

The Effects of Interbody Device Design and Placement on Lumbar Lordosis and Disc Height in Transforaminal Lumbar Interbody Fusion
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
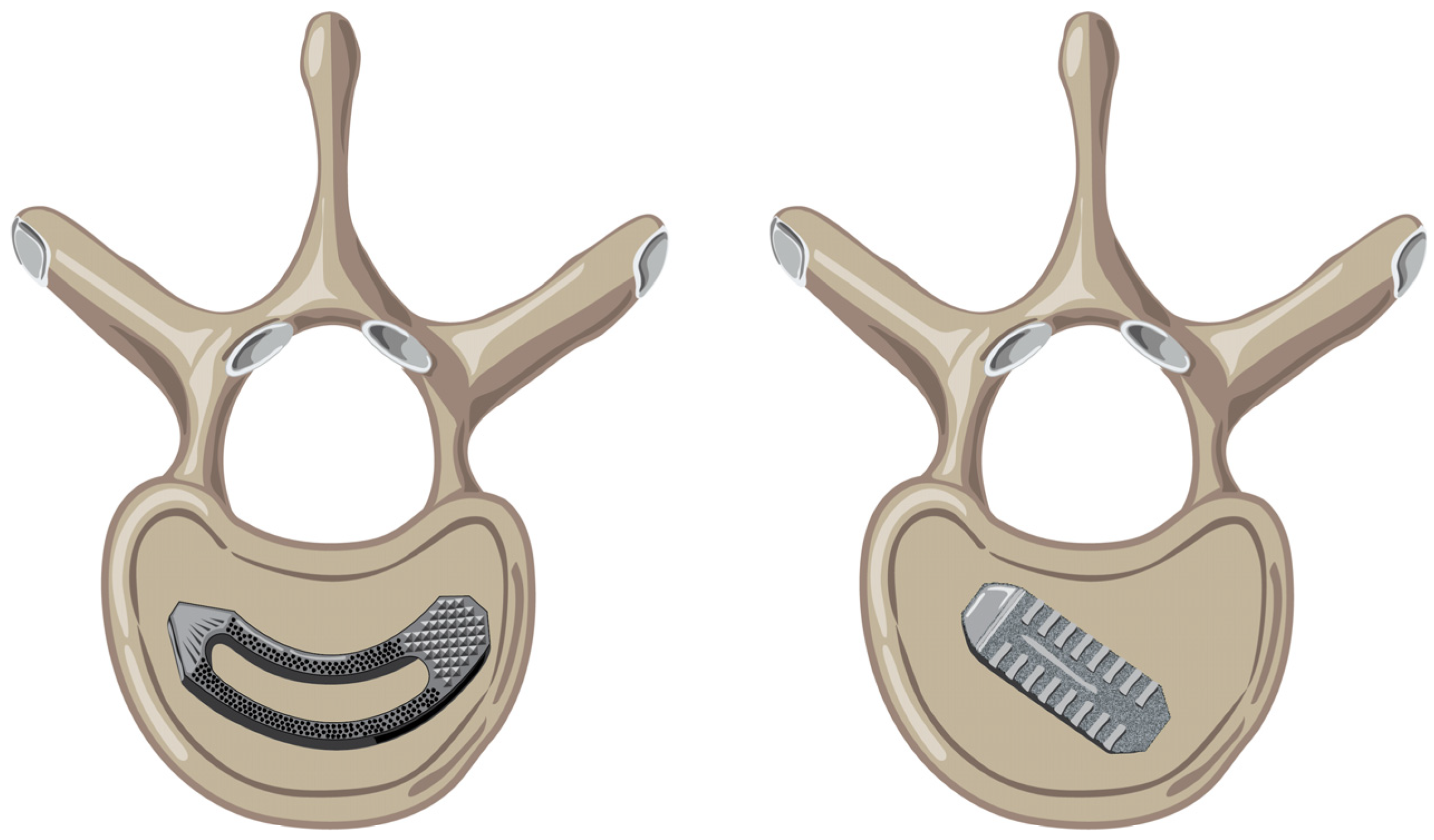
2.1. Surgical Technique
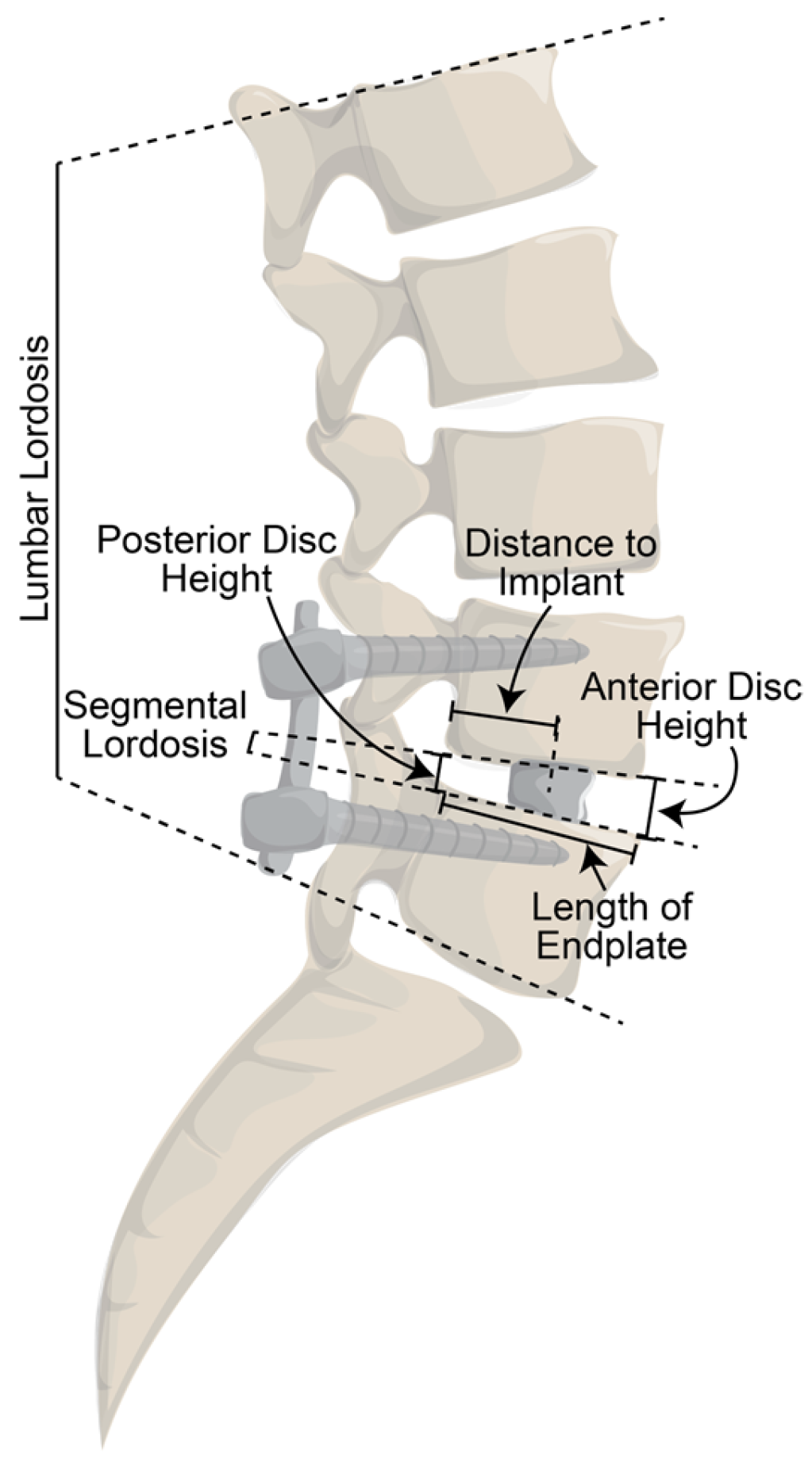
2.2. Radiographic Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mobbs, R.J.; Phan, K.; Malham, G.; Seex, K.; Rao, P.J. Lumbar interbody fusion: Techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J. Spine Surg. 2015, 1, 2–18. [Google Scholar] [CrossRef]
- Cole, C.D.; McCall, T.D.; Schmidt, M.H.; Dailey, A.T. Comparison of low back fusion techniques: Transforaminal lumbar interbody fusion (TLIF) or posterior lumbar interbody fusion (PLIF) approaches. Curr. Rev. Musculoskelet. Med. 2009, 2, 118–126. [Google Scholar] [CrossRef] [Green Version]
- Schwender, J.D.; Holly, L.T.; Rouben, D.P.; Foley, K.T. Minimally invasive transforaminal lumbar interbody fusion (TLIF): Technical feasibility and initial results. Clin. Spine Surg. 2005, 18, S1–S6. [Google Scholar] [CrossRef] [Green Version]
- Lin, G.X.; Akbary, K.; Kotheeranurak, V.; Quillo-Olvera, J.; Jo, H.J.; Yang, X.W.; Mahatthanatrakul, A.; Kim, J.S. Clinical and Radiologic Outcomes of Direct Versus Indirect Decompression with Lumbar Interbody Fusion: A Matched-Pair Comparison Analysis. World Neurosurg. 2018, 119, e898–e909. [Google Scholar] [CrossRef]
- Yoshihara, H. Indirect decompression in spinal surgery. J. Clin. Neurosci. 2017, 44, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Schwab, F.J.; Blondel, B.; Bess, S.; Hostin, R.; Shaffrey, C.I.; Smith, J.S.; Boachie-Adjei, O.; Burton, D.C.; Akbarnia, B.A.; International Spine Study Group; et al. Radiographical spinopelvic parameters and disability in the setting of adult spinal deformity: A prospective multicenter analysis. Spine 2013, 38, E803–E812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Protopsaltis, T.; Schwab, F.; Bronsard, N.; Smith, J.S.; Klineberg, E.; Mundis, G.; Ryan, D.J.; Hostin, R.; Hart, R.; Burton, D.; et al. The T1 pelvic angle, a novel radiographic measure of global sagittal deformity, accounts for both spinal inclination and pelvic tilt and correlates with health-related quality of life. JBJS 2014, 96, 1631–1640. [Google Scholar] [CrossRef] [PubMed]
- Glassman, S.D.; Berven, S.; Bridwell, K.; Horton, W.; Dimar, J.R. Correlation of radiographic parameters and clinical symptoms in adult scoliosis. Spine 2005, 30, 682–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Duan, P.; Mummaneni, P.V.; Xie, R.; Li, B.; Dong, Y.; Berven, S.; Chou, D. Does transforaminal lumbar interbody fusion induce lordosis or kyphosis? Radiographic evaluation with a minimum 2-year follow-up. J. Neurosurg. Spine 2021, 35, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Yue, W.M.; Yeo, W.; Soeharno, H.; Tan, S.B. Clinical and radiological outcomes of open versus minimally invasive transforaminal lumbar interbody fusion. Eur. Spine J. 2012, 21, 2265–2270. [Google Scholar] [CrossRef] [Green Version]
- Burneikiene, S.; Roeca, C.; Nelson, L.; Mason, A.; Villavicencio, A. Minimally invasive versus open transforaminal lumbar interbody fusion. Surg. Neurol. Int. 2010, 1, 12. [Google Scholar] [CrossRef] [Green Version]
- Peng, C.W.B.; Yue, W.M.; Poh, S.Y.; Yeo, W.; Tan, S.B. Clinical and radiological outcomes of minimally invasive versus open transforaminal lumbar interbody fusion. Spine 2009, 34, 1385–1389. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.S.; Kim, J.S.; Hur, J.W.; Seong, J.H. Minimally invasive transforaminal lumbar interbody fusion using banana-shaped and straight cages: Radiological and clinical results from a prospective randomized clinical trial. Clin. Neurosurg. 2018, 82, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Tassemeier, T.; Haversath, M.; Jäger, M. Transforaminal lumbar interbody fusion with expandable cages: Radiological and clinical results of banana-shaped and straight implants. J. Craniovertebral Junction Spine 2018, 9, 196. [Google Scholar] [CrossRef]
- Truckenmueller, P.; Czabanka, M.; Bayerl, S.H.; Mertens, R.; Vajkoczy, P. Oblique insertion of a straight cage during single level TLIF procedure proves to be non-inferior in terms of restoring segmental lordosis. Brain Spine 2021, 1, 100302. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.L.; Mendenhall, S.K.; Shau, D.N.; Zuckerman, S.L.; Godil, S.S.; Cheng, J.S.; McGirt, M.J. Minimally Invasive versus Open Transforaminal Lumbar Interbody Fusion for Degenerative Spondylolisthesis: Comparative Effectiveness and Cost-Utility Analysis. World Neurosurg. 2014, 82, 230–238. [Google Scholar] [CrossRef]
- Karikari, I.O.; Isaacs, R.E. Minimally invasive transforaminal lumbar interbody fusion: A review of techniques and outcomes. Spine 2010, 35, S294–S301. [Google Scholar] [CrossRef]
- Adogwa, O.; Parker, S.L.; Bydon, A.; Cheng, J.; McGirt, M.J. Comparative effectiveness of minimally invasive versus open transforaminal lumbar interbody fusion: 2-year assessment of narcotic use, return to work, disability, and quality of life. J. Spinal Disord. Tech. 2011, 24, 479–484. [Google Scholar] [CrossRef]
- Jin-tao, Q.; Yu, T.; Mei, W.; Xu-dong, T.; Tian-jian, Z.; Guo-hua, S.; Lei, C.; Yue, H.; Zi-tian, W.; Yue, Z. Comparison of MIS vs. open PLIF/TLIF with regard to clinical improvement, fusion rate, and incidence of major complication: A meta-analysis. Eur. Spine J. 2015, 24, 1058–1065. [Google Scholar] [CrossRef]
- Goldstein, C.L.; Phillips, F.M.; Rampersaud, Y.R. Comparative Effectiveness and Economic Evaluations of Open Versus Minimally Invasive Posterior or Transforaminal Lumbar Interbody Fusion. Spine 2016, 41, s74–s89. [Google Scholar] [CrossRef]
- Parker, S.L.; Adogwa, O.; Paul, A.R.; Anderson, W.N.; Aaronson, O.; Cheng, J.S.; McGirt, M.J. Utility of minimum clinically important difference in assessing pain, disability, and health state after transforaminal lumbar interbody fusion for degenerative lumbar spondylolisthesis: Clinical article. J. Neurosurg. Spine 2011, 14, 598–604. [Google Scholar] [CrossRef]
- Lee, K.H.; Yeo, W.; Soeharno, H.; Yue, W.M. Learning Curve of a Complex Surgical Technique: Minimally Invasive Transforaminal Lumbar Interbody Fusion (MIS TLIF). J. Spinal Disord. Tech. 2014, 27, E234–E240. [Google Scholar] [CrossRef] [PubMed]
- Alanay, A.; Pekmezci, M.; Karaeminogullari, O.; Acaroglu, E.; Yazici, M.; Cil, A.; Pijnenburg, B.; Genç, Y.; Oner, F.C. Radiographic measurement of the sagittal plane deformity in patients with osteoporotic spinal fractures evaluation of intrinsic error. Eur. Spine J. 2007, 16, 2126–2132. [Google Scholar] [CrossRef] [Green Version]
- Carlson, B.B.; Saville, P.; Dowdell, J.; Goto, R.; Vaishnav, A.; Gang, C.H.; McAnany, S.; Albert, T.J.; Qureshi, S. Restoration of lumbar lordosis after minimally invasive transforaminal lumbar interbody fusion: A systematic review. Spine J. 2019, 19, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Chen, J.; Chen, J.; Wu, Y.; Chen, X.; Liu, Y.; Chu, Z.; Sheng, L.; Qin, R.; Chen, M. Three-year postoperative outcomes between MIS and conventional TLIF in1-segment lumbar disc herniation. Minim. Invasive Ther. Allied Technol. 2017, 26, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Wang, L.; Zhang, H.; Gu, X.; Gu, G.; He, S. Radiographic Analysis of One-level Minimally Invasive Transforaminal Lumbar Interbody Fusion (MI-TLIF) With Unilateral Pedicle Screw Fixation for Lumbar Degenerative Diseases. J. Spinal Disord. Tech. 2016, 29, E1–E8. [Google Scholar] [CrossRef]
- Isaacs, R.E.; Sembrano, J.N.; Tohmeh, A.G. Two-Year Comparative Outcomes of MIS Lateral and MIS Transforaminal Interbody Fusion in the Treatment of Degenerative Spondylolisthesis. Spine 2016, 41, s133–s144. [Google Scholar] [CrossRef]
- Polly, D.W., Jr.; Kilkelly, F.X.; McHale, K.A.; Asplund, L.M.; Mulligan, M.; Chang, A.S. Measurement of lumbar lordosis: Evaluation of intraobserver, interobserver, and technique variability. Spine 1996, 21, 1530–1535. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group | p-Value | |||||
|---|---|---|---|---|---|---|
| MB (n = 23) | MC (n = 34) | OB (n = 30) | OC (n = 44) | |||
| Age (SD) | 48.5 (12.1) | 51.0 (11.2) | 64.2 (10.9) | 65.3 (9.5) | p < 0.001 | |
| # Female (%) | 10 (43%) | 21 (61%) | 9 (30%) | 20 (45%) | 0.087 | |
| BMI (SD) | 29.4 (4.5) | 29.8 (5.3) | 30.0 (6.1) | 30.4 (6.5) | 0.900 | |
| Active Smokers (%) | 4 (17%) | 5 (15%) | 4 (13%) | 7 (16%) | 0.993 | |
| Instrumented Level (%) | L1-L2 | 0 | 0 | 0 | 1 (2%) | 0.638 |
| L2-L3 | 0 | 0 | 0 | 1 (2%) | ||
| L3-L4 | 0 | 3 (9%) | 3 (10%) | 4 (9%) | ||
| L4-L5 | 11 (49%) | 14 (41%) | 18 (60%) | 22 (50%) | ||
| L5-S1 | 12 (51%) | 17 (50%) | 9 (30%) | 16 (36%) | ||
| Change Compared to Preoperative | |||
|---|---|---|---|
| Measurement | Group | Initial (SD) | Final (SD) |
| Lumbar Lordosis (°) | MB | −4.0 (5.8) | −0.2 (4.2) |
| MC | −3.7 (10.6) | 2.9 (9.8) | |
| OB | −0.3 (7.0) | 3.5 (5.3) | |
| OC | −0.9 (13.2) | 1.9 (10.8) | |
| Segmental Lordosis (°) | MB | 3.0 (6.5) | 2.0 (5.6) |
| MC | 2.7 (5.3) | 1.8 (5.5) | |
| OB | 1.5 (5.6) | 1.7 (6.1) | |
| OC | 4.2 (4.1) | 3.1 (5.5) | |
| Anterior Disc Height (mm) | MB | 4.6 (3.7) | 3.0 (3.0) |
| MC | 4.1 (3.0) | 3.1 (3.1) | |
| OB | 6.0 (2.7) | 4.7 (3.2) | |
| OC | 5.6 (3.7) | 5.2 (4.2) | |
| Posterior Disc Height (mm) | MB | 2.7 (1.6) | 6.2 (1.1) |
| MC | 2.6 (2.4) | 1.9(2.6) | |
| OB | 3.7 (2.4) | 3.2 (2.3) | |
| OC | 1.3 (2.4) | 1.2 (3.0) | |
| Total Measurement | |||
| Implant Position | MB | 0.56 (0.07) | 0.55 (0.07) |
| MC | 0.61 (0.09) | 0.60 (0.10) | |
| OB | 0.54 (0.05) | 0.53 (0.06) | |
| OC | 0.69 (0.08) | 0.68 (0.10) | |
| Initial Postoperative | Final Postoperative | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 95% Confidence Interval | 95% Confidence Interval | |||||||||
| Comparison | Difference in Change | p-Value | Lower | Higher | Difference in Change | p-Value | Lower | Higher | ||
| Lumbar Lordosis (°) | MC | MB | 0.2 | 0.93 | −4.6 | 5.1 | 3.2 | 0.13 | −0.9 | 7.2 |
| OB | MB | 3.7 | 0.15 | −1.3 | 8.7 | 3.7 | 0.08 | −0.5 | 7.9 | |
| OC | MB | 3.1 | 0.19 | −1.5 | 7.7 | 2.1 | 0.28 | −1.7 | 6.0 | |
| OB | MC | 3.5 | 0.13 | −1.0 | 8.0 | 0.5 | 0.79 | −3.3 | 4.3 | |
| OC | MC | 2.9 | 0.17 | −1.2 | 7.0 | −1.0 | 0.56 | −4.5 | 2.4 | |
| OC | OB | −0.6 | 0.79 | −4.8 | 3.7 | −1.6 | 0.39 | −5.1 | 2.0 | |
| Segmental Lordosis (°) | MC | MB | 1.5 | 0.31 | −1.4 | 4.3 | 1.0 | 0.52 | −2.0 | 4.0 |
| OB | MB | 1.2 | 0.42 | −1.7 | 4.1 | 1.0 | 0.52 | −2.1 | 4.1 | |
| OC | MB | 3.3 | 0.02 | 0.6 | 6.0 | 2.3 | 0.11 | −0.5 | 5.2 | |
| OB | MC | −0.3 | 0.83 | −2.9 | 2.4 | 0.1 | 0.98 | −2.8 | 2.8 | |
| OC | MC | 1.9 | 0.13 | −0.5 | 4.3 | 1.3 | 0.30 | −1.2 | 3.9 | |
| OC | OB | 2.1 | 0.09 | −0.4 | 4.6 | 1.3 | 0.33 | −1.3 | 3.9 | |
| Anterior Disc Height (mm) | MC | MB | −0.1 | 0.54 | −2.3 | 1.2 | 0.2 | 0.88 | −1.7 | 2.0 |
| OB | MB | 1.4 | 0.12 | −0.4 | 3.2 | 1.8 | 0.06 | −0.1 | 3.7 | |
| OC | MB | 1.0 | 0.25 | −0.7 | 2.6 | 2.2 | 0.01 | 0.5 | 3.9 | |
| OB | MC | 2.0 | 0.02 | 0.3 | 3.6 | 1.6 | 0.06 | −0.1 | 3.3 | |
| OC | MC | 1.5 | 0.04 | 0.1 | 3.0 | 2.1 | 0.01 | 0.5 | 3.6 | |
| OC | OB | −0.4 | 0.58 | −2.0 | 1.1 | 0.4 | 0.61 | −1.2 | 2.0 | |
| Posterior Disc Height (mm) | MC | MB | −0.1 | 0.88 | −1.4 | 1.2 | −4.3 | 0.04 | −8.4 | −0.2 |
| OB | MB | 1.0 | 0.14 | −0.3 | 2.4 | −3.1 | 0.16 | −7.3 | 1.2 | |
| OC | MB | −1.4 | 0.03 | −2.7 | −0.2 | −5.0 | 0.01 | −9.0 | −1.1 | |
| OB | MC | 1.1 | 0.07 | −0.1 | 2.3 | 1.3 | 0.52 | −2.6 | 5.1 | |
| OC | MC | −1.3 | 0.02 | −2.44 | −0.22 | −0.7 | 0.68 | −4.2 | 2.8 | |
| OC | OB | −2.4 | <0.01 | −3.58 | −1.28 | −2.0 | 0.29 | −5.6 | 1.7 | |
| Implant Position | MC | MB | 0.62 | 0.02 | −0.12 | −0.01 | 0.05 | 0.18 | −0.11 | 0.02 |
| OB | MB | −0.17 | 0.86 | −0.07 | 0.04 | −0.02 | 0.02 | −0.12 | −0.01 | |
| OC | MB | 0.14 | <0.01 | 0.09 | 0.19 | 0.13 | <0.01 | 0.70 | 0.19 | |
| OB | MC | −0.08 | <0.01 | 0.03 | 0.13 | −0.07 | 0.02 | −0.12 | −0.01 | |
| OC | MC | 0.08 | <0.01 | 0.03 | 0.12 | 0.08 | <0.01 | 0.03 | 0.13 | |
| OC | OB | 0.15 | <0.01 | 0.02 | 0.20 | 0.15 | <0.01 | 0.09 | 0.20 | |
| Group | R2 | p-Value | |
|---|---|---|---|
| Implant Position vs. Initial Segmental Lordosis Correction | MB | −0.13 | 0.555 |
| MC | 0.566 | <0.001 | |
| OB | 0.475 | 0.009 | |
| OC | 0.203 | 0.187 | |
| Implant Position vs. Last Segmental Lordosis Correction | MB | 0.138 | 0.531 |
| MC | 0.346 | 0.034 | |
| OB | 0.512 | 0.005 | |
| OC | 0.215 | 0.162 | |
| Preoperative Anterior Disc Height vs. Initial Segmental Lordosis Correction | MB | 0.009 | 0.967 |
| MC | −0.27 | 0.123 | |
| OB | −0.052 | 0.004 | |
| OC | −0.169 | 0.274 | |
| Preoperative Anterior Disc Height vs. Final Segmental Lordosis Correction | MB | −0.313 | 0.146 |
| MC | −0.525 | 0.001 | |
| OB | −0.49 | 0.007 | |
| OC | −0.308 | 0.042 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wellington, I.J.; Kaufman, C.R.; Antonacci, C.L.; Coskun, E.; Cote, M.P.; Singh, H.; Mallozzi, S.S.; Moss, I.L. The Effects of Interbody Device Design and Placement on Lumbar Lordosis and Disc Height in Transforaminal Lumbar Interbody Fusion. Prosthesis 2023, 5, 752-762. https://doi.org/10.3390/prosthesis5030053
Wellington IJ, Kaufman CR, Antonacci CL, Coskun E, Cote MP, Singh H, Mallozzi SS, Moss IL. The Effects of Interbody Device Design and Placement on Lumbar Lordosis and Disc Height in Transforaminal Lumbar Interbody Fusion. Prosthesis. 2023; 5(3):752-762. https://doi.org/10.3390/prosthesis5030053
Chicago/Turabian StyleWellington, Ian J., Caroline R. Kaufman, Christopher L. Antonacci, Ergin Coskun, Mark P. Cote, Hardeep Singh, Scott S. Mallozzi, and Isaac L. Moss. 2023. "The Effects of Interbody Device Design and Placement on Lumbar Lordosis and Disc Height in Transforaminal Lumbar Interbody Fusion" Prosthesis 5, no. 3: 752-762. https://doi.org/10.3390/prosthesis5030053
APA StyleWellington, I. J., Kaufman, C. R., Antonacci, C. L., Coskun, E., Cote, M. P., Singh, H., Mallozzi, S. S., & Moss, I. L. (2023). The Effects of Interbody Device Design and Placement on Lumbar Lordosis and Disc Height in Transforaminal Lumbar Interbody Fusion. Prosthesis, 5(3), 752-762. https://doi.org/10.3390/prosthesis5030053