
Quality of Life and Health Determinants of Informal Caregivers Aged 65 Years and Over

 , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Study Population
2.3. Data Collected
2.3.1. Data Collection
Socio-Demographic Data
Informal Caregivers
Quality of Life
Access to Technologies
Level of Physical Activity
Physical Activity Preferences
Subjective Age and Age of Becoming Young or Old
Health Literacy
Sense of Coherence
2.3.2. Study Instruments
2.4. Statistical Analysis
3. Results
3.1. Study Participants
3.2. Informal Caregivers
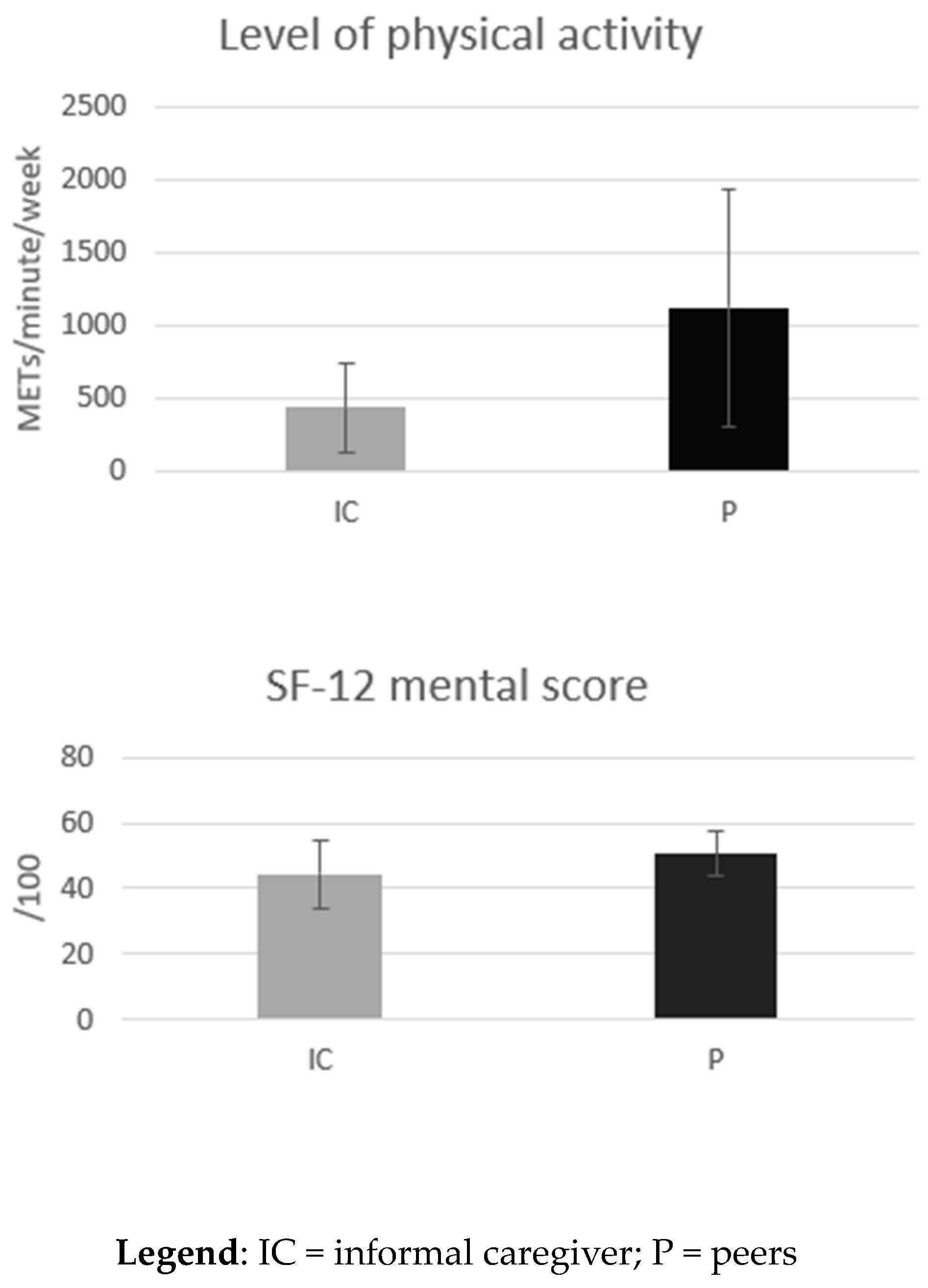
3.3. Quality of Life
3.4. Access to Technology
3.5. Level of Physical Activity
3.6. Physical Activity Preferences
3.6.1. Preferences for Face-to-Face Physical Activity
3.6.2. Preferences for Online Physical Activity
3.7. Subjective Age and Age When Becoming Young or Old
3.8. Health Literacy
3.9. Sense of Coherence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lindt, N.; van Berkel, J.; Mulder, B.C. Determinants of overburdening among informal carers: A systematic review. BMC Geriatr. 2020, 20, 304. [Google Scholar] [CrossRef]
- de Klerk, M.; de Boer, A.; Plaisier, I. Determinants of informal care-giving in various social relationships in The Netherlands. Health Soc. Care Community 2021, 29, 1779–1788. [Google Scholar] [CrossRef]
- Verbakel, E.; Tamlagsrønning, S.; Winstone, L.; Fjær, E.L.; Eikemo, T.A. Informal care in Europe: Findings from the European Social Survey (2014) special module on the social determinants of health. Eur. J. Public Health 2017, 27 (Suppl. S1), 90–95. [Google Scholar] [CrossRef] [PubMed]
- De Koker, B. Socio-demographic determinants of informal caregiving: Co-resident versus extra-resident care. Eur. J. Ageing 2009, 6, 3–15. [Google Scholar] [CrossRef]
- Plöthner, M.; Schmidt, K.; de Jong, L.; Zeidler, J.; Damm, K. Needs and preferences of informal caregivers regarding outpatient care for the elderly: A systematic literature review. BMC Geriatr. 2019, 19, 82. [Google Scholar] [CrossRef]
- Burton, L.C.; Zdaniuk, B.; Schulz, R.; Jackson, S.; Hirsch, C. Transitions in spousal caregiving. Gerontologist 2003, 43, 230–241. [Google Scholar] [CrossRef] [PubMed]
- Bom, J.; Bakx, P.; Schut, F.; van Doorslaer, E. The Impact of Informal Caregiving for Older Adults on the Health of Various Types of Caregivers: A Systematic Review. Gerontologist 2019, 59, e629–e642. [Google Scholar] [CrossRef] [PubMed]
- Di Novi, C.; Jacobs, R.; Migheli, M. The Quality of Life of Female Informal Caregivers: From Scandinavia to the Mediterranean Sea. Eur. J. Popul. 2015, 31, 309–333. [Google Scholar] [CrossRef]
- Roth, D.L.; Fredman, L.; Haley, W.E. Informal caregiving and its impact on health: A reappraisal from population-based studies. Gerontologist 2015, 55, 309–319. [Google Scholar] [CrossRef]
- Pinquart, M.; Sörensen, S. Differences between caregivers and noncaregivers in psychological health and physical health: A meta-analysis. Psychol. Aging 2003, 18, 250–267. [Google Scholar] [CrossRef]
- Roth, D.L.; Perkins, M.; Wadley, V.G.; Temple, E.M.; Haley, W.E. Family caregiving and emotional strain: Associations with quality of life in a large national sample of middle-aged and older adults. Qual. Life Res. 2009, 18, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Sherwood, P.R. Physical and mental health effects of family caregiving. Am. J. Nurs. 2008, 108 (Suppl. S9), 23–27; quiz 27. [Google Scholar] [CrossRef]
- Vitaliano, P.P.; Zhang, J.; Scanlan, J.M. Is caregiving hazardous to one’s physical health? A meta-analysis. Psychol. Bull. 2003, 129, 946–972. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Beach, S.R.; Czaja, S.J.; Martire, L.M.; Monin, J.K. Family Caregiving for Older Adults. Annu. Rev. Psychol. 2020, 71, 635–659. [Google Scholar] [CrossRef] [PubMed]
- Riffin, C.; Van Ness, P.H.; Wolff, J.L.; Fried, T. Multifactorial Examination of Caregiver Burden in a National Sample of Family and Unpaid Caregivers. J. Am. Geriatr. Soc. 2019, 67, 277–283. [Google Scholar] [CrossRef]
- Jütten, L.H.; Mark, R.E.; Sitskoorn, M.M. Predicting self-esteem in informal caregivers of people with dementia: Modifiable and non-modifiable factors. Aging Ment. Health 2020, 24, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Committee on Using Performance Monitoring to Improve Community Health. Improving Health in the Community: A Role for Performance Monitoring; Durch, J.S., Bailey, L.A., Stoto, M.A., Eds.; National Academies Press: Washington, DC, USA, 1997. [Google Scholar]
- Yazdanmanesh, M.; Esmaeili, R.; Nasiri, M.; Vasli, P. Relieving care burden and promoting health-related quality of life for family caregivers of elderly people with Alzheimer’s disease via an empowerment program. Aging Clin. Exp. Res. 2023, 35, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Posadzki, P.; Pieper, D.; Bajpai, R.; Makaruk, H.; Könsgen, N.; Neuhaus, A.L.; Semwal, M. Exercise/physical activity and health outcomes: An overview of Cochrane systematic reviews. BMC Public Health 2020, 20, 1724. [Google Scholar] [CrossRef]
- Twiddy, H.M.; Wilson, P.B.; Swain, D.P.; Branch, J.D.; Morrison, S.; Reynolds, L.J. The association of moderate-to-vigorous and light-intensity physical activity on static balance in middle-aged and older-aged adults. Aging Clin. Exp. Res. 2023, 35, 541–550. [Google Scholar] [CrossRef]
- Jansons, P.; Fyfe, J.J.; Dalla Via, J.; Daly, R.M.; Scott, D. Barriers and enablers associated with participation in a home-based pragmatic exercise snacking program in older adults delivered and monitored by Amazon Alexa: A qualitative study. Aging Clin. Exp. Res. 2023, 35, 561–569. [Google Scholar] [CrossRef]
- Harpham, C.; Gunn, H.; Marsden, J.; Connolly, L. The feasibility, safety, physiological and clinical effects of high-intensity interval training for people with Parkinson’s: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2023, 35, 497–523. [Google Scholar] [CrossRef]
- Lindsay, R.K.; Vseteckova, J.; Horne, J.; Smith, L.; Trott, M.; De Lappe, J.; Soysal, P.; Pizzol, D.; Kentzer, N. The prevalence of physical activity among informal carers: A systematic review of international literature. Sport Sci. Health 2022, 18, 1071–1118. [Google Scholar] [CrossRef]
- Institute of Medicine Committee on Assuring the Health of the Public in the 21st Century. The Future of the Public’s Health in the 21st Century; National Academies Press: Washington, DC, USA, 2002. [Google Scholar]
- Sieck, C.J.; Sheon, A.; Ancker, J.S.; Castek, J.; Callahan, B.; Siefer, A. Digital inclusion as a social determinant of health. NPJ Digit. Med. 2021, 4, 52. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, K.M.; Chow, P.I.; Cohn, W.F.; Ingersoll, K.S.; Ritterband, L.M. Informal Caregivers’ Use of Internet-Based Health Resources: An Analysis of the Health Information National Trends Survey. JMIR Aging 2018, 1, e11051. [Google Scholar] [CrossRef]
- Officer, A.; de la Fuente-Núñez, V. A global campaign to combat ageism. Bull. World Health Organ. 2018, 96, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Mikton, C.; de la Fuente-Núñez, V.; Officer, A.; Krug, E. Ageism: A social determinant of health that has come of age. Lancet 2021, 397, 1333–1334. [Google Scholar] [CrossRef] [PubMed]
- Zwar, L.; König, H.H.; Hajek, A. Can Informal Caregiving be Perceived as Rejuvenating? Changes in Perceptions of Ageing at Onset and End of Informal Caregiving during Different Stages of Life. Gerontology 2023, 69, 483–494. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Coughlin, S.S.; Vernon, M.; Hatzigeorgiou, C.; George, V. Health Literacy, Social Determinants of Health, and Disease Prevention and Control. J. Environ. Health Sci. 2020, 6, 3061. [Google Scholar] [PubMed]
- Lorini, C.; Buscemi, P.; Mossello, E.; Schirripa, A.; Giammarco, B.; Rigon, L.; Albora, G.; Giorgetti, D.; Biamonte, M.A.; Fattorini, L.; et al. Health literacy of informal caregivers of older adults with dementia: Results from a cross-sectional study conducted in Florence (Italy). Aging Clin. Exp. Res. 2023, 35, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Drageset, J.; Nygaard, H.A.; Eide, G.E.; Bondevik, M.; Nortvedt, M.W.; Natvig, G.K. Sense of coherence as a resource in relation to health-related quality of life among mentally intact nursing home residents—A questionnaire study. Health Qual. Life Outcomes 2008, 6, 85. [Google Scholar] [CrossRef]
- Potier, F.; Degryse, J.M.; Henrard, S.; Aubouy, G.; de Saint-Hubert, M. A high sense of coherence protects from the burden of caregiving in older spousal caregivers. Arch. Gerontol. Geriatr. 2018, 75, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Dziuba, A.; Krell-Roesch, J.; Schmidt, S.C.E.; Bös, K.; Woll, A. Association Between Sense of Coherence and Health Outcomes at 10 and 20 Years Follow-Up: A Population-Based Longitudinal Study in Germany. Front. Public Health 2021, 9, 739394. [Google Scholar] [CrossRef] [PubMed]
- Del-Pino-Casado, R.; Espinosa-Medina, A.; López-Martínez, C.; Orgeta, V. Sense of coherence, burden and mental health in caregiving: A systematic review and meta-analysis. J. Affect. Disord. 2019, 242, 14–21. [Google Scholar] [CrossRef]
- Zarit, S.H.; Reever, K.E.; Bach-Peterson, J. Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist 1980, 20, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Ware, J., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Marquet, M.; Missotten, P.; Schroyen, S.; van Sambeek, I.; van den Akker, M.; Van Den Broeke, C.; Buntinx, F.; Adam, S. A Validation of the French Version of the Attitudes to Aging Questionnaire (AAQ): Factor Structure, Reliability and Validity. Psychol. Belg. 2016, 56, 80–100. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Charles, A.; Rygaert, X.; Reginster, J.Y.; Adam, S.; Bruyère, O. Own attitude toward aging among nursing home residents: Results of the SENIOR cohort. Aging Clin. Exp. Res. 2018, 30, 1151–1159. [Google Scholar] [CrossRef]
- Levy, B.R.; Zonderman, A.B.; Slade, M.D.; Ferrucci, L. Memory shaped by age stereotypes over time. J. Gerontol. B Psychol. Sci. Soc. Sci. 2012, 67, 432–436. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Pelikan, J.M.; Fullam, J.; Doyle, G.; Slonska, Z.; Kondilis, B.; Stoffels, V.; Osborne, R.H.; Brand, H. Measuring health literacy in populations: Illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health 2013, 13, 948. [Google Scholar] [CrossRef] [PubMed]
- Mekhail, K.T.; Burström, B.; Marttila, A.; Wångdahl, J.; Lindberg, L. Psychometric qualities of the HLS-EU-Q16 instrument for parental health literacy in Swedish multicultural settings. BMC Public Health 2022, 22, 293. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. The structure and properties of the sense of coherence scale. Soc. Sci. Med. 1993, 36, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Chong, E.; Crowe, L.; Mentor, K.; Pandanaboyana, S.; Sharp, L. Systematic review of caregiver burden, unmet needs and quality-of-life among informal caregivers of patients with pancreatic cancer. Support Care Cancer 2022, 31, 74. [Google Scholar] [CrossRef] [PubMed]
- D’Aoust, R.F.; Brewster, G.; Rowe, M.A. Depression in informal caregivers of persons with dementia. Int. J. Older People Nurs. 2015, 10, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Simons, A.; Toland, S.; Zhang, J.; Zheng, K. Informal caregivers’ quality of life and management strategies following the transformation of their cancer caregiving role: A qualitative systematic review. Int. J. Nurs. Sci. 2021, 8, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Ervin, J.; Taouk, Y.; Fleitas Alfonzo, L.; Peasgood, T.; King, T. Longitudinal association between informal unpaid caregiving and mental health amongst working age adults in high-income OECD countries: A systematic review. eClinicalMedicine 2022, 53, 101711. [Google Scholar] [CrossRef]
- Sheppard, K.D.; Brown, C.J.; Hearld, K.R.; Roth, D.L.; Sawyer, P.; Locher, J.L.; Allman, R.M.; Ritchie, C.S. Symptom burden predicts nursing home admissions among older adults. J. Pain Symptom. Manag. 2013, 46, 591–597. [Google Scholar] [CrossRef]
- Egan, K.J.; Hodgson, W.; Imperatore, G.; Dunlop, M.D.; Maguire, R.; Kirk, A. Supporting Physical Activity for Informal Caregivers during and beyond COVID-19: Exploring the Feasibility, Usability and Acceptability of a Digital Health Smartphone Application, ‘CareFit’. Int. J. Environ. Res. Public Health 2022, 19, 2506. [Google Scholar] [CrossRef]
- Puig-Ribera, A.; Arumí-Prat, I.; Cirera, E.; Solà, M.; Codina-Nadal, A.; Palència, L.; Biaani, B.; Pérez, K. Use of the Superblock model for promoting physical activity in Barcelona: A one-year observational comparative study. Arch. Public Health Arch. Belg. Sante Publique 2022, 80, 257. [Google Scholar] [CrossRef]
- Rokicka, M.; Zajkowska, O. Informal Elderly Caregiving and Time Spent on Leisure: Evidence from Time Use Survey. Ageing Int. 2020, 45, 393–410. [Google Scholar]
- Cubukcu, M. Evaluation of quality of life in caregivers who are providing home care to cancer patients. Support Care Cancer 2018, 26, 1457–1463. [Google Scholar] [CrossRef] [PubMed]
- Baik, D.; Song, J.; Tark, A.; Coats, H.; Shive, N.; Jankowski, C. Effects of Physical Activity Programs on Health Outcomes of Family Caregivers of Older Adults with Chronic Diseases: A Systematic Review. Geriatr. Nurs. 2021, 42, 1056–1069. [Google Scholar] [CrossRef] [PubMed]
- Granet, J.; Peyrusqué, E.; Ruiz, F.; Buckinx, F.; Abdelkader, L.B.; Dang-Vu, T.T.; Sirois, M.J.; Gouin, J.P.; Pageaux, B.; Aubertin-Leheudre, M. Online physical exercise intervention in older adults during lockdown: Can we improve the recipe? Aging Clin. Exp. Res. 2023, 35, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Aubertin-Leheudre, M.; Daoust, R.; Hegg, S.; Martel, D.; Martel-Thibault, M.; Sirois, M.J. Feasibility and Acceptability of Remote Physical Exercise Programs to Prevent Mobility Loss in Pre-Disabled Older Adults during Isolation Periods Such as the COVID-19 Pandemic. J. Nutr. Health Aging 2021, 25, 1106–1111. [Google Scholar] [CrossRef] [PubMed]
- Diehl, M.; Wahl, H.W.; Barrett, A.E.; Brothers, A.F.; Miche, M.; Montepare, J.M.; Westerhof, G.J.; Wurm, S. Awareness of Aging: Theoretical Considerations on an Emerging Concept. Dev. Rev. 2014, 34, 93–113. [Google Scholar] [CrossRef]
- Kotter-Grühn, D.; Kleinspehn-Ammerlahn, A.; Gerstorf, D.; Smith, J. Self-perceptions of aging predict mortality and change with approaching death: 16-year longitudinal results from the Berlin Aging Study. Psychol. Aging 2009, 24, 654–667. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.C.; Berntsen, D. People over forty feel 20% younger than their age: Subjective age across the lifespan. Psychon. Bull. Rev. 2006, 13, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Langballe, E.M.; Skirbekk, V.; Strand, B.H. Subjective age and the association with intrinsic capacity, functional ability, and health among older adults in Norway. Eur. J. Ageing 2023, 20, 4. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.; Loura, D.S.; Nogueira, P.; Melo, G.; Gomes, I.; Ferraz, I.; Viegas, L.; Henriques, M.A. Informal Caregivers’ Health Literacy in Lisbon, Portugal: A Profile for Health Promotion Prioritization. Geriatrics 2022, 7, 92. [Google Scholar] [CrossRef]
- Jiang, Y.; Sereika, S.M.; Lingler, J.H.; Tamres, L.K.; Erlen, J.A. Health literacy and its correlates in informal caregivers of adults with memory loss. Geriatr. Nurs. 2018, 39, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Koelen, M.; Eriksson, M. Older People, Sense of Coherence and Community. In The Handbook of Salutogenesis; Mittelmark, M.B., Bauer, G.F., Vaandrager, L., Pelikan, J.M., Sagy, S., Eriksson, M., Lindström, B., Meier Magistretti, C., Eds.; Springer: Cham, Switzerland, 2022; pp. 185–199. [Google Scholar]


{kind=link}
| Variables | n | Mean ± SD OR n (%) |
|---|---|---|
| Age (years) | 111 | 70.0 ± 3.8 |
| Sex (ratio men:women) | 111 | 32 (28.8):79 (71.2) |
| BMI (kg/m2) | 106 | 26.6 ± 3.6 |
| Country: | 109 | |
| Belgium | 100 (91.7) | |
| Canada | 9 (8.3) | |
| Marital status: | 110 | |
| Married | 55 (50) | |
| Married since (years) | 55 | 36.3 ± 13.5 |
| Bachelor | 9 (8.2) | |
| Widower | 26 (23.6) | |
| Widower since (years) | 26 | 13 ± 10.7 |
| Divorced/separated | 20 (18.2) | |
| Divorced since (years) | 20 | 19.4 ± 10.1 |
| Living place: | 98 | |
| House | 83 (84.7) | |
| Apartment | 13 (13.3) | |
| Nursing home | 2 (2) | |
| Number of people living with the respondent: | 98 | |
| 0 | 27 (27.6) | |
| 1 | 53 (54.1) | |
| 2 | 16 (16.3) | |
| 3 | 2 (2) | |
| Highest level of education: | 97 | |
| University | 19 (19.6) | |
| Higher education | 30 (30.9) | |
| Upper secondary education | 31 (32) | |
| Lower secondary education | 14 (14.4) | |
| Primary education | 1 (1) | |
| None | 2 (2.1) | |
| Monthly household income: | 95 | |
| >EUR 3000 | 29 (30.5) | |
| EUR 2000–3000 | 19 (20) | |
| EUR 1000–2000 | 32 (33.7) | |
| <EUR 1000 | 0 (0) | |
| Refusal to answer | 13 (13.7) | |
| Do not know | 2 (2.1) | |
| Smoker (yes) | 97 | 4 (4.1) |
| Number of cigarettes per day | 4 | 18.3 ± 7.7 |
| Number of alcoholic drinks: | 93 | |
| 0 per week | 25 (26.9) | |
| 1 or 2 per week | 35 (37.6) | |
| 1 or 2 per day | 26 (28) | |
| >2 per day | 7 (7.5) | |
| Number of prevalent chronic diseases | 93 | 1.8 ± 1.4 |
| Number of drugs consumed per day | 93 | 3.1 ± 2.2 |
| Number of vitamins or food supplements consumed per day | 91 | 1.6 ± 1.2 |
| Variables | n | Mean ± SD OR n (%) |
|---|---|---|
| The care-receiver is: | 30 | |
| The spouse | 10 (33.3) | |
| A parent/grandparent | 10 (33.3) | |
| A child | 2 (6.7) | |
| A friend | 5 (16.7) | |
| A neighbor | 2 (6.7) | |
| Other | 1 (3.3) | |
| The care-receiver and the caregiver live together (yes) | 30 | 12 (40) |
| Distance between the homes of the care-receiver and the caregiver (km) | 18 | 16.3 ± 21.1 |
| Age of the care-receiver (years) | 27 | 75.9 ± 12.7 |
| Tasks with which the care-receiver is helped: | 27 | |
| Basic activities of daily living (e.g., toileting, dressing, and mobility) | 6 (22.2) | |
| Meals | 12 (44.4) | |
| Household | 13 (48.1) | |
| Laundry | 10 (37.0) | |
| Budget management | 17 (63) | |
| Administrative management | 18 (66.7) | |
| Drug management (e.g., preparation of the drugs) | 15 (55.6) | |
| Work | 1 (3.7) | |
| Hobbies | 13 (48.1) | |
| Social relations | 11 (40.7) | |
| Transport | 20 (74) | |
| Surveillance | 14 (51.9) | |
| What is the care-receiver suffering from? | 28 | |
| Physical difficulties | 13 (46.4) | |
| Mental difficulties | 4 (14.3) | |
| Physical and mental difficulties | 11 (39.3) | |
| Number of days per week devoted to the care-receiver: | 29 | |
| <1 day/week | 5 (17.2) | |
| 1–2 days/week | 5 (17.2) | |
| 3–4 days/week | 5 (17.2) | |
| 5–6 days/week | 0 (0) | |
| 7 days/week | 14 (48.3) | |
| Number of hours per week devoted to the care-receiver (hours) | 27 | 11.9 ± 9.5 |
| How long the caregiver has been caring for the person (in years) | 29 | 8.9 ± 7.2 |
| Personal motivations for caregiving: | 28 | |
| Love, affection, or friendship | 23 (82.1) | |
| Acknowledgment | 2 (7.1) | |
| The challenge | 0 (0) | |
| Obligation | 1 (3.6) | |
| Keeping a promise | 8 (28.6) | |
| Duty | 11 (39.3) | |
| Religious beliefs | 1 (3.6) | |
| Financial constraints | 0 (0) | |
| Other | 1 (3.6) | |
| Is the carer the only one caring for the person? (yes) | 29 | 12 (42.7) |
| Another person who helps him/her: | 17 | |
| Family member(s) | 13 (76.5) | |
| Friend(s) | 0 (0) | |
| Health professional(s) | 8 (47.1) | |
| Zarit burden (/88) | 24 | 61.9 ± 15.2 |
| Informal Caregivers (n = 30) | Peers (n = 60) | ||||
|---|---|---|---|---|---|
| Variables | n | Mean ± SD OR n (%) | N | Mean ± SD OR n (%) | p-Value |
| Use of the internet: | 27 | 58 | 0.23 1 | ||
| Never | 2 (7.4) | 1 (1.7) | |||
| Every month | 1 (3.7) | 2 (3.5) | |||
| Every week | 2 (7.4) | 4 (6.9) | |||
| Every day | 22 (81.5) | 51 (87.9) | |||
| Use of the internet for how many years | 24 | 19.6 ± 5.9 | 54 | 18.8 ± 6.5 | 0.34 2 |
| Do you have the following connected objects? | 26 | 57 | 0.19 1 | ||
| A smartphone | 22 (84.6) | 54 (94.7) | |||
| A tablet | 17 (65.4) | 29 (50.9) | |||
| A laptop | 16 (61.5) | 40 (70.2) | |||
| A computer | 12 (46.2) | 22 (38.6) | |||
| How long have you owned these connected objects? | 24 | 17.5 ± 7.4 | 55 | 17.1 ± 6.8 | 0.45 2 |
| Do you regularly use messaging and video-calling applications (e.g., Messenger, WhatsApp, Skype, FaceTime, etc.)? (yes) | 26 | 21 (80.7) | 58 | 52 (89.7) | 0.30 1 |
| Have you ever used an application(s) for physical activity? (yes) | 26 | 8 (30.8) | 58 | 22 (37.7) | 0.63 1 |
| Have you ever used an application(s) to measure your level of physical activity (number of steps, calories burned, number of kilometers traveled, etc.)? (yes) | 26 | 15 (57.7) | 57 | 25 (43.9) | 0.41 1 |
| Barriers to Physical Activity: n (%) | Facilitators of Physical Activity: n (%) | ||
|---|---|---|---|
| Cost of physical activities | 7 (28) | Health benefits | 20 (80) |
| Lack of time | 9 (36) | Previous sports participation | 2 (8) |
| Schedule constraints | 6 (24) | Free of charge | 13 (52) |
| Aging (e.g., “I am too old to exercise”) | 2 (8) | Proximity to home | 11 (44) |
| Health condition | 3 (12) | Limited duration of the sessions | 9 (36) |
| Fatigue | 10 (40) | Atmosphere (e.g., conviviality of the group) | 16 (64) |
| Distance (e.g., far from home, access to public transport, or inability to drive) | 4 (16) | Groups of people of the same age | 10 (40) |
| Fear of getting involved | 5 (20) | Supervision of the sessions by a professional | 11 (44) |
| Fear of getting injured | 0 (0) | Opportunities for physical activity at home | 6 (24) |
| Lack of physical activities adapted to a particular health condition | 2 (8) | The possibility of being accompanied by a partner during the session | 3 (12) |
| Lack of physical activities adapted to a particular age | 2 (8) | Other | 0 (0) |
| Lack of motivation | 8 (32) | ||
| Impossibility of leaving the person that is being helped on their own | 2 (8) | ||
| Other | 1 (4) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buckinx, F.; Adam, S.; Aubertin-Leheudre, M.; De Saint Hubert, M.; Mouton, A.; Potier, F.; Reginster, J.-Y.; Bruyere, O. Quality of Life and Health Determinants of Informal Caregivers Aged 65 Years and Over. Epidemiologia 2023, 4, 464-482. https://doi.org/10.3390/epidemiologia4040039
Buckinx F, Adam S, Aubertin-Leheudre M, De Saint Hubert M, Mouton A, Potier F, Reginster J-Y, Bruyere O. Quality of Life and Health Determinants of Informal Caregivers Aged 65 Years and Over. Epidemiologia. 2023; 4(4):464-482. https://doi.org/10.3390/epidemiologia4040039
Chicago/Turabian StyleBuckinx, Fanny, Stéphane Adam, Mylène Aubertin-Leheudre, Marie De Saint Hubert, Alexandre Mouton, Florence Potier, Jean-Yves Reginster, and Olivier Bruyere. 2023. "Quality of Life and Health Determinants of Informal Caregivers Aged 65 Years and Over" Epidemiologia 4, no. 4: 464-482. https://doi.org/10.3390/epidemiologia4040039
APA StyleBuckinx, F., Adam, S., Aubertin-Leheudre, M., De Saint Hubert, M., Mouton, A., Potier, F., Reginster, J. -Y., & Bruyere, O. (2023). Quality of Life and Health Determinants of Informal Caregivers Aged 65 Years and Over. Epidemiologia, 4(4), 464-482. https://doi.org/10.3390/epidemiologia4040039