1. Introduction
Living kidney donation has significantly and gradually increased in the United States, with 6867 donations being performed in 2019 [
1]. Technical advancement from an open to minimally invasive approach has impactfully contributed to the increased organ donation efforts by living kidney donors. Laparoscopic living donor nephrectomy (LLDN), first adopted in 1995 [
2], is now considered a standard surgical approach for kidney donation due to the decreased morbidity, mortality, and better recovery when compared to open nephrectomy [
3]. Benefits of such a minimally invasive approach are largely due to better pain management. However, despite the technical advantage of LLDN, its benefits are not fully utilized, as patients still require opioids for optimal pain management [
4], most of whom are opioid-naïve and would not be exposed to opioids if not for the kidney donation.
In 2017, more than 47,000 people in the United States died due to opioid overdose with 1.7 million people suffering from substance use disorders [
5]. Pain management with opioids is a careful balance of risk and benefits due to the association of significant adverse effects including, hyperalgesia, sedation, and physical dependence. Conversely, inadequate pain control is also associated with adverse events like, significantly reduced quality of life, impaired sleep, and impaired physical function [
6,
7]. Therefore, it is essential that healthcare providers use a balanced approach when managing postoperative pain. This consideration is particularly vital and ethically prudent for living donors, wherein, maintaining a double equipoise, i.e., a balance of donor risk versus recipient benefit, is essential. Hence, alternate modes of providing safe and effective analgesics are indeed timely to match the technical advancements in health care for improved patient satisfaction and better patient experience.
An example of an advanced form of perioperative analgesia to match the technical advancements of surgery and patient needs is a transverse abdominis plane (TAP) block, which is a perineural block that affects the anterior rami of the T7-L1 spinal nerves. These nerves innervate the anterolateral abdominal wall [
8]. TAP block, with the aid of liposomal bupivacaine—a local anesthetic that inhibits voltage gated sodium ion channels decreasing neuronal membrane permeability and preventing initiation and conduction of nerve impulses—has effectively reduced opioid analgesic consumption and improved post-operative pain control in a variety of surgical settings, including bariatric surgery [
9,
10]. Following on, similar benefits of TAP block may also be utilized in LLDN patients, who are ethically considered an extremely high risk of patients as they accept surgical, medical and pharmaceutical risks upon themselves to benefit someone else, and thus, require the highest possible safety standards. Besides the immediate local anesthetic effects of bupivacaine in a TAP block, the liposomal binding of the drug permits gradual and sustained release from multi-lamellar vesicles, minimizing its systemic toxicity [
11].
The objective of this retrospective review was to evaluate the efficacy and safety of TAP block with liposomal bupivacaine for opioid reduction and comparable analgesia, to serve as an alternate choice for patients undergoing LLDN.
2. Methods
2.1. Study Design
This was a single center, retrospective chart review of patients 18 years and older who underwent LLDN. The study protocol was approved by the Institutional Review Board at Yale New Haven Hospital.
Data were collected from January 2017 to May 2018. As part of our standard transplant practice, from January 2017 to June 2017, LLDN patients received hydromorphone-based patient-controlled analgesia (PCA) post-operatively and were transitioned to oral analgesics once they were able to tolerate oral medications, serving as the control group. In December 2017, our transplant center adopted the use of liposomal bupivacaine in TAP block as part of the default pain regimen for LLDN patients. Thus, our study group comprised of LLDN patients from December 2017 to May 2018 who received a pre-operative and pre-anesthesia TAP block with liposomal bupivacaine. During this time, optimization of non-opioids was also ensured, placing patients on acetaminophen 650 mg every six hours, ketorolac 15 mg every six hours for eight doses, and tramadol for breakthrough analgesia as needed. Registered nurses administered the pain intensity score ranging from zero to ten at a minimum of every six hours.
2.2. TAP Block with Liposomal Bupivacaine
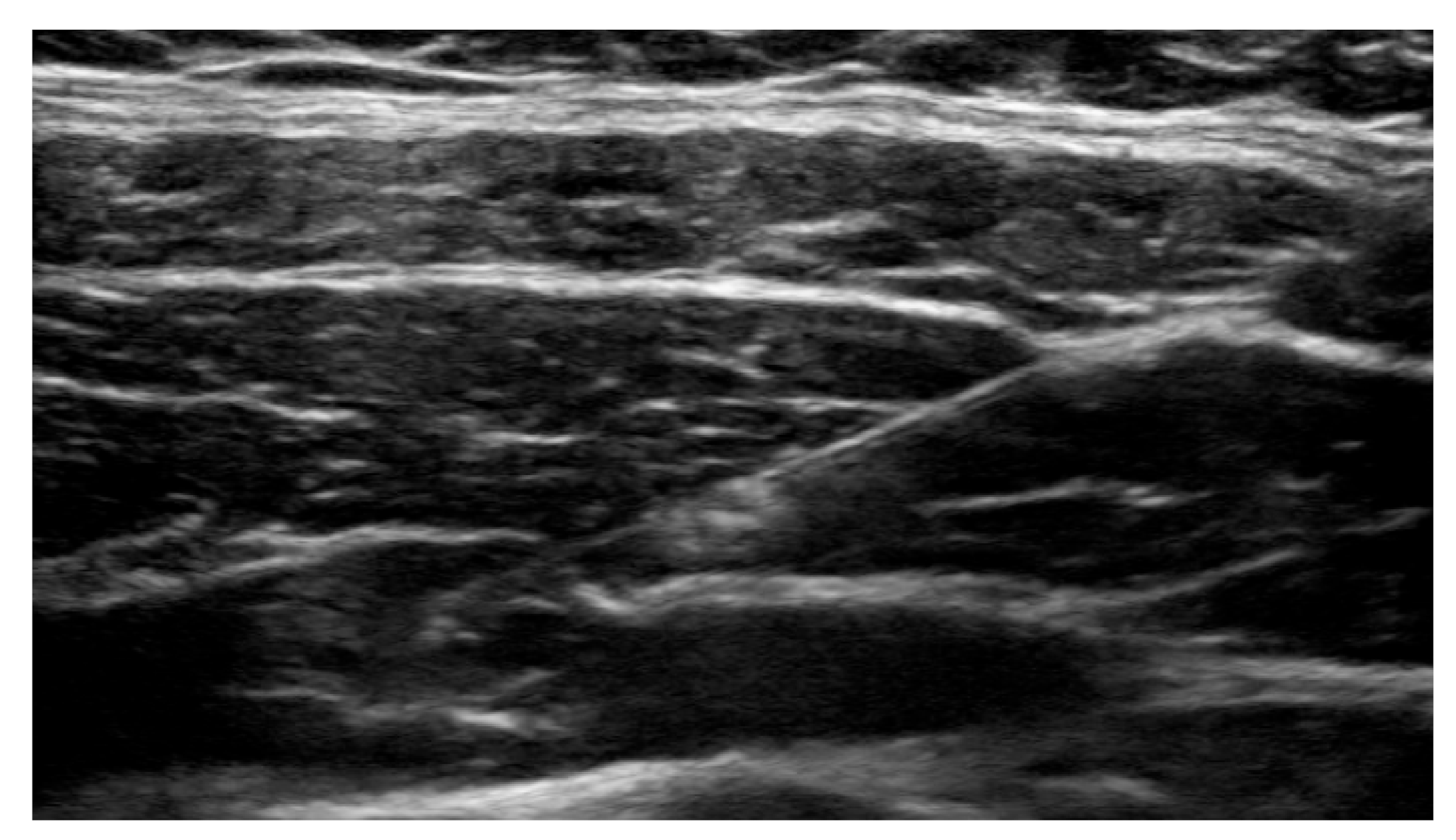
Anesthesiologists specializing in regional anesthesia, used an ultrasound guided 21-gauge needle to access the transversus abdominis plane. Once the position was confirmed, liposomal bupivacaine was administered, and appropriate spread of the medication was monitored and confirmed in real time. Ultrasound images of critical points were stored in the patient’s chart for future reference (
Figure 1).
The ultrasound image depicts a 21-gauge, 4 inch needle containing liposomal bupivacaine in the transversus abdominis plane adjacent to the nerve plexus.
2.3. Study Endpoints and Statistics
The primary endpoint was a reduction in post-operative opioid use in morphine milligram equivalents (MME). Secondary endpoints included: total opioid used (MME), post-operative pain scores, postoperative length of hospital stay, and re-hospitalizations. A Fisher’s exact test was used to compare categorical data and a student t-test was used to compare continuous data. A p-value of <0.05 was considered to be statistically significant.
3. Results
The study included a total of 66 patients with 33 in each group. Both groups were well matched on demographics including: age, body mass index, and race (
Table 1).
Post-operative opioid use was significantly lower (53.98 vs. 92.05 MME, p < 0.05) in the study group (patients who received TAP block) vs. the control group (patients who received opioid based PCA).
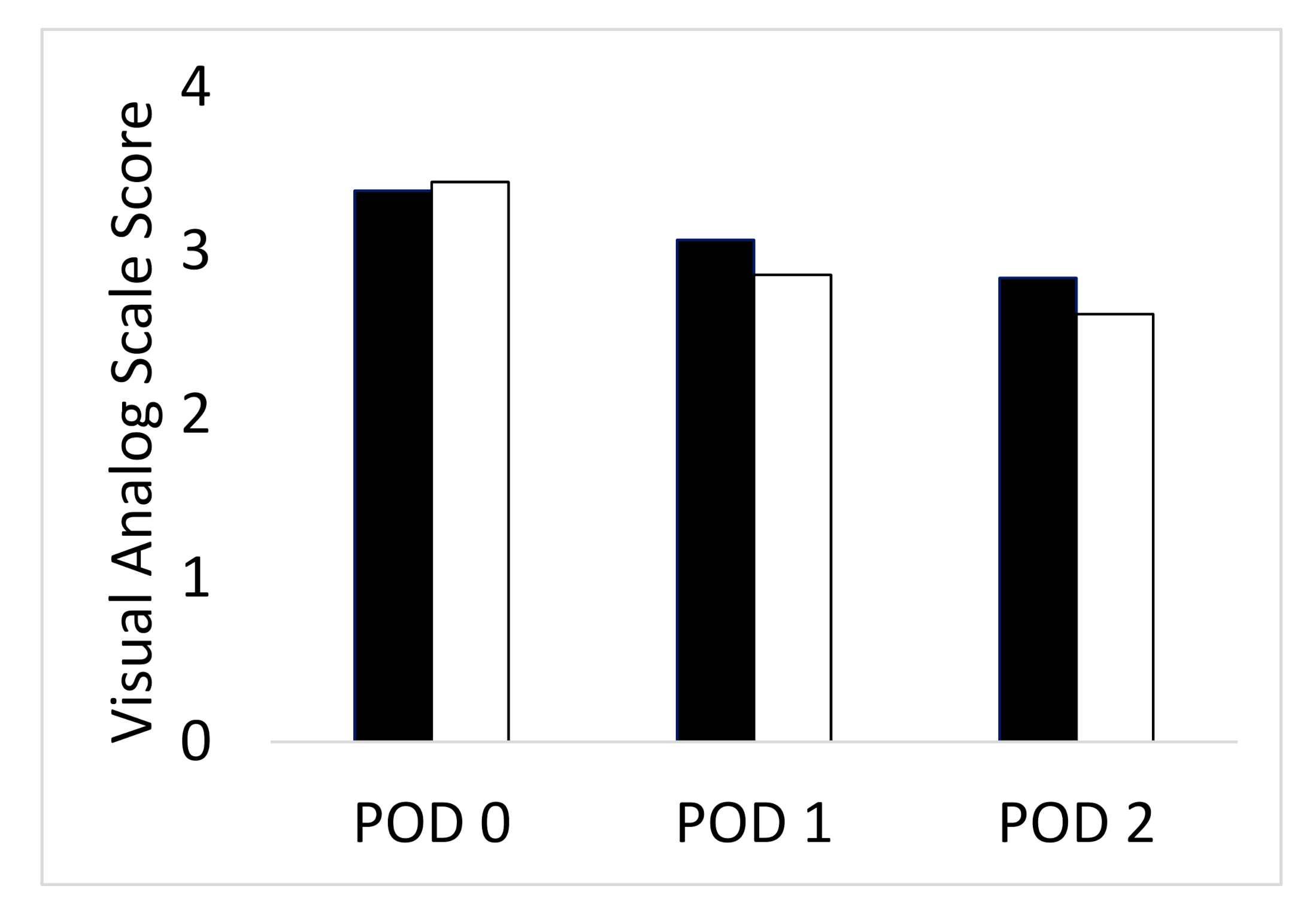
Mean postoperative pain scores were similar between the two groups, and this was the same for all postoperative days (Day 0–2) (
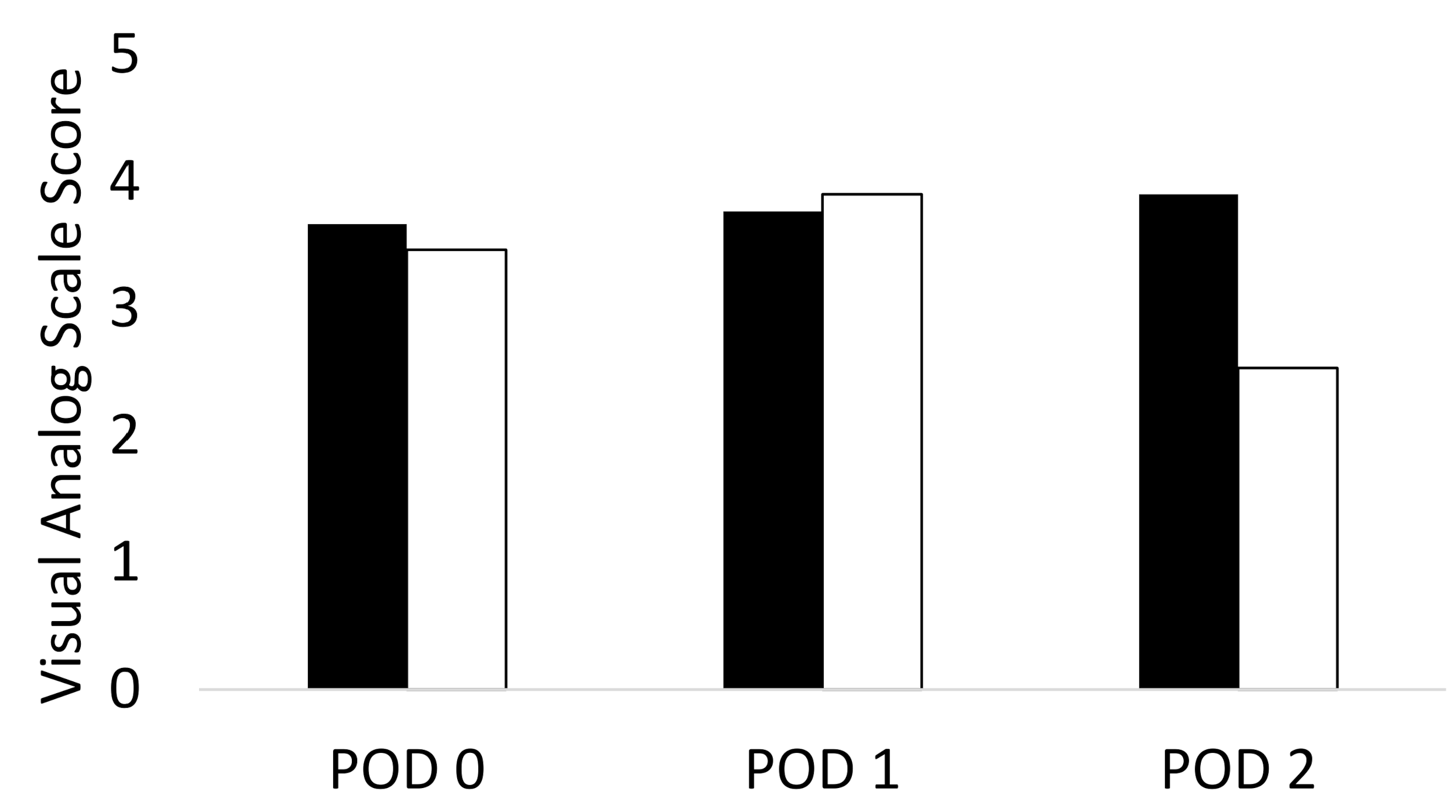
Figure 2). Furthermore, there was no significant difference in pain score variance (averaging the highest and lowest pain score per patient) on each post-operative day between the two groups (
Figure 3). The lack of peaks in pain score were also reassuring in suggesting good analgesic coverage in both groups.
This bar graph represents the average pain score on each post-operative day (POD), 0, 1 and 2, with the transversus abdominis plane (TAP) block compared to opioid based patient-controlled analgesia (PCA). There was no statistical significance on each POD between both groups.
This bar graph represents the average variance in pain score on each post-operative day for TAP block compared with opioid based PCA. Variance in pain score was calculated by taking the difference between the highest and lowest pain score on each day per patient and then averaging this and compared values between both groups. There was no statistical significance on each POD between both groups.
There was no significant difference in mean postoperative length of hospital stay between the two groups (3.12 ± 0.42 days vs. 3.3 ± 0.53 days, =0.13) (
Table 2). Two patients were re-admitted due to small bowel obstruction in the opioid PCA group within seven days of discharge, which was managed non-operatively. There were no adverse effects with the drug used in TAP block (liposomal bupivacaine) or the procedure itself.
Additionally, there was no significant difference in the change in serum creatinine from baseline to discharge (0.48 ± 0.16 mg/dL vs. 0.49 ± 0.16 mg/dL,
p = 0.938) or first week follow up visit in either group (0.44 ± 0.12 mg/dL vs. 0.40 ± 0.21,
p = 0.239), confirming no detrimental effects of TAP block on the residual kidney function in the donor (
Table 2).
4. Discussion
The primary objective of the study was to determine if TAP block with liposomal bupivacaine could safely reduce post-operative opioid use after LLDN and still achieve comparable postoperative analgesia. Our study concludes that TAP block significantly reduced postoperative opioid use, while achieving similar, efficacious and safe post-operative pain control.
Non-opioid analgesics represent a typical consideration in order to decrease opioid use, while providing enhanced postoperative pain management but with varying degrees of success. In cases of LLDNs, intravenous acetaminophen has failed to achieve a significant decrease in opioid use or pain control [
12]. On the other hand, non-steroidal anti-inflammatory drugs (NSAIDs), such as ketorolac, have shown to significantly decrease opioid consumption and also the length of hospital stay when compared to opioids alone [
13]. However, the use of NSAIDs, such as ketorolac, for more than five days has been associated with renal impairment and post-operative bleeding, both of which are painstakingly avoided in living kidney donors to protect the remnant kidney [
14,
15]. In our experience, the use of a TAP block with liposomal bupivacaine was able to decrease opioid use without any adverse events or complications from either the TAP block technique or the drug itself, while preserving remnant renal function.
Opioids have also been long associated with opioid induced bowel dysfunction due to activation of the µ-opioid receptors located in the gut wall in the myenteric plexus and submucosal plexus. Activation of these receptors inhibits peristaltic contractions while promoting delayed gastric emptying [
16]. By minimizing the use of opioids, many of these adverse events and complications can be avoided. In our study, two patients in our control group who received opioid based PCA were readmitted within seven days of discharge with symptoms of bowel obstruction and features of ileus due to opioids. Fortunately, this was managed non-operatively, however it underscores the potential hazards of opioid consumption this study hopes to avoid.
Several published studies have evaluated the use of TAP block with liposomal bupivacaine to reduce post-operative opioid use. In a retrospective study of patients undergoing laparoscopic sleeve gastrectomy and laparoscopic gastric bypass, there was a significant reduction in opioid use by 36 MME and 44 MME, respectively, by using TAP block [
9]. In another retrospective review of patients for bariatric surgery, there was a reduction by 44 MME when TAP block was used [
17]. Hutchins, et al. assessed this treatment option on living donor nephrectomies and found a significant decrease by 23 MME at 48–72 h with no difference at 0–24 h or 24–48 h [
18]. Our retrospective review on LLDN adds to the growing literature supporting the use of TAP block with a significant reduction of 38 MME.
It is noteworthy that on postoperative day 2, there was a significantly lower variation in pain scores per patient, thus favoring the TAP block group. This indicates a more stable and uniform analgesic spread with TAP block over opioid PCA. This, although a clinically significant and impactful finding, was not statistically significant due to the small cohort of patients (
Figure 3).
There are limitations to this study. The retrospective review limits the ability to control differences in pain management between groups. During the time that TAP block became part of the default pain regimen used at our institution, the hospital policy standardized supplemental analgesia for breakthrough pain, with use of acetaminophen and ketorolac for the inpatient hospital stay, increasing its use and consequently making it difficult to exclude their impact on either group’s analgesic spread. Additionally, unmeasured characteristics of patients that may affect the perception and management of post-operative pain may have confounded the results.
5. Conclusions
Multimodality pain management including TAP block with liposomal bupivacaine provides effective and safe analgesia when compared to the use of hydromorphone PCA, significantly reducing the amount of opioids required in LLDN patients. Future prospective randomized studies will help eliminate the weaknesses of this retrospective study.
Author Contributions
V.D., E.C., D.J.H., R.K.B., and R.D. developed the project. V.D. researched data, and wrote the manuscript. All authors contributed to the discussion, and reviewed/edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This study was not funded by any organization.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Yale New Haven Hospital (protocol code 2000022643 and date of approval—8 March 2018).
Informed Consent Statement
Patient consent was waived due to retrospective nature of the review.
Conflicts of Interest
The authors declare no conflict of interest relevant to this study.
References
- National Data. OPTN. Available online: https://optn.transplant.hrsa.gov/data/view-data-reports/national-data/# (accessed on 22 February 2021).
- Ratner, L.E.; Ciseck, L.J.; Moore, R.G.; Cigarroa, F.G.; Kaufman, H.S.; Kavoussi, L.R. Laparoscopic live donor nephrectomy. Transplantation 1995, 60, 1047–1049. [Google Scholar]
- Wilson, C.H.; Sanni, A.; Rix, D.A.; Soomro, N.A. Laparoscopic versus open nephrectomy for live kidney donors. Cochrane Database Syst. Rev. 2011, 11, CD006124. [Google Scholar] [CrossRef] [PubMed]
- Matas, A.J.; Bartlett, S.T.; Leichtman, A.B.; Delmonico, F.L. Morbidity and mortality after living kidney donation, 1999-2001: Survey of United States transplant centers. Am. J. Transplant. 2003, 3, 830–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute on Drug Abuse. Opioid Overdose Crisis. NIDA. Available online: https://www.drugabuse.gov/drugs-abuse/opioids/opioid-overdose-crisis (accessed on 12 June 2019).
- Benyamin, R.; Trescot, A.; Datta, S.; Buenaventura, R.; Adlaka, R.; Sehgal, N.; Glaser, S.E.; Vallejo, R. Opioid complications and side effects. Pain Physician 2008, 11 (Suppl. 2), S105–S120. [Google Scholar] [PubMed]
- Sinatra, R. Causes and consequences of inadequate management of acute pain. Pain Med. 2010, 11, 1859–1871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukhtar, K. Transversus abdominis plane (TAP) block. NYSORA 2009, 12, 28–33. [Google Scholar]
- Moon, R.C.; Lastrapes, L.; Wier, J.; Nakajima, M.; Gaskins, W.; Teixeira, A.F.; Moon, R.C. Preoperative Transversus Abdominis Plane (TAP) Block with Liposomal Bupivacaine for Bariatric Patients to Reduce the Use of Opioid Analgesics. Obes. Surg. 2019, 29, 1099–1104. [Google Scholar] [CrossRef]
- Robertson, T.C.; Hall, K.; Bear, S.; Thompson, K.J.; Kuwada, T.; Gersin, K.S. Transversus abdominis block utilizing liposomal bupivacaine as a non-opioid analgesic for postoperative pain management. Surg. Endosc. 2018, 33, 2657–2662. [Google Scholar] [CrossRef]
- Malik, O.; Kaye, A.D.; Kaye, A.; Belani, K.; Urman, R.D. Emerging roles of liposomal bupivacaine in anesthesia practice. J. Anaesthesiol. Clin. Pharmacol. 2017, 33, 151–156. [Google Scholar] [PubMed]
- Vu, V.; Baker, W.L.; Tencza, E.M.; Rochon, C.; Sheiner, P.A.; Martin, S.T. Intravenous Acetaminophen for Postoperative Pain Management in Patients Undergoing Living Laparoscopic Living-Donor Nephrectomy. Ann. Pharm. 2017, 51, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Campsen, J.; Call, T.; Allen, C.M.; Presson, A.P.; Martinez, E.; Rofaiel, G.; Kim, R.D. Prospective, double-blind, randomized clinical trial comparing an ERAS pathway with ketorolac and pregabalin versus standard of care plus placebo during live donor nephrectomy for kidney transplant. Am. J. Transpl. 2019, 19, 1777–1781. [Google Scholar] [CrossRef] [PubMed]
- Feldman, H.I.; Kinman, J.L.; Berlin, J.A.; Hennessy, S.; Kimmel, S.E.; Farrar, J.; Carson, J.L.; Strom, B.L. Parenteral ketorolac: The risk for acute renal failure. Ann. Intern. Med. 1997, 126, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Strom, B.L.; Berlin, J.A.; Kinman, J.L.; Spitz, P.W.; Hennessy, S.; Feldman, H.; Kimmel, S.; Carson, J.L. Parenteral ketorolac and risk of gastrointestinal and operative site bleeding. A postmarketing surveillance study. JAMA 1996, 275, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Leppert, W. The impact of opioid analgesics on the gastrointestinal tract function and the current management possibilities. Contemp. Oncol. (Pozn) 2012, 16, 125–131. [Google Scholar]
- Bhakta, A.; Glotzer, O.; Ata, A.; Tafen, M.; Stain, S.C.; Singh, P.T. Analgesic efficacy of laparoscopic-guided transverse abdominis plane block using liposomal bupivacaine in bariatric surgery. Am. J. Surg. 2018, 215, 643–646. [Google Scholar] [CrossRef]
- Hutchins, J.L.; Kesha, R.; Blanco, F.; Dunn, T.; Hochhalter, R. Ultrasound-guided subcostal transversus abdominis plane blocks with liposomal bupivacaine vs. non-liposomal bupivacaine for postoperative pain control after laparoscopic hand-assisted donor nephrectomy: A prospective randomised observer-blinded study. Anaesthesia 2016, 71, 930–937. [Google Scholar] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).


 ,
, 



{kind=link}
{kind=link}
{kind=link}