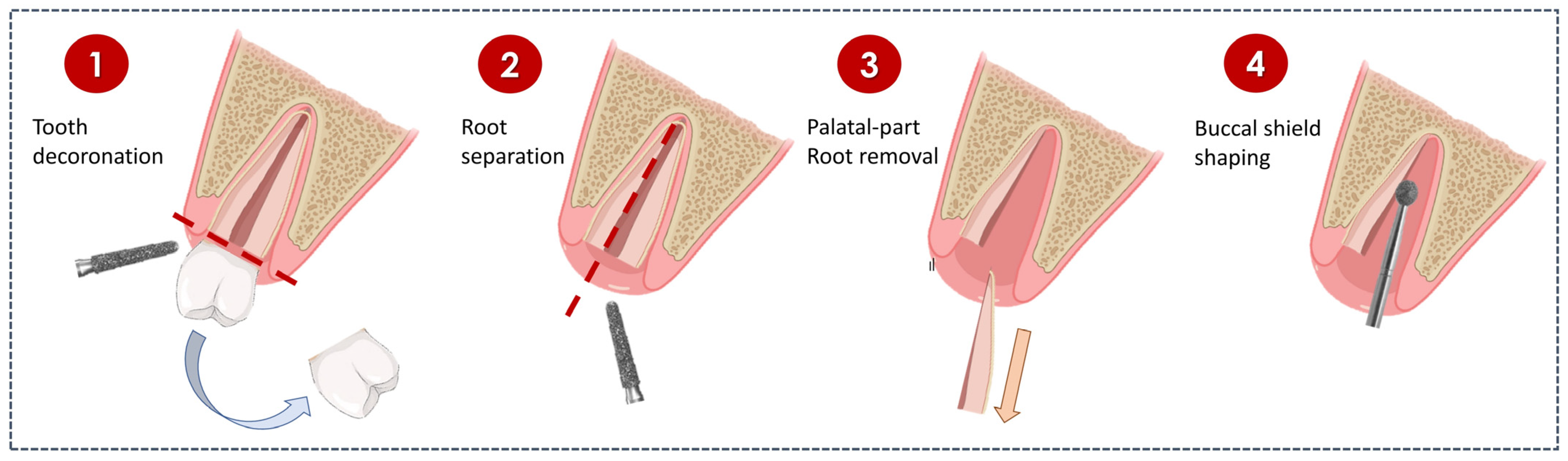
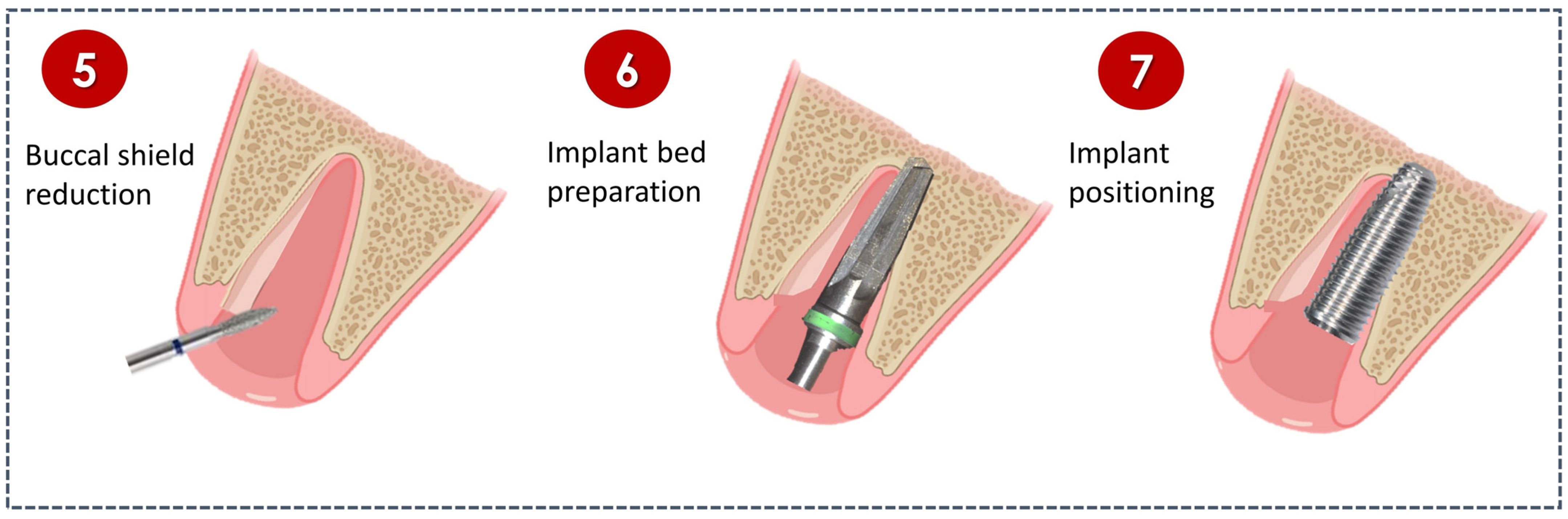
- Intervention: Immediate dental implantation with SST.
- Comparison: Immediate dental implantation without SST.
- Outcomes:
- ▪
- Horizontal bone loss (i.e., changes in buccal bone width), determined by radiographs
- ▪
- Vertical bone loss (i.e., changes in buccal bone height), determined by radiographs
- ▪
- Implant stability, determined by measuring via implant stability quotient.
- ▪
- Esthetic evaluation, determined by pink esthetic score (PES).
- ▪
- Crestal bone loss (i.e., changes in marginal bone levels), determined by radiographs.
- ▪
- Probing depth, measured by a periodontal probe.
- ▪
- Post-operative complications
- ▪
- Rate of implant failure, determined by the number of implants removed
- Study design: Randomized clinical trial (RCT)
2.2. Information Sources and Search
2.3. Study Selection
2.4. Data Collection and Items
2.5. Risk of Bias in Individual Studies
2.6. Outcome Measure
2.7. Data Synthesis
2.8. Certainty Assessment
3. Results
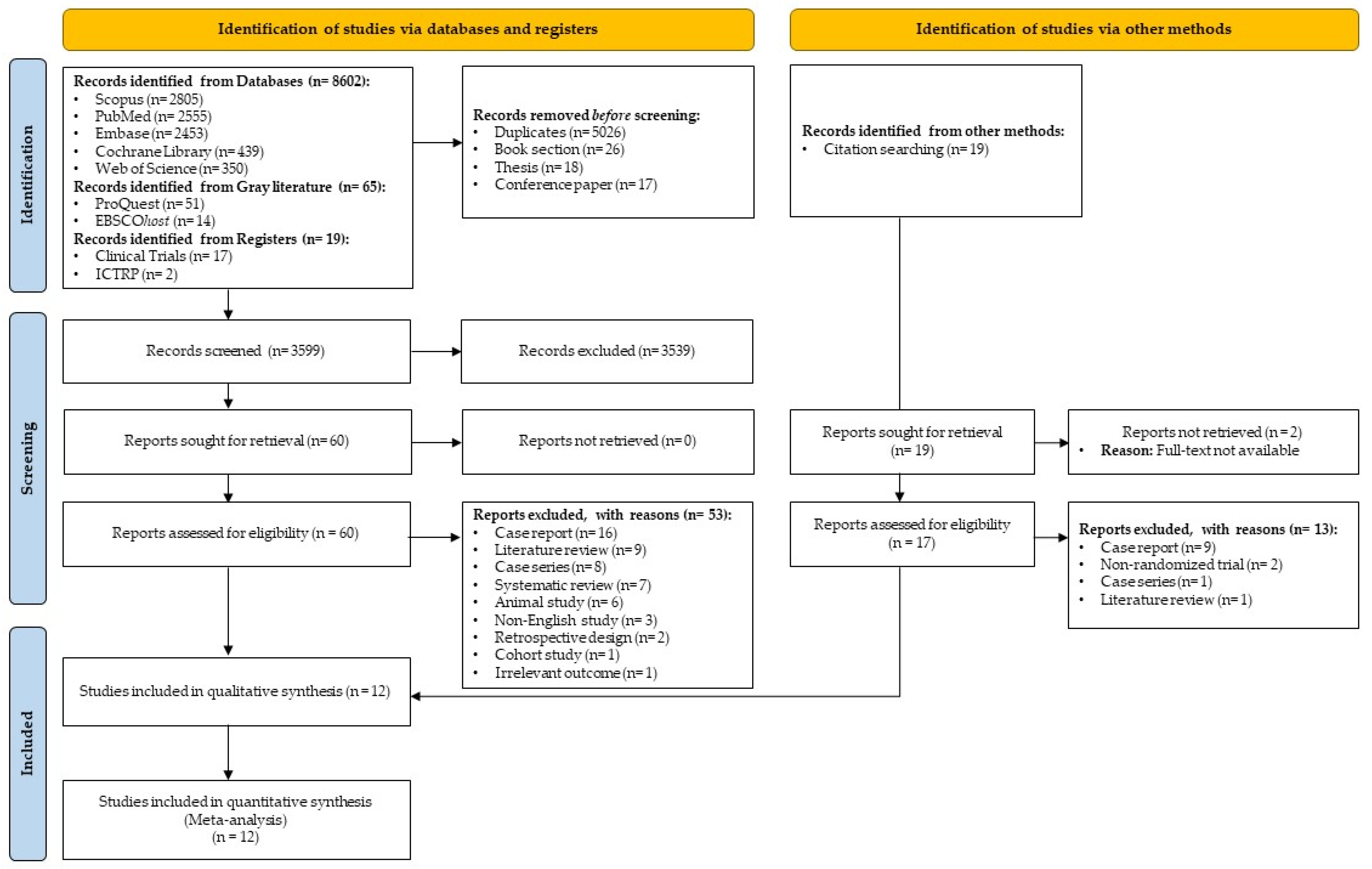
3.1. Study Selection
3.2. Study Characteristics
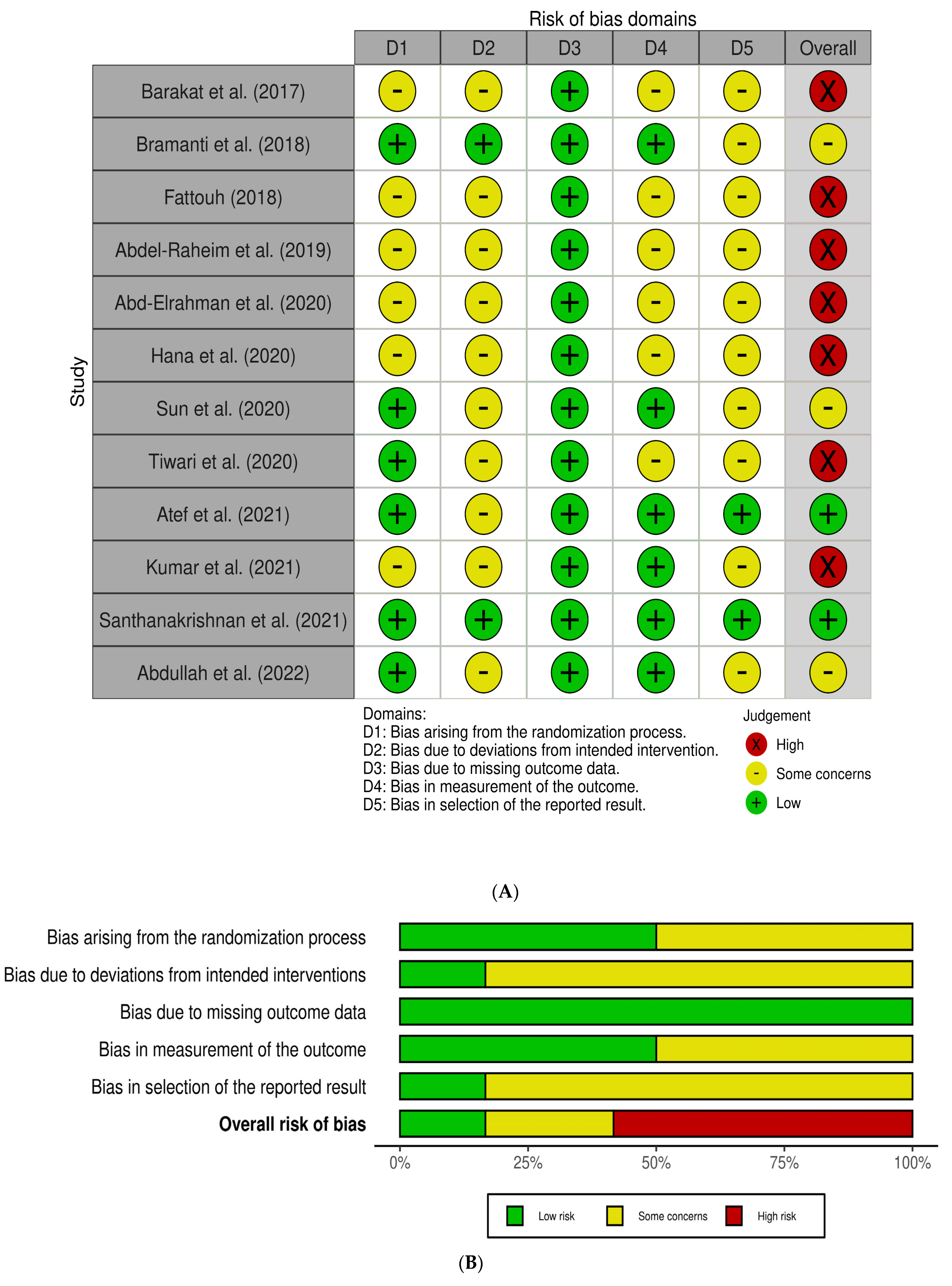
3.3. Risk of Bias within Studies
3.4. Results of Individual Studies
3.5. Results of Syntheses
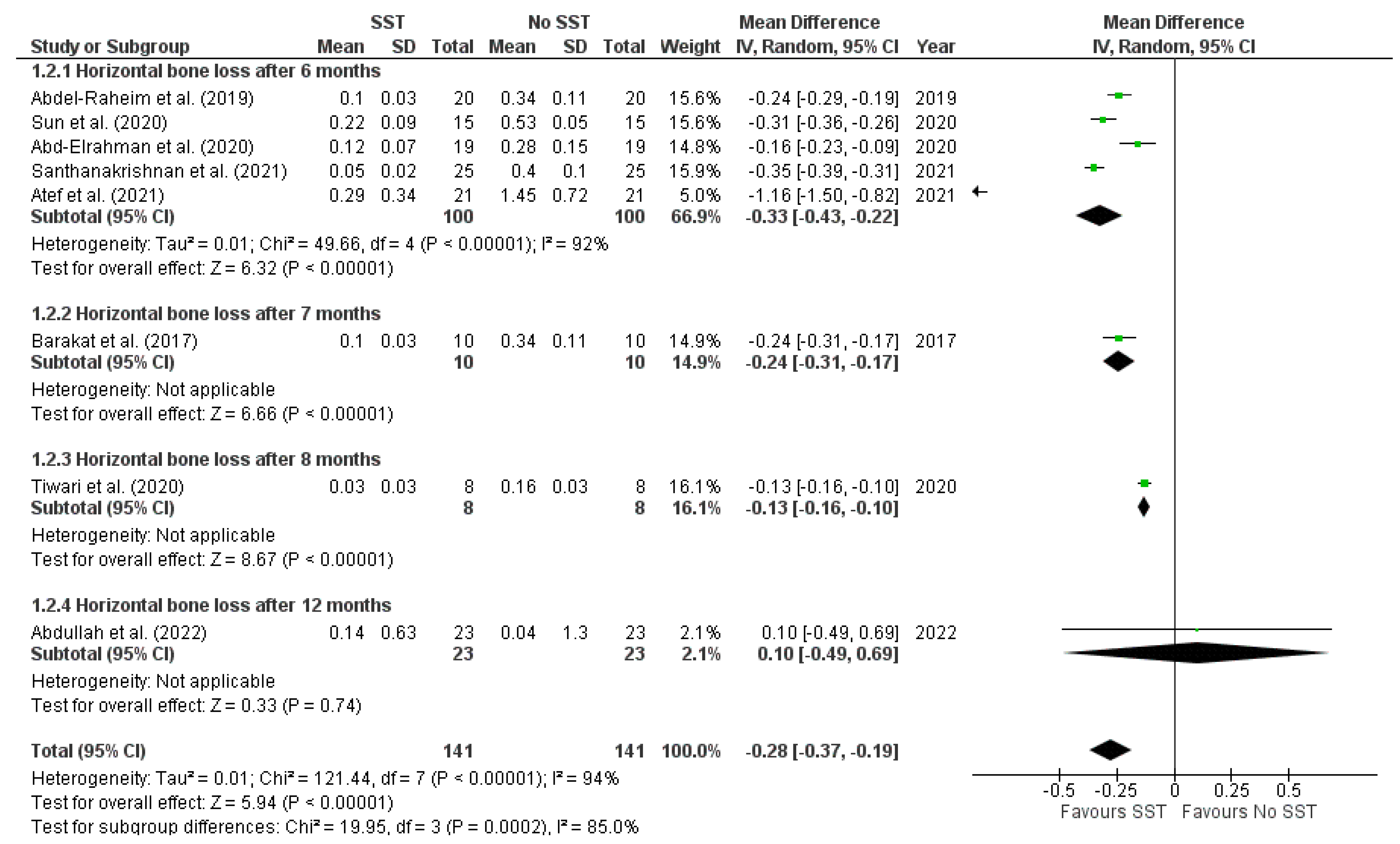
3.5.1. Horizontal Bone Loss (i.e., Changes in Buccal Bone Width)
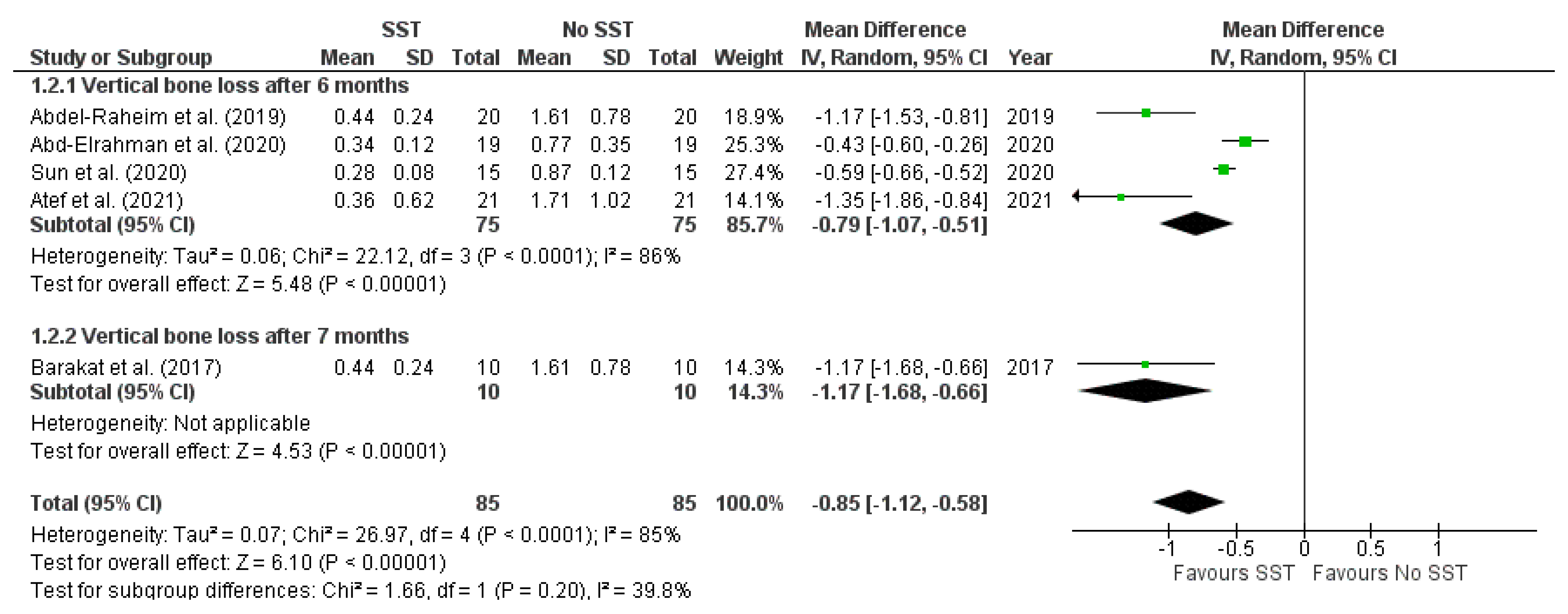
3.5.2. Vertical Bone Loss (i.e., Changes in Buccal Bone Height)
3.5.3. Implant Stability Quotient (ISQ)
3.5.4. Pink Esthetic Score (PES)
3.5.5. Crestal Bone Loss (i.e., Changes in Marginal Bone Levels)
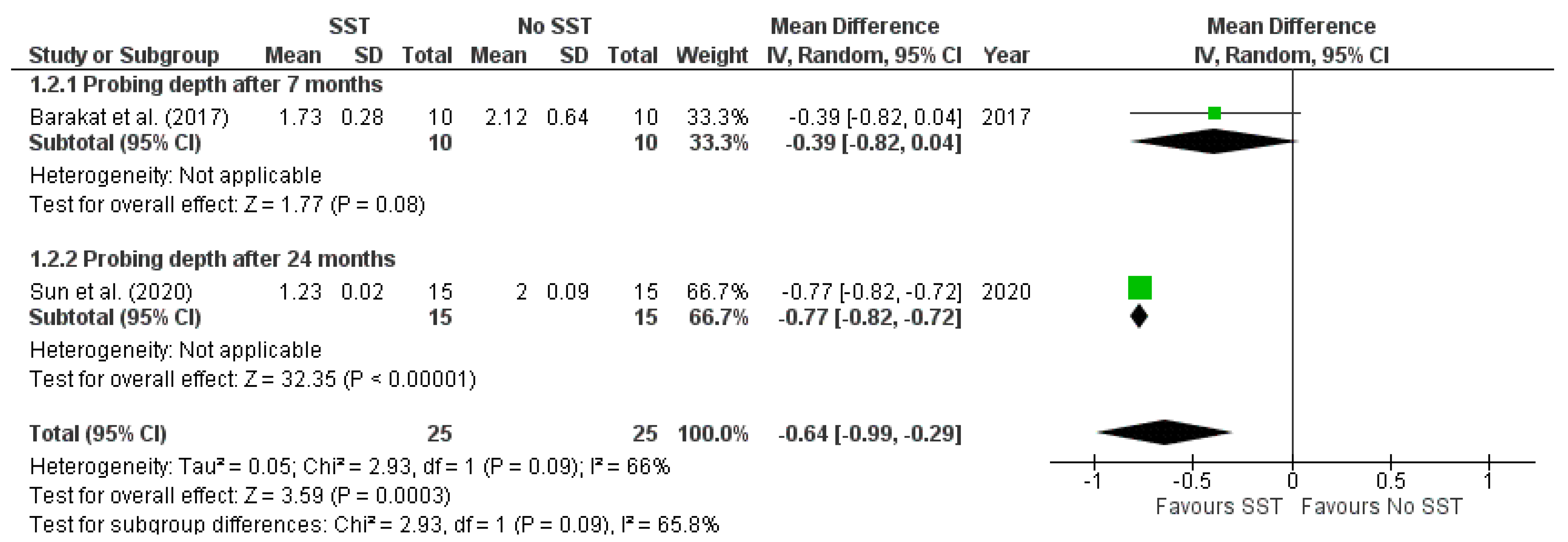
3.5.6. Probing Depth
3.5.7. Complications
3.5.8. Implant Failure
3.6. Sensitivity Analysis
3.7. Certainty of Evidence
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cornelini, R.; Scarano, A.; Covani, U.; Petrone, G.; Piattelli, A. Immediate One-Stage Postextraction Implant: A Human Clinical and Histologic Case Report. Int. J. Oral Maxillofac. Implant. 2000, 15, 432–437. [Google Scholar]
- Scarano, A.; Conte, E.; Mastrangelo, F.; Greco Lucchina, A.; Lorusso, F. Narrow Single Tooth Implants for Congenitally Missing Maxillary Lateral Incisors: A 5-Year Follow-Up. J. Biol. Regul. Homeost. Agents 2019, 33, 69–76. [Google Scholar] [PubMed]
- Scarano, A.; Assenza, B.; Di Cerbo, A.; Candotto, V.; De Oliveira, S.P.; Lorusso, F. Bone Regeneration in Aesthetic Areas Using Titanium Micromesh. Three Case Reports. Oral Implant. 2017, 10, 488–494. [Google Scholar] [CrossRef]
- Buser, D.; Martin, W.; Belser, U.C. Optimizing Esthetics for Implant Restorations in the Anterior Maxilla: Anatomic and Surgical Considerations. Int. J. Oral Maxillofac. Implant. 2004, 19, 43–61. [Google Scholar]
- Chappuis, V.; Araújo, M.G.; Buser, D. Clinical Relevance of Dimensional Bone and Soft Tissue Alterations Post-Extraction in Esthetic Sites. Periodontol. 2000 2017, 73, 73–83. [Google Scholar] [CrossRef]
- Tsigarida, A.; Toscano, J.; de Brito Bezerra, B.; Geminiani, A.; Barmak, A.B.; Caton, J.; Papaspyridakos, P.; Chochlidakis, K. Buccal Bone Thickness of Maxillary Anterior Teeth: A Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2020, 47, 1326–1343. [Google Scholar] [CrossRef]
- Huynh-Ba, G.; Pjetursson, B.E.; Sanz, M.; Cecchinato, D.; Ferrus, J.; Lindhe, J.; Lang, N.P. Analysis of the Socket Bone Wall Dimensions in the Upper Maxilla in Relation to Immediate Implant Placement: Socket Bone Wall Dimensions and Immediate Implant Placement. Clin. Oral Implant. Res. 2010, 21, 37–42. [Google Scholar] [CrossRef]
- Pagni, G.; Pellegrini, G.; Giannobile, W.V.; Rasperini, G. Postextraction Alveolar Ridge Preservation: Biological Basis and Treatments. Int. J. Dent. 2012, 2012, 1–13. [Google Scholar] [CrossRef]
- Al Yafi, F.; Alchawaf, B.; Nelson, K. What Is the Optimum for Alveolar Ridge Preservation? Dent. Clin. N. Am. 2019, 63, 399–418. [Google Scholar] [CrossRef]
- López-Pacheco, A.; Soto-Peñaloza, D.; Gómez, M.; Peñarrocha-Oltra, D.; Alarcón, M.A. Socket Seal Surgery Techniques in the Esthetic Zone: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Clinical Trials. Int. J. Implant. Dent. 2021, 7, 13. [Google Scholar] [CrossRef]
- Lee, C.-T.; Chiu, T.-S.; Chuang, S.-K.; Tarnow, D.; Stoupel, J. Alterations of the Bone Dimension Following Immediate Implant Placement into Extraction Socket: Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2014, 41, 914–926. [Google Scholar] [CrossRef]
- Hürzeler, M.B.; Zuhr, O.; Schupbach, P.; Rebele, S.F.; Emmanouilidis, N.; Fickl, S. The Socket-Shield Technique: A Proof-of-Principle Report: The Socket Shield Technique. J. Clin. Periodontol. 2010, 37, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Reames, R.L.; Nickel, J.S.; Patterson, S.S.; Boone, M.; El-Kafrawy, A.H. Clinical, Radiographic, and Histological Study of Endodontically Treated Retained Roots to Preserve Alveolar Bone. J. Endod. 1975, 1, 367–373. [Google Scholar] [CrossRef]
- O’Neal, R.B.; Gound, T.; Levin, M.P.; Del Rio, C.E. Submergence of Roots for Alveolar Bone Preservation. Oral Surg. Oral Med. Oral Pathol. 1978, 45, 803–810. [Google Scholar] [CrossRef]
- Buser, D.; Warrer, K.; Karring, T. Formation of a Periodontal Ligament Around Titanium Implants. J. Periodontol. 1990, 61, 597–601. [Google Scholar] [CrossRef] [PubMed]
- Plata, R.L.; Kelln, E.E. Intentional Retention of Vital Submerged Roots in Dogs. Oral Surg. Oral Med. Oral Pathol. 1976, 42, 100–108. [Google Scholar] [CrossRef]
- Filippi, A.; Pohl, Y.; Von Arx, T. Decoronation of an Ankylosed Tooth for Preservation of Alveolar Bone Prior to Implant Placement*: Decoronation for Preservation of Alveolar Bone. Dent. Traumatol. 2001, 17, 93–95. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, H.; Du Toit, J.; Salama, M.; Nagy, K.; Dard, M. A Decade of the Socket-Shield Technique: A Step-by-Step Partial Extraction Therapy Protocol. Int. J. Esthet. Dent. 2020, 15, 212–225. [Google Scholar]
- Gluckman, H.; Salama, M.; Du Toit, J. Partial Extraction Therapies (PET) Part 2: Procedures and Technical Aspects. Int. J. Periodontics Restor. Dent. 2017, 37, 377–385. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 1st ed.; Wiley: Hoboken, NJ, USA, 2019; ISBN 978-1-119-53662-8. [Google Scholar]
- Schünemann, H.; Brożek, J.; Guyatt, G.; Oxman, A. Handbook for Grading the Quality of Evidence and the Strength of Recommendations Using the GRADE Approach, (updated October 2013). Available online: https://gdt.gradepro.org/app/handbook/handbook.html (accessed on 10 March 2023).
- Barakat, D.A.; Hassan, R.S.; Eldibany, R.M. Evaluation of the Socket Shield Technique for Immediate Implantation. Alex. Dent. J. 2017, 42, 155–161. [Google Scholar] [CrossRef]
- Bramanti, E.; Norcia, A.; Cicciù, M.; Matacena, G.; Cervino, G.; Troiano, G.; Zhurakivska, K.; Laino, L. Postextraction Dental Implant in the Aesthetic Zone, Socket Shield Technique Versus Conventional Protocol. J. Craniofac. Surg. 2018, 29, 1037–1041. [Google Scholar] [CrossRef]
- Fattouh, H. Socket-Shield Technique versus Guided Bone Regeneration Technique for Ridge Preservation with Immediate Implant Placement in the Esthetic Zone. Egypt. Dent. J. 2018, 64, 2047–2055. [Google Scholar] [CrossRef]
- Abdel-Raheim, A.S.; Al-Fakharany, A.-M.H. Evaluation of Immediate Immediate Implant with Socket Shield Technique in Aesthetic Zone. Al-Azhar J. Dent. Sci. 2019, 22, 129. [Google Scholar]
- Abd-Elrahman, A.; Shaheen, M.; Askar, N.; Atef, M. Socket Shield Technique vs Conventional Immediate Implant Placement with Immediate Temporization. Randomized Clinical Trial. Clin. Implant. Dent. Relat. Res. 2020, 22, 602–611. [Google Scholar] [CrossRef]
- Hana, S.A.; Omar, O.A. Socket Shield Technique for Dental Implants in the Esthetic Zone, Clinical and Radiographical Evaluation. J. Duhok Univ. 2020, 23, 69–80. [Google Scholar] [CrossRef]
- Sun, C.; Zhao, J.; Liu, Z.; Tan, L.; Huang, Y.; Zhao, L.; Tao, H. Comparing Conventional Flap-Less Immediate Implantation and Socket-Shield Technique for Esthetic and Clinical Outcomes: A Randomized Clinical Study. Clin. Oral Implant. Res. 2020, 31, 181–191. [Google Scholar] [CrossRef]
- Tiwari, S.; Bedi, R.S.; Wadhwani, P.; Aurora, J.K.; Chauhan, H. Comparison of Immediate Implant Placement Following Extraction with and without Socket-Shield Technique in Esthetic Region. J. Maxillofac. Oral Surg. 2020, 19, 552–560. [Google Scholar] [CrossRef]
- Atef, M.; El Barbary, A.; Dahrous, M.S.E.-D.; Zahran, A.F. Comparison of the Soft and Hard Peri-Implant Tissue Dimensional Changes around Single Immediate Implants in the Esthetic Zone with Socket Shield Technique versus Using Xenograft: A Randomized Controlled Clinical Trial. Clin. Implant. Dent. Relat. Res. 2021, 23, 456–465. [Google Scholar] [CrossRef]
- Kumar, P.R.; Vikram, J.; Kher, U.; Tunkiwala, A.; Sawhney, H. Pink Esthetic and Radiological Scores around Immediate Implants Placed in the Esthetic Zone—Socket-Shield Technique versus Immediate Conventional Technique: A Pilot Study. J. Indian Soc. Periodontol. 2021, 25, 510–517. [Google Scholar] [CrossRef]
- Santhanakrishnan, M.; Subramanian, V.; Ramesh, N.; Kamaleeshwari, R. Radiographic and Esthetic Evaluation Following Immediate Implant Placement with or without Socket Shield and Delayed Implant Placement Following Socket Preservation in the Maxillary Esthetic Region—A Randomized Controlled Clinical Trial. Clin. Cosmet. Investig. Dent. 2021, 13, 479–494. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, A.H.; Abdel Gaber, H.K.; Adel-Khattab, D. Evaluation of Soft Tissue and Labial Plate of Bone Stability with Immediate Implant in Direct Contact versus Gap with Socket Shield: A Randomized Clinical Trial with 1 Year Follow-up. Clin. Implant. Dent. Rel. Res. 2022, 24, 548–558. [Google Scholar] [CrossRef] [PubMed]
- Mitsias, M.E.; Siormpas, K.D.; Kotsakis, G.A.; Ganz, S.D.; Mangano, C.; Iezzi, G. The Root Membrane Technique: Human Histologic Evidence after Five Years of Function. BioMed Res. Int. 2017, 2017, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fürhauser, R.; Florescu, D.; Benesch, T.; Haas, R.; Mailath, G.; Watzek, G. Evaluation of Soft Tissue around Single-Tooth Implant Crowns: The Pink Esthetic Score: Esthetic Score. Clin. Oral Implant. Res. 2005, 16, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Siormpas, K.D.; Mitsias, M.E.; Kotsakis, G.A.; Tawil, I.; Pikos, M.A.; Mangano, F.G. The Root Membrane Technique: A Retrospective Clinical Study With Up to 10 Years of Follow-Up. Implant Dent. 2018, 27, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Bäumer, D.; Zuhr, O.; Rebele, S.; Hürzeler, M. Socket Shield Technique for Immediate Implant Placement—Clinical, Radiographic and Volumetric Data after 5 Years. Clin. Oral Implant. Res. 2017, 28, 1450–1458. [Google Scholar] [CrossRef]
- Siormpas, K.; Mitsias, M.; Kontsiotou-Siormpa, E.; Garber, D.; Kotsakis, G. Immediate Implant Placement in the Esthetic Zone Utilizing the “Root-Membrane” Technique: Clinical Results up to 5 Years Postloading. Int. J. Oral Maxillofac. Implant. 2014, 29, 1397–1405. [Google Scholar] [CrossRef]
- Gluckman, H.; Salama, M.; Du Toit, J. A Retrospective Evaluation of 128 Socket-Shield Cases in the Esthetic Zone and Posterior Sites: Partial Extraction Therapy with up to 4 Years Follow-Up. Clin. Implant. Dent. Relat. Res. 2018, 20, 122–129. [Google Scholar] [CrossRef]
- Kher, U. Surgical Technique for Socket Shield Procedure. In Partial Extraction Therapy in Implant Dentistry; Kher, U., Tunkiwala, A., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 17–42. ISBN 978-3-030-33609-7. [Google Scholar]
- Cochran, D.L.; Hermann, J.S.; Schenk, R.K.; Higginbottom, F.L.; Buser, D. Biologic Width around Titanium Implants. A Histometric Analysis of the Implanto-Gingival Junction around Unloaded and Loaded Nonsubmerged Implants in the Canine Mandible. J. Periodontol. 1997, 68, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Abadzhiev, M.; Nenkov, P.; Velcheva, P. Conventional Immediate Implant Placement and Immediate Placement with Socket-Shield Technique—Which Is Better. Int. J. Clin. Med. Res. 2014, 1, 176–180. [Google Scholar]
- Buser, D.; Weber, H.P.; Donath, K.; Fiorellini, J.P.; Paquette, D.W.; Williams, R.C. Soft Tissue Reactions to Non-Submerged Unloaded Titanium Implants in Beagle Dogs. J. Periodontol. 1992, 63, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, H.; Salama, M.; Du Toit, J. Partial Extraction Therapies (PET) Part 1: Maintaining Alveolar Ridge Contour at Pontic and Immediate Implant Sites. Int. J. Periodontics Restor. Dent. 2016, 36, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Tan, Z.; Kang, J.; Liu, W.; Wang, H. The Effect of the Heights and Thicknesses of the Remaining Root Segments on Buccal Bone Resorption in the Socket-Shield Technique: An Experimental Study in Dogs. Clin. Implant. Dent. Relat. Res. 2018, 20, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.; Akl, E.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. MetaArXiv 2020. Available online: www.prisma-statement.org (accessed on 10 March 2023).











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors (Year) Country | Design (Location) | Age (Range) Mean ± SD | Sample Size (M/F Ratio) | Number Evaluated (Participants/Implants) | Extracted Teeth | Reason for Extraction | Population | Socket Shield Procedures | Control Procedures | Implant | Radiographic Assessment | Funding Source | Conflicts of Interest | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Medical Status | Smoking Habit | Periodontal Phenotype | System | Settings | Prosthetic | ||||||||||||
| Barakat et al. (2017) Egypt [23] | RCT-Pa (University Clinic) | (20:50) 35 years | 20 (NR) | Tot: 20/20 SST: 10/10 Con: 10/10 | Maxillary incisors and canines | NR | NR | NR | <1.5 mm Labial bone plate thickness | Tooth decoronated: 1 mm above gingival level Root sectioned: a Buccal shield: e Buccal gap: No graft | Tooth extraction: g Flap: h GBR: No graft | Superline implant, Dentium, Gangnam-gu, Seoul, Republic of Korea. | D: 3.3 and 3.8 mm L: 12 and 14 mm T: NR | Delayed implant loading at four months | CBCT | NR | NR |
| Bramanti et al. (2018) Italy [24] | RCT-Pa (University Clinic) | NR | 40 (NR) | Tot: 40/40 SST: 20/20 Con: 20/20 | Maxillary/Mandibular incisors and canines | Fractures, destructive caries, internal resorption, and failed root canal treatment | NR | NR | NR | Tooth decoronated: to gingival level Root sectioned: c Buccal shield: e Buccal gap: Bone allograft (j) | Tooth extraction: g Flap: h GPR: Bone allograft (j) | NR | D: 4.5 mm L: NR T: <35 Ncm | Immediate provisional restoration | Periapical radiographs (parallel technique) | Funded (p) | None |
| Fattouh (2018) Egypt [25] | RCT-Pa (University Clinic) | NR | 20 (8 M:12 F) | Tot: 20/20 SST: 10/10 Con: 10/10 | Maxillary incisors and canines | NR | NR | Non-smokers | NR | Tooth decoronated: to gingival level Root sectioned: a Buccal shield: f Buccal gap: No graft | Tooth extraction: g Flap: i GPR: Xenograft and collagen membrane (k) | NR | D: 4.1 mm L: 13 mm T: 30 Ncm | Immediate provisional restoration | Periapical radiographs (parallel technique) | NR | NR |
| Abdel-Raheim et al. (2019) Egypt [26] | RCT-SM (University Clinic) | (20:35) 29.8 ± 5.3 years | 10 (4 M:6 F) | Tot: 20/20 SST: 10/10 Con: 10/10 | Maxillary incisors and canines | NR | NR | NR | <1.5 mm Labial bone plate thickness | Tooth decoronated: to gingival level Root sectioned: b Buccal shield: e Buccal gap: No graft | Tooth extraction: g Flap: h GBR: No graft | NR | D: NR L: NR T: NR | Immediate provisional restoration | CBCT | NR | NR |
| Abd-Elrahman et al. (2020) Egypt [27] | RCT-Pa (University Clinic) | (21:39) 30.9 ± 5.5 years | 25 (11 M:14 F) | Tot: 25/40 SST: 16/20 Con: 18/20 | Maxillary incisors and canines | NR | NR | NR | Both (thick and thin) periodontal phenotype | Tooth decoronated: 1mm above gingival level Root sectioned: a Buccal shield: d Buccal gap: No graft | Tooth extraction: g Flap: h GBR: No graft | Dual implant, Titan Industries EG, Cairo, Egypt | D: 3.3 and 3.7 mm L: 14 and 16 mm T: NR | Immediate provisional restoration | CBCT | NR | None |
| Hana et al. (2020) Iraq [28] | RCT-Pa (University Clinic) | (28:65) 51 years | 40 (24 M:16 F) | Tot: 40/40 SST: 20/20 Con: 20/20 | Maxillary/Mandibular incisors and canines | NR | ASA I and ASA II | Non-smokers | NR | Tooth decoronated: 1mm above gingival level Root sectioned: a Buccal shield: d Buccal gap: No graft | Tooth extraction: g Flap: h GBR: No graft | EUROTeknika implant, Sallanches, France | D: 3.5 to 5 (4.1mm) L: 11 to 14 (2.3 mm) T: 49 Ncm | Immediate provisional restoration | CBCT | NR | NR |
| Sun et al. (2020) China [29] | RCT-Pa (University Clinic) | NR | 30 (23 M:7 F) | Tot: 30/30 SST: 15/15 Con: 15/15 | Maxillary/Mandibular incisors and canines | Trauma, Decay/pulp lesions | NR | Smokers (<10 cigarettes/day) | Thick gingival biotype with healthy marginal gingiva | Tooth decoronated: 1mm above gingival level Root sectioned: NR Buccal shield: e Buccal gap: Xenograft (if gap >1 mm) (m) | Tooth extraction: g Flap: h GPR: Xenograft (if gap >1 mm) (l) | Nobel Replace®cc, Nobel Biocare, Gothenburg, Sweden. | D: 3.5, 4.0 L: NR T: 35 Ncm | Immediate provisional restoration | CBCT | NR | None |
| Tiwari et al. (2020) India [30] | RCT-Pa (University Clinic) | (18:30) years | 16 (NR) | Tot: 16/16 SST: 8/8 Con: 8/8 | Maxillary incisors and canines | NR | ASA I and ASA II | NR | Intact buccal cortical plate with <2 mm thickness | Tooth decoronated: below gingival level Root sectioned: a Buccal shield: e Buccal gap: Suture + Periodontal pack | Tooth extraction: g Flap: i GBR: No graft | NR | D: NR L: NR T: 40 Ncm | Delayed implant loading at four months | CBCT | None | None |
| Atef et al. (2021) Egypt [31] | RCT-Pa (University Clinic) | 36 ± 5.55 years | 42 (11 M:31 F) | Tot: 42/42 SST: 21/21 Con: 21/21 | Maxillary premolars and anteriors | NR | NR | Non-smokers | Thick gingival biotype | Tooth decoronated: to gingival level Root sectioned: a Buccal shield: d Buccal gap: Collagen plug | Tooth extraction: g Flap: i GPR: Xenograft (m) | IS II, Neobiotech Co., Seoul, Republic of Korea | D: NR L: NR T: NR | Delayed implant loading at four months | CBCT | None | None |
| Kumar et al. (2021) India [32] | RCT-Pa (University Clinic) | 37 years | 20 (14 M:6 F) | Tot: 20/30 SST: 10/15 Con: 10/15 | Maxillary incisors and canines | NR | NR | NR | NR | Tooth decoronated: to gingival level Root sectioned: a Buccal shield: e Buccal gap: No graft | Tooth extraction: g Flap: h GBR: No graft | Megagen Implant Co. Ltd., Seoul, Republic of Korea | D: 3.5-mm L: NR T: NR | Delayed implant loading at four months | Periapical radiographs (parallel technique) | Funded (q,r) | None |
| Santhanakrishnan et al. (2021) India [33] | RCT-Pa (University Clinic) | (18:50) 30.6 ± 6.0 years | 50 (23 M:27 F) | Tot: 50/50 SST: 25/25 Con: 25/25 | Maxillary incisors and canines | NR | NR | NR | Intact facial bone with <2 mm thickness | Tooth decoronated: 1mm above gingival level Root sectioned: a Buccal shield: d Buccal gap: No graft | Tooth extraction: g Flap: h GPR: Xenograft and autogenous bone (n) | DIO implant system, Busan, Republic of Korea | D: 3.3 and 3.8 mm L: 13 and 15 mm T: 40 Ncm | Immediate provisional restoration | CBCT | None | None |
| Abdullah et al. (2022) Egypt [34] | RCT-Pa (University Clinic) | 29.4 years | 46 (20 M:26 F) | Tot: 46/46 SST: 23/23 Con: 23/23 | Maxillary premolars and anteriors | Failed root canal treatment | NR | NR | Both (thick and thin) periodontal phenotype | Tooth decoronated: 1 mm above gingival level Root sectioned: a Buccal shield: d Buccal gap: No graft | Tooth extraction: g Flap: h GPR: Xenograft (o) | IS II, Neobiotech Co., Seoul, Republic of Korea | NR | Immediate provisional restoration | CBCT | None | None |
Explanations:
|
| ||||||||||||||||
| Outcomes | Nº of Participants/Implants (Studies) | Certainty of the Evidence (GRADE) | Relative Effect (95% CI) | Anticipated Absolute Effects | |
|---|---|---|---|---|---|
| Risk with [No SST] | Risk Difference with [SST] | ||||
| Horizontal bone loss (i.e., changes in buccal bone width) assessed with: mm follow-up range: four months to twelve months | 268/284 (8 RCTs) | ⨁◯◯◯ Very low | - | The mean horizontal bone loss (i.e., changes in buccal bone width) was 0 mm | MD 0.28 mm fewer (0.37 fewer to 0.19 fewer) |
| Vertical bone loss (i.e., changes in buccal bone height) assessed with: mm follow-up range: six months to seven months | 156/166 (6 RCTs) | ⨁◯◯◯ Very low | - | The mean vertical bone loss (i.e., changes in buccal bone height) was 0 mm | MD 0.85 mm fewer (1.12 fewer to 0.58 fewer) |
| Implant Stability assessed with: ISQ measurements follow-up range: four months to six months | 140/156 (5 RCTs) | ⨁◯◯◯ Very low | - | The mean implant Stability Quotient (ISQ) was 0 | MD 3.46 more (1.22 more to 5.69 more) |
| Esthetic evaluation assessed with: PES measurements follow-up range: four months to three years | 280/296 (8 RCTs) | ⨁◯◯◯ Very low | - | The mean pink Esthetic Score (PES) was 0 | MD 1.6 more (0.9 more to 2.3 more) |
| Crestal bone loss (i.e., changes in marginal bone levels) assessed with: mm follow-up range: three months to three years | 106/106 (3 RCTs) | ⨁◯◯◯ Very low | - | The mean crestal bone loss (i.e., changes in marginal bone levels) was 0 mm | MD 0.35 mm fewer (0.56 fewer to 0.13 fewer) |
| Probing depth assessed with: mm follow-up range: four months to two years | 50/50 (2 RCTs) | ⨁◯◯◯ Very low | - | The mean probing depth was 0 mm | MD 0.64 mm fewer (0.99 fewer to 0.29 fewer) |
| * The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference | |||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scarano, A.; Di Carmine, M.; Al-Hamed, F.S.; Khater, A.G.A.; Gehrke, S.A.; Tari, S.R.; Leo, L.; Inchingolo, F.; Lorusso, F. Socket Shield Technique to Improve the Outcomes of Immediate Implant: A Systematic Review and Meta-Analysis. Prosthesis 2023, 5, 509-526. https://doi.org/10.3390/prosthesis5020035
Scarano A, Di Carmine M, Al-Hamed FS, Khater AGA, Gehrke SA, Tari SR, Leo L, Inchingolo F, Lorusso F. Socket Shield Technique to Improve the Outcomes of Immediate Implant: A Systematic Review and Meta-Analysis. Prosthesis. 2023; 5(2):509-526. https://doi.org/10.3390/prosthesis5020035
Chicago/Turabian StyleScarano, Antonio, Mariastella Di Carmine, Faez Saleh Al-Hamed, Ahmad G. A. Khater, Sergio Alexandre Gehrke, Sergio Rexhep Tari, Lucia Leo, Francesco Inchingolo, and Felice Lorusso. 2023. "Socket Shield Technique to Improve the Outcomes of Immediate Implant: A Systematic Review and Meta-Analysis" Prosthesis 5, no. 2: 509-526. https://doi.org/10.3390/prosthesis5020035
APA StyleScarano, A., Di Carmine, M., Al-Hamed, F. S., Khater, A. G. A., Gehrke, S. A., Tari, S. R., Leo, L., Inchingolo, F., & Lorusso, F. (2023). Socket Shield Technique to Improve the Outcomes of Immediate Implant: A Systematic Review and Meta-Analysis. Prosthesis, 5(2), 509-526. https://doi.org/10.3390/prosthesis5020035