
Childhood Mediterranean Diet Adherence Is Associated with Lower Prevalence of Childhood Obesity, Specific Sociodemographic, and Lifestyle Factors: A Cross-Sectional Study in Pre-School Children

 ,
,  ,
, 
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
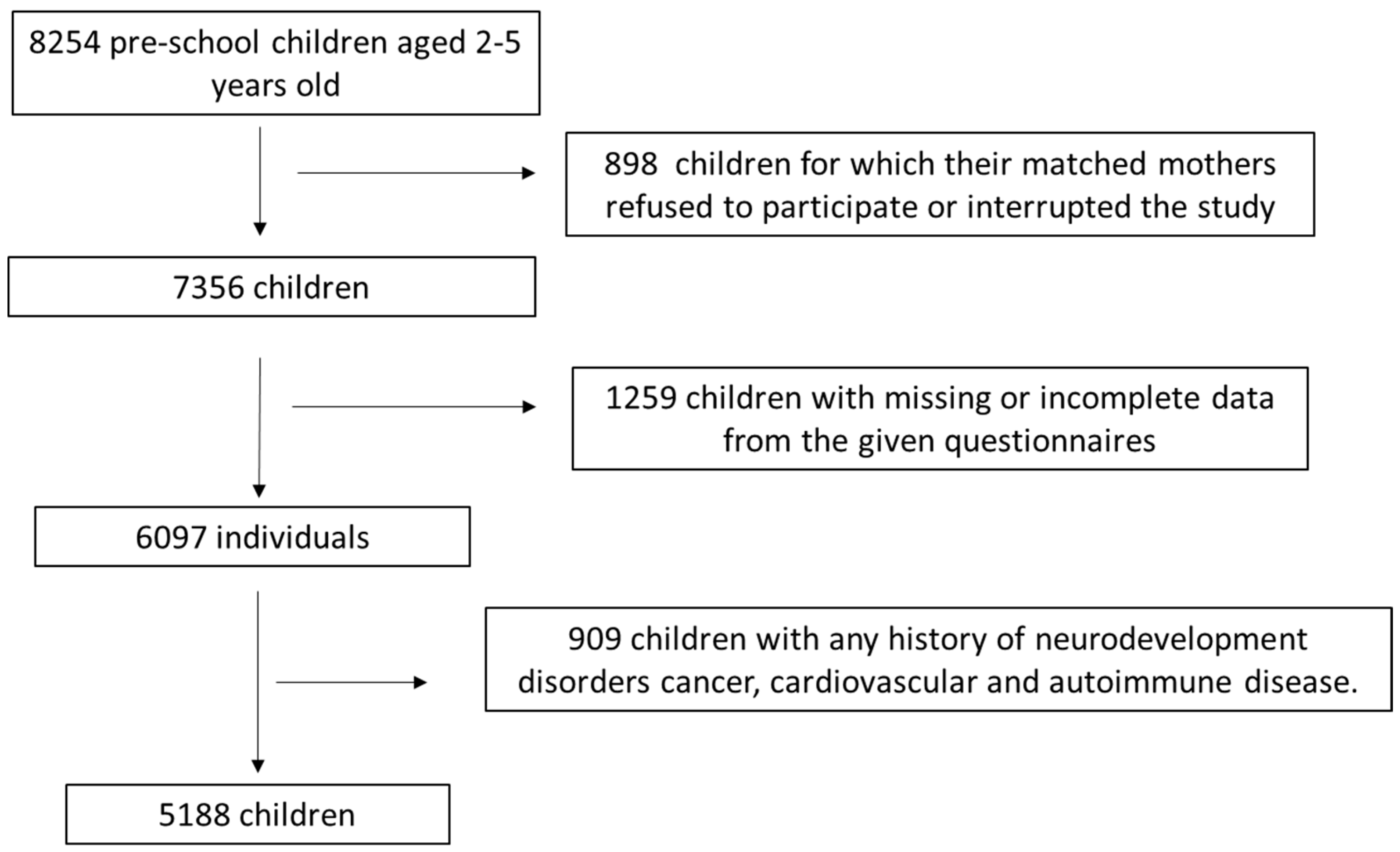
2.1. Study Population
2.2. Study Design
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics of the Study Population
3.2. Association of Children MD Adherence with Sociodemographic and Anthropometric Characteristics
3.3. Association of Childhood MD Adherence with Lifestyle Factors, Childhood Asthma and Diabetes Mellitus 1
3.4. Multivariate Binary Logistic Regression Analysis for MD Adherence of the Study Population
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barber, T.M.; Kabisch, S.; Pfeiffer, A.F.H.; Weickert, M.O. The Effects of the Mediterranean Diet on Health and Gut Microbiota. Nutrients 2023, 15, 2150. [Google Scholar] [CrossRef] [PubMed]
- Cenni, S.; Sesenna, V.; Boiardi, G.; Casertano, M.; Di Nardo, G.; Esposito, S.; Strisciuglio, C. The Mediterranean Diet in Paediatric Gastro-intestinal Disorders. Nutrients 2022, 15, 79. [Google Scholar] [CrossRef] [PubMed]
- Farias-Pereira, R.; Zuk, J.B.; Khavaran, H. Plant bioactive compounds from Mediterranean diet improve risk factors for metabolic syndrome. Int. J. Food Sci. Nutr. 2023, 74, 403–423. [Google Scholar] [CrossRef] [PubMed]
- Franco, G.A.; Interdonato, L.; Cordaro, M.; Cuzzocrea, S.; Di Paola, R. Bioactive Compounds of the Mediterranean Diet as Nutritional Support to Fight Neurodegenerative Disease. Int. J. Mol. Sci. 2023, 24, 7318. [Google Scholar] [CrossRef]
- Delgado, A.; Gonçalves, S.; Romano, A. Mediterranean Diet: The Role of Phenolic Compounds from Aromatic Plant Foods. Foods 2023, 12, 840. [Google Scholar] [CrossRef]
- López-Gil, J.F.; García-Hermoso, A.; Sotos-Prieto, M.; Cavero-Redondo, I.; Martínez-Vizcaíno, V.; Kales, S.N. Mediterranean Diet-Based Interventions to Improve Anthropometric and Obesity Indicators in Children and Adolescents: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2023, 14, 858–869. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Verde, L.; Sulu, C.; Katsiki, N.; Hassapidou, M.; Frias-Toral, E.; Cucalón, G.; Pazderska, A.; Yumuk, V.D.; Colao, A.; et al. Mediterranean Diet and Obesity-related Disorders: What is the Evidence? Curr. Obes. Rep. 2022, 11, 287–304. [Google Scholar] [CrossRef]
- Waltenberger, B.; Halabalaki, M.; Schwaiger, S.; Adamopoulos, N.; Allouche, N.; Fiebich, B.L.; Hermans, N.; Jansen-Dürr, P.; Kesternich, V.; Pieters, L.; et al. Novel Natural Products for Healthy Ageing from the Mediterranean Diet and Food Plants of Other Global Sources-The MediHealth Project. Molecules 2018, 23, 1097. [Google Scholar] [CrossRef]
- Poulios, E.; Koukounari, S.; Psara, E.; Vasios, G.K.; Sakarikou, C.; Giaginis, C. Anti-obesity Properties of Phytochemicals: Highlighting their Molecular Mechanisms against Obesity. Curr. Med. Chem. 2024, 31, 25–61. [Google Scholar] [CrossRef]
- Li, H.; Qi, J.; Li, L. Phytochemicals as potential candidates to combat obesity via adipose non-shivering thermogenesis. Pharmacol. Res. 2019, 147, 104393. [Google Scholar] [CrossRef]
- Borah, A.K.; Sharma, P.; Singh, A.; Kalita, K.J.; Saha, S.; Chandra Borah, J. Adipose and non-adipose perspectives of plant derived natural compounds for mitigation of obesity. J. Ethnopharmacol. 2021, 280, 114410. [Google Scholar] [CrossRef] [PubMed]
- Vourdoumpa, A.; Paltoglou, G.; Charmandari, E. The Genetic Basis of Childhood Obesity: A Systematic Review. Nutrients 2023, 15, 1416. [Google Scholar] [CrossRef]
- Onyimadu, O.; Violato, M.; Astbury, N.M.; Hüls, H.; Heath, L.; Shipley, A.; Taylor, H.; Wilkins, L.E.; Abhari, R.E.; Jebb, S.A.; et al. A systematic review of economic evaluations of interventions targeting childhood overweight and obesity. Obes. Rev. 2023, 24, e13597. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 9 June 2023).
- Zhang, Y.; Yin, Y.; Zhang, X.; Ye, J.; Zhang, J. Association of adverse childhood experiences with diabetes: A systematic review and meta-analysis. J. Diabetes Its Complicat. 2022, 36, 108289. [Google Scholar] [CrossRef] [PubMed]
- Suspitsin, E.N.; Imyanitov, E.N. Hereditary Conditions Associated with Elevated Cancer Risk in Childhood. Biochemistry 2023, 88, 880–891. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.T.; Krenek, A.; Magge, S.N. Childhood Obesity and Cardiovascular Disease Risk. Curr. Atheroscler. Rep. 2023, 25, 405–415. [Google Scholar] [CrossRef]
- Palacios-Marin, I.; Serra, D.; Jiménez-Chillarón, J.C.; Herrero, L.; Todorčević, M. Childhood obesity: Implications on adipose tissue dynamics and metabolic health. Obes. Rev. 2023, 24, e13627. [Google Scholar] [CrossRef]
- Lim, C.Y.S.; Foo, Y.W.; Tok, C.L.X.; Lim, Y.Y.; Loke, K.Y.; Lee, Y.S.; Ng, N.B.H. Screening for metabolic complications of childhood and adolescent obesity: A scoping review of national and international guidelines. Obes. Rev. 2022, 23, e13513. [Google Scholar] [CrossRef]
- Shaban Mohamed, M.A.; AbouKhatwa, M.M.; Saifullah, A.A.; Hareez Syahmi, M.; Mosaad, M.; Elrggal, M.E.; Dehele, I.S.; Elnaem, M.H. Risk Factors, Clinical Consequences, Prevention, and Treatment of Childhood Obesity. Children 2022, 9, 1975. [Google Scholar] [CrossRef]
- Pavlidou, E.; Papandreou, D.; Taha, Z.; Mantzorou, M.; Tyrovolas, S.; Kiortsis, D.N.; Psara, E.; Papadopoulou, S.K.; Yfantis, M.; Spanoudaki, M.; et al. Association of Maternal Pre-Pregnancy Overweight and Obesity with Childhood Anthropometric Factors and Perinatal and Postnatal Outcomes: A Cross-Sectional Study. Nutrients 2023, 15, 3384. [Google Scholar] [CrossRef]
- Zhou, J.; Zeng, L.; Wang, D.; Li, C.; Liu, Y.; Yan, H.; Xiao, Y. Effects of birth weight on body composition and overweight/obesity at early school age. Clin. Nutr. 2019, 39, 1778–1784. [Google Scholar] [CrossRef] [PubMed]
- Koutelidakis, A.E.; Alexatou, O.; Kousaiti, S.; Gkretsi, E.; Vasios, G.; Sampani, A.; Tolia, M.; Kiortsis, D.N.; Giaginis, C. Higher adherence to Mediterranean diet prior to pregnancy is associated with decreased risk for deviation from the maternal recommended gestational weight gain. Int. J. Food Sci. Nutr. 2018, 69, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Xia, W.; Li, Y.; Xu, S.; Zhang, Y. Associations of Gestational Weight Gain Rate during Different Trimesters with Early-Childhood Body Mass Index and Risk of Obesity. Obesity 2020, 28, 1941–1950. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.J.; Yu, J.; Choi, J. Maternal Pre-Pregnancy Obesity and Gestational Diabetes Mellitus Increase the Risk of Childhood Obesity. Children 2022, 9, 928. [Google Scholar] [CrossRef] [PubMed]
- Mantzorou, M.; Papandreou, D.; Pavlidou, E.; Papadopoulou, S.K.; Tolia, M.; Mentzelou, M.; Poutsidi, A.; Antasouras, G.; Vasios, G.K.; Giaginis, C. Maternal Gestational Diabetes Is Associated with High Risk of Childhood Overweight and Obesity: A Cross-Sectional Study in Pre-School Children Aged 2–5 Years. Medicina 2023, 59, 455. [Google Scholar] [CrossRef]
- Kang, H.-T.; Ju, Y.-S.; Park, K.-H.; Kwon, Y.-J.; Im, H.-J.; Paek, D.-M.; Lee, H.-J. Study on the relationship between childhood obesity and various determinants, including socioeconomic factors, in an urban area. J. Prev. Med. Public Health 2006, 39, 371–378. [Google Scholar] [PubMed]
- Lee, E.Y.; Yoon, K.H. Epidemic obesity in children and adolescents: Risk factors and prevention. Front. Med. 2018, 12, 658–666. [Google Scholar] [CrossRef]
- Storz, M.A. The COVID-19 pandemic: An unprecedented tragedy in the battle against childhood obesity. Clin. Exp. Pediatr. 2020, 63, 477–482. [Google Scholar] [CrossRef]
- Ferentinou, E.; Koutelekos, I.; Pappa, D.; Manthou, P.; Dafogianni, C. The Impact of the COVID-19 Pandemic on Childhood Obesity: A Review. Cureus 2023, 15, e45470. [Google Scholar] [CrossRef]
- Paul, I.M.; Savage, J.S.; Anzman-Frasca, S.; Marini, M.E.; Beiler, J.S.; Hess, L.B.; Loken, E.; Birch, L.L. Effect of a responsive parenting educational intervention on childhood weight outcomes at 3 years of age: The INSIGHT randomized clinical trial. JAMA 2018, 320, 461. [Google Scholar] [CrossRef]
- Eichner-Seitz, N.; Pate, R.R.; Paul, I.M. Physical activity in infancy and early childhood: A narrative review of interventions for prevention of obesity and associated health outcomes. Front. Endocrinol. 2023, 14, 1155925. [Google Scholar] [CrossRef] [PubMed]
- Lakshman, R.; Elks, C.E.; Ong, K.K. Childhood Obesity. Circulation 2012, 126, 1770–1779. [Google Scholar] [CrossRef] [PubMed]
- Flynn, A.C.; Suleiman, F.; Windsor-Aubrey, H.; Wolfe, I.; O’Keeffe, M.; Poston, L.; Dalrymple, K.V. Preventing and treating childhood overweight and obesity in children up to 5 years old: A systematic review by intervention setting. Matern. Child Nutr. 2022, 18, e13354. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cai, L.; Wu, Y.; Wilson, R.F.; Weston, C.; Fawole, O.; Bleich, S.N.; Cheskin, L.J.; Showell, N.N.; Lau, B.D.; et al. What childhood obesity prevention programmes work? A systematic review and meta-analysis. Obes. Rev. 2015, 16, 547–565. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Vercammen, K.A.; Zatz, L.Y.; Frelier, J.M.; Ebbeling, C.B.; Peeters, A. Interventions to prevent global childhood overweight and obesity: A systematic review. Lancet Diabetes Endocrinol. 2018, 6, 332–346. [Google Scholar] [CrossRef] [PubMed]
- Fornari, E.; Brusati, M.; Maffeis, C. Nutritional Strategies for Childhood Obesity Prevention. Life 2021, 11, 532. [Google Scholar] [CrossRef] [PubMed]
- Blake-Lamb, T.L.; Locks, L.M.; Perkins, M.E.; Woo Baidal, J.A.; Cheng, E.R.; Taveras, E.M. Interventions for Childhood Obesity in the First 1000 Days. A Systematic Review. Am. J. Prev. Med. 2016, 50, 780–789. [Google Scholar] [CrossRef]
- Pereira, A.R.; Oliveira, A. Dietary Interventions to Prevent Childhood Obesity: A Literature Review. Nutrients 2021, 13, 3447. [Google Scholar] [CrossRef]
- Psaltopoulou, T.; Tzanninis, S.; Ntanasis-Stathopoulos, I.; Panotopoulos, G.; Kostopoulou, M.; Tzanninis, I.G.; Tsagianni, A.; Sergentanis, T.N. Prevention and treatment of childhood and adolescent obesity: A systematic review of meta-analyses. World J. Pediatr. 2019, 15, 350–381. [Google Scholar] [CrossRef]
- Garrido-Miguel, M.; Oliveira, A.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Pozuelo-Carrascosa, D.P.; Soriano-Cano, A.; Martínez-Vizcaíno, V. Prevalence of Overweight and Obesity among European Preschool Children: A Systematic Review and Meta-Regression by Food Group Consumption. Nutrients 2019, 11, 1698. [Google Scholar] [CrossRef]
- Campbell, M.K. Biological, environmental, and social influences on childhood obesity. Pediatr. Res. 2016, 79, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Mantzorou, M.; Papandreou, D.; Vasios, G.K.; Pavlidou, E.; Antasouras, G.; Psara, E.; Taha, Z.; Poulios, E.; Giaginis, C. Exclusive Breastfeeding for at Least Four Months Is Associated with a Lower Prevalence of Overweight and Obesity in Mothers and Their Children after 2–5 Years from Delivery. Nutrients 2022, 14, 3599. [Google Scholar] [CrossRef] [PubMed]
- Papandreou, D.; Mantzorou, M.; Tyrovolas, S.; Pavlidou, E.; Antasouras, G.; Psara, E.; Poulios, E.; Vasios, G.K.; Giaginis, C. Pre-Pregnancy Excess Weight Association with Maternal Sociodemographic, Anthropometric and Lifestyle Factors and Maternal Perinatal Outcomes. Nutrients 2022, 14, 3810. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The World Health Report: 2006: Working Together for Health; World Health Organization: Geneva, Switzerland, 2006; Available online: https://apps.who.int/iris/handle/10665/43432 (accessed on 18 July 2023).
- Jamesm, W.P. WHO recognition of the global obesity epidemic. Int J Obes. 2008, 32, S120–S126. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation, Geneva, 8–11 December 2008; World Health Organization: Geneva, Switzerland, 2011; Available online: https://apps.who.int/iris/handle/10665/44583 (accessed on 18 July 2023).
- Ahmad, N.; Adam, S.I.M.; Nawi, A.M.; Hassan, M.R.; Ghazi, H.F. Abdominal Obesity Indicators: Waist Circumference or Waist-to-hip Ratio in Malaysian Adults Population. Int. J. Prev. Med. 2016, 7, 82. [Google Scholar] [CrossRef] [PubMed]
- Pray, R.; Riskin, S. The History and Faults of the Body Mass Index and Where to Look Next: A Literature Review. Cureus 2023, 15, e48230. [Google Scholar] [CrossRef] [PubMed]
- Yanga, F.; Lv, J.H.; Lei, S.F.; Chena, X.D. Receiver-operating characteristic analyses of body mass index, waist circumference and waist-to-hip ratio for obesity: Screening in young adults in central south of China. Clin. Nutr. 2006, 25, 1030–1039. [Google Scholar] [CrossRef]
- Cheng, C.H.; Ho, C.C.; Yang, C.F.; Huang, Y.C.; Lai, C.H.; Liaw, Y.P. Waist-to-hip ratio is a better anthropometric index than body mass index for predicting the risk of type 2 diabetes in Taiwanese population. Nutr. Res. 2010, 30, 585–593. [Google Scholar] [CrossRef]
- Bacci, S.; Bartolucci, F.; Chiavarini, M.; Minelli, L.; Pieroni, L. Differences in birthweight outcomes: A longitudinal study based on siblings. Int. J. Environ. Res. Public Health 2014, 11, 6472–6484. [Google Scholar] [CrossRef]
- Dwyer, G.M.; Hardy, L.L.; Peat, J.K.; Baur, L.A. The validity and reliability of a home environment preschool-age physical activity questionnaire (Pre-PAQ). Int. J. Behav. Nutr. Phys. Act. 2011, 8, 86. [Google Scholar] [CrossRef]
- Gkoltsiou, K.; Dimitrakaki, C.; Tzavara, C.; Papaevangelou, V.; Varni, J.W.; Tountas, Y. Measuring health-related quality of life in Greek children: Psychometric properties of the Greek version of the Pediatric Quality of Life Inventory (TM) 4.0 Generic Core Scales. Qual. Life Res. 2008, 17, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Lichtlé, J.; Devouche, E.; Downes, N.; Mottron, L.; Cappe, E. Psychometric validation of the French version of the PedsQLTM4.0 generic health-related quality of life questionnaire for 2–4-year-old children. Eur. J. Pediatr. 2023, 182, 1213–1219. [Google Scholar] [CrossRef] [PubMed]
- Štefan, L.; Prosoli, R.; Juranko, D.; Čule, M.; Milinović, I.; Novak, D.; Sporiš, G. The Reliability of the Mediterranean Diet Quality Index (KIDMED) Questionnaire. Nutrients 2017, 9, 419. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.I.; Keil, U.; Anderson, H.R.; Beasley, R.; Crane, J.; Martinez, F.; Mitchell, E.A.; Pearce, N.; Sibbald, B.; Stewart, A.W.; et al. International Study of Asthma and Allergies in Childhood (ISAAC): Rationale and methods. Eur. Respir. J. 1995, 8, 483–491. [Google Scholar] [CrossRef]
- Rosa, M.J.; Hartman, T.J.; Adgent, M.; Gardner, K.; Gebretsadik, T.; Moore, P.E.; Davis, R.L.; LeWinn, K.Z.; Bush, N.R.; Tylavsky, F.; et al. Prenatal polyunsaturated fatty acids and child asthma: Effect modification by maternal asthma and child sex. J. Allergy Clin. Immunol. 2020, 145, 800–807.e4. [Google Scholar] [CrossRef]
- Kanellopoulou, A.; Giannakopoulou, S.P.; Notara, V.; Antonogeorgos, G.; Rojas-Gil, A.P.; Kornilaki, E.N.; Konstantinou, E.; Lagiou, A.; Panagiotakos, D.B. The association between adherence to the Mediterranean diet and childhood obesity; the role of family structure: Results from an epidemiological study in 1728 Greek students. Nutr. Health 2021, 27, 39–47. [Google Scholar] [CrossRef]
- Kosti, R.I.; Kanellopoulou, A.; Fragkedaki, E.; Notara, V.; Giannakopoulou, S.P.; Antonogeorgos, G.; Rojas-Gil, A.P.; Kornilaki, E.N.; Lagiou, A.; Panagiotakos, D.B. The Influence of Adherence to the Mediterranean Diet among Children and Their Parents in Relation to Childhood Overweight/Obesity: A Cross-Sectional Study in Greece. Child Obes. 2020, 16, 571–578. [Google Scholar] [CrossRef]
- Farajian, P.; Risvas, G.; Karasouli, K.; Pounis, G.D.; Kastorini, C.M.; Panagiotakos, D.B.; Zampelas, A. Very high childhood obesity prevalence and low adherence rates to the Mediterranean diet in Greek children: The GRECO study. Atherosclerosis 2011, 217, 525–530. [Google Scholar] [CrossRef]
- Lazarou, C.; Panagiotakos, D.B.; Matalas, A.L. Physical activity mediates the protective effect of the Mediterranean diet on children’s obesity status: The CYKIDS study. Nutrition 2010, 26, 61–67. [Google Scholar] [CrossRef]
- Wu, Y.X.; Fan, H.L.; Dai, J.; Wu, H.L.; Yang, J.Y.; Wang, Y.; Tung, T.H.; Wang, L.Z.; Zhang, M.X. Analysis of association between eating behaviours and childhood obesity among pre-school children: A cross-sectional study. Front. Pediatr. 2023, 10, 1073711. [Google Scholar] [CrossRef]
- von Kries, R.; Beyerlein, A.; Müller, M.; Heinrich, J.; Landsberg, B.; Bolte, G.; Chmitorz, A.; Plachta-Danielzik, S. Different age-specific incidence and remission rates in pre-school and primary school suggest need for targeted obesity prevention in childhood. Int. J. Obes. 2012, 36, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Gewa, C.A. Childhood overweight and obesity among Kenyan pre-school children: Association with maternal and early child nutritional factors. Public Health Nutr. 2010, 13, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Miguel-Berges, M.L.; Mouratidou, T.; Santaliestra-Pasias, A.; Androutsos, O.; Iotova, V.; Galcheva, S.; De Craemer, M.; Cardon, G.; Koletzko, B.; Kulaga, Z.; et al. Longitudinal associations between diet quality, sedentary behaviours and physical activity and risk of overweight and obesity in preschool children: The ToyBox-study. Pediatr. Obes. 2023, 18, e13068. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Wang, H.; Wu, H. Association between diet quality scores and risk of overweight and obesity in children and adolescents. BMC Pediatr. 2023, 23, 169. [Google Scholar] [CrossRef] [PubMed]
- Oliver Olid, A.; Moreno-Galarraga, L.; Moreno-Villares, J.M.; Bibiloni, M.D.M.; Martínez-González, M.Á.; de la O, V.; Fernandez-Montero, A.; Martín-Calvo, N. Breastfeeding Is Associated with Higher Adherence to the Mediterranean Diet in a Spanish Population of Preschoolers: The SENDO Project. Nutrients 2023, 15, 1278. [Google Scholar] [CrossRef]
- Martíncrespo-Blanco, M.C.; Varillas-Delgado, D.; Blanco-Abril, S.; Cid-Exposito, M.G.; Robledo-Martín, J. Effectiveness of an Intervention Programme on Adherence to the Mediterranean Diet in a Preschool Child: A Randomised Controlled Trial. Nutrients 2022, 14, 1536. [Google Scholar] [CrossRef]
- Latorre-Román, P.Á.; Guzmán-Guzmán, I.P.; Párraga-Montilla, J.A.; Caamaño-Navarrete, F.; Salas-Sánchez, J.; Palomino-Devia, C.; Reyes-Oyola, F.A.; Álvarez, C.; de la Casa-Pérez, A.; Cardona Linares, A.J.; et al. Healthy lifestyles and physical fitness are associated with abdominal obesity among Latin-American and Spanish preschool children: A cross-cultural study. Pediatr. Obes. 2022, 17, e12901. [Google Scholar] [CrossRef]
- Caamaño-Navarrete, F.; Guzmán-Guzmán, I.P.; Palomino-Devia, C.; Reyes-Oyola, F.A.; Bustos-Barahona, R.; Jerez-Mayorga, D.; Delgado-Floody, P. The association between modifiable lifestyle behaviour in Latin-American schoolchildren with abdominal obesity and excess weight. A comparison of Chile and Colombia. Endocrinol. Diabetes Nutr. 2022, 69, 4–14. [Google Scholar] [CrossRef]
- Bučan Nenadić, D.; Kolak, E.; Selak, M.; Smoljo, M.; Radić, J.; Vučković, M.; Dropuljić, B.; Pijerov, T.; Babić Cikoš, D. Anthropometric Parameters and Mediterranean Diet Adherence in Preschool Children in Split-Dalmatia County, Croatia-Are They Related? Nutrients 2021, 13, 4252. [Google Scholar] [CrossRef]
- Sanlier, N.; Ulusoy, H.G.; Kocabaş, S.; Çelik, B.; Göbel, P.; Yilmaz, S. Mediterranean Diet Adherence among Preschoolers and its Association with Parents’ Beliefs, Attitudes, and Practices. Ecol. Food Nutr. 2021, 60, 225–243. [Google Scholar] [CrossRef]
- Sørensen, L.M.N.; Aamodt, G.; Brantsæter, A.L.; Meltzer, H.M.; Papadopoulou, E. Diet quality of Norwegian children at 3 and 7 years: Changes, predictors and longitudinal association with weight. Int. J. Obes. 2022, 46, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Notario-Barandiaran, L.; Valera-Gran, D.; Gonzalez-Palacios, S.; Garcia-de-la-Hera, M.; Fernández-Barrés, S.; Pereda-Pereda, E.; Fernández-Somoano, A.; Guxens, M.; Iñiguez, C.; Romaguera, D.; et al. High adherence to a mediterranean diet at age 4 reduces overweight, obesity and abdominal obesity incidence in children at the age of 8. Int. J. Obes. 2020, 44, 1906–1917. [Google Scholar] [CrossRef] [PubMed]
- Katsagoni, C.N.; Psarra, G.; Georgoulis, M.; Tambalis, K.; Panagiotakos, D.B.; Sidossis, L.S.; EYZHN Study Group. High and moderate adherence to Mediterranean lifestyle is inversely associated with overweight, general and abdominal obesity in children and adolescents: The MediLIFE-index. Nutr. Res. 2020, 73, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Labayen Goñi, I.; Arenaza, L.; Medrano, M.; García, N.; Cadenas-Sanchez, C.; Ortega, F.B. Associations between the adherence to the Mediterranean diet and cardiorespiratory fitness with total and central obesity in preschool children: The PREFIT project. Eur. J. Nutr. 2018, 57, 2975–2983. [Google Scholar] [CrossRef] [PubMed]
- Pereira-da-Silva, L.; Rêgo, C.; Pietrobelli, A. The Diet of Preschool Children in the Mediterranean Countries of the European Union: A Systematic Review. Int. J. Environ. Res. Public Health 2016, 13, 572. [Google Scholar] [CrossRef] [PubMed]
- Calatayud-Sáez, F.M.; Calatayud Moscoso Del Prado, B.; Gallego Fernández-Pacheco, J.G.; González-Martín, C.; Alguacil Merino, L.F. Mediterranean diet and childhood asthma. Allergol. Immunopathol. 2016, 44, 99–105. [Google Scholar] [CrossRef]
- Castro-Rodriguez, J.A.; Ramirez-Hernandez, M.; Padilla, O.; Pacheco-Gonzalez, R.M.; Pérez-Fernández, V.; Garcia-Marcos, L. Effect of foods and Mediterranean diet during pregnancy and first years of life on wheezing, rhinitis and dermatitis in preschoolers. Allergol. Immunopathol. 2016, 44, 400–409. [Google Scholar] [CrossRef]
- Koumpagioti, D.; Boutopoulou, B.; Moriki, D.; Priftis, K.N.; Douros, K. Does Adherence to the Mediterranean Diet Have a Protective Effect against Asthma and Allergies in Children? A Systematic Review. Nutrients 2022, 14, 1618. [Google Scholar] [CrossRef]
- Dominguez-Riscart, J.; Buero-Fernandez, N.; Garcia-Zarzuela, A.; Morales-Perez, C.; Garcia-Ojanguren, A.; Lechuga-Sancho, A.M. Adherence to Mediterranean Diet Is Associated with Better Glycemic Control in Children with Type 1 Diabetes: A Cross-Sectional Study. Front. Nutr. 2022, 9, 813989. [Google Scholar] [CrossRef]
- López-Gajardo, M.A.; Leo, F.M.; Sánchez-Miguel, P.A.; López-Gajardo, D.; Soulas, C.; Tapia-Serrano, M.A. KIDMED 2.0, An update of the KIDMED questionnaire: Evaluation of the psychometric properties in youth. Front. Nutr. 2022, 9, 945721. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics (n = 5188) | Descriptive Statistics |
|---|---|
| Age (mean ± SD; years) | 4.1 ± 1.5 |
| Sex (n, %) | |
| Boys | 2546 (49.1%) |
| Girls | 2642 (50.9%) |
| Nationality (n, %) | |
| Greek | 4938 (95.2%) |
| Other | 250 (4.8%) |
| Type of residence (n, %) | |
| Urban | 3399 (65.5%) |
| Rural | 1789 (34.5%) |
| BMI (n, %) | |
| Normal weight | 3934 (75.8%) |
| Overweight | 880 (17.0%) |
| Obese | 374 (7.2%) |
| Abdominal obesity status (WtHR) (n, %) | |
| No | 4244 (81.8%) |
| Yes | 944 (18.2%) |
| Abdominal obesity status (WC) (n, %) | |
| No | 4076 (78.6%) |
| Yes | 1112 (21.4%) |
| Birth weight (n, %) | |
| Low child weight (<2500 gr) | 436 (8.4%) |
| Normal child weight (2500–4000 gr) | 4391 (84.6%) |
| High child weight (>4000 gr) | 361 (7.0%) |
| Physical activity 1 (n, %) | |
| Low | 2368 (45.6%) |
| Medium | 2169 (41.8%) |
| High | 651 (12.6%) |
| Quality of life 2 (mean score ± SD) | 68.5 ± 7.1 |
| Exclusive breastfeeding (n, %) | |
| No | 2549 (49.1%) |
| Yes | 2639 (50.9%) |
| Asthma (n, %) | |
| No | 4795 (92.4%) |
| Yes | 393 (7.6%) |
| Diabetes type 1 (n, %) | |
| No | 4851 (93.5%) |
| Yes | 337 (6.5%) |
| MD adherence 3 (n, %) | |
| Low | 2164 (41.7%) |
| Moderate | 1890 (36.4%) |
| High | 1134 (21.9%) |
| Characteristics (n = 5188) | Mediterranean Diet Adherence 1 | |||
|---|---|---|---|---|
| Low 2164 (41.7%) | Moderate 1890 (36.4%) | High 1134 (21.9%) | p-Value | |
| Age (mean ± SD; years) | 7.61 ± 1.06 | 7.58 ± 1.09 | 7.56 ± 1.08 | p = 0.2391 |
| Sex (n, %) | p = 0.0005 | |||
| Boys | 986 (45.6%) | 958 (50.7%) | 602 (53.1%) | |
| Girls | 1178 (54.4%) | 932 (49.3%) | 532 (46.9%) | |
| Nationality (n, %) | p = 0.0088 | |||
| Greek | 2038 (94.2%) | 1806 (95.6%) | 1094 (96.5%) | |
| Other | 126 (5.8%) | 84 (4.4%) | 40 (3.5%) | |
| Type of residence (n, %) | p = 0.0099 | |||
| Urban | 1478 (68.3%) | 1214 (64.2%) | 707 (62.3%) | |
| Rural | 686 (31.7%) | 676 (35.8%) | 427 (37.7%) | |
| BMI (n, %) | p < 0.0001 | |||
| Normal weight | 1205 (55.7%) | 1677 (88.7%) | 1052 (92.8%) | |
| Overweight | 669 (30.9%) | 148 (7.8%) | 63 (5.5%) | |
| Obese | 290 (13.4%) | 65 (3.5%) | 19 (1.7%) | |
| Abdominal obesity (WtHR) (n, %) | p < 0.0001 | |||
| No | 1547 (71.5%) | 1657 (87.7%) | 1040 (91.7%) | |
| Yes | 617 (28.5%) | 233 (12.3%) | 94 (8.3%) | |
| Abdominal obesity (WC) (n, %) | p < 0.0001 | |||
| No | 1466 (67.7%) | 1598 (84.5%) | 1012 (89.2%) | |
| Yes | 698 (32.3%) | 292 (15.5%) | 122 (10.8%) | |
| Birth weight (n, %) | p < 0.0001 | |||
| Low (<2500 gr) | 212 (9.8%) | 159 (8.4%) | 110 (9.7%) | |
| Normal (2500–4000 gr) | 1655 (76.5%) | 1629 (86.2%) | 971 (85.6%) | |
| High (>4000 gr) | 297 (13.7%) | 102 (5.4%) | 53 (4.7%) | |
| Physical activity 2 (n, %) | p = 0.0041 | |||
| Low | 1003 (46.4%) | 870 (46.0%) | 495 (43.6%) | |
| Medium | 918 (42.4%) | 792 (41.9%) | 459 (40.5%) | |
| High | 243 (11.2%) | 228 (12.1%) | 180 (15.9%) | |
| Quality of life 3 (mean score ± SD) | 61 ± 6.8 | 67.9 ± 7.2 | 73.4 ± 7.5 | p = 0.0008 |
| Exclusive breastfeeding (n, %) | p < 0.0001 | |||
| No | 1156 (53.4%) | 882 (46.7%) | 511 (45.1%) | |
| Yes | 1008 (46.6%) | 1008 (53.3%) | 623 (54.9%) | |
| Asthma (n, %) | p = 0.0001 | |||
| No | 1942 (89.7%) | 1776 (94.0%) | 1077 (95.0%) | |
| Yes | 222 (10.3%) | 114 (6.0%) | 57 (5.0%) | |
| Diabetes type 1 (n, %) | p = 0.0002 | |||
| No | 1991 (92.0%) | 1776 (94.0%) | 1084 (95.6%) | |
| Yes | 173 (8.0%) | 114 (6.0%) | 50 (4.4%) | |
| Characteristics | Mediterranean Diet Adherence 1 (Low vs. Moderate & High) | |
|---|---|---|
| OR * (95% CI **) | p-Value | |
| Age (Over/Below mean value) | 0.98 (0.23–1.74) | p = 0.57483 |
| Gender (Male/Female) | 1.27 (0.64–1.91) | p = 0.1728 |
| Nationality (Greek/Other) | 1.18 (0.61–1.86) | p = 0.2011 |
| Type of residence (Rural/Urban) | 1.32 (0.68–1.97) | p = 0.2879 |
| BMI (Overweight & Obese/Normal weight) | 2.27 (1.98–2.59) | p = 0.0024 |
| Abdominal obesity (WtHR) (No/Yes) | 2.02 (1.78–2.31) | p = 0.0021 |
| Abdominal obesity (WC) (No/Yes) | 1.98 (1.75–2.24) | p = 0.0038 |
| Birth weight (Low & normal/High) | 1.88 (1.37–2.39) | p = 0.1563 |
| Physical activity 2 (Low/Medium & High) | 1.57 (1.21–1.98) | p = 0.0175 |
| Quality of life 3 (Below/Over mean value) | 2.08 (1.85–2.31) | p = 0.0086 |
| Exclusive breastfeeding (No/Yes) | 2.19 (1.98–2.35) | p = 0.0056 |
| Asthma (No/Yes) | 1.69 (1.34–2.03) | p = 0.0182 |
| Diabetes type 1 (No/Yes) | 1.48 (1.13–1.86) | p = 0.0289 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavlidou, E.; Papadopoulou, S.K.; Alexatou, O.; Voulgaridou, G.; Mentzelou, M.; Biskanaki, F.; Psara, E.; Tsourouflis, G.; Lefantzis, N.; Dimoliani, S.; et al. Childhood Mediterranean Diet Adherence Is Associated with Lower Prevalence of Childhood Obesity, Specific Sociodemographic, and Lifestyle Factors: A Cross-Sectional Study in Pre-School Children. Epidemiologia 2024, 5, 11-28. https://doi.org/10.3390/epidemiologia5010002
Pavlidou E, Papadopoulou SK, Alexatou O, Voulgaridou G, Mentzelou M, Biskanaki F, Psara E, Tsourouflis G, Lefantzis N, Dimoliani S, et al. Childhood Mediterranean Diet Adherence Is Associated with Lower Prevalence of Childhood Obesity, Specific Sociodemographic, and Lifestyle Factors: A Cross-Sectional Study in Pre-School Children. Epidemiologia. 2024; 5(1):11-28. https://doi.org/10.3390/epidemiologia5010002
Chicago/Turabian StylePavlidou, Eleni, Sousana K. Papadopoulou, Olga Alexatou, Gavriela Voulgaridou, Maria Mentzelou, Fani Biskanaki, Evmorfia Psara, Gerasimos Tsourouflis, Nikos Lefantzis, Sophia Dimoliani, and et al. 2024. "Childhood Mediterranean Diet Adherence Is Associated with Lower Prevalence of Childhood Obesity, Specific Sociodemographic, and Lifestyle Factors: A Cross-Sectional Study in Pre-School Children" Epidemiologia 5, no. 1: 11-28. https://doi.org/10.3390/epidemiologia5010002
APA StylePavlidou, E., Papadopoulou, S. K., Alexatou, O., Voulgaridou, G., Mentzelou, M., Biskanaki, F., Psara, E., Tsourouflis, G., Lefantzis, N., Dimoliani, S., Apostolou, T., Sampani, A., Chatziprodromidou, I. P., Angelakou, E. -P., & Giaginis, C. (2024). Childhood Mediterranean Diet Adherence Is Associated with Lower Prevalence of Childhood Obesity, Specific Sociodemographic, and Lifestyle Factors: A Cross-Sectional Study in Pre-School Children. Epidemiologia, 5(1), 11-28. https://doi.org/10.3390/epidemiologia5010002