
Donor-Derived Cell-Free DNA to Diagnose Graft Rejection Post-Transplant: Past, Present and Future

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
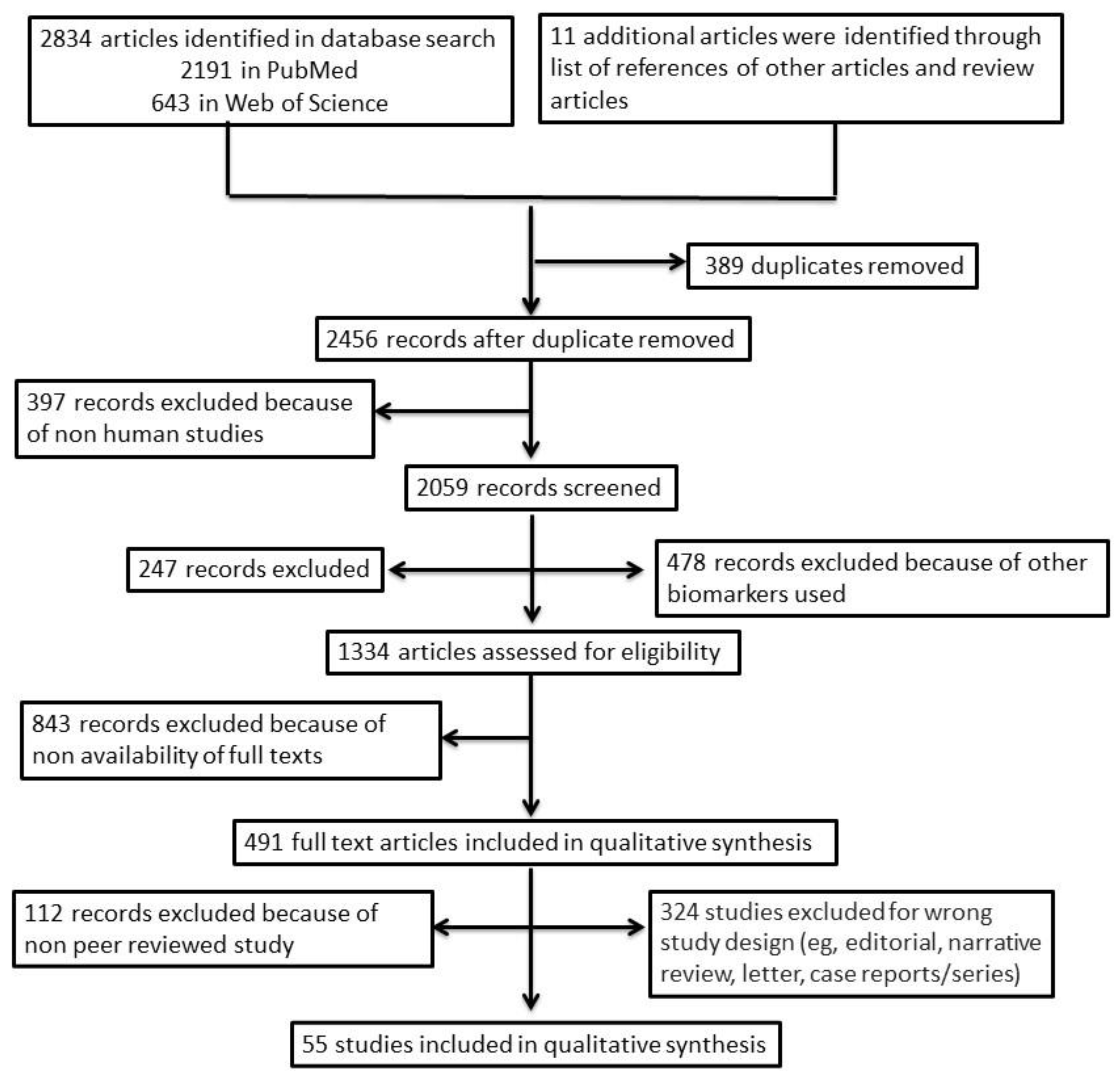
2.1. Search Strategy
2.2. Study Selection
3. Evolution of Analytical Approaches and Techniques to Diagnose Graft Rejection Using dd-cfDNA
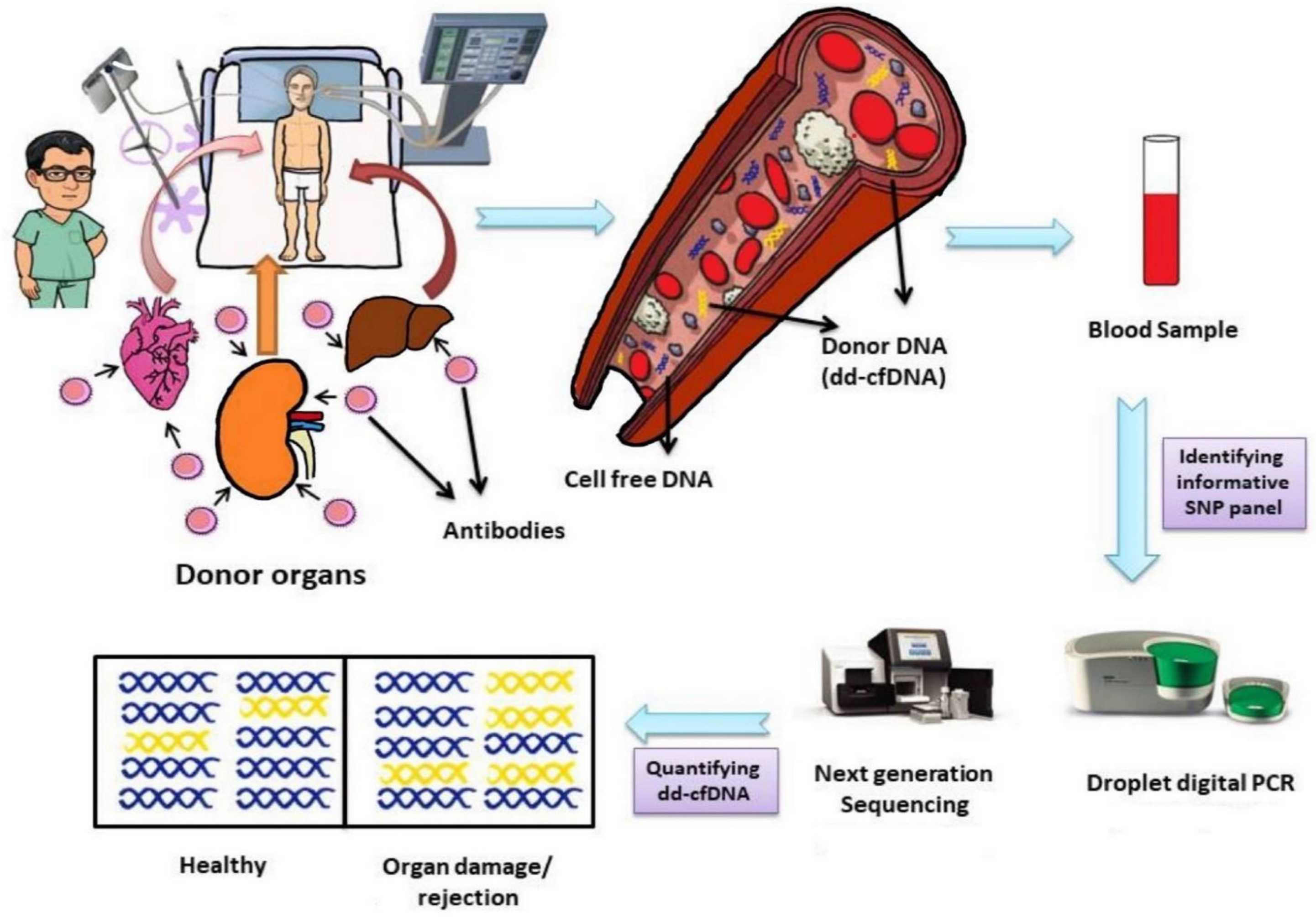
4. The dd-cfDNA as a Potential Biomarker
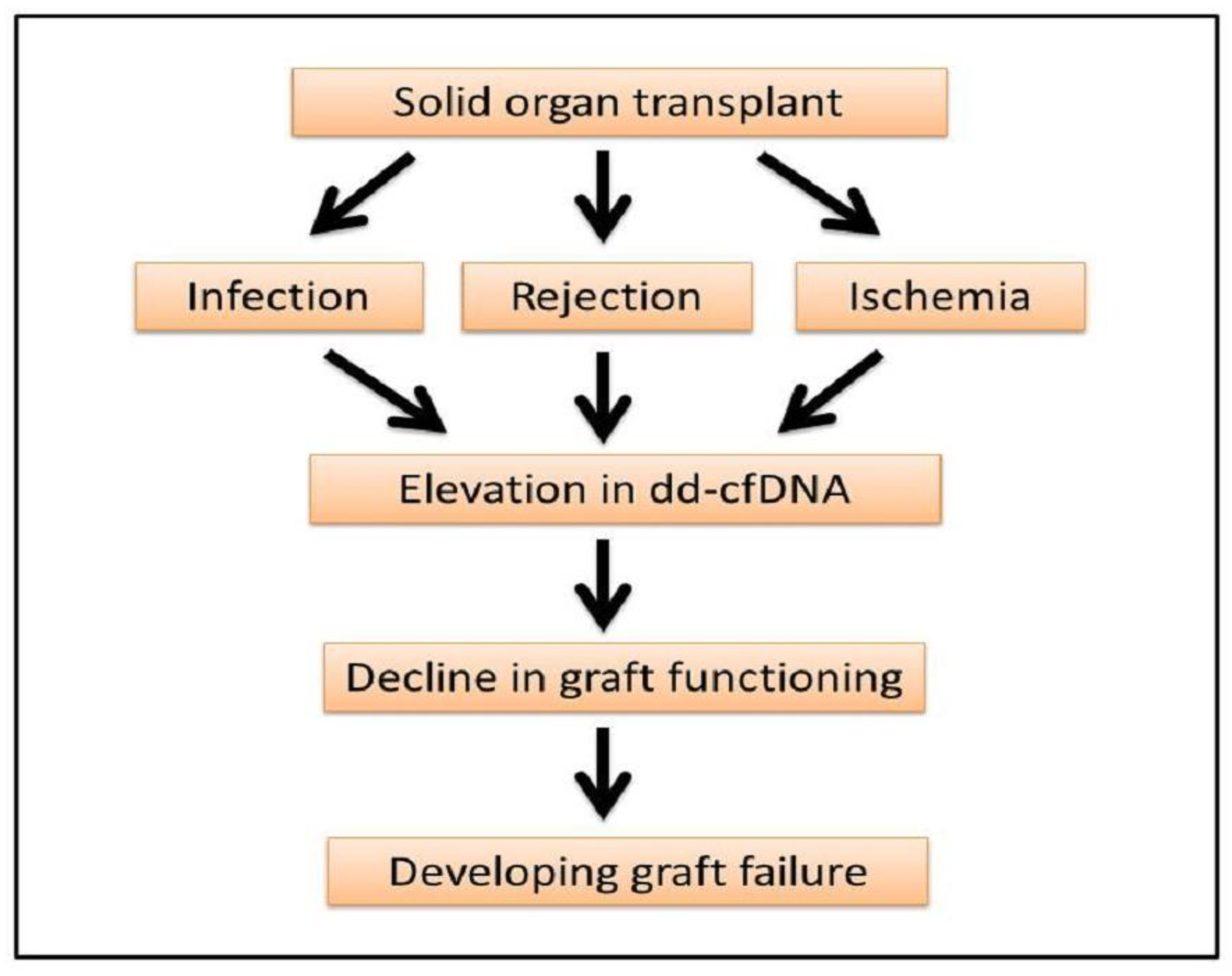
5. Monitoring of Organ Damage and Rejection through dd-cfDNA
6. Limitations of dd-cfDNA as a Potential Biomarker
7. Conclusions
8. Future Prospect of dd-cfDNA
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Observatory on Donation and Transplantation. Available online: http://www.transplant-observatory.org/data-charts-and-tables/ (accessed on 27 February 2021).
- Beck, J.; Oellerich, M.; Schutz, E. A New Universal Multiplex Digital PCR Method with Improve Precision for the Quantification of Donor Derived graft cfDNA Traces. Available online: http://chronixbiomedical.com/wp-content/uploads/2018/08/transplant-Beck-AACC-2015-2-copy.pdf (accessed on 20 March 2020).
- Schütz, E.; Fischer, A.; Beck, J.; Harden, M.; Koch, M.; Wuensch, T.; Stockmann, M.; Nashan, B.; Kollmar, O.; Matthaei, J.; et al. Graft-derived cell-free DNA, a noninvasive early rejection and graft damage marker in liver transplantation: A prospective, observational, multicenter cohort study. PLoS Med. 2017, 14, e1002286. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.Y.; Sarwal, R.D.; Sigdel, T.K.; Damm, I.; Rosenbaum, B.; Liberto, J.M.; Chan-On, C.; Arreola-Guerra, J.M.; Alberu, J.; Vincenti, F.; et al. A urine score for non-invasive accurate diagnosis and prediction of kidney transplant rejection. Sci. Transl. Med. 2020, 12, eaba2501. [Google Scholar] [CrossRef]
- Alraies, M.C.; Eckman, P. Adult heart transplant: Indications and outcomes. J. Thorac. Dis. 2014, 6, 1120. [Google Scholar] [PubMed]
- National Kidney Foundation. Steps to Keep Your Transplanted Kidney. Available online: https://www.kidney.org/atoz/content/keepyourtransplantedkidney (accessed on 2 January 2021).
- Mayo Clinic. Liver Transplant. Available online: https://www.mayoclinic.org/tests-procedures/liver-transplant/about/pac-20384842 (accessed on 24 December 2020).
- National Kidney Foundation. Dialysis. Available online: https://www.kidney.org/atoz/content/dialysisinfo/ (accessed on 30 October 2020).
- Russo, M.J.; Rana, A.; Chen, J.M.; Hong, K.N.; Gelijns, A.; Moskowitz, A.; Widmann, W.D.; Ratner, L.; Naka, Y.; Hardy, M.A. Pretransplantation patient characteristics and survival following combined heart and kidney transplantation: An analysis of the United Network for Organ Sharing Database. Arch. Surg. 2009, 144, 241–246. [Google Scholar] [CrossRef] [Green Version]
- Russo, M.J.; Chen, J.M.; Hong, K.N.; Stewart, A.S.; Ascheim, D.D.; Argenziano, M.; Mancini, D.M.; Oz, M.C.; Naka, Y. Columbia University Heart Transplant Outcomes Research Group. Survival after heart transplantation is not diminished among recipients with uncomplicated diabetes mellitus. Circulation 2006, 114, 2280–2287. [Google Scholar] [CrossRef] [Green Version]
- Russo, M.J.; Davies, R.R.; Sorabella, R.A.; Martens, T.P.; George, I.; Cheema, F.H.; Mital, S.; Mosca, R.S.; Chen, J.M. Adult-age donors offer acceptable long-term survival to pediatric heart transplant recipients: An analysis of the United Network of Organ Sharing database. J. Thorac. Cardiovasc. Surg. 2006, 132, 1208–1212. [Google Scholar] [CrossRef] [Green Version]
- Chu, K.K.; Chan, S.C.; Sharr, W.W.; Chok, K.S.; Dai, W.C.; Lo, C.M. Low-volume deceased donor liver transplantation alongside a strong living donor liver transplantation service. World J. Surg. 2014, 38, 1522–1528. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.D.; Hayashi, P.H.; Barritt, A. Liver transplantation in 2013: Challenges and controversies. Minerva Gastroenterol. 2013, 59, 117–131. [Google Scholar]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Benjamin, O.; Lappin, S.L. End-stage renal disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA. Available online: https://www.ncbi.nlm.nih.gov/books/NBK499861/ (accessed on 25 March 2020).
- Bui, A.L.; Horwich, T.B.; Fonarow, G.C. Epidemiology and risk profile of heart failure. Nat. Rev. Cardiol. 2011, 8, 30. [Google Scholar] [CrossRef] [Green Version]
- Roger, V.L.; Weston, S.A.; Redfield, M.M.; Hellermann-Homan, J.P.; Killian, J.; Yawn, B.P.; Jacobsen, S.J. Trends in heart failure incidence and survival in a community-based population. JAMA 2004, 292, 344–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart disease and stroke statistics—2013 update: A report from the American Heart Association. Circulation 2013, 127, e6–e245. [Google Scholar] [CrossRef]
- Sepanlou, S.G.; Safiri, S.; Bisignano, C.; Ikuta, K.S.; Merat, S.; Saberifiroozi, M.; Poustchi, H.; Tsoi, D.; Colombara, D.V.; Abdoli, A.; et al. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 245–266. [Google Scholar] [CrossRef] [Green Version]
- Starzl, T.E.; Putnam, C.W. Experience in Hepatic Transplantation; WB Saunders Company: Philadelphia, PA, USA, 1969. [Google Scholar]
- Iwalrl, Y.; Starzl, T.E.; Yagihashi, A. Replacement of donor lymphoid tissue in human small bowel transplants under FK 506 immunosuppression. Lancet 1991, 337, 818. [Google Scholar]
- Startzl, T.E.; Dimetris, A.J.; Trucco, M. Chimerism and donorspecific nonreactivity 27–29 years after kidney transplantation. Transplantation 1993, 55, 1272–1277. [Google Scholar] [CrossRef] [Green Version]
- Fung, J.J.; Zeevi, A.; Kaufman, C.; Paradis, I.L.; Dauber, J.H.; Hardesty, R.L.; Griffith, B.; Duquesnoy, R.J. Interactions between bronchoalveolar lymphocytes and macrophages in heart-lung transplant recipients. Hum. Immunol. 1985, 14, 287–294. [Google Scholar] [CrossRef]
- Demtris, A.J.; Murase, N.; Starzl, T.E. Donor dendritic cells in graft and host lymphoid and non-lymphoid tissues after liver and heart allotransplantation under short term immunosuppression. Lancet 1992, 339, 1610. [Google Scholar] [CrossRef] [Green Version]
- Valdivia, L.A.; Demetris, A.J.; Langer, A.M.; Celli, S.; Fung, J.J.; Starzl, T.E. Dendritic cell replacement in long-surviving liver and cardiac xenografts. Transplantation 1993, 56, 482. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Tong, K.L.; Li, P.K.; Chan, A.Y.; Yeung, C.K.; Pang, C.C.; Wong, T.Y.; Lee, K.C.; Lo, Y.D. Presence of donor-and recipient-derived DNA in cell-free urine samples of renal transplantation recipients: Urinary DNA chimerism. Clin. Chem. 1999, 45, 1741–1746. [Google Scholar] [CrossRef]
- García Moreira, V.; Prieto García, B.; Baltar Martín, J.M.; Ortega Suárez, F.; Alvarez, F.V. Cell-free DNA as a noninvasive acute rejection marker in renal transplantation. Clin. Chem. 2009, 55, 1958–1966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macher, H.C.; Suárez-Artacho, G.; Guerrero, J.M.; Gómez-Bravo, M.A.; Álvarez-Gómez, S.; Bernal-Bellido, C.; Dominguez-Pascual, I.; Rubio, A. Monitoring of transplanted liver health by quantification of organ-specific genomic marker in circulating DNA from receptor. PLoS ONE 2014, 9, e113987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigdel, T.K.; Vitalone, M.J.; Tran, T.Q.; Dai, H.; Hsieh, S.C.; Salvatierra, O.; Sarwal, M.M. A rapid noninvasive assay for the detection of renal transplant injury. Transplantation 2013, 96, 97. [Google Scholar] [CrossRef] [Green Version]
- Snyder, T.M.; Khush, K.K.; Valantine, H.A.; Quake, S.R. Universal noninvasive detection of solid organ transplant rejection. Proc. Natl. Acad. Sci. USA 2011, 108, 6229–6234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, J.; Oellerich, M.; Schütz, E. A Universal Droplet Digital PCR Approach for Monitoring of Graft Health after Transplantation Using a Preselected SNP Set; Digital PCR; Humana Press: New York, NY, USA, 2018; pp. 335–348. [Google Scholar]
- Beck, J.; Bierau, S.; Balzer, S.; Andag, R.; Kanzow, P.; Schmitz, J.; Gaedcke, J.; Moerer, O.; Slotta, J.E.; Walson, P.; et al. Digital droplet PCR for rapid quantification of donor DNA in the circulation of transplant recipients as a potential universal biomarker of graft injury. Clin. Chem. 2013, 59, 1732–1741. [Google Scholar] [CrossRef] [Green Version]
- Grskovic, M.; Hiller, D.J.; Eubank, L.A.; Sninsky, J.J.; Christopherson, C.; Collins, J.P.; Thompson, K.; Song, M.; Wang, Y.S.; Ross, D.; et al. Validation of a clinical-grade assay to measure donor-derived cell-free DNA in solid organ transplant recipients. J. Mol. Diagn. 2016, 18, 890–902. [Google Scholar] [CrossRef] [Green Version]
- Weir, M.; Hiller, D.; Yee, J.; Matas, A. Donor-derived cell-free DNA outperforms serum creatinine changes for identifying kidney transplant rejection. Am. J. Transplant. 2018, 18 (Suppl. 4), 506. [Google Scholar]
- Consortium, G.P. A global reference for human genetic variation. Nature 2015, 526, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Grskovic, M.; Hiller, D.J.; Eubank, L.A.; Sninsky, J.J.; Christopherson, C.; Collins, J.P.; Thompson, K.; Song, M.; Wang, Y.S.; Ross, D.; et al. Circulating cell-free DNA enables noninvasive diagnosis of heart transplant rejection. Sci. Transl. Med. 2014, 6, 241ra77. [Google Scholar]
- De Vlaminck, I.; Martin, L.; Kertesz, M.; Patel, K.; Kowarsky, M.; Strehl, C.; Cohen, G.; Luikart, H.; Neff, N.F.; Okamoto, J.; et al. Noninvasive monitoring of infection and rejection after lung transplantation. Proc. Natl. Acad. Sci. USA 2015, 112, 13336–13341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, J.; Oellerich, M.; Schulz, U.; Schauerte, V.; Reinhard, L.; Fuchs, U.; Knabbe, C.; Zittermann, A.; Olbricht, C.; Gummert, J.F.; et al. Donor-derived cell-free DNA is a novel universal biomarker for allograft rejection in solid organ transplantation. Transplant. Proc. 2015, 47, 2400–2403. [Google Scholar] [CrossRef] [PubMed]
- Burnham, P.; Kim, M.S.; Agbor-Enoh, S.; Luikart, H.; Valantine, H.A.; Khush, K.K.; De Vlaminck, I. Single-stranded DNA library preparation uncovers the origin and diversity of ultrashort cell-free DNA in plasma. Sci. Rep. 2016, 6, 1–9. [Google Scholar]
- Macher, H.C.; Suárez-Artacho, G.; Jiménez-Arriscado, P.; Álvarez-Gómez, S.; García-Fernández, N.; Guerrero, J.M.; Molinero, P.; Trujillo-Arribas, E.; Gómez-Bravo, M.A.; Rubio, A. Evaluation of the state of transplanted liver health by monitoring of organ-specific genomic marker in circulating DNA from receptor. Adv. Exp. Med. Biol. 2016, 924, 113–116. [Google Scholar] [PubMed]
- Schutz, E.; Blum, A.; Beck, J.; Harden, M.; Koch, M.; Wuensch, T.; Stockmann, M.; Nashan, B.; Kollmar, O.; Matthaei, J.; et al. Graft-derived cell-free DNA-a promising rejection marker in liver transplantation-results from a prospective multicenter trial. Clin. Chem. 2016, 62, S41. [Google Scholar]
- Zou, J.; Duffy, B.; Slade, M.; Young, A.L.; Steward, N.; Hachem, R.; Mohanakumar, T. Rapid detection of donor cell-free DNA in lung transplant recipients with rejections using donor-recipient HLA mismatch. Hum. Immunol. 2017, 78, 342–349. [Google Scholar] [CrossRef] [Green Version]
- Bromberg, J.S.; Brennan, D.C.; Poggio, E.; Bunnapradist, S.; Langone, A.; Sood, P.; Matas, A.J.; Mannon, R.B.; Mehta, S.; Sharfuddin, A.; et al. Biological variation of donor-derived cell-free DNA in renal transplant recipients: Clinical implications. J. Appl. Lab. Med. 2017, 2, 309–321. [Google Scholar] [CrossRef] [Green Version]
- Goh, S.K.; Muralidharan, V.; Christophi, C.; Do, H.; Dobrovic, A. Probe-free digital PCR quantitative methodology to measure donor-specific cell-free DNA after solid-organ transplantation. Clin. Chem. 2017, 63, 742–750. [Google Scholar] [CrossRef] [Green Version]
- Bloom, R.D.; Bromberg, J.S.; Poggio, E.D.; Bunnapradist, S.; Langone, A.J.; Sood, P.; Matas, A.J.; Mehta, S.; Mannon, R.B.; Sharfuddin, A.; et al. Cell-free DNA and active rejection in kidney allografts. J. Am. Soc. Nephrol. 2017, 28, 2221–2232. [Google Scholar] [CrossRef]
- Tanaka, S.; Sugimoto, S.; Kurosaki, T.; Miyoshi, K.; Otani, S.; Suzawa, K.; Hashida, S.; Yamane, M.; Oto, T.; Toyooka, S. Donor-derived cell-free DNA is associated with acute rejection and decreased oxygenation in primary graft dysfunction after living donor-lobar lung transplantation. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef]
- Jordan, S.C.; Bunnapradist, S.; Bromberg, J.S.; Langone, A.J.; Hiller, D.; Yee, J.P.; Sninsky, J.J.; Woodward, R.N.; Matas, A.J. Donor-derived cell-free DNA identifies antibody-mediated rejection in donor specific antibody positive kidney transplant recipients. Transplant. Direct. 2018, 4, e379. [Google Scholar] [CrossRef]
- Gielis, E.M.; Beirnaert, C.; Dendooven, A.; Meysman, P.; Laukens, K.; De Schrijver, J.; Van Laecke, S.; Van Biesen, W.; Emonds, M.P.; De Winter, B.Y.; et al. Plasma donor-derived cell-free DNA kinetics after kidney transplantation using a single tube multiplex PCR assay. PLoS ONE 2018, 13, e0208207. [Google Scholar]
- Goh, S.K.; Do, H.; Testro, A.; Pavlovic, J.; Vago, A.; Lokan, J.; Jones, R.M.; Christophi, C.; Dobrovic, A.; Muralidharan, V. The measurement of donor-specific cell-free DNA identifies recipients with biopsy-proven acute rejection requiring treatment after liver transplantation. Transplant. Direct. 2019, 5, e462. [Google Scholar] [CrossRef]
- Khush, K.K.; Patel, J.; Pinney, S.; Kao, A.; Alharethi, R.; DePasquale, E.; Ewald, G.; Berman, P.; Kanwar, M.; Hiller, D.; et al. Noninvasive detection of graft injury after heart transplant using donor-derived cell-free DNA: A prospective multicenter study. Am. J. Transplant. 2019, 19, 2889–2899. [Google Scholar] [CrossRef] [Green Version]
- Altuğ, Y.; Liang, N.; Ram, R.; Ravi, H.; Ahmed, E.; Brevnov, M.; Swenerton, R.K.; Zimmermann, B.; Malhotra, M.; Demko, Z.P.; et al. Analytical validation of a single-nucleotide polymorphism-based donor-derived cell-free DNA assay for detecting rejection in kidney transplant patients. Transplantation 2019, 103, 2657. [Google Scholar] [CrossRef] [Green Version]
- Sigdel, T.K.; Archila, F.A.; Constantin, T.; Prins, S.A.; Liberto, J.; Damm, I.; Towfighi, P.; Navarro, S.; Kirkizlar, E.; Demko, Z.P.; et al. Optimizing detection of kidney transplant injury by assessment of donor-derived cell-free DNA via massively multiplex PCR. J. Clin. Med. 2019, 8, 19. [Google Scholar] [CrossRef] [Green Version]
- Oellerich, M.; Shipkova, M.; Asendorf, T.; Walson, P.D.; Schauerte, V.; Mettenmeyer, N.; Kabakchiev, M.; Hasche, G.; Gröne, H.J.; Friede, T.; et al. Absolute quantification of donor-derived cell-free DNA as a marker of rejection and graft injury in kidney transplantation: Results from a prospective observational study. Am. J. Transplant. 2019, 19, 3087–3099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sayah, D.; Weigt, S.S.; Ramsey, A.; Ardehali, A.; Golden, J.; Ross, D.J. Plasma Donor-derived Cell-free DNA Levels Are Increased During Acute Cellular Rejection After Lung Transplant: Pilot Data. Transplant. Direct. 2020, 6, e608. [Google Scholar] [CrossRef]
- Potter, S.R.; Hinojosa, R.; Miles, C.D.; O’brien, D.; Ross, D.J. Remote monitoring using donor-derived, cell-free DNA after kidney transplantation during the coronavirus disease 2019 pandemic. Kidney Res. Clin. Pract. 2020, 39, 495. [Google Scholar] [CrossRef]
- Schütz, E.; Asendorf, T.; Beck, J.; Schauerte, V.; Mettenmeyer, N.; Shipkova, M.; Wieland, E.; Kabakchiev, M.; Walson, P.D.; Schwenger, V.; et al. Time-dependent apparent increase in dd-cfDNA percentage in clinically stable patients between one and five years following kidney transplantation. Clin. Chem. 2020, 66, 1290–1299. [Google Scholar] [CrossRef]
- Shen, J.; Guo, L.; Yan, P.; Zhou, J.; Zhou, Q.; Lei, W.; Liu, H.; Liu, G.; Lv, J.; Liu, F.; et al. Prognostic value of the donor-derived cell-free DNA assay in acute renal rejection therapy: A prospective cohort study. Clin. Transplant. 2020, 34, e14053. [Google Scholar] [CrossRef]
- Puliyanda, D.P.; Swinford, R.; Pizzo, H.; Garrison, J.; De Golovine, A.M.; Jordan, S.C. Donor-derived cell-free DNA (dd-cfDNA) for detection of allograft rejection in pediatric kidney transplants. Pediatric Transplant. 2020, 25, e13850. [Google Scholar]
- Stites, E.; Kumar, D.; Olaitan, O.; John Swanson, S.; Leca, N.; Weir, M.; Bromberg, J.; Melancon, J.; Agha, I.; Fattah, H.; et al. High levels of dd-cfDNA identify patients with TCMR 1A and borderline allograft rejection at increased risk of graft injury. Am. J. Transplant. 2020, 20, 2491–2498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khush, K.K.; De Vlaminck, I.; Luikart, H.; Ross, D.J.; Nicolls, M.R. Donor-derived, cell-free DNA levels by next-generation targeted sequencing are increased in allograft rejection after lung transplantation. ERJ Open Res. 2021, 7, 00462-2020. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Vaitla, P.; Craici, I.M.; Thongprayoon, C.; Vaitla, P.; Craici, I.M.; Leeaphorn, N.; Hansrivijit, P.; Salim, S.A.; Bathini, T.; et al. The use of donor-derived cell-free DNA for assessment of allograft rejection and injury status. J Clin. Med. 2020, 9, 1480. [Google Scholar] [CrossRef]
- Bronkhorst, A.J.; Ungerer, V.; Holdenrieder, S. The emerging role of cell-free DNA as a molecular marker for cancer management. Biomol. Detect. Quantif. 2019, 17, 100087. [Google Scholar] [CrossRef]
- Diehl, F.; Schmidt, K.; Choti, M.A.; Romans, K.; Goodman, S.; Li, M.; Thornton, K.; Agrawal, N.; Sokoll, L.; Szabo, S.A.; et al. Circulating mutant DNA to assess tumor dynamics. Nat. Med. 2008, 14, 985–990. [Google Scholar] [CrossRef]
- Alekseeva, L.A.; Mironova, N.L.; Brenner, E.V.; Kurilshikov, A.M.; Patutina, O.A.; Zenkova, M.A. Alteration of the exDNA profile in blood serum of LLC-bearing mice under the decrease of tumour invasion potential by bovine pancreatic DNase I treatment. PLoS ONE 2017, 12, e0171988. [Google Scholar]
- Yu, S.C.; Lee, S.W.; Jiang, P.; Leung, T.Y.; Chan, K.A.; Chiu, R.W.; Lo, Y.D. High-resolution profiling of fetal DNA clearance from maternal plasma by massively parallel sequencing. Clin. Chem. 2013, 59, 1228–1237. [Google Scholar] [CrossRef] [Green Version]
- Gounden, V.; Bhatt, H.; Jialal, I. Renal function tests. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2018. [Google Scholar]
- Wilkinson, A. Protocol transplant biopsies: Are they really needed? Clin. J. Am. Soc. Nephrol. 2006, 1, 130–137. [Google Scholar] [CrossRef] [Green Version]
- Berl, T. American Society of Nephrology renal research report. J. Am. Soc. Nephrol. 2005, 16, 1886–1903. [Google Scholar]
- Rush, D.; Arlen, D.; Boucher, A.; Busque, S.; Cockfield, S.M.; Girardin, C.; Knoll, G.; Lachance, J.G.; Landsberg, D.; Shapiro, J.; et al. Lack of benefit of early protocol biopsies in renal transplant patients receiving TAC and MMF: A randomized study. Am. J. Transplant. 2007, 7, 2538–2545. [Google Scholar] [CrossRef] [PubMed]
- Gadi, V.K.; Nelson, J.L.; Boespflug, N.D.; Guthrie, K.A.; Kuhr, C.S. Soluble donor DNA concentrations in recipient serum correlate with pancreas-kidney rejection. Clin. Chem. 2006, 52, 379–382. [Google Scholar] [CrossRef] [Green Version]
- Mehta, S.G.; Chang, J.H.; Alhamad, T.; Bromberg, J.S.; Hiller, D.J.; Grskovic, M.; Yee, J.P.; Mannon, R.B. Repeat kidney transplant recipients with active rejection have increased donor-derived cell-free DNA. Am. J. Transplant. 2019, 19, 1597. [Google Scholar] [CrossRef]
- Gordon, P.M.; Khan, A.; Sajid, U.; Chang, N.; Suresh, V.; Dimnik, L.; Lamont, R.E.; Parboosingh, J.S.; Martin, S.R.; Pon, R.T.; et al. An algorithm measuring donor cell-free DNA in plasma of cellular and solid organ transplant recipients that does not require donor or recipient genotyping. Front. Cardiovasc. Med. 2016, 22, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, D.J.; Ross, D.J.; Sako, E. Single Center “Snapshot” Experience With Donor-Derived Cell-Free DNA after Lung Transplantation. Biomark. Insights 2020, 15, 1177271920958704. [Google Scholar] [CrossRef]
- Richmond, M.E.; Zangwill, S.D.; Kindel, S.J.; Deshpande, S.R.; Schroder, J.N.; Bichell, D.P.; Knecht, K.R.; Mahle, W.T.; Wigger, M.A.; Gaglianello, N.A.; et al. Donor fraction cell-free DNA and rejection in adult and pediatric heart transplantation. J. Heart Lung Transplant. 2020, 39, 454–463. [Google Scholar] [CrossRef] [Green Version]
- Zhao, D.; Zhou, T.; Luo, Y.; Wu, C.; Xu, D.; Zhong, C.; Cong, W.; Liu, Q.; Zhang, J.; Xia, Q. Preliminary clinical experience applying donor-derived cell-free DNA to discern rejection in pediatric liver transplant recipients. Sci. Rep. 2021, 11, 1–9. [Google Scholar]
- Rinaldi, M.; Bartoletti, M.; Bussini, L.; Pancaldi, L.; Pascale, R.; Comai, G.; Morelli, M.; Ravaioli, M.; Cescon, M.; Cristini, F.; et al. COVID-19 in solid organ transplant recipients: No difference in survival compared to general population. Transpl. Infect. Dis. 2021, 23, 13421. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Name | Organ(s) | Sample Type | dd-cfDNA Method | Technique | Donor Sample Required |
|---|---|---|---|---|---|
| Zhang 1999 [26] | Kidney | Urine | Sex mismatch (SRY gene) | Real-time quantitative PCR | No |
| Moreira 2009 [27] | Kidney | Plasma, Urine | Hemoglobin, beta (HBB) gene & TSPY1 gene | Quantitative PCR | Yes |
| Synder 2011 [30] | Heart | Plasma | Sex mismatch (Chr Y) & shotgun sequencing | Digital PCR | Yes |
| Sigdel 2013 [29] | Kidney | Urine | Sex mismatch (SRY gene) | Digital PCR | No |
| Beck 2013 [32] | Heart, Kidney, Liver | Plasma | Informative SNP panel | Droplet digital PCR | No |
| Vlaminck 2014 [36] | Heart | Plasma | Whole-genome arrays | Quantitative PCR | Yes |
| Macher 2014 [28] | Liver | Plasma | SRY & beta-globin gene | Real time quantitative PCR | No |
| Vlaminck 2015 [37] | Lungs | Plasma | Whole-genome arrays | Quantitative PCR | Yes |
| Beck 2015 [38] | Heart, Kidney | Plasma | Informative SNP panel | Droplet digital PCR | No |
| Burnham 2016 [39] | Lungs | Plasma | SNP sequencing with mitochondrial reference sequences | Quantitative PCR | Yes |
| Macher 2016 [40] | Liver | Plasma | RH-negative recipient & RH-positive donor pair | Real time PCR | Yes |
| Grskovic 2016 [33] | Heart, Kidney | Plasma | Informative SNP panel | Next-generation sequencing | No |
| Schutz 2016 [41] | Liver | Plasma | Informative SNP panel | Droplet digital PCR | No |
| Zou 2017 [42] | Lung | Plasma | HLA specific primers and probes | Droplet digital PCR | No |
| Bromberg 2017 [43] | Kidney | Plasma | Informative SNP panel | Next-generation sequencing | No |
| Goh 2017 [44] | Liver | Plasma | Deletion/Insertion Polymorphism (DIP) panel | Droplet digital PCR | Yes |
| Schutz 2017 [3] | Liver | Plasma | Informative SNP panel | Droplet digital PCR | No |
| Bloom 2017 [45] | Kidney | Plasma | Informative SNP panel | Next-generation sequencing | No |
| Tanaka 2018 [46] | Lung | Plasma | SNP genotyping & informative SNP panel | Droplet digital PCR | Yes |
| Jordan 2018 [47] | Kidney | Plasma | Informative SNP panel | Next-generation sequencing | No |
| Weir 2018 [34] | Kidney | Plasma | Informative SNP panel | Next-generation sequencing | No |
| Beck 2018 [2] | Heart | Plasma | Informative SNP panel | Droplet digital PCR | No |
| Gielis 2018 [48] | Kidney | Plasma | Multiplex PCR assay | Next-generation sequencing | Yes |
| Goh 2019 [49] | Liver | Plasma | Deletion/Insertion Polymorphism (DIP) panel | Droplet digital PCR | Yes |
| Khush 2019 [50] | Heart | Plasma | Informative SNP panel | Next-generation sequencing | No |
| Altug 2019 [51] | Kidney | Plasma | Bi-allelic SNP on Chr-2,13,18,21 | Massively multiplexed PCR | No |
| Sigdel 2019 [52] | Kidney | Plasma | SNP-based assay & LabChip NGS 5k | Massively multiplex PCR-next-generation sequencing | No |
| Oellerich 2019 [53] | Kidney | Plasma | Informative SNP panel | Droplet digital PCR | No |
| Sayah 2020 [54] | Lung | Plasma | Informative SNP panel | Next-generation sequencing | No |
| Potter 2020 [55] | Kidney | Plasma | Informative SNP panel | Next-generation sequencing | No |
| Schutz 2020 [56] | Kidney | Plasma | Informative SNP panel | Droplet digital PCR | No |
| Shen 2020 [57] | Kidney | Plasma | Informative SNP panel | Next-generation sequencing | No |
| Puliyanda 2020 [58] | Lung | Plasma | Informative SNP panel | Next-generation sequencing | No |
| Stites 2020 [59] | Kidney | Plasma | Informative SNP panel | Next-generation sequencing | No |
| Khush 2021 [60] | Lung | Plasma | Informative SNP panel | Next-generation sequencing | No |
| Name | Organ(s) | Sample Type | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|
| Moiera 2009 [27] | Kidney | Plasma, Urine | 89 | 85 | 53 | 98 |
| Sigdel 2013 [29] | Kidney | Urine | 81 | 75 | - | - |
| Schutz 2016 [41] | Liver | Plasma | 91.2 | 92.5 | - | - |
| Schutz 2017 [3] | Liver | Plasma | 90.3 | 92.9 | - | - |
| Bloom 2017 [45] | Kidney | Plasma | 81 | 83 | 44 | 96 |
| Jordan 2018 [47] | Kidney | Plasma | 81 | 82 | 81 | 83 |
| Weir 2018 [34] | Kidney | Plasma | 69.6 | 84 | 60.9 | 88.6 |
| Khush 2019 [50] | Heart | Plasma | 80 | 44 | 8.7 | 97.1 |
| Sigdel 2019 [52] | Kidney | Plasma | 88.7 | 72.6 | 52 | 95 |
| Oellerich 2019 [53] | Kidney | Plasma | 73 | 73 | 13 | 98 |
| Sayah 2020 [54] | Lung | Plasma | 73.1 | 52.9 | 34 | 85.5 |
| Levine 2020 [73] | Lung | Plasma | 81 | 100 | - | - |
| Richmond 2020 [74] | Heart | Plasma | 75 | 79 | - | - |
| Puliyanda 2020 [58] | Lung | Plasma | 86 | 100 | - | - |
| Zhao 2021 [75] | Liver | Plasma | 81.8 | 81.9 | 56.2 | 93.9 |
| Khush 2021 [60] | Lung | Plasma | 55.6 | 75.8 | 43.3 | 83.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumar, N.; Rana, R.; Rana, D.S.; Gupta, A.; Sachdeva, M.P. Donor-Derived Cell-Free DNA to Diagnose Graft Rejection Post-Transplant: Past, Present and Future. Transplantology 2021, 2, 348-361. https://doi.org/10.3390/transplantology2030034
Kumar N, Rana R, Rana DS, Gupta A, Sachdeva MP. Donor-Derived Cell-Free DNA to Diagnose Graft Rejection Post-Transplant: Past, Present and Future. Transplantology. 2021; 2(3):348-361. https://doi.org/10.3390/transplantology2030034
Chicago/Turabian StyleKumar, Naveen, Rashmi Rana, Devender Singh Rana, Anurag Gupta, and Mohinder Pal Sachdeva. 2021. "Donor-Derived Cell-Free DNA to Diagnose Graft Rejection Post-Transplant: Past, Present and Future" Transplantology 2, no. 3: 348-361. https://doi.org/10.3390/transplantology2030034
APA StyleKumar, N., Rana, R., Rana, D. S., Gupta, A., & Sachdeva, M. P. (2021). Donor-Derived Cell-Free DNA to Diagnose Graft Rejection Post-Transplant: Past, Present and Future. Transplantology, 2(3), 348-361. https://doi.org/10.3390/transplantology2030034