
Barriers to the Utilization of Primary Health Centers (PHCs) in Iraq


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Data Extraction
3. Results
3.1. Primary Health Centers (PHCs)
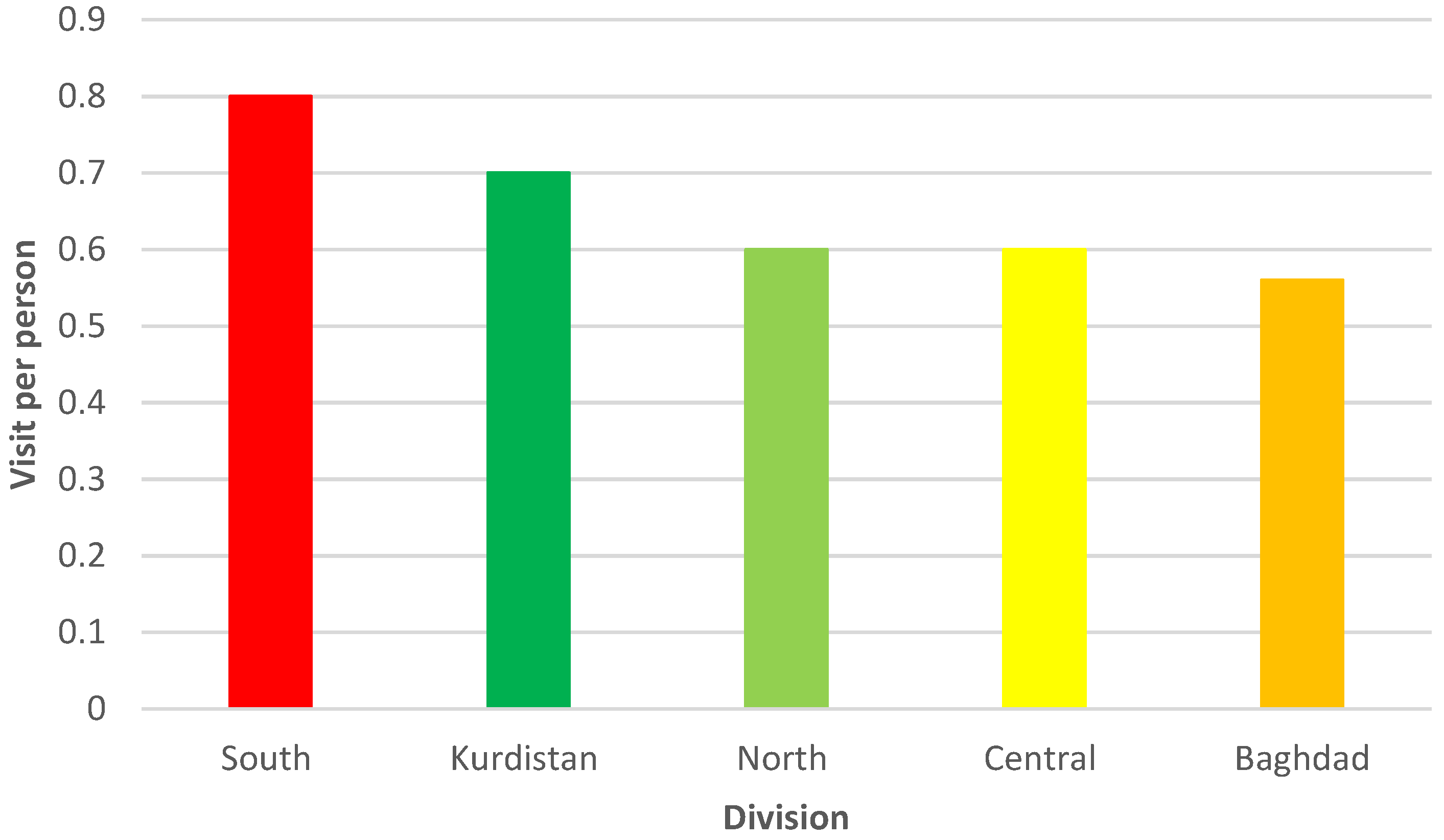
3.2. Results by Region
3.2.1. Kurdistan
3.2.2. North
3.2.3. Baghdad
3.2.4. Central
3.2.5. South
3.3. Vulnerable Groups
3.3.1. Age-Friendly PHCs
3.3.2. Urban–Rural Gap
3.3.3. Antenatal Care (ANC)
3.4. Health Utilization as a Realized Access
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yang, S.; Zhou, M.; Liao, J.; Ding, X.; Hu, N.; Kuang, L. Association between Primary Care Utilization and Emergency Room or Hospital Inpatient Services Utilization among the Middle-Aged and Elderly in a Self-Referral System: Evidence from the China Health and Retirement Longitudinal Study 2011–2018. Int. J. Environ. Res. Public Health 2022, 19, 12979. [Google Scholar] [CrossRef]
- Qureshi, S.; Xiong, J. Equitable Healthcare Provision: Uncovering the Impact of the Mobility Effect on Human Development. Inf. Syst. Manag. 2021, 38, 2–20. [Google Scholar] [CrossRef]
- Jakovljevic, M.; Pallegedara, A.; Vinayagathasan, T.; Kumara, A.S. Editorial: Inequality in healthcare utilization and household spending in developing countries. Front. Public Health 2022, 10, 970819. [Google Scholar] [CrossRef] [PubMed]
- Senn, N.; Breton, M.; Ebert, S.T.; Lamoureux-Lamarche, C.; Lévesque, J.-F. Assessing primary care organization and performance: Literature synthesis and proposition of a consolidated framework. Health Policy 2021, 125, 160–167. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, W. Utilization and out-of-pocket expenses of primary care among the multimorbid elderly in China: A two-part model with nationally representative data. Front. Public Health 2022, 10, 1057595. [Google Scholar] [CrossRef] [PubMed]
- WHO. Quality in Primary Health Care; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Lafta, R.K.; Al-Nuaimi, M.A. War or health: A four-decade armed conflict in Iraq. Med. Confl. Surviv. 2019, 35, 209–226. [Google Scholar] [CrossRef]
- WHO. Iraq Health Profile 2015; World Health Organization: Cairo, Egypt, 2017; pp. 14–15. [Google Scholar]
- WHO. Iran Health Profile 2015; World Health Organization: Cairo, Egypt, 2017; pp. 11–13. [Google Scholar]
- WHO. Jordan Health Profile 2015; World Health Organization: Cairo, Egypt, 2017; pp. 14–15. [Google Scholar]
- MoH. Health Status in Iraq-Challenges and Priorities; Ministry of Health: Baghdad, Iraq, 2019; pp. 2–3.
- Al Janabi, T.; Chung, S. Current Impact and Long-Term Influence of the COVID-19 Pandemic on Iraqi Healthcare Systems: A Case Study. Epidemiologia 2022, 3, 412–433. [Google Scholar] [CrossRef]
- Godichet, O.; Ghanem, V. Iraqi system of primary health care: A communitarian system of family medicine under a dictatorship framework. Contemp. Nurse 2004, 17, 113–124. [Google Scholar] [CrossRef]
- MoH. Health Services Fees 2022; Ministry of Health: Baghdad, Iraq, 2022.
- HomeOffice. Iraq: Medical and Healthcare Provision; Home Office: London, UK, 2021.
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Global Health; Committee on the Evaluation of Strengthening Human Resources for Health Capacity in the Republic of Rwanda Under the President’s Emergency Plan for AIDS Relief (PEPFAR). Evaluation of PEPFAR’s Contribution (2012–2017) to Rwanda’s Human Resources for Health Program; National Academies Press: Washington, DC, USA, 2020.
- WHO. The Global Health Observatory. Available online: https://www.who.int/data/gho/data/themes/topics/indicator-groups/indicator-group-details/GHO/nursing-and-midwifery-personnel (accessed on 26 January 2023).
- MoH. Annual Statistical Report 2020; Ministry of Health: Baghdad, Iraq, 2021.
- UN. Iraq Socio-Economic Response Plan; UN: New York, NY, USA, 2020. [Google Scholar]
- Thakur, B.; Pathak, M. Editorial: Utilization of healthcare services for children in low and middle-income countries: Its determinants and child health outcomes. Front. Pediatr. 2022, 10, 1014775. [Google Scholar] [CrossRef]
- Legatum Institute. The 2021 Legatum Prosperity Index Report; Legatum Institute: London, UK, 2021. [Google Scholar]
- WHO. Global Reference List of 100 Core Health Indicators; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- WHO. 2018 Global Reference List of 100 Core Health Indicators (Plus Health-Related SDGs); World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Abera Abaerei, A.; Ncayiyana, J.; Levin, J. Health-Care utilization and associated factors in Gauteng province, South Africa. Glob. Health Action 2017, 10, 1305765. [Google Scholar] [CrossRef]
- Levesque, J.-F.; Harris, M.F.; Russell, G. Patient-Centred access to health care: Conceptualising access at the interface of health systems and populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habib, O.S.; Vaughan, J.P. The determinants of health services utilization in southern Iraq: A household interview survey. Int. J. Epidemiol. 1986, 15, 395–403. [Google Scholar] [CrossRef] [PubMed]
- WBG. Iraq—Systematic Country Diagnostic (English); 112333-IQ.; World Bank Group: Washington, DC, USA, 2017; p. 26. [Google Scholar]
- Verguet, S.; Hailu, A.; Eregata, G.T.; Memirie, S.T.; Johansson, K.A.; Norheim, O.F. Toward universal health coverage in the post-COVID-19 era. Nat. Med. 2021, 27, 380–387. [Google Scholar] [CrossRef]
- MoH. A Basic Health Services Package for Iraq; Ministry of Health: Baghdad, Iraq, 2010; pp. 17–20.
- Ahmad, R.F.; Al-juburi, N.H. The Future Need for Health Services in Salah Al-Din Governorate. J. Hist. Cult. Stud. 2021, 12, 390–412. [Google Scholar]
- Taher, H.A. Efficiency of health development services in the presence of Warka District Center for the year 2021. Al-Qadisiya J. Humanit. Sci. 2022, 25, 301–314. [Google Scholar]
- USAID. USAID Primary Health Care Project in Iraq (PHCPI); URC: Chevy Chase, MD, USA, 2011. [Google Scholar]
- Seyed-Nezhad, M.; Ahmadi, B.; Akbari-Sari, A. Factors affecting the successful implementation of the referral system: A scoping review. J. Fam. Med. Prim. Care 2021, 10, 4364–4375. [Google Scholar] [CrossRef]
- Al-Shatari, S.A.; Rayhan, T.H.; Younis, M.H.; Abutiheen, A.; Hasan, L.A.; Ahmed, S.; Tariq, Z.; Kamoana, B.; Al-Mosawey, S.; Ismail, M. Practice & Opinion of Doctors in Hospitals toward Referral System in Iraq. AL-Kindy Coll. Med. J. 2022, 18, 222–227. [Google Scholar] [CrossRef]
- Shaihan, S.H.; Makhlif, M.J. Administration Implication of the Change on the Efficiency of the Performance of Health Institution—Referral Health System Case Study. AL-Anbar Univ. J. Econ. Adm. Sci. 2014, 6, 25–49. [Google Scholar]
- Ba’amer, A.A. Coverage of and barriers to routine child vaccination in Mukalla district, Hadramout governorate, Yemen. East. Mediterr. Health J. 2010, 16, 223–227. [Google Scholar] [CrossRef]
- Al-Jumaili, A.A.; Al-Rekabi, M.D.; Sorofman, B. Evaluation of instruments to assess health literacy in Arabic language among Iraqis. Res. Soc. Adm. Pharm. 2015, 11, 803–813. [Google Scholar] [CrossRef]
- Dewalt, D.A.; Berkman, N.D.; Sheridan, S.; Lohr, K.N.; Pignone, M.P. Literacy and health outcomes: A systematic review of the literature. J. Gen. Intern. Med. 2004, 19, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- EMRO. Health System Strengthening. Available online: https://www.emro.who.int/iraq/priority-areas/health-system-strengthening.html (accessed on 23 February 2023).
- Mansour, A.A.; Odaa, A.H.; Wanoose, H.L. Corticosteroid nonprescription use: A cross-sectional hospital-based study in Basrah. Med. Princ. Pract. 2010, 19, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Shabila, N.P.; Al-Tawil, N.G.; Al-Hadithi, T.S.; Sondorp, E. Using Q-methodology to explore people’s health seeking behavior and perception of the quality of primary care services. BMC Public Health 2014, 14, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anthony, C.R.; Moore, M.; Hilborne, L.H.; Rooney, A.; Hickey, S.; Ryu, Y.; Botwinick, L. Health Sector Reform in the Kurdistan Region—Iraq: Primary Care Management Information System, Physician Dual Practice Finance Reform, and Quality of Care Training; RAND Corporation: Santa Monica, CA, USA, 2017. [Google Scholar]
- Anthony, C.R.; Moore, M.; Hilborne, L.H.; Mulcahy, A.W. Health Sector Reform in the Kurdistan Region—Iraq: Financing Reform, Primary Care, and Patient Safety (Arabic-Language Version); RAND Corporation: Santa Monica, CA, USA, 2014. [Google Scholar]
- Mohammad, M.Y.; Firas, F.H.; Yahia, A.H. Patients satisfaction to quality of health services of family doctors in family medicine centers in left side of Mosul city. Ann. Coll. Med. Mosul 2020, 42, 76–81. [Google Scholar] [CrossRef]
- Hasani, S.; Al-Jahishi, S. Evaluating the efficiency of health services in Salah Al-Din Governorate using GIS. Al-Qadisiya J. Humanit. Sci. 2018, 21, 445–472. [Google Scholar]
- Jasim, B.J.; Khalifa, M.F. Evaluation of Quality of Primary Health Care Services at Primary Health Care Centers in Baghdad City: A Comparative Study. Iraqi Natl. J. Nurs. Spec. 2018, 31, 110–117. [Google Scholar]
- Mishari, A.K.; Essa, S.A.; Muhammed, A.N. Introduction of an Appointment System in Primary Health Care Setting in Baghdad: Views of Patients and Health Care Providers. Al-Kindy Coll. Med. J. 2021, 17, 45–49. [Google Scholar] [CrossRef]
- Salih, J.M.; Hathaf, N.F.; Al-Kinani, S.S. Epidemiology of Health Problems Among Internally Displaced Persons (IDPS)’ Camps. Diyala Agric. Sci. J. 2018, 10, 280–289. [Google Scholar]
- Shareef, M.M. The Efficiency of Health Services in Al-Baghdadi City. J. Univ. Anbar Humanit. 2021, 2, 311–324. [Google Scholar] [CrossRef]
- Abbas, N. The relationship between quality of service and customer satisfaction in the health sector An analytical study at Al-Aqsa Health Center in Al-Qadi District—Babel. Adm. Econ. Coll. J. Econ. Adm. Financ. Stud. 2021, 13, 407–428. [Google Scholar]
- Sa’adoon, A.A.; Hussien, A.H.; Museher, T.R. Patients’ Satisfaction for Health Care Services at Thi-qar Province, Iraq. Thi-Qar Med. J. 2008, 2, 39–45. [Google Scholar]
- Aboud, A.A. The Spatial Differentiation for Health Development Indicators and Its Prospects in Basra Province (A Study in Development Geography). Basra Stud. J. 2016, 21, 85–128. [Google Scholar]
- Moussa, R.A. Evaluation of the Efficiency of Educational and Health Services in the City of Ghar Sokar. J. Educ. Coll. 2021, 2, 199–240. [Google Scholar]
- Hammadi, H.A.; Taher, H.A. Spatial Analysis of Household Deprivation in Indicators of the Health Field in Al Muthanna Governorate for the Year 2019. Al-Qadisiya J. Humanit. Sci. 2020, 23, 191–211. [Google Scholar]
- Tariq, E.; Lafta, R. A Profile on Health-Care Services for Old in Baghdad. Mustansiriya Med. J. 2018, 17, 52–56. [Google Scholar] [CrossRef]
- KAPITA. Overview on the Expenditure of the Iraqi Household; KAPITA: Baghdad, Iraq, 2021. [Google Scholar]
- Taniguchi, H.; Rahman, M.M.; Swe, K.T.; Islam, M.R.; Rahman, M.S.; Parsell, N.; Hussain, A.; Shibuya, K.; Hashizume, M. Equity and determinants in universal health coverage indicators in Iraq, 2000–2030: A national and subnational study. Int. J. Equity Health 2021, 20, 196. [Google Scholar] [CrossRef]
- Ismael, W.I.; Farhood, H.F. Evaluation of the Quality of Maternal Health Services in Primary Health-Care Centers by Using Service Provision Assessment. Med. J. Babylon 2019, 16, 25–30. [Google Scholar] [CrossRef]
- Molan, J.A. Barriers to Accessing Antenatal Care Services in Primary Health Care Centers in Rural Areas of Basrah. Iraqi Natl. J. Med. 2021, 3, 43–52. [Google Scholar]
- Burnham, G.; Hoe, C.; Hung, Y.W.; Ferati, A.; Dyer, A.; Hifi, T.A.; Aboud, R.; Hasoon, T. Perceptions and utilization of primary health care services in Iraq: Findings from a national household survey. BMC Int. Health Hum. Rights 2011, 11, 15. [Google Scholar] [CrossRef] [Green Version]
- Alasady, S.H.; Alsahlany, J.T. Measurement of the Efficiency of Health Services in the Nasiriyah City. Adab Al-Basrah 2014, 184, 253–294. [Google Scholar]
- UNHCR. Iraq Camp Master List and Population Flow—November 2022; UNHCR: Geneva, Switzerland, 2022. [Google Scholar]
- Yaddanapalli, S.; Srinivas, R.; Simha, B.; Devaki, T.; Viswanath, V.; Pachava, S.; Chandu, V. Utilization of health services in Tenali Mandal, Andhra Pradesh—A cross-sectional study. J. Fam. Med. Prim. Care 2019, 8, 2997–3004. [Google Scholar] [CrossRef]
- Gage, A.D.; Leslie, H.H.; Bitton, A.; Jerome, J.G.; Joseph, J.P.; Thermidor, R.; Kruk, M.E. Does quality influence utilization of primary health care? Evidence from Haiti. Glob. Health 2018, 14, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A’Aqoulah, A.; Kuyini, A.B.; Albalas, S. Exploring the Gap Between Patients’ Expectations and Perceptions of Healthcare Service Quality. Patient Prefer. Adherence 2022, 16, 1295. [Google Scholar] [CrossRef] [PubMed]
- Bartsokas, C.; Sissouras, A.; Jelastopulu, E. Healthcare services utilisation, subjective perception of health and satisfaction with services in Patras, Greece. J. Public Health 2021, 29, 369–373. [Google Scholar] [CrossRef]
- Alghamdi, K.; Aljohani, A.; Taha, J.; Qari, L.; Demyati, M.; Alzahrani, S. Public Awareness and Utilization of the Primary Health Care Services in Al-Madinah, Saudi Arabia. Middle East J. Fam. Med. 2020, 18, 33–41. [Google Scholar] [CrossRef]
- Adebayo, A.M.; Asuzu, M.C. Utilisation of a community-based health facility in a low-income urban community in Ibadan, Nigeria. Afr. J. Prim. Health Care Fam. Med. 2015, 7, 735. [Google Scholar] [CrossRef] [Green Version]
- Mohiuddin, A.K. Patient Satisfaction: A Healthcare Services Scenario in Bangladesh. Am. J. Med. Sci. Pharm. Res. 2020, 1, 1–8. [Google Scholar] [CrossRef]
- Edmealem, A.; Tsegaye, D.; Andualem, A.; Ademe, S.; Gedamu, S. Implementation of Compassionate and Respectful Health Care Service at Northeast Ethiopia: Patients’ Perspective. Int. J. Caring Sci. 2020, 13, 991–1003. [Google Scholar]
- Sultan, A.S. Medicine in the 21st century: The situation in a rural Iraqi community. Patient Educ. Couns. 2007, 68, 66–69. [Google Scholar] [CrossRef]
- Onwujekwe, O. Inequities in healthcare seeking in the treatment of communicable endemic diseases in Southeast Nigeria. Soc. Sci. Med. 2005, 61, 455–463. [Google Scholar] [CrossRef]
- Al-Lela, O.Q.B.; Baidi Bahari, M.; Al-Abbassi, M.G.; Salih, M.R.M.; Basher, A.Y. Influence of health providers on pediatrics’ immunization rate. J. Trop. Pediatr. 2012, 58, 441–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Lela, O.Q.; Bahari, M.B.; Al-Abbassi, M.G.; Salih, M.R.; Basher, A.Y. Iraqi parents’ views of barriers to childhood immunization. East Mediterr. Health J. 2013, 19, 295–297. [Google Scholar] [CrossRef] [PubMed]
- Galea, S.; Erwin, P.C. Improving the US and Global Pandemic Response: Lessons from Cuba. Am. J. Public Health 2023, 113, 361–362. [Google Scholar] [CrossRef]
- Nwokoro, U.U.; Ugwa, O.M.; Ekenna, A.C.; Obi, I.F.; Onwuliri, C.D.; Agunwa, C. Determinants of primary healthcare services utilisation in an under-resourced rural community in Enugu State, Nigeria: A cross-sectional study. Pan Afr. Med. J. 2022, 42, 209. [Google Scholar] [CrossRef]
- Khadim, H.J.; Farhan, A.R.; ALRubaey, M.G. The Impact of Accreditation of Primary Healthcare Centers on Quality of Care as Perceived by Healthcare Providers and Directors in Baghdad. Iraqi J. Community Med. 2018, 31, 1–5. [Google Scholar]
- Alotaibi, S.Y. Accreditation of primary health care centres in the KSA: Lessons from developed and developing countries. J. Taibah Univ. Med. Sci. 2023, 18, 711–725. [Google Scholar] [CrossRef]
- Shabila, N. Assessment of the Iraqi primary care referral system: Reporting a high self-requested referral rate. Middle East J. Fam. Med. 2012, 10, 4–10. [Google Scholar]
- Al-Shatari, S.A.; Hasan, L.A.; Shwaish, Z.; Abutiheen, A.; Ryhan, T.; Younise, M.; Kamoona, B.; Al-Mosawey, S.; Khaleel, M.; Al-Ashaq, O. Practice and Opinion of Doctors in Primary Health Care Centers Toward Referral System: Samples from Nine Governorates in Iraq. AL-Kindy Coll. Med. J. 2021, 17, 100–106. [Google Scholar] [CrossRef]
- Nasrin, J.; Leila, D.; Mahdi, M.; Jafar Sadegh, T.; Vladimir Sergeevich, G. Public-Private partnerships in primary health care: A scoping review. BMC Health Serv. Res. 2021, 21, 4. [Google Scholar] [CrossRef]
- Aghdash, S.A.; Sharifzade, H.; Bande-Ehahi, K.; Bolbanabad, A.M.; Gharaee, H. Public-Private Partnership Experiences and Achievements in Providing Primary Health Care to the Elderly: A Scoping Review. Health Technol. Assess. Action 2022, 5, 3. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Governorate | Population | Females | Male | Urban (%) | Rural (%) | PHC Number | Per Capita Visit |
|---|---|---|---|---|---|---|---|
| Baghdad | 8,558,625 | 4,215,859 | 4,342,766 | 87.5 | 12.5 | 260 | 0.56 |
| Basrah | 3,063,059 | 1,524,286 | 1,538,773 | 81.2 | 18.8 | 135 | 0.90 |
| Nineveh | 3,928,215 | 1,921,564 | 2,006,651 | 60.6 | 39.4 | 185 | 0.67 |
| Maysan | 1,171,802 | 588,036 | 583,766 | 73.9 | 26.1 | 79 | 0.43 |
| Al-Dewaniya | 1,359,642 | 674,362 | 685,280 | 57.3 | 42.7 | 84 | 0.51 |
| Diala | 1,724,238 | 853,239 | 870,999 | 49.2 | 50.8 | 102 | 0.81 |
| Al-Anbar | 1,865,818 | 907,275 | 958,543 | 50.0 | 50.0 | 187 | 0.43 |
| Babylon | 2,174,783 | 1,075,899 | 1,098,884 | 48.3 | 51.7 | 121 | 0.59 |
| Kerbela | 1,283,484 | 636,022 | 647,462 | 66.9 | 33.1 | 62 | 0.88 |
| Kirkuk | 1,682,809 | 835,689 | 847,120 | 73.9 | 26.1 | 127 | 0.38 |
| Wasit | 1,452,007 | 718,986 | 733,021 | 60.2 | 39.8 | 78 | 0.69 |
| Thi-Qar | 2,206,514 | 1,098,993 | 1,107,521 | 64.2 | 35.8 | 168 | 0.64 |
| Al-Muthanna | 857,652 | 426,675 | 430,977 | 46.4 | 53.6 | 71 | 0.70 |
| Salah Al-Deen | 1,680,015 | 831,380 | 848,635 | 45.1 | 54.9 | 129 | 0.50 |
| Al-Najaf | 1,549,788 | 772,754 | 777,034 | 71.4 | 28.6 | 82 | 0.74 |
| Erbil | 1,953,341 | 967,192 | 986,149 | 83.2 | 16.8 | 272 | 0.57 |
| Duhouk | 1,361,211 | 679,122 | 682,089 | 74.1 | 25.9 | 171 | 1.14 |
| Al-Sulaimaniya | 2,277,171 | 1,138,018 | 1,139,153 | 84.7 | 15.3 | 492 | 0.54 |
| Strengths | Weaknesses | |
|---|---|---|
|
| |
| Opportunities |
|
|
| ||
| Threats |
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Janabi, T. Barriers to the Utilization of Primary Health Centers (PHCs) in Iraq. Epidemiologia 2023, 4, 121-133. https://doi.org/10.3390/epidemiologia4020013
Al Janabi T. Barriers to the Utilization of Primary Health Centers (PHCs) in Iraq. Epidemiologia. 2023; 4(2):121-133. https://doi.org/10.3390/epidemiologia4020013
Chicago/Turabian StyleAl Janabi, Taysir. 2023. "Barriers to the Utilization of Primary Health Centers (PHCs) in Iraq" Epidemiologia 4, no. 2: 121-133. https://doi.org/10.3390/epidemiologia4020013
APA StyleAl Janabi, T. (2023). Barriers to the Utilization of Primary Health Centers (PHCs) in Iraq. Epidemiologia, 4(2), 121-133. https://doi.org/10.3390/epidemiologia4020013