Effect of High-Dose Intravenous Vitamin C on Postpartum Oxidative Stress in Severe Preeclampsia

 , ,
, ,
Abstract
:1. Introduction
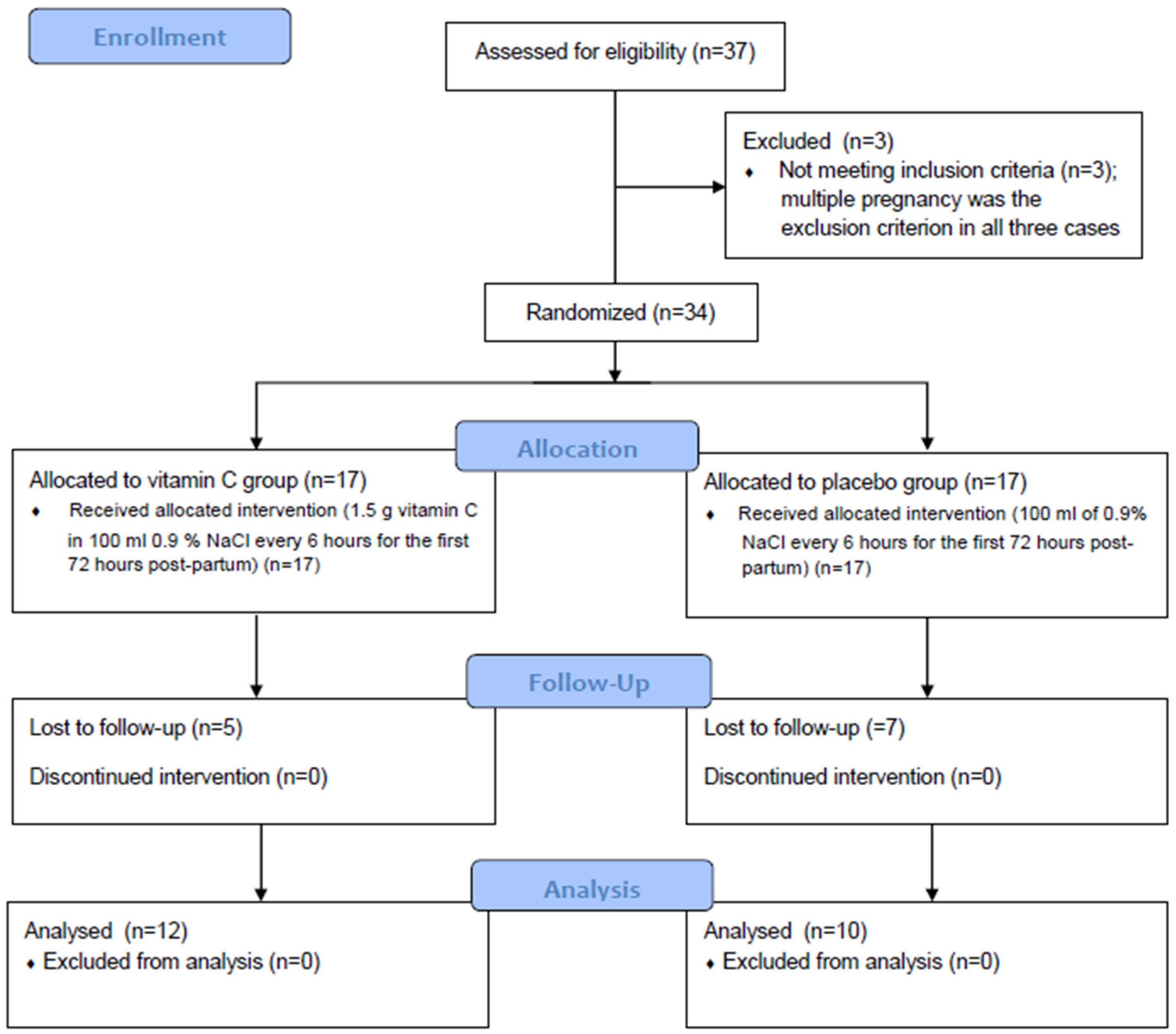
2. Methods
2.1. Oxidative Stress Biomarker Measurements
2.2. Statistical Analysis
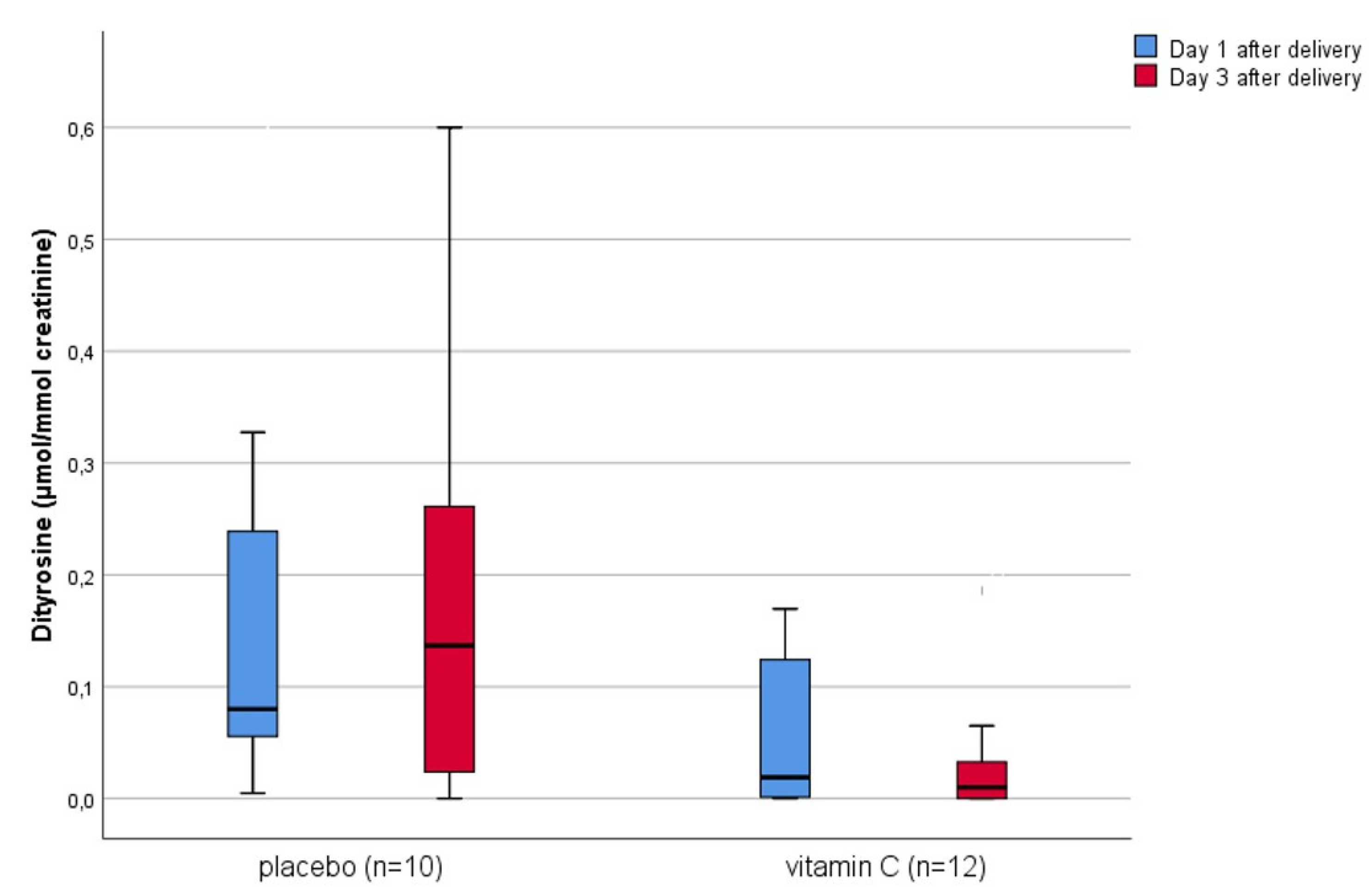
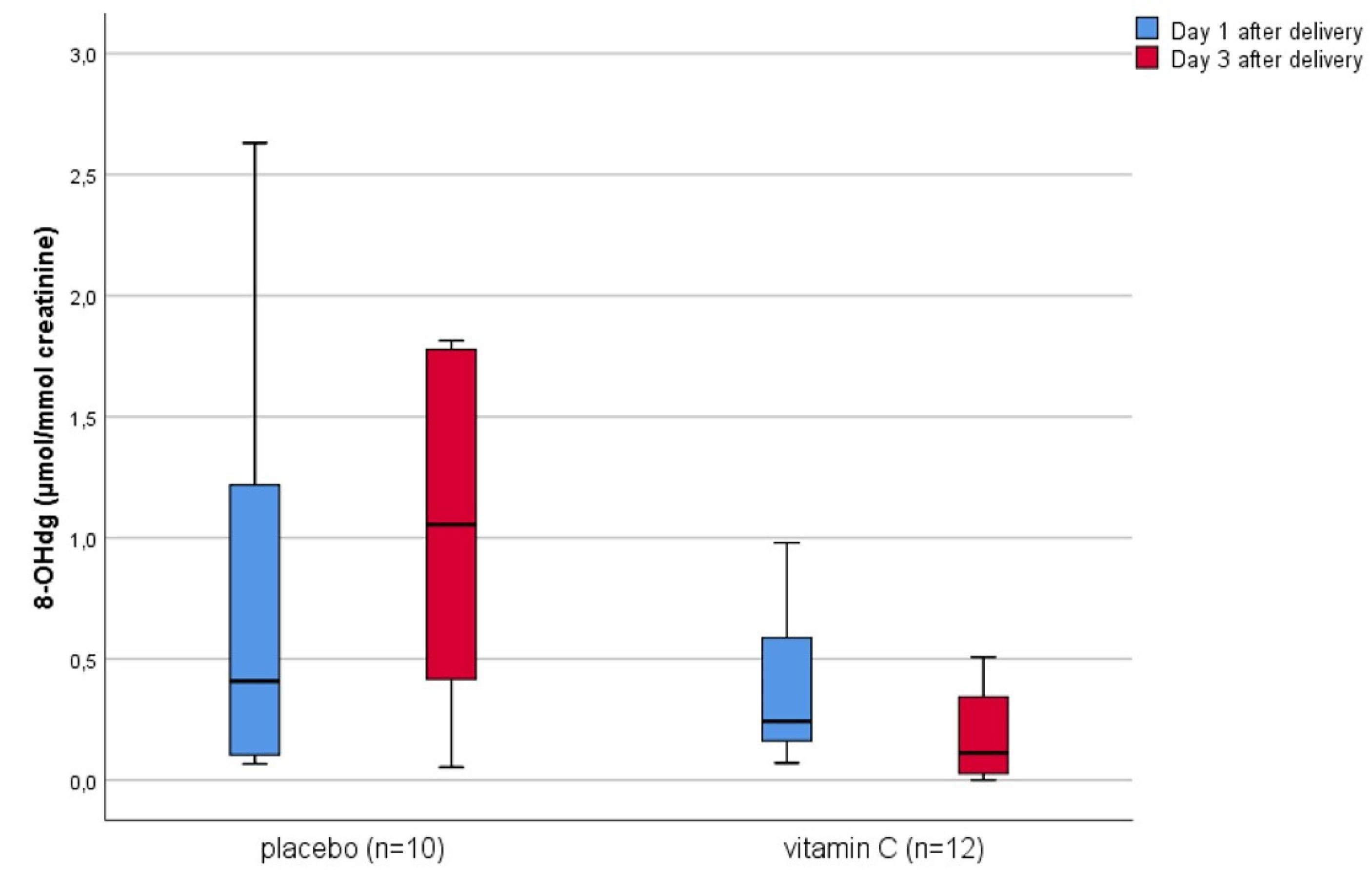
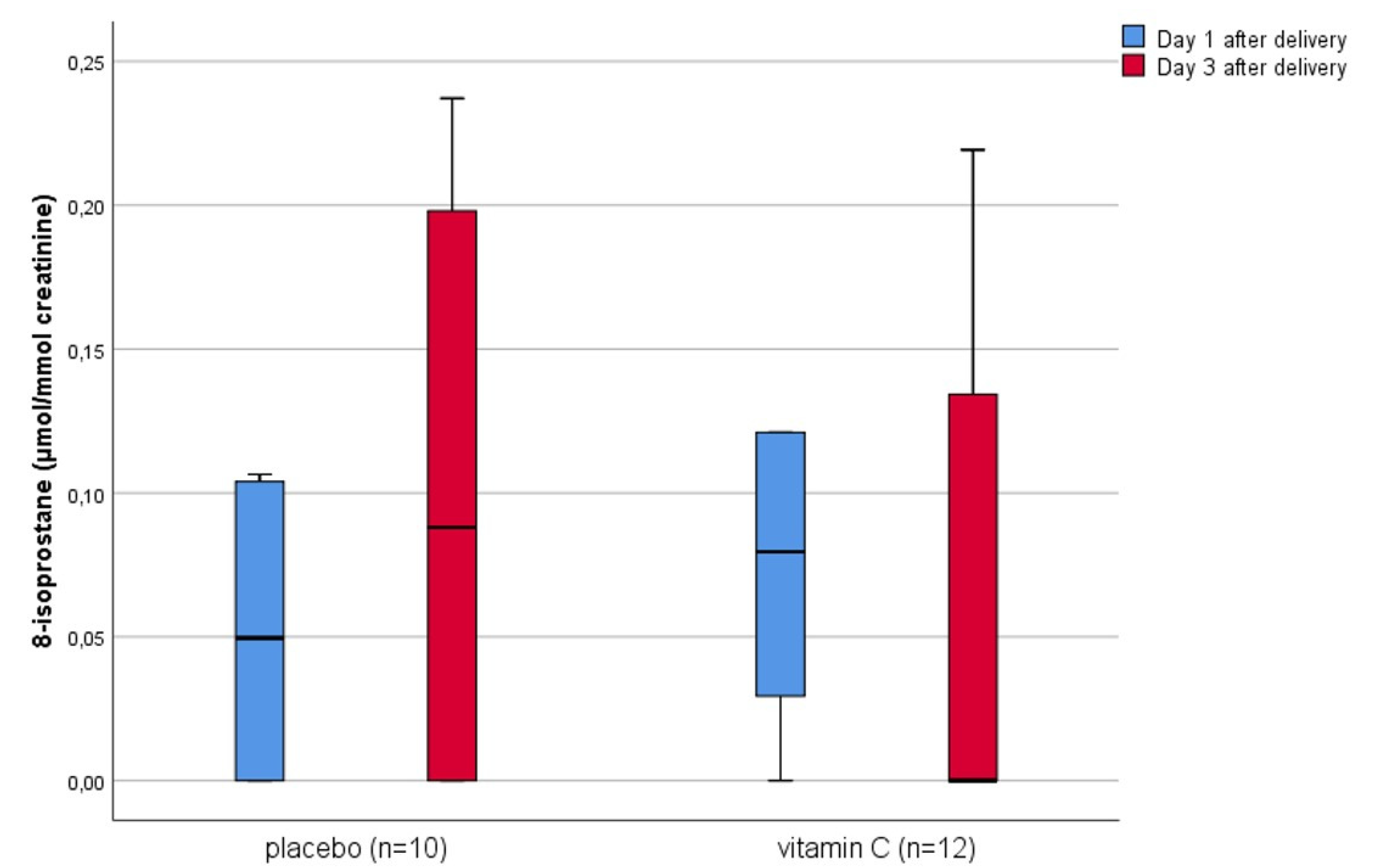
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Ananth, C.V.; Keyes, K.M.; Wapner, R.J. Pre-eclampsia rates in the United States, 1980–2010: Age-period-cohort analysis. BMJ 2013, 347, f6564. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Díaz, S.; Toh, S.; Cnattingius, S. Risk of pre-eclampsia in first and subsequent pregnancies: Prospective cohort study. BMJ 2009, 338, b2255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutcheon, J.A.; Lisonkova, S.; Joseph, K.S. Epidemiology of pre-eclampsia and the other hypertensive disorders of pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2011, 25, 391–403. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists; Task Force on Hypertension in Pregnancy. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet. Gynecol. 2013, 122, 1122–1131. [Google Scholar] [CrossRef]
- World Health Organization. The World Health Report 2005: Make Every Mother and Child Count. 2005. Available online: https://www.who.int/whr/2005/whr2005_en.pdf?ua=1 (accessed on 28 May 2020).
- Chaiworapongsa, T.; Chaemsaithong, P.; Yeo, L.; Romero, R. Pre-eclampsia part 1: Current understanding of its pathophysiology. Nat. Rev. Nephrol. 2014, 10, 466–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabello-Verrugio, C.; Simon, F.; Trollet, C.; Santibañez, J.F. Oxidative stress in disease and aging: Mechanisms and therapies 2016. Oxid. Med. Cell. Longev. 2017, 4310469. [Google Scholar] [CrossRef]
- McClure, J.H.; Cooper, G.M.; Clutton-Brock, T.H.; Centre for Maternal and Child Enquiries. Saving mothers’ lives: Reviewing maternal deaths to make motherhood safer: 2006-8: A review. Br. J. Anaesth. 2011, 107, 127–132. [Google Scholar] [CrossRef] [Green Version]
- Staff, A.C.; Benton, S.J.; von Dadelszen, P.; Roberts, J.M.; Taylor, R.N.; Powers, R.W.; Charnock-Jones, D.S.; Redman, C.W. Redefining preeclampsia using placenta-derived biomarkers. Hypertension 2013, 61, 932–942. [Google Scholar] [CrossRef] [Green Version]
- Mikhail, M.S.; Anyaegbunam, A.; Garfinkel, D.; Palan, P.R.; Basu, J.; Romney, S.L. Preeclampsia and antioxidant nutrients: Decreased plasma levels of reduced ascorbic acid, alpha-tocopherol, and beta-carotene in women with preeclampsia. Am. J. Obstet. Gynecol. 1994, 171, 150–157. [Google Scholar] [CrossRef]
- Honore, P.M.; Jacobs, R.; Hendrickx, I.; De Waele, E.; Spapen, H.D. Adjuvant vitamin C treatment in sepsis-how many oranges a day keep (vasopressor-dependent) septic shock away? J. Thorac. Dis. 2016, 8, E993–E995. [Google Scholar] [CrossRef]
- Lichtenstein, D.; Mézière, G.; Biderman, P.; Gepner, A.; Barré, O. The comet-tail artifact. An ultrasound sign of alveolar-interstitial syndrome. Am. J. Respir. Crit. Care Med. 1997, 156, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Buehner, M.; Pamplin, J.; Studer, L.; Hughes, R.L.; King, B.T.; Graybill, J.C.; Chung, K.K. Oxalate nephropathy after continuous infusion of high-dose vitamin C as an adjunct to burn resuscitation. J. Burn Care Res. 2016, 37, e374–e379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagamine, J.; Hansen, J.; Ashmore, R.C. Postpartum preeclampsia complicated by acute pulmonary edema. Hawaii Med. J. 1994, 53, 248–249. [Google Scholar] [PubMed]
- Matthys, L.A.; Coppage, K.H.; Lambers, D.S.; Barton, J.R.; Sibai, B.M. Delayed postpartum preeclampsia: An experience of 151 cases. Am. J. Obstet. Gynecol. 2004, 190, 1464–1466. [Google Scholar] [CrossRef]
- Chappell, L.C.; Seed, P.T.; Briley, A.L.; Kelly, F.J.; Lee, R.; Hunt, B.J.; Parmar, K.; Bewley, S.J.; Shennan, A.H.; Steer, P.J.; et al. Effect of antioxidants on the occurrence of pre-eclampsia in women at increased risk: A randomised trial. Lancet 1999, 354, 810–816. [Google Scholar] [CrossRef]
- Beazley, D.; Ahokas, R.; Livingston, J.; Griggs, M.; Sibai, B.M. Vitamin C and E supplementation in women at high risk for preeclampsia: A double-blind, placebo-controlled trial. Am. J. Obstet. Gynecol. 2005, 192, 520–521. [Google Scholar] [CrossRef]
- Rumbold, A.R.; Crowther, C.A.; Haslam, R.R.; Dekker, G.A.; Robinson, J.S.; ACTS Study Group. Vitamins C and E and the risks of preeclampsia and perinatal complications. N. Engl. J. Med. 2006, 354, 1796–1806. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, T.; Tanaka, H.; Hanumadass, M.; Gayle, R.; Yuasa, H.; Abcarian, H.; Matsuda, H.; Reyes, H. Effects of high-dose vitamin C administration on postburn microvascular fluid and protein flux. J. Burn Care Rehabil. 1992, 13, 560–566. [Google Scholar] [CrossRef]
- Matsuda, T.; Tanaka, H.; Reyes, H.M.; Richter, H.M., 3rd; Hanumadass, M.M.; Shimazaki, S.; Matsuda, H.; Nyhus, L.M. Antioxidant therapy using high dose vitamin C: Reduction of postburn resuscitation fluid volume requirements. World J. Surg. 1995, 19, 287–291. [Google Scholar] [CrossRef]
- Teng, J.; Pourmand, A.; Mazer-Amirshahi, M. Vitamin C: The next step in sepsis management? J. Crit. Care 2018, 43, 230–234. [Google Scholar] [CrossRef]
- Pryor, W.A. Oxy-radicals and related species: Their formation, lifetimes, and reactions. Annu. Rev. Physiol. 1986, 48, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Halliwell, B.; Whiteman, M. Measuring reactive species and oxidative damage in vivo and in cell culture: How should you do it and what do the results mean? Br. J. Pharmacol. 2004, 142, 231–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Il’yasova, D.; Scarbrough, P.; Spasojevic, I. Urinary biomarkers of oxidative status. Clin. Chim. Acta 2012, 413, 1446–1453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakai, K.; Kino, S.; Masuda, A.; Takeuchi, M.; Ochi, T.; Osredkar, J.; Rejc, B.; Gersak, K.; Ramarathnam, N.; Kato, Y. Determination of HEL (Hexanoyl-lysine adduct): A novel biomarker for omega-6 PUFA oxidation. Subcell. Biochem. 2014, 77, 61–72. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Ogawa, Y.; Yoshida, R.; Shimamori, A.; Kasai, H.; Ohta, H. The stability of the oxidative stress marker, urinary 8-hydroxy-2′-deoxyguanosine (8-OHdG), when stored at room temperature. J. Occup. Health 2008, 50, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Czerska, M.; Mikołajewska, K.; Zieliński, M.; Gromadzińska, J.; Wąsowicz, W. Today’s oxidative stress markers. Med. Pr. 2015, 66, 393–405. [Google Scholar] [CrossRef]
- León-Reyes, G.; Maida-Claros, R.F.; Urrutia-Medina, A.X.; Jorge-Galarza, E.; Guzmán-Grenfell, A.M.; Fuentes-García, S.; Medina-Navarro, R.; Moreno-Eutimio, M.A.; Muñoz-Sánchez, J.L.; Hicks, J.J.; et al. Oxidative profiles of LDL and HDL isolated from women with preeclampsia. Lipids Health Dis. 2017, 16, 90. [Google Scholar] [CrossRef] [Green Version]
- Scholl, T.O.; Stein, T.P. Oxidant damage to DNA and pregnancy outcome. J. Matern. Fetal Med. 2001, 10, 182–185. [Google Scholar] [CrossRef]
- Barden, A.; Beilin, L.J.; Ritchie, J.; Croft, K.D.; Walters, B.N.; Michael, C.A. Plasma and urinary 8-iso-prostane as an indicator of lipid peroxidation in pre-eclampsia and normal pregnancy. Clin. Sci. 1996, 91, 711–718. [Google Scholar] [CrossRef] [Green Version]
- McKinney, E.T.; Shouri, R.; Hunt, R.S.; Ahokas, R.A.; Sibai, B.M. Plasma, urinary, and salivary 8-epi-prostaglandin f2alpha levels in normotensive and preeclamptic pregnancies. Am. J. Obstet. Gynecol. 2000, 183, 874–877. [Google Scholar] [CrossRef]
- Yancey, L.M.; Withers, E.; Bakes, K.; Abbott, J. Postpartum preeclampsia: Emergency department presentation and management. J. Emerg. Med. 2011, 40, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Dennis, A.T.; Solnordal, C.B. Acute pulmonary oedema in pregnant women. Anaesthesia 2012, 67, 646–659. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick, S.J.; Berg, C.; Bernstein, P.; Bingham, D.; Delgado, A.; Callaghan, W.M.; Harris, K.; Lanni, S.; Mahoney, J.; Main, E.; et al. Standardized severe maternal morbidity review: Rationale and process. Obstet. Gynecol. 2014, 124, 361–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Vitamin C (n = 12) | Placebo (n = 10) | p-Value |
|---|---|---|---|
| Maternal age (years) | 30 (22–41) | 30 (23–40) | 0.97 |
| Pre-pregnancy BMI (kg/m2) | 23 (17–35) | 26 (18–41) | 0.23 |
| BMI at delivery (kg/m2) | 29 (22–56) | 31 (20–49) | 0.69 |
| Nulliparity | 10 (83%) | 7 (70%) | 0.28 |
| Gestational age (weeks) | 33 (24–38) | 33 (26–39) | 0.38 |
| Caesarean delivery | 9 (75%) | 9 (90%) | 0.69 |
| Neonatal birth weight (g) | 1465 (490–3110) | 1820 (630–3870) | 0.33 |
| SGA | 8 (67%) | 4 (40%) | 0.15 |
| Systolic blood pressure ≥160 mm Hg at inclusion | 12 (100%) | 10 (100%) | / |
| Diastolic blood pressure ≥110 mm Hg at inclusion | 12 (100%) | 10 (100%) | / |
| Neurological symptoms | 3 (25%) | 4 (40%) | 0.21 |
| Serum creatinine >97 µmol/L | 1 (8%) | 0 (0%) | 0.33 |
| Elevated liver enzymes and/or pain in the right upper or middle upper abdomen | 8 (67%) | 3 (30%) | 0.09 |
| Thrombocytopenia | 3 (25%) | 2 (20%) | 0.78 |
| Urine output at inclusion (mL/kg/h) | 0.62 (0.40–1.17) | 0.52 (0.27–1.33) | 0.42 |
| Serum creatinine at inclusion (µmol/L) | 59 (48–133) | 55 (43–67) | 0.35 |
| sFlt-1/PlGF | 268 (152–2324) | 399 (111–998) | 0.12 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korenc, M.; Osredkar, J.; Gersak, K.; Kumer, K.; Fabjan, T.; Sterpin, S.; Lucovnik, M. Effect of High-Dose Intravenous Vitamin C on Postpartum Oxidative Stress in Severe Preeclampsia. Reprod. Med. 2020, 1, 122-131. https://doi.org/10.3390/reprodmed1020009
Korenc M, Osredkar J, Gersak K, Kumer K, Fabjan T, Sterpin S, Lucovnik M. Effect of High-Dose Intravenous Vitamin C on Postpartum Oxidative Stress in Severe Preeclampsia. Reproductive Medicine. 2020; 1(2):122-131. https://doi.org/10.3390/reprodmed1020009
Chicago/Turabian StyleKorenc, Monika, Joško Osredkar, Ksenija Gersak, Kristina Kumer, Teja Fabjan, Sasa Sterpin, and Miha Lucovnik. 2020. "Effect of High-Dose Intravenous Vitamin C on Postpartum Oxidative Stress in Severe Preeclampsia" Reproductive Medicine 1, no. 2: 122-131. https://doi.org/10.3390/reprodmed1020009
APA StyleKorenc, M., Osredkar, J., Gersak, K., Kumer, K., Fabjan, T., Sterpin, S., & Lucovnik, M. (2020). Effect of High-Dose Intravenous Vitamin C on Postpartum Oxidative Stress in Severe Preeclampsia. Reproductive Medicine, 1(2), 122-131. https://doi.org/10.3390/reprodmed1020009