
Posterior Chamber Phakic Intraocular Lenses for the Correction of Myopia: Factors Influencing the Postoperative Refraction

 and
and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Preoperative and Postoperative Protocol
2.2. Surgical Procedure
2.3. Clinical Data Analysis
2.4. Paraxial Ray-Tracing
3. Results
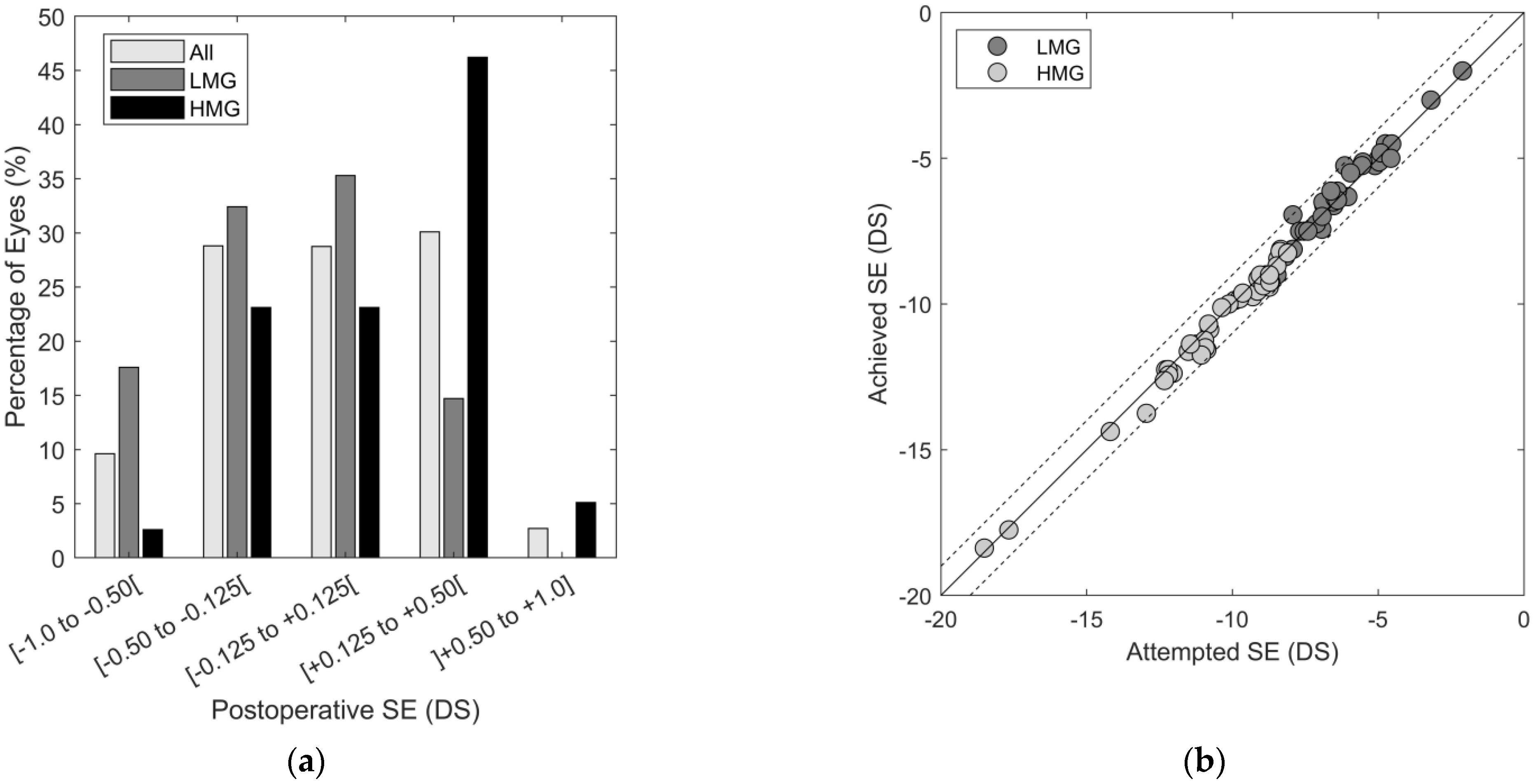
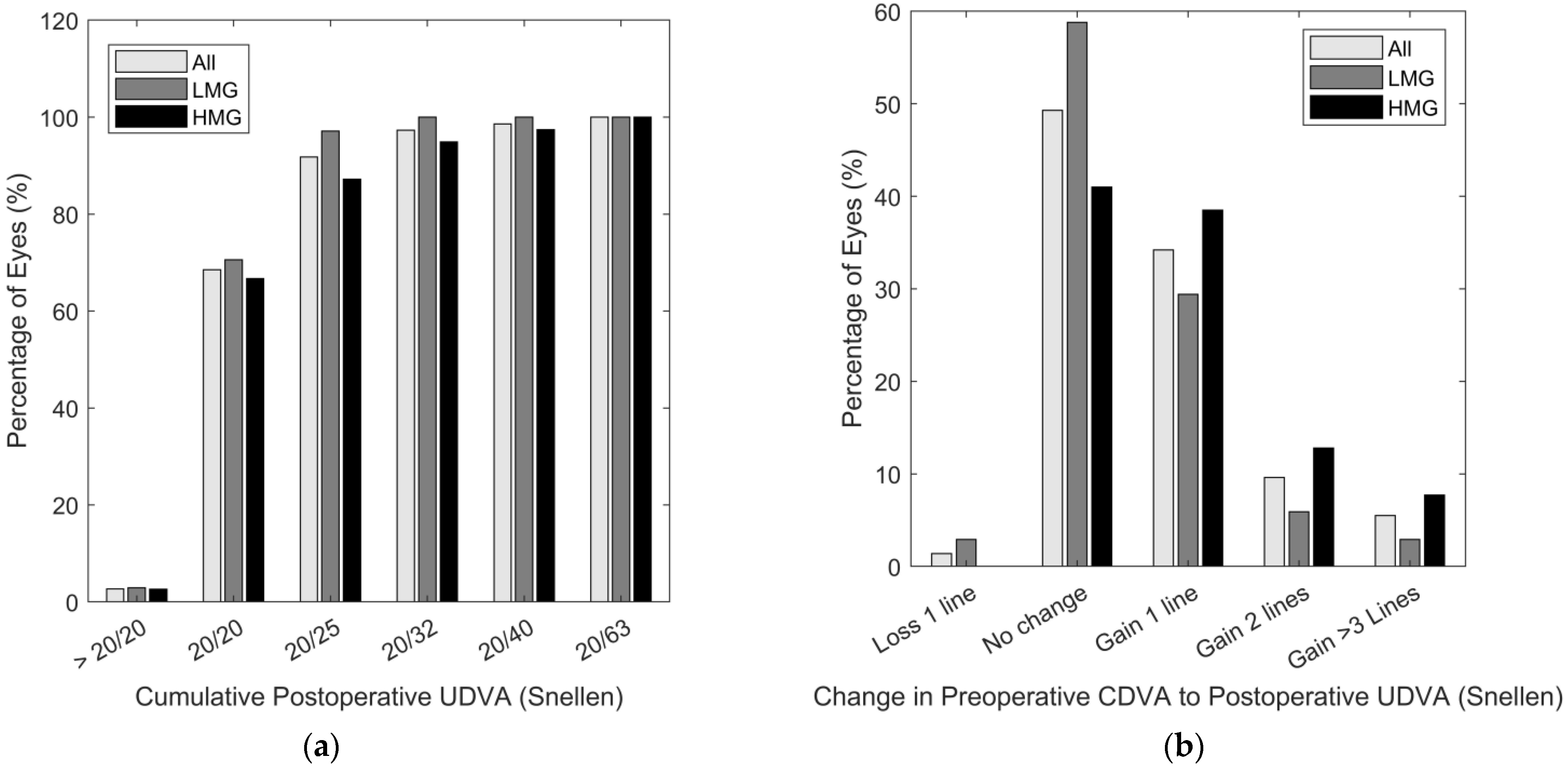
3.1. Clinical Data
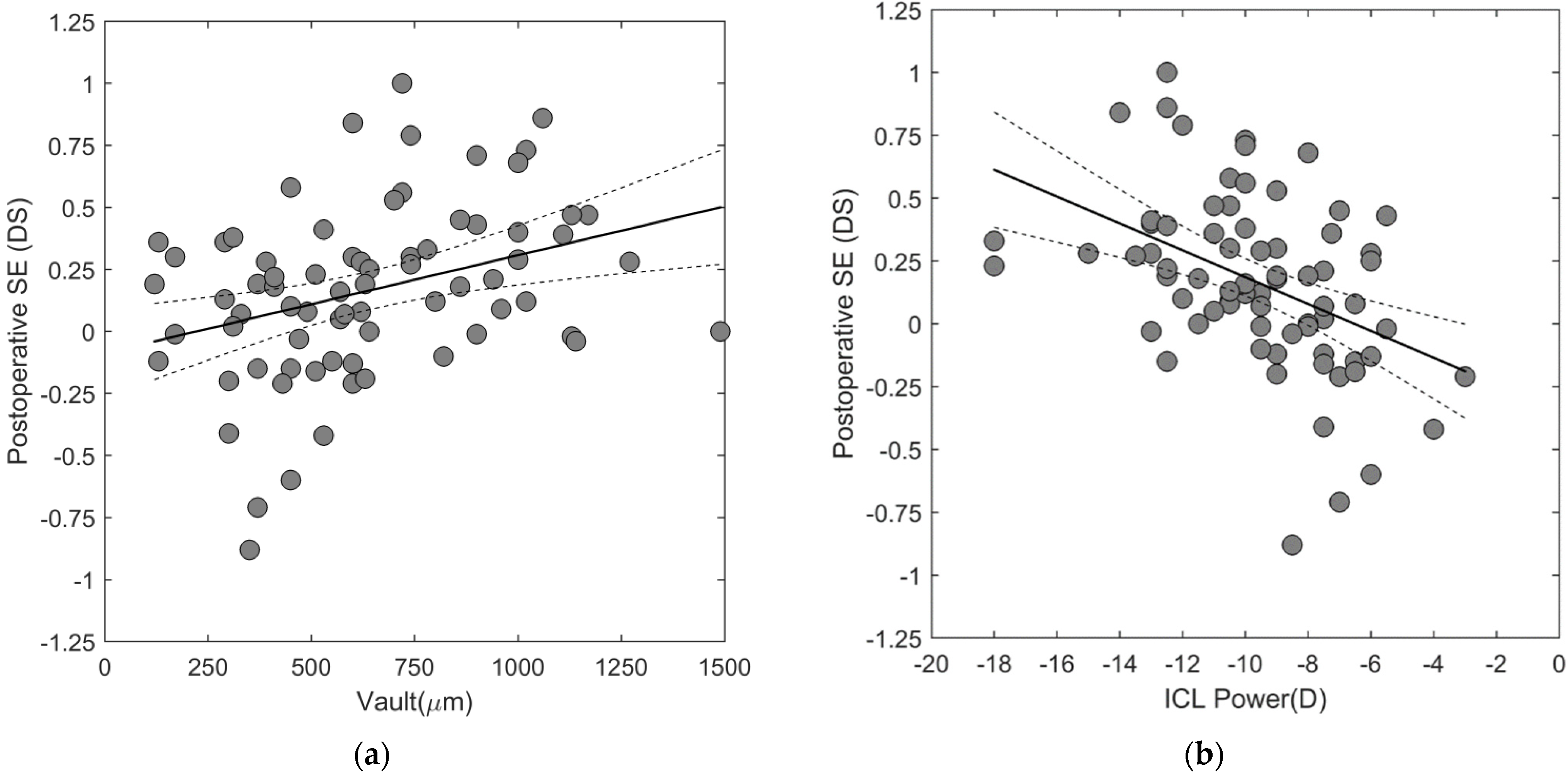
3.2. Association between Postoperative Refraction with Demographic, Anatomical, Refractive or ICL-Related Factors
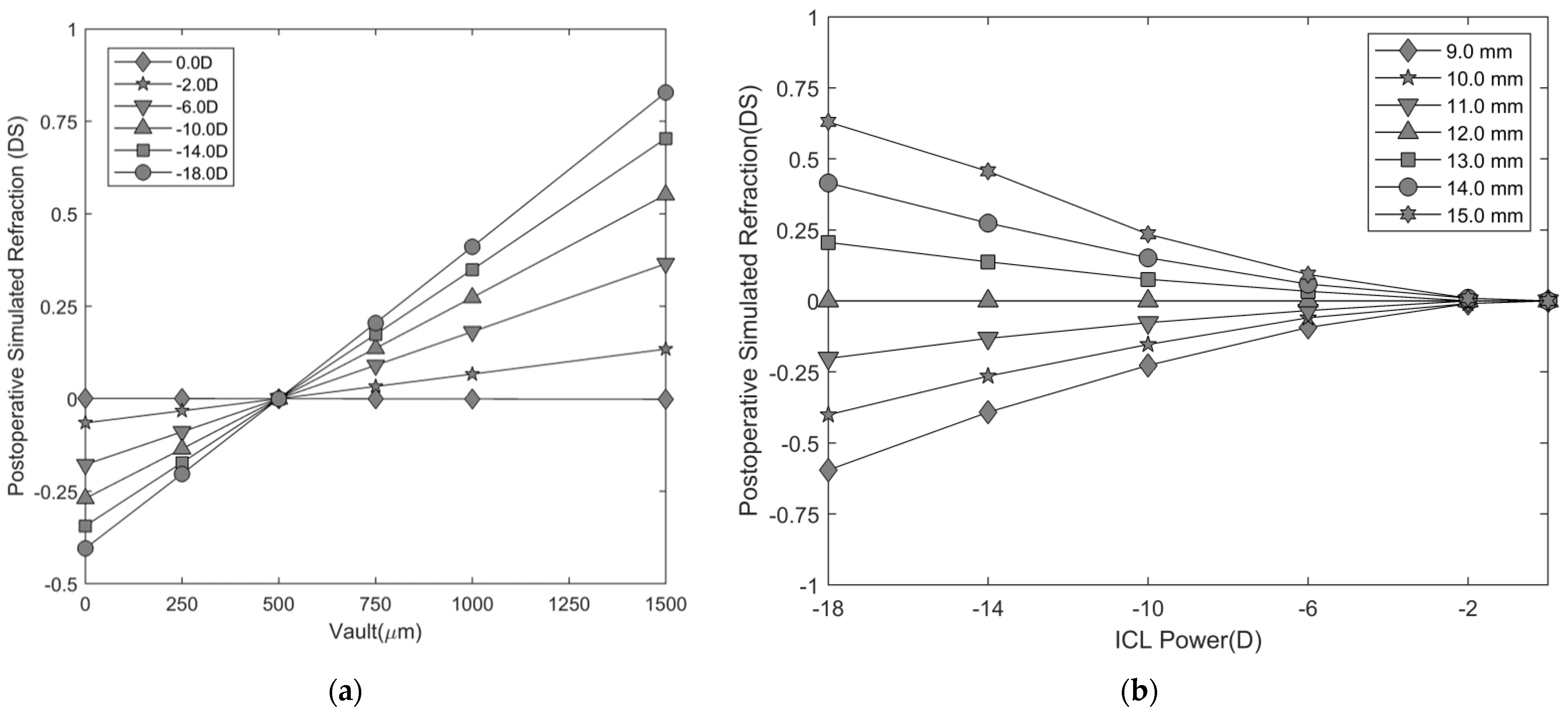
3.3. Paraxial Ray-Tracing
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pineda, R.; Chauhan, T. Phakic intraocular lenses and their special indications. JOVR 2016, 11, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Reinstein, D.Z.; Lovisolo, C.F.; Archer, T.J.; Gobbe, M. Comparison of postoperative vault height predictability using white-to-white or sulcus diameter-based sizing for the visian implantable collamer lens. J. Refract. Surg. 2013, 29, 30–35. [Google Scholar] [CrossRef]
- Packer, M. The Implantable Collamer Lens with a central port: Review of the literature. Clin. Ophthalmol. 2018, 12, 2427–2438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ieong, A.; Hau, S.C.H.; Rubin, G.S.; Allan, B.D.S. Quality of life in high myopia before and after implantable Collamer lens implantation. Ophthalmology 2010, 117, 2295–2300. [Google Scholar] [CrossRef]
- Atchison, D.A. Refractive errors induced by displacement of intraocular lenses within the pseudophakic eye. Optom. Vis. Sci. 1989, 66, 146–152. [Google Scholar] [CrossRef]
- Nawa, Y.; Ueda, T.; Nakatsuka, M.; Tsuji, H.; Marutani, H.; Hara, Y.; Uozato, H. Accommodation obtained per 1.0 mm forward movement of a posterior chamber intraocular lens. J. Cataract Refract. Surg. 2003, 29, 2069–2072. [Google Scholar] [CrossRef]
- Holladay, J.T. Refractive power calculations for intraocular lenses in the phakic eye. Am. J. Ophthalmol. 1993, 116, 63–66. [Google Scholar] [CrossRef]
- Lee, H.; Kang, D.S.; Choi, J.Y.; Ha, B.J.; Kim, E.K.; Seo, K.Y.; Kim, T.I. Analysis of pre-operative factors affecting range of optimal vaulting after implantation of 12.6-mm V4c implantable collamer lens in myopic eyes. BMC Ophthalmol. 2018, 18, 163. [Google Scholar] [CrossRef] [Green Version]
- Packer, M. Meta-analysis and review: Effectiveness, safety, and central port design of the intraocular collamer lens. Clin. Ophthalmol. 2016, 10, 1059–1077. [Google Scholar] [CrossRef] [Green Version]
- Kamiya, K.; Shimizu, K.; Kawamorita, T. Changes in vaulting and the effect on refraction after phakic posterior chamber intraocular lens implantation. J. Cataract Refract. Surg. 2009, 35, 1582–1586. [Google Scholar] [CrossRef]
- Weiss, R.; Berke, W.; Gottlieb, L.; Horvath, P. Clinical importance of accurate refractor vertex distance measurements prior to refractive surgery. J. Refract. Surg. 2002, 18, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Shimizu, K.; Igarashi, A.; Kitazawa, Y.; Kojima, T.; Nakamura, T.; Oka, Y.; Matsumoto, R. Posterior chamber phakic intraocular lens implantation: Comparative, multicentre study in 351 eyes with low-to-moderate or high myopia. Br. J. Ophthalmol. 2018, 102, 177–181. [Google Scholar] [CrossRef]
- Langenbucher, A.; Szentmáry, N.; Seitz, B. Magnification and accommodation with phakic intraocular lenses. Ophthalmic Physiol. Opt. 2007, 27, 295–302. [Google Scholar] [CrossRef]
- Hernández-Rodríguez, C.J.; Piñero, D.P. A systematic review about the impact of phakic intraocular lenses on accommodation. J. Optom. 2020, 13, 139. [Google Scholar] [CrossRef] [PubMed]
- Holladay, J.T. Proper method for calculating average visual acuity. J. Refract. Surg. 1997, 13, 388–391. [Google Scholar] [CrossRef]
- Atchison, D.A.; Smith, G. Optics of the Human Eye; Butterworth-Heinemann: Oxford, UK; Elsevier: Amsterdam, The Netherlands, 2000; p. 288. [Google Scholar]
- Langenbucher, A.; Reese, S.; Sauer, T.; Seitz, B. Matrix-based calculation scheme for toric intraocular lenses. Ophthalmic Physiol. Opt. 2004, 24, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Sanders, D.R.; Doney, K.; Poco, M. United States Food and Drug Administration clinical trial of the Implantable Collamer Lens (ICL) for moderate to high myopia: Three-year follow-up. Ophthalmology 2004, 111, 1683–1692. [Google Scholar]
- Alfonso, J.F.; Baamonde, B.; Fernández-Vega, L.; Fernandes, P.; González-Méijome, J.M.; Montés-Micó, R. Posterior chamber collagen copolymer phakic intraocular lenses to correct myopia: Five-year follow-up. J. Cataract Refract. Surg. 2011, 37, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Yan, Z.; Miao, H.; Zhao, F.; Wang, X.; Chen, X.; Li, M.; Zhou, X. Two-Year Outcomes of Visian Implantable Collamer Lens with a Central Hole for Correcting High Myopia. J. Ophthalmol. 2018, 2018, 8678352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, K.; Kamiya, K.; Igarashi, A.; Shiratani, T. Early clinical outcomes of implantation of posterior chamber phakic intraocular lens with a central hole (Hole ICL) for moderate to high myopia. Br. J. Ophthalmol. 2012, 96, 409–412. [Google Scholar] [CrossRef] [Green Version]
- García, M.; González, C.; Pascual, I.; Fimia, A. Magnification and visual acuity in highly myopic phakic eyes corrected with an anterior chamber intraocular lens versus by other methods. J. Cataract Refract. Surg. 1996, 22, 1416–1422. [Google Scholar] [CrossRef]
- Lee, D.H.; Choi, S.H.; Chung, E.S.; Chung, T.Y. Correlation between preoperative biometry and posterior chamber phakic Visian Implantable Collamer Lens vaulting. Ophthalmology 2012, 119, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Cerpa Manito, S.; Sánchez Trancón, A.; Torrado Sierra, O.; Baptista, A.M.; Serra, P.M. Biometric and ICL-related risk factors associated to sub-optimal vaults in eyes implanted with implantable collamer lenses. Eye Vis. 2021, 8, 26. [Google Scholar] [CrossRef]
- Mordi, J.A.; Ciuffreda, K.J. Static aspects of accommodation: Age and presbyopia. Vis. Res. 1998, 38, 1643–1653. [Google Scholar] [CrossRef] [Green Version]
- Trancón, A.S.; Manito, S.C.; Sierra, O.T.; Baptista, A.M.; Serra, P.M. Determining vault size in implantable collamer lenses: Preoperative anatomy and lens parameters. J. Cataract Refract. Surg. 2020, 46, 728–736. [Google Scholar] [CrossRef]
- Kamiya, K.; Ryu, I.H.; Yoo, T.K.; Kim, J.S.; Lee, I.S.; Kim, J.K.; Ando, W.; Shoji, N.; Yamauchi, T.; Tabuchi, H. Prediction of Phakic Intraocular Lens Vault Using Machine Learning of Anterior Segment Optical Coherence Tomography Metrics. Am. J. Ophthalmol. 2021, 226, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Ando, W.; Kamiya, K.; Hayakawa, H.; Takahashi, M.; Shoji, N. Comparison of Phakic Intraocular Lens Vault Using Conventional Nomogram and Prediction Formulas. J. Clin. Med. 2020, 9, 4090. [Google Scholar] [CrossRef]
- Nakamura, T.; Isogai, N.; Kojima, T.; Yoshida, Y.; Sugiyama, Y. Optimization of implantable collamer lens sizing based on swept-source anterior segment optical coherence tomography. J. Cataract Refract. Surg. 2020, 46, 742–748. [Google Scholar] [CrossRef]
- Igarashi, A.; Shimizu, K.; Kato, S.; Kamiya, K. Predictability of the vault after posterior chamber phakic intraocular lens implantation using anterior segment optical coherence tomography. J. Cataract Refract. Surg. 2019, 45, 1099–1104. [Google Scholar] [CrossRef]
- Sebag, M.; Meslin, D. Refraction: Vertex Distance Matters. Points de Vue. 2020, pp. 1–5. Available online: https://www.pointsdevue.com/sites/default/files/refraction_vertex_distance_matters.pdf (accessed on 10 December 2021).
- Gonzalez-Lopez, F.; Mompean, B.; Bilbao-Calabuig, R.; Vila-Arteaga, J.; Beltran, J.; Baviera, J. Dynamic Assessment of Light-Induced Vaulting Changes of Implantable Collamer Lens With Central Port by Swept-Source OCT: Pilot Study. Transl. Vis. Sci. Technol. 2018, 7, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, C.; Wang, J.; Wang, X.; Dong, Y.; Gu, Y.; Shen, Y. Ultrasound biomicroscopy of anterior segment accommodative changes with posterior chamber phakic intraocular lens in high myopia. Ophthalmology 2012, 119, 99–105. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Refractive Index | ||
|---|---|---|---|
| Spectacle Refraction | Variable | ||
| Vertex Distance (mm) | 12.0 | Air | 1.0 |
| Anterior Corneal Radius (mm) | 7.80 | ||
| Central Corneal Thickness (mm) | 0.55 | Cornea | 1.3771 |
| Posterior Corneal Radius (mm) | 6.50 | ||
| Cornea Endothelium to Crystalline Lens Anterior Surface Distance (Anterior Chamber Depth) (mm) | 3.05 | Aqueous humor | 1.3374 |
| Crystalline Lens Anterior Radius (mm) | 10.20 | ||
| Crystalline Lens Thickness (mm) | 4.00 | Crystalline lens | 1.420 |
| Crystalline Lens Posterior Radius (mm) | −6.00 | ||
| Vitreous Body Length (mm) | Variable | Vitreous body | 1.3360 |
| Model Eye with Refractive Surfaces Representative of an ICL | |||
| Cornea Endothelium to ICL Anterior Surface Distance (mm) | 2.32 | Aqueous Humor | 1.3374 |
| ICL Anterior Radius of Curvature (mm) | ∞ | ||
| ICL Thickness (mm) | 0.23 | ICL Refractive Index | 1.442 |
| ICL Posterior Radius of Curvature (mm) | Variable | ||
| ICL Posterior Surface to Crystalline Lens Anterior Surface Distance, i.e., Vault (mm) | 0.50 | Aqueous humor | 1.3374 |
| All (n = 73) | Low Myopia: ICL > −9.5 DS (n = 34) | High Myopia: ICL ≤ −9.5 DS (n = 39) | ||||
|---|---|---|---|---|---|---|
| Parameter | Mean ± SD | Range | Mean ± SD | Range | Mean ± SD | Range |
| Age (years) | 32.8 ± 8.7 | 18, 50 | 34.8 ± 9.0 | 20, 50 | 31.1 ± 8.1 | 18, 50 |
| Preoperative | ||||||
| Preoperative Refraction (Trail-frame ) | ||||||
| Sphere (DS) | −8.67 ± 2.93 | −19.00, −2.25 | −6.34 ± 1.40 | −8.50, −2.25 | −10.71 ± 2.33 | −19.00, −8.00 |
| Cylinder (DC) | −0.16 ± 0.26 | −0.75, 0.00 | −0.19 ± 0.28 | −0.75, 0.00 | −0.14 ± 0.24 | −0.75, 0.00 |
| Spherical Equivalent (DS) | −8.76 ± 2.90 | −19.00, −2.63 | −6.43 ± 1.3 | −8.50, −2.63 | −10.78 ± 2.32 | −19.00, −8.00 |
| CDVA (logMAR) | 0.07 ± 0.11 | 0.0, 0.40 | 0.04 ± 0.05 | 0.00, 0.40 | 0.12 ± 0.16 | 0.0, 0.70 |
| Biometry | ||||||
| CCT (µm) | 531.8 ± 33.2 | 473.0, 610.0 | 518.1 ± 27.6 | 479.0, 582.0 | 543.8 ± 35.1 | 473.0, 610.0 |
| Mean Sim K (DS) | 44.2 ± 1.5 | 40.30, 47.6 | 44.2 ± 1.4 | 40.3, 46.6 | 44.2 ± 1.7 | 40.3, 47.6 |
| Corneal Astigmatism (DC) | −0.66 ± 0.39 | −1.70, 0.00 | −0.69 ± 0.38 | −1.70, 0.00 | −0.64 ± 0.40 | −1.50, 0.00 |
| WTW (mm) | 12.1 ± 0.3 | 11.4, 12.8 | 12.1 ± 0.3 | 11.5, 12.8 | 12.1 ± 0.3 | 11.4, 12.8 |
| ACD (mm) | 3.26 ± 0.24 | 2.80, 3.80 | 3.25 ± 0.23 | 2.80, 3.80 | 3.27 ± 0.25 | 2.84, 3.80 |
| ICL Power (DS) | −9.63 ± 2.86 | −18.00, −3.00 | −7.26 ± 1.46 | −9.00, −3.00 | −11.69 ± 2.06 | −18.00, −9.50 |
| Postoperative Predicted Refraction | ||||||
| Sphere (DS) | −0.02 ± 0.25 | −0.48, +0.88 | ±0.00 ± 0.26 | −0.38, +0.88 | −0.03 ± 0.24 | −0.48, +0.67 |
| Cylinder (DC) | −0.16 ± 0.21 | −0.71, 0.00 | −0.18 ± 0.24 | −0.71, ±0.00 | −0.14 ± 0.18 | −0.56, ± 0.00 |
| Spherical Equivalent (DS) | −0.10 ± 0.22 | −0.55, +0.68 | −0.09 ± 0.22 | −0.50, +0.68 | −0.10 ± 0.22 | −0.55, +0.67 |
| Postoperative | ||||||
| Follow-Up (days) | 99 ± 36 | 41 – 366 | 105 ± 23 | 76, 167 | 99 ± 62 | 41 – 366 |
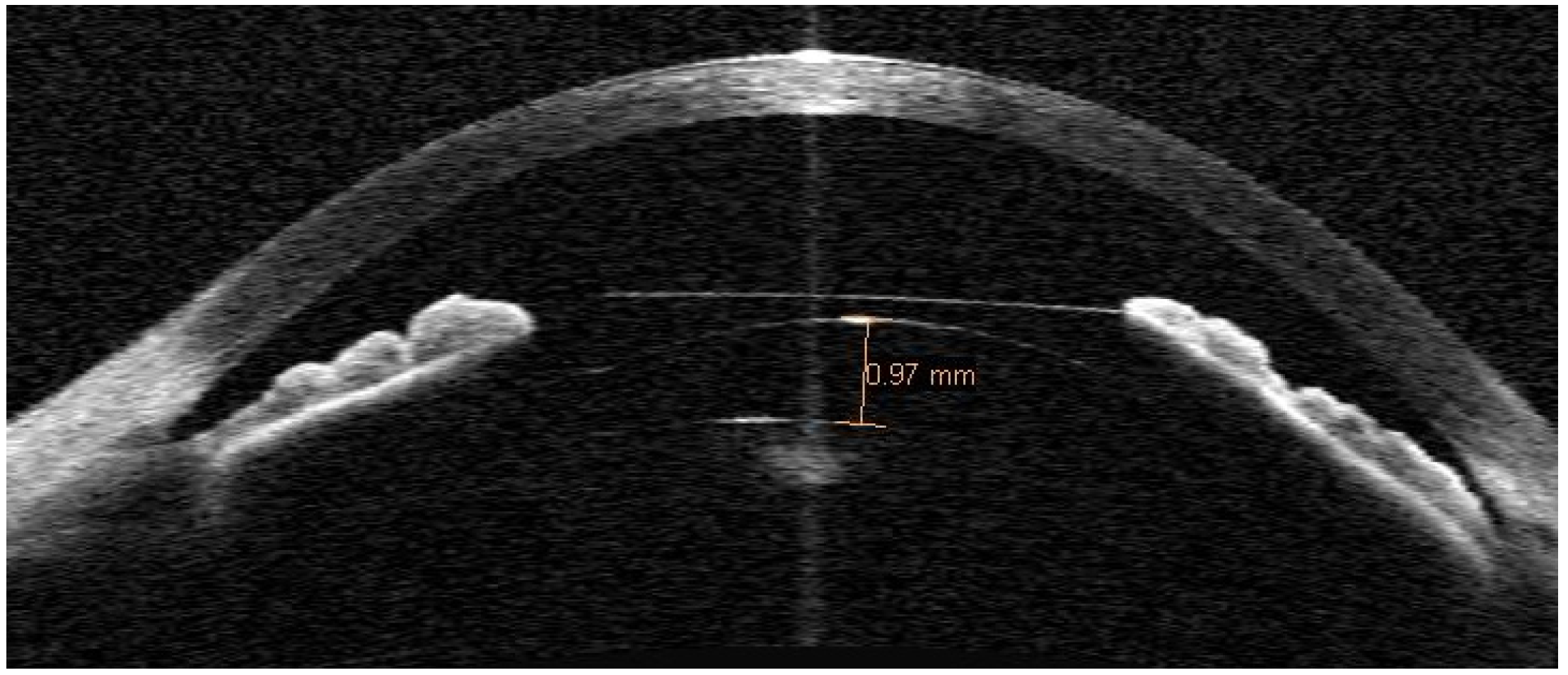
| Vault (µm) | 641.9 ± 303.7 | 120.0, 1490.0 | 590.3 ± 320.4 | 120, 1490 | 686.9 ± 284.9 | 170.0, 1270.0 |
| Postoperative Manifest Refraction | ||||||
| Sphere (DS) | ±0.15 ± 0.38 | −0.75, +1.25 | 0.00 ± 0.34 | −0.75, +0.62 | +0.29 ± 0.37 | −0.37, +1.25 |
| Cylinder (DC) | −0.35 ± 0.25 | −1.00, ± 0.00 | −0.31 ± 0.26 | −1.00, ± 0.00 | −0.38 ± 0.24 | −1.00, 0.00 |
| Spherical Equivalent (DS) | −0.02 ± 0.37 | −0.88, +0.75 | −0.16 ± 0.36 | −0.88, +0.50 | +0.09 ± 0.35 | −0.63, +0.75 |
| UDVA (logMAR) | 0.03 ± 0.08 | −0.08, 0.30 | 0.02 ± 0.05 | −0.08, 0.30 | 0.06 ± 0.13 | −0.08, 0.50 |
| Postoperative Manifest–Predicted Refraction | ||||||
| Spherical Equivalent (DS) | +0.07 ± 0.33 | −0.99, +0.80 | +0.07 ± 0.34 | −0.99, +0.53 | +0.19 ± 0.28 | −0.25, +0.80 |
| Correlation between Postoperative SE § vs. | All (n = 73) | Low Myopia: ICL > −9.5 DS (n = 34) | High Myopia: ICL ≤ −9.5 DS (n = 39) |
|---|---|---|---|
| Age (years) | R = −0.071 p = 0.553 | R = 0.002 p = 0.992 | R = 0.089 p = 0.589 |
| Preoperative Spherical Equivalent (DS) | R = −0.367 p = 0.001 * | R = −0.217 p = 0.218 | R = −0.027 p = 0.871 |
| Central Corneal Thickness (µm) | R = 0.205 p = 0.081 | R = 0.289 p = 0.098 | R = −0.078 p = 0.639 |
| Keratometry (DS) | R = 0.209 p = 0.058 | R = 0.111 p= 0.533 | R = 0.313 p = 0.052 |
| Corneal Cylinder (DC) | R = −0.091 p= 0.445 | R = −0.068 p= 0.704 | R = −0.160 p = 0.330 |
| White-to-White Distance (mm) | R = 0.181 p = 0.126 | R = −0.105 p = 0.556 | R = 0.029 p = 0.860 |
| Anterior Chamber Depth (mm) | R = −0.023 p = 0.845 | R = 0.011 p = 0.952 | R = 0.311 p = 0.054 |
| ICL Power (DS) | R = −0.382 p = 0.001 * | R = −0.230 p = 0.191 | R = −0.091 p = 0.584 |
| Vault (µm) | R = 0.408 p = 0.001 * | R = 0.410 p = 0.016 * | R = 0.356 p = 0.026 * |
| Refractive Error Spectacle Plane (DS) 12.0 mm | Vitreous Body Length (mm) | Eye Axial Length (mm) | ICL | |
|---|---|---|---|---|
| Posterior Radius of Curvature (mm) | Power (D) | |||
| 0 | 16.66 | 24.2 | −3787.3 | 0.03 |
| −2.00 | 17.34 | 24.9 | 4.41 | −2.37 |
| −6.00 | 18.86 | 26.5 | 1.54 | −6.78 |
| −10.00 | 20.43 | 28.0 | 0.97 | −10.78 |
| −14.00 | 22.04 | 29.6 | 0.73 | −14.33 |
| −18.00 | 23.68 | 31.3 | 0.59 | −17.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serra, P.; Sánchez Trancón, Á.; Torrado Sierra, O.; Baptista, A.; Cerpa Manito, S. Posterior Chamber Phakic Intraocular Lenses for the Correction of Myopia: Factors Influencing the Postoperative Refraction. Optics 2021, 2, 292-305. https://doi.org/10.3390/opt2040028
Serra P, Sánchez Trancón Á, Torrado Sierra O, Baptista A, Cerpa Manito S. Posterior Chamber Phakic Intraocular Lenses for the Correction of Myopia: Factors Influencing the Postoperative Refraction. Optics. 2021; 2(4):292-305. https://doi.org/10.3390/opt2040028
Chicago/Turabian StyleSerra, Pedro, Ángel Sánchez Trancón, Oscar Torrado Sierra, António Baptista, and Santiago Cerpa Manito. 2021. "Posterior Chamber Phakic Intraocular Lenses for the Correction of Myopia: Factors Influencing the Postoperative Refraction" Optics 2, no. 4: 292-305. https://doi.org/10.3390/opt2040028
APA StyleSerra, P., Sánchez Trancón, Á., Torrado Sierra, O., Baptista, A., & Cerpa Manito, S. (2021). Posterior Chamber Phakic Intraocular Lenses for the Correction of Myopia: Factors Influencing the Postoperative Refraction. Optics, 2(4), 292-305. https://doi.org/10.3390/opt2040028