


Cannabis Use and Its Impact on Mental Health in Youth in Australia and the United States: A Scoping Review





Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Question
2.2. Eligibility
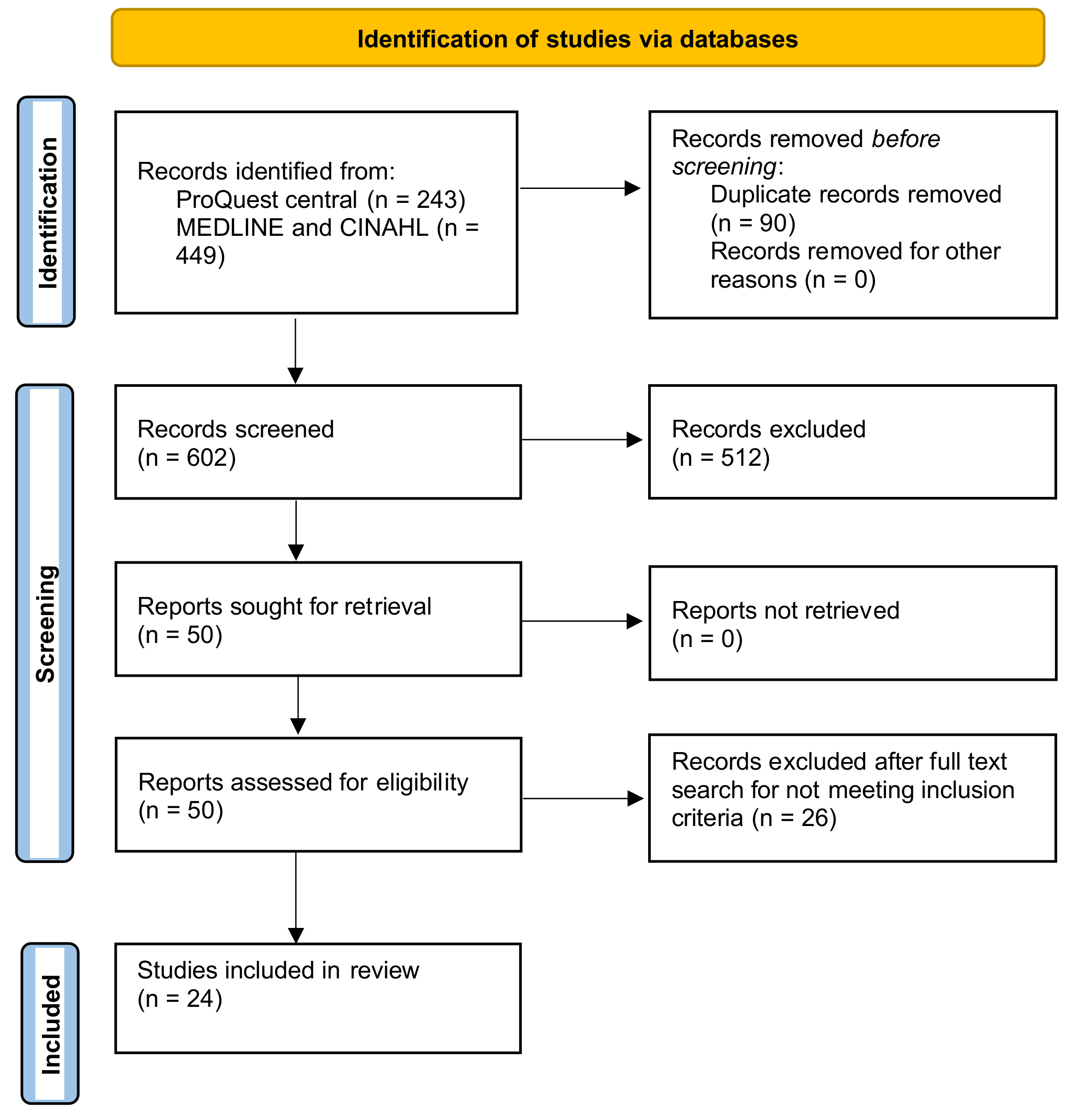
2.3. Search Strategy, Information Source, and Study Selection
- Mental health: Anxiety OR depression OR bipolar mood disorder OR psychosis OR schizophrenia OR attention deficit hyperactive disorder OR ADHD OR PTSD OR Anti-sociality disorder OR conduct Disorder OR Panic attack OR Mental disorder OR Mental*;
- Cannabis: Marijuana OR Tetra hydro cannabidiol OR THC OR pot OR bong OR joint OR cannabis;
- Young population: Adolescence OR adolescent OR young adult OR youth OR young.
2.4. Data Extraction
2.5. Thematic Analysis and Charting
3. Results
3.1. Cannabis Use among Young Population and Depression and Depressive Symptoms
3.2. Cannabis Use among Young Population and Anxiety
3.3. Cannabis Use among Young Population and Risk of Suicide, Suicidal Ideation, Plan, and Attempt
3.4. Cannabis Use among Young Population and Risk of Psychosis and Psychotic Symptoms
3.5. Cannabis Use among Young Population and Risk of Cannabis Use Disorder and Dependence
3.6. Cannabis Use and Development of Other Mental Disorder
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bauman, A.; Phongsavan, P. Epidemiology of substance use in adolescence: Prevalence, trends and policy implications. Drug Alcohol Depend. 1999, 55, 187–207. [Google Scholar] [CrossRef] [PubMed]
- Mansell, H. Selective Studies on the Challenges of Cannabis Use in Children, Youth and Young Adults; University of Saskatchewan: Saskatoon, SK, Canada, 2022. [Google Scholar]
- Haberstick, B.C.; Young, S.E.; Zeiger, J.S.; Lessem, J.M.; Hewitt, J.K.; Hopfer, C.J. Prevalence and correlates of alcohol and cannabis use disorders in the United States: Results from the national longitudinal study of adolescent health. Drug Alcohol Depend. 2014, 136, 158–161. [Google Scholar] [CrossRef] [PubMed]
- Livingston, M.; Holmes, J.; Oldham, M.; Vashishtha, R.; Pennay, A. Trends in the sequence of first alcohol, cannabis and cigarette use in Australia, 2001–2016. Drug Alcohol Depend. 2020, 207, 107821. [Google Scholar] [CrossRef]
- Iede, M.A.; Nunn, K.; Milne, B.; Fitzgerald, D.A. The consequences of chronic cannabis smoking in vulnerable adolescents. Paediatr. Respir. Rev. 2017, 24, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Hall, W.; Lynskey, M. Evaluating the public health impacts of legalizing recreational cannabis use in the United States. Addiction 2016, 111, 1764–1773. [Google Scholar] [CrossRef] [PubMed]
- Rotermann, M. What has changed since cannabis was legalized? Health Rep. 2020, 31, 11–20. [Google Scholar]
- Zaman, T.; Malowney, M.; Knight, J.; Boyd, J.W. Co-Occurrence of Substance-Related and Other Mental Health Disorders Among Adolescent Cannabis Users. J. Addict. Med. 2015, 9, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Mandelbaum, D.E.; de la Monte, S.M. Adverse structural and functional effects of marijuana on the brain: Evidence reviewed. Pediatr. Neurol. 2017, 66, 12–20. [Google Scholar] [CrossRef]
- Grotenhermen, F.; Müller-Vahl, K. Medicinal uses of marijuana and cannabinoids. Crit. Rev. Plant Sci. 2016, 35, 378–405. [Google Scholar] [CrossRef]
- Sellers, C.M.; McRoy, R.G.; O’Brien, K.H.M. Substance use and suicidal ideation among child welfare involved adolescents: A longitudinal examination. Addict. Behav. 2019, 93, 39–45. [Google Scholar] [CrossRef]
- White, C.T.; Shamim, H.; Al Shouli, R.; Habbal, A.B.; Mohammed, L. Cannabis use and the development of depression in adolescents: Is there an established linear relationship between the two? Cureus 2022, 14, e27394. [Google Scholar] [CrossRef]
- Pahl, K.; Brook, J.S.; Lee, J.Y. Adolescent self-control predicts joint trajectories of marijuana use and depressive mood into young adulthood among urban African Americans and Puerto Ricans. J. Behav. Med. 2014, 37, 675–682. [Google Scholar] [CrossRef]
- Weinberger, A.H.; Zhu, J.; Lee, J.; Anastasiou, E.; Copeland, J.; Goodwin, R.D. Cannabis use among youth in the United States, 2004–2016: Faster rate of increase among youth with depression. Drug Alcohol Depend. 2020, 209, 107894. [Google Scholar] [CrossRef]
- Knopf, A. MTF: Cannabis use with vaping goes up, cannabis smoking down. Brown Univ. Child. Adolesc. Psychopharmacol. Update 2022, 24, 5. [Google Scholar] [CrossRef]
- Khalsa, J.H.; Bunt, G.; Blum, K.; Maggirwar, S.B.; Galanter, M.; Potenza, M.N. Review: Cannabinoids as Medicinals. Curr. Addict. Rep. 2022, 9, 630–646. [Google Scholar] [CrossRef]
- Chiu, V.; Hall, W.; Chan, G.; Hides, L.; Leung, J. A Systematic Review of Trends in US Attitudes toward Cannabis Legalization. Subst. Use Misuse 2022, 57, 1052–1061. [Google Scholar] [CrossRef]
- Kaur, N.; Keyes, K.M.; Hamilton, A.D.; Chapman, C.; Livingston, M.; Slade, T.; Swift, W. Trends in cannabis use and attitudes toward legalization and use among Australians from 2001–2016: An age-period-cohort analysis. Addiction 2021, 116, 1152–1161. [Google Scholar] [CrossRef] [PubMed]
- Single, E.; Christie, P.; Ali, R. The Impact of Cannabis Decriminalisation in Australia and the United States. J. Public Health Policy 2000, 21, 157–186. [Google Scholar] [CrossRef] [PubMed]
- Khalil, H.; Peters, M.; Godfrey, C.M.; McInerney, P.; Soares, C.B.; Parker, D. An evidence-based approach to scoping reviews. Worldviews Evid.-Based Nurs. 2016, 13, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Dennhardt, S.; Apramian, T.; Lingard, L.; Torabi, N.; Arntfield, S. Rethinking research in the medical humanities: A scoping review and narrative synthesis of quantitative outcome studies. Med. Educ. 2016, 50, 285–299. [Google Scholar] [CrossRef]
- Moller, C.I.; Tait, R.J.; Byrne, D.G. Self-harm, substance use and psychological distress in the Australian general population. Addiction 2013, 108, 211–220. [Google Scholar] [CrossRef]
- McCabe, S.E.; Arterberry, B.J.; Dickinson, K.; Evans-Polce, R.J.; Ford, J.A.; Ryan, J.E.; Schepis, T.S. Assessment of Changes in Alcohol and Marijuana Abstinence, Co-Use, and Use Disorders Among US Young Adults From 2002 to 2018. JAMA Pediatr. 2021, 175, 64–72. [Google Scholar] [CrossRef]
- Knopf, A. Teen cannabis use increases risk of suicidality and depression during young adulthood. Brown Univ. Child Adolesc. Behav. Lett. 2019, 35, 3–4. [Google Scholar] [CrossRef]
- Wong, S.S.; Zhou, B.; Goebert, D.; Hishinuma, E.S. The risk of adolescent suicide across patterns of drug use: A nationally representative study of high school students in the United States from 1999 to 2009. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 1611–1620. [Google Scholar] [CrossRef]
- Horwood, L.J.; Fergusson, D.M.; Coffey, C.; Patton, G.C.; Tait, R.; Smart, D.; Letcher, P.; Silins, E.; Hutchinson, D.M. Cannabis and depression: An integrative data analysis of four Australasian cohorts. Drug Alcohol. Depend. 2012, 126, 369–378. [Google Scholar] [CrossRef]
- Floyd Campbell, L. Depression and Marijuana Use among a Sample of Urban Females: Is Stage of Development Important? Subst. Use Misuse 2018, 53, 1008–1014. [Google Scholar] [CrossRef]
- Scholes-Balog, K.E.; Hemphill, S.A.; Patton, G.C.; Toumbourou, J.W. Cannabis use and related harms in the transition to young adulthood: A longitudinal study of Australian secondary school students. J. Adolesc. 2013, 36, 519–527. [Google Scholar] [CrossRef]
- Wilkinson, A.L.; Halpern, C.T.; Herring, A.H.; Shanahan, M.; Ennett, S.T.; Hussey, J.M.; Harris, K.M. Testing Longitudinal Relationships Between Binge Drinking, Marijuana Use, and Depressive Symptoms and Moderation by Sex. J. Adolesc. Health 2016, 59, 681–687. [Google Scholar] [CrossRef]
- Richter, L.; Pugh, B.S.; Ball, S.A. Assessing the risk of marijuana use disorder among adolescents and adults who use marijuana. Am. J. Drug Alcohol Abus. 2017, 43, 247–260. [Google Scholar] [CrossRef]
- Cohn, A.; Johnson, A.; Ehlke, S.; Villanti, A.C. Characterizing substance use and mental health profiles of cigar, blunt, and non-blunt marijuana users from the National Survey of Drug Use and Health. Drug Alcohol. Depend. 2016, 160, 105–111. [Google Scholar] [CrossRef]
- Bechtold, J.; Simpson, T.; White, H.R.; Pardini, D. Chronic adolescent marijuana use as a risk factor for physical and mental health problems in young adult men. Psychol. Addict. Behav. 2015, 29, 552–563. [Google Scholar] [CrossRef]
- Welsh, J.W.; Knight, J.R.; Hou, S.S.; Malowney, M.; Schram, P.; Sherritt, L.; Boyd, J.W. Association Between Substance Use Diagnoses and Psychiatric Disorders in an Adolescent and Young Adult Clinic-Based Population. J. Adolesc. Health 2017, 60, 648–652. [Google Scholar] [CrossRef]
- Leadbeater, B.J.; Ames, M.E.; Linden-Carmichael, A.N. Age-varying effects of cannabis use frequency and disorder on symptoms of psychosis, depression and anxiety in adolescents and adults. Addiction 2019, 114, 278–293. [Google Scholar] [CrossRef]
- Chadi, N.; Li, G.; Cerda, N.; Weitzman, E.R. Depressive Symptoms and Suicidality in Adolescents Using e-Cigarettes and Marijuana: A Secondary Data Analysis From the Youth Risk Behavior Survey. J. Addict. Med. 2019, 13, 362–365. [Google Scholar] [CrossRef]
- London-Nadeau, K.; Rioux, C.; Parent, S.; Vitaro, F.; Côté, S.M.; Boivin, M.; Tremblay, R.E.; Séguin, J.R.; Castellanos-Ryan, N. Longitudinal associations of cannabis, depression, and anxiety in heterosexual and LGB adolescents. J. Abnorm. Psychol. 2021, 130, 333–345. [Google Scholar] [CrossRef]
- Phillips, K.T.; Phillips, M.M.; Duck, K.D. Factors Associated With Marijuana use and Problems Among College Students in Colorado. Subst. Use Misuse 2018, 53, 477–483. [Google Scholar] [CrossRef]
- Levy, S.; Weitzman, E.R. Acute Mental Health Symptoms in Adolescent Marijuana Users. JAMA Pediatr. 2019, 173, 185–186. [Google Scholar] [CrossRef]
- Power, E.; Sabherwal, S.; Healy, C.; O’ Neill, A.; Cotter, D.; Cannon, M. Intelligence quotient decline following frequent or dependent cannabis use in youth: A systematic review and meta-analysis of longitudinal studies. Psychol. Med. 2021, 51, 194–200. [Google Scholar] [CrossRef]
- Gobbi, G.; Atkin, T.; Zytynski, T.; Wang, S.; Askari, S.; Boruff, J.; Ware, M.; Marmorstein, N.; Cipriani, A.; Dendukuri, N.; et al. Association of Cannabis Use in Adolescence and Risk of Depression, Anxiety, and Suicidality in Young Adulthood: A Systematic Review and Meta-analysis. JAMA Psychiatry 2019, 76, 426–434. [Google Scholar] [CrossRef]
- Han, B.; Compton, W.M.; Einstein, E.B.; Volkow, N.D. Associations of Suicidality Trends With Cannabis Use as a Function of Sex and Depression Status. JAMA Netw. Open 2021, 4, e2113025. [Google Scholar] [CrossRef]
- Meier, M.H.; Beardslee, J.; Pardini, D. Associations between Recent and Cumulative Cannabis Use and Internalizing Problems in Boys from Adolescence to Young Adulthood. J. Abnorm. Child Psychol. 2020, 48, 771–782. [Google Scholar] [CrossRef]
- Chimoriya, R.; Mohammad, Y.; Thomson, R.; Webster, C.; Dunne, R.; Aibangbee, M.; Ip, D.; Slewa-Younan, S. Mental illness stigma and associated factors among Arabic-speaking refugee and migrant populations in Australia. Int. J. Ment. Health Syst. 2023, 17, 11. [Google Scholar] [CrossRef]
- Douglass, C.H.; Win, T.M.; Goutzamanis, S.; Lim, M.S.C.; Block, K.; Onsando, G.; Hellard, M.; Higgs, P.; Livingstone, C.; Horyniak, D. Stigma Associated with Alcohol and Other Drug Use Among People from Migrant and Ethnic Minority Groups: Results from a Systematic Review of Qualitative Studies. J. Immigr. Minor. Health 2023, 25, 1402–1425. [Google Scholar] [CrossRef]
- GBD 2016 Alcohol and Drug Use Collaborators. The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry 2018, 5, 987–1012. [Google Scholar] [CrossRef]
- Mahone, I.H.; Farrell, S.; Hinton, I.; Johnson, R.; Moody, D.; Rifkin, K.; Moore, K.; Becker, M.; Barker, M.R. Shared decision making in mental health treatment: Qualitative findings from stakeholder focus groups. Arch. Psychiatr. Nurs. 2011, 25, e27–e36. [Google Scholar] [CrossRef]
- Tiruneh, Y.M.; Elliott, K.S.; Oyer, L.; Elueze, E.; Casanova, V. Addressing Substance Use and Misuse in East Texas: Stakeholder-Driven Needs and Priorities. Int. J. Environ. Res. Public. Health 2022, 19, 5215. [Google Scholar] [CrossRef]
- Aarons, G.A.; Wells, R.S.; Zagursky, K.; Fettes, D.L.; Palinkas, L.A. Implementing Evidence-Based Practice in Community Mental Health Agencies: A Multiple Stakeholder Analysis. Am. J. Public Health 2009, 99, 2087–2095. [Google Scholar] [CrossRef]
- Haller, D.M.; Meynard, A.; Lefebvre, D.; Hasselgård-Rowe, J.; Broers, B.; Narring, F. Excessive substance use among young people consulting family doctors: A cross-sectional study. Fam. Pract. 2015, 32, 500–504. [Google Scholar] [CrossRef]
- Turner, S.D.; Spithoff, S.; Kahan, M. Approach to cannabis use disorder in primary care: Focus on youth and other high-risk users. Can. Fam. Physician 2014, 60, 801–808.e423-832. [Google Scholar]
- Shi, L.; Stevens, G.D. Vulnerable Populations in the United States; John Wiley & Sons: Hoboken, NJ, USA, 2021. [Google Scholar]
- Steinberg, K.L.; Roffman, R.A.; Carroll, K.M.; Kabela, E.; Kadden, R.; Miller, M.; Duresky, D.; Marijuana Treatment Project Research Group. Tailoring cannabis dependence treatment for a diverse population. Addiction 2002, 97, 135–142. [Google Scholar] [CrossRef]
- Hyshka, E. Applying a social determinants of health perspective to early adolescent cannabis use–An overview. Drugs Educ. Prev. Policy 2013, 20, 110–119. [Google Scholar] [CrossRef]
- Rana, K.; Shrestha, V.; Chimoriya, R. The effect of housing on health and challenges of demographic changes. Glob. J. Sci. Front. Res. 2020, 20, 75–82. [Google Scholar]
- Amanda, R.; Rana, K.; Saunders, P.; Tracy, M.; Bridges, N.; Poudel, P.; Arora, A. Evaluation of the usability, content, readability and cultural appropriateness of online alcohol and other drugs resources for Aboriginal and Torres Strait Islander Peoples in New South Wales, Australia. BMJ Open 2023, 13, e069756. [Google Scholar] [CrossRef]
- Connery, H.S.; McHugh, R.K.; Reilly, M.; Shin, S.; Greenfield, S.F. Substance use disorders in global mental health delivery: Epidemiology, treatment gap, and implementation of evidence-based treatments. Harv. Rev. Psychiatry 2020, 28, 316. [Google Scholar] [CrossRef]
- Johnson, L.L. Design of observational studies. In Principles and Practice of Clinical Research; Elsevier: London, UK, 2018; pp. 231–248. [Google Scholar]
- Faggiano, F.; Vigna-Taglianti, F.D.; Versino, E.; Zambon, A.; Borraccino, A.; Lemma, P. School-based prevention for illicit drugs use: A systematic review. Prev. Med. 2008, 46, 385–396. [Google Scholar] [CrossRef]
- Van Boekel, L.C.; Brouwers, E.P.M.; van Weeghel, J.; Garretsen, H.F.L. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: Systematic review. Drug Alcohol Depend. 2013, 131, 23–35. [Google Scholar] [CrossRef]
- Rana, K.; Poudel, P.; Chimoriya, R. Qualitative Methodology in Translational Health Research: Current Practices and Future Directions. Healthcare 2023, 11, 2665. [Google Scholar] [CrossRef]
- Norberg, M.M.; Kezelman, S.; Lim-Howe, N. Primary prevention of cannabis use: A systematic review of randomized controlled trials. PLoS ONE 2013, 8, e53187. [Google Scholar] [CrossRef]
- Popova, L.; McDonald, E.A.; Sidhu, S.; Barry, R.; Richers Maruyama, T.A.; Sheon, N.M.; Ling, P.M. Perceived harms and benefits of tobacco, marijuana, and electronic vaporizers among young adults in Colorado: Implications for health education and research. Addiction 2017, 112, 1821–1829. [Google Scholar] [CrossRef]
- Robertson, E.B.; David, S.L.; Rao, S.A. Preventing Drug Use among Children and Adolescents: A Research-Based Guide for Parents, Educators, and Community Leaders; National Institute on Drug Abuse (NIDA): North Bethesda, MD, USA, 2003. [Google Scholar]
- Choi, S.; Hong, S.; Gatanaga, O.; Yum, A.; Lim, S.; Neighbors, C.; Yi, S. Substance Use and Treatment Disparities Among Asian Americans, Native Hawaiians, and Pacific Islanders: A Systematic Review. Drug Alcohol Depend. 2024, 256, 111088. [Google Scholar] [CrossRef] [PubMed]
- Radosevich, D. Designing an outcomes research study. In Understanding Health Care Outcomes Research, 2nd ed.; Jones and Bartlett: Sudbury, MA, USA, 2006; pp. 23–58. [Google Scholar]


{kind=link}
| PICO Elements | Inclusion Criteria |
|---|---|
| Population | Young population aged 12–45 years (both male and female) |
| Intervention | Cannabis use |
| Comparison | N/A |
| Outcome | Mental health outcomes diagnosed using standard diagnostic tool (e.g., DSM III or IV) |
| Context | Australia and/or United States |
| Study Design | Primary research studies, systematic reviews and meta-analyses, prospective or retrospective cohort studies, case–control, randomised control trials, cross-sectional studies, longitudinal studies, and guidelines published between 1 January 2012 and 1 November 2022 |
| No. | Author and Year of Publication | Country | Sample Size and Population | Study Design | Aim/Objective | Summary of Findings |
|---|---|---|---|---|---|---|
| 1 | Moller et al., 2013 [23] | Australia | Sample size = 4160; aged 20–24 and 40–44. | Cohort | To investigate the factors that predict self-harm among Australian adults, with a focus on substance use and psychological distress. | Past-year self-harm was reported by 8.2% of participants (95% CI 7.4–9.0%), with 9.3% of males (8.0–10.6%) and 7.3% of females (6.2–8.4%) who reported current cannabis use. |
| 2 | McCabe et al., 2021 [24] | United States | Sample size = 182,722; aged 18–22 years | Cross-sectional | To evaluate national trends over time in past-year alcohol and marijuana abstinence, co-use, alcohol use disorder, and marijuana use disorder among young adults in the US, considering their college status (2002–2018). | There was a yearly rise in marijuana use among young adults from 2002 to 2018, both for those in college (0.46%; 95% CI, 0.37–0.55%) and those not in college (0.49%; 95% CI, 0.40–0.59%). However, there was no corresponding increase in marijuana use disorder among all young adults. |
| 3 | Knopf, 2019 [25] | United States | Sample size = 23,317 in 11 articles; aged 12–32 years | Systematic review and meta-analysis | To assess cannabis use among adolescents under 18 years old (at least one assessment point) and determine its association with the development of depression in young adulthood (ages 18 to 32). | Teen cannabis users had more than three times the risk of attempting suicide in young adulthood compared to nonusers (OR: 3.46). Additionally, they faced an increased risk of developing depression (OR: 1.37) and experiencing suicidal ideation (OR: 1.50). |
| 4 | Zaman et al., 2015 [8] | United States | Sample size = 483; aged 12–18 years | Cohort | To assess the rates of cannabis abuse and dependence among adolescents referred for substance use evaluations, as well as the incidence of co-occurring psychiatric illnesses and substance use disorders among those individuals. | Found that 47% of the participants met the criteria for the Diagnostic and Statistical Manual of Mental Disorders IV, and an additional 32% met the criteria for cannabis abuse. Among adolescents with cannabis use disorders, there was a high co-occurrence of alcohol and opioid abuse or dependence. These individuals also experienced significant psychiatric comorbidities. |
| 5 | Wong et al., 2013 [26] | United States | Sample size = 73,183; high school students aged between 12 and 15 years | Cross-sectional | To investigate the link between different patterns of substance use and suicidality among a nationally representative sample of high school students in the United States. | Adolescents with a history of marijuana use showed associations with suicidal ideation, suicide planning, suicide attempts, and severe suicide attempts in the past year, even after adjusting for other confounding factors (OR = 1.9–5.2). |
| 6 | Horwood et al., 2012 [27] | Australia | Sample size = 6900; aged 12–45 years | Cohort | To assess the association between the frequency of cannabis use and the severity of depressive symptoms using data from four Australasian cohort studies. | The frequency of cannabis use was significantly associated with increasing depressive symptoms (p < 0.001). After adjusting for confounders, the depression scores for weekly users were 0.24 (95% CI 0.18–0.30) standard deviations higher than those for non-users. This association was consistent across the cohorts studied. Adolescents showed a particularly increased association. |
| 7 | Floyd Campbell, 2018 [28] | United States | Sample size = 120; African American and 111 white females; aged 18–30 years | Cross-sectional | To assess how the connection between depression and marijuana use varies between females in emerging adulthood and young adult females. | Found that 35% (75) of the participants tested positive for cannabis, and 21% (48) were experiencing depression, with an odds ratio (OR = 2.1; 95% CI 1.08–3.93). African Americans had higher odds of testing positive for marijuana compared to whites (OR = 4.6; 95% CI 2.52–8.68). There was no difference in the relationship between depression and marijuana use based on developmental stage. |
| 8 | Scholes-Balog et al., 2013 [29] | Australia | Sample size = 927; young people at ages of 15, 16, 17 and 19 years | Cohort | To examine the changing rates of cannabis use, misuse, and cannabis-related social harms among Australian adolescents as they transition into young adulthood. | The rates of cannabis use increased with age, with past-year use rising from 7.5% at age 15 to 29.8% at age 19. Cannabis use was more common among males than females at ages 17 and 19. Among cannabis users, the rates of cannabis-related harms were moderate, with anxiety and depression being the most prevalent, affecting 20–30% of users at each age. |
| 9 | Wilkinson et al., 2016 [30] | United States | Sample size = 9816; aged 18–32 years | Cohort | To investigate the longitudinal associations between substance use frequency and depressive symptoms from adolescence into young adulthood, with a focus on potential moderation by sex. | The frequency of cannabis use increases from adolescence to young adulthood, aligning with the rise in adolescent depressive symptoms, and this increase is positively associated with depressive symptoms from adolescence to young adulthood, with a stronger association for females. The proportion of respondents reporting cannabis use increases from 14% at ages 14–16 years to 25% at ages 20–22 years, then decreases to 17% for ages 32–34 years. Depressive symptoms follow the opposite pattern, starting higher in adolescence, decreasing in emerging adulthood, and then increasing slightly in young adulthood. For instance, the mean CES-D score for ages 14–16 years is 5.72, decreasing to 4.28 at ages 23–25 years, but then increasing again to 5.08 between ages 29 and 31 years. |
| 10 | Richter et al., 2017 [31] | United States | Sample size = 55,271; adolescent and young adult (exact age not specified) | Cohort | To provide recent national estimates of cannabis use disorder based on usage patterns, age, and other sociodemographic, substance use, and mental health variables. | The prevalence of cannabis use disorder (CUD) was higher among heavy (22.35%) or moderate (15.54%) users compared to light users (10.10%), and about twice as high among youth compared to adults. Anxiety was associated with a higher prevalence of CUD among heavy marijuana users only, while depression showed no significant association. Current marijuana use at any level was linked to increased odds of CUD compared to no current use, with odds increasing with intensity of use (OR = 8.20 for light, OR = 13.61 for moderate, and OR = 23.59 for heavy users, all p < 0.002). Age of initiation, anxiety, and depression did not show significant associations with CUD. In 2014, 3.49% of lifetime, 11.62% of past-year, and 15.32% of past-30-day marijuana users met DSM-IV criteria for CUD, with rates among youth generally at least double those of adults. |
| 11 | Cohn et al., 2016 [32] | United States | Sample size = 54,309; aged 12–45 years | Cross-sectional | To identify subtype differences, this study examined the prevalence and correlates of four exclusive groups of users (cigar-only, blunt-only, non-blunt marijuana, or dual cigar–blunt) in terms of demographic, mental health, and substance use characteristics. | Those who reported using blunts only or both cigars and blunts endorsed a greater number of symptoms of cannabis use disorder (CUD) compared to those who reported using cigars only or non-blunt marijuana. Lower perceptions of marijuana risk were associated with increased odds of cannabis use, with or without blunts. Major depressive episode (MDE) was uniquely linked to non-blunt cannabis use. Participants who reported blunt-only (AOR = 9.80) and dual cigar–blunt use (AOR = 9.76) endorsed the highest number of CUD symptoms, followed by those who reported non-blunt marijuana use (AOR = 7.61) and cigar-only use (AOR = 2.55). |
| 12 | Bechtold et al., 2015 [33] | United States | Sample size = 506; 41.7% White, 54.5% Black, 3.8% other | Longitudinal | To assess whether distinct developmental trajectories of marijuana use, tracked annually from early adolescence to the mid-20s, were linked to negative physical (e.g., asthma, high blood pressure) and mental (e.g., psychosis, anxiety disorders) health outcomes in the mid-30s. | Latent class growth curve analysis revealed four distinct subgroups of marijuana users: early onset chronic users, late increasing users, adolescence-limited users, and low/nonusers. However, these groups did not significantly differ in terms of their physical and mental health outcomes, including anxiety and suicide problems, assessed in the mid-30s. |
| 13 | Welsh et al., 2017 [34] | United States | Sample size = 483; aged 12–24 years | Cohort | To examine the relationship between mental health diagnoses and substance use disorders in adolescents and explore differences between different mental health diagnoses and types of substances used. | Cannabis use was associated with the development of externalising behaviour disorders (OR = 2.10, p = 0.024). Youths with problematic use, abuse, or dependence on marijuana were 2.20 times as likely to have an externalising behavioural disorder and twice as likely to have attention deficit hyperactivity disorder (ADHD) (odds ratio = 2.10, p = 0.024). |
| 14 | Leadbeater et al., 2019 [35] | United States | Sample size = 36,309; aged 18 and above | Longitudinal | To assess the strength of the associations between cannabis use frequency, cannabis use disorder (CUD), and mental health symptoms. | More frequent cannabis use was associated with increased psychotic symptoms from age 18 (b = 0.21, 95% CI = 0.10, 0.33) to age 65 (b = 0.36, 95% CI = 0.16, 0.56), higher depressive symptoms from age 18 (b = 0.22, 95% CI = 0.05, 0.40) to age 64 (b = 0.25, 95% CI = 0.01, 0.48), and increased anxiety symptoms from age 20 (b = 0.07, 95% CI = 0.01, 0.13) to age 63 (b = 0.13, 95% CI = 0.01, 0.25). Cannabis use disorder (CUD) was associated with more psychotic symptoms from age 18 (b = 1.21, 95% CI = 0.66, 1.76) to age 64 (b = 1.09, 95% CI = 0.05, 2.12), more depressive symptoms from age 18 (b = 0.96, 95% CI = 0.19, 1.73) to age 61 (b = 1.11, 95% CI = 0.01, 2.21), and more anxiety symptoms from age 18 (b = 0.45, 95% CI = 0.02, 0.88) to age 62 (b = 0.75, 95% CI = 0.08, 1.43). Time-varying interactions of CUD with early age of onset were not statistically significant. Females exhibited stronger associations between CUD and mental health symptoms than males for psychotic symptoms between ages 18 and 23, depressive symptoms between ages 18 and 26, and anxiety symptoms between ages 18 and 22. |
| 15 | Chadi et al., 2019 [36] | United States | Sample size = 26,821; aged 12–18 years | Cohort | To investigate the association between e-cigarette and marijuana use and depressive symptoms and suicidality in a large, nationally representative sample of high school students. | Cannabis use was reported by 9.7% of participants and was associated with depression (AOR: 1.25, 95% CI 1.04–1.50) and suicidality (AOR: 1.49, 95% CI 1.27–1.75). |
| 16 | London-Nadeau et al., 2021 [37] | United States | Sample size = 1430; conducted in waves when age of the participants was 13, 15, and 17 years | Longitudinal | To investigate the relationships between cannabis use and symptoms of depression and anxiety at ages 13, 15, and 17 years. | Cannabis use at 13 and 15 years predicted anxiety symptoms at 15 and 17 years, while depression symptoms at 15 years predicted cannabis use at 17 years. Differences were found between heterosexual and LGBTQI participants. LGBTQI individuals showed a stronger association between depression symptoms at 15 years and cannabis use at 17 years, and a negative association between anxiety symptoms at 15 years and cannabis use at 17 years. This suggests bidirectional relationships between cannabis use and depression/anxiety symptoms in adolescence. |
| 17 | Weinberger et al., 2020 [14] | United States | Sample size = 204,102; aged 12–17 years | Cross-sectional | To investigate the association between depression and increased cannabis use among youth in the United States, both overall and by demographic factors. The study also aimed to examine trends in cannabis use by depression status among youth from 2004 to 2016. | Between 2004 and 2016, cannabis use rose among both youth with and without depression. However, the increase was significantly faster among youth with depression (8.45% to 11.65%) compared to those without depression (4.28% to 4.71%). Youth with depression were more than twice as likely to report cannabis use (12.86% versus 6.40%) compared to those without depression. |
| 18 | Phillips et al., 2018 [38] | United States | Sample size = 300; university students from 18–25 years | Cross-sectional | To examine whether marijuana use and related issues were associated with various demographic, personality, and psychological factors among college students at a mid-sized university in Colorado. | Out of 300 participants, 219 (73%) reported lifetime marijuana use, 195 (65%) reported use in the last year, and 126 (42%) reported use within the last 30 days. Approximately 29% of all participants (n = 88; 21% of females and 43% of males) tested positive for marijuana on the urine screen, confirming recent use. Among the three psychological factors (social anxiety, general anxiety, and depression), only depression was associated with cannabis use. |
| 19 | Levy and Weitzman, 2019 [39] | United States | Sample size = 527; aged 14–18 years | Cohort | To evaluate whether adolescents presenting for routine medical care had experienced acute psychotic symptoms during or immediately after marijuana use. | Overall, 27.4% of respondents reported hallucinations, 33.6% reported paranoia or anxiety, and 42.9% reported at least one symptom. None of hallucinations, paranoia, or anxiety correlated with age, sex, race/ethnicity, general health status, or socioeconomic status. However, respondents meeting criteria for cannabis use disorder were more likely to report these symptoms. Among respondents, 47.9% reported using marijuana “monthly or more” in the past year, and this group was more likely to report hallucinations and paranoia compared to those who used “once or twice” (60.0% vs. 40%). |
| 20 | Power et al., 2021 [40] | United States | Over 650 subjects and 5600 controls | Systematic review and meta-analysis | To explore whether cannabis has an impact on full-scale IQ in general population samples, contributing to a better understanding of this potential pathway. | Cannabis use in youth was associated with modest IQ differences, equating to approximately a two-point decrease in young cannabis users. |
| 21 | Gobbi et al., 2019 [41] | United States | A total of 11 studies comprising 23,317 individuals were included in the quantitative synthesis | Systematic review and meta-analysis | To quantify the association between cannabis use during adolescence and the risk of developing subsequent major depression, anxiety, and suicidal behaviour. | The OR for developing depression in young adulthood for cannabis users compared with nonusers was 1.37 (95% CI, 1.16–1.62; I2 = 0%). The pooled OR for anxiety was not statistically significant, at 1.18 (95% CI, 0.84–1.67; I2 = 42%). However, the pooled OR for suicidal ideation was 1.50 (95% CI, 1.11–2.03; I2 = 0%), and for suicidal attempt, it was 3.46 (95% CI, 1.53–7.84, I2 = 61.3%). |
| 22 | Han et al., 2021 [42] | United States | Sample size = 281,650; aged 18–34 years | Cohort | To assess whether cannabis use and cannabis use disorder (CUD) are linked to a higher prevalence of suicidality among young adults, with or without depression, and to assess if these associations differ by sex. | The adjusted prevalence of suicidal ideation, plan, and attempt increased 1.4 to 1.6 times from the 2008–2009 to 2018–2019 periods (adjusted risk ratio (ARR) for suicidal ideation, 1.4 (95% CI, 1.3–1.5); ARR for suicide plan, 1.6 (95% CI, 1.5–1.9); ARR for suicide attempt, 1.4 (95% CI, 1.2–1.7)). Past-year cannabis use disorder (CUD), daily cannabis use, and nondaily cannabis use were associated with a higher prevalence of past-year suicidal ideation, plan, and attempt in both sexes. Among individuals without major depressive episode, the prevalence of suicidal ideation for those with CUD was 13.9% vs. 3.5% among women and 9.9% vs. 3.0% among men; p < 0.001. The suicide plan among those with CUD and major depressive episode was 52% higher for women (23.7%) than men (15.6%); p < 0.001. |
| 23 | Pahl et al., 2014 [13] | United States | Sample size = 838; conducted in waves when participants were 14, 19, 24, and 29 years | Cohort | To examine adolescent self-control as a predictor of membership in joint developmental trajectories of depressive mood and marijuana use from adolescence to young adulthood. | The low marijuana use and low depressive mood (LL) group, reporting no marijuana use, consistently had the lowest depressive mood over time. The low marijuana use and intermediate depressive mood (LI) group, with minimal use in early adolescence and no use by age 29, showed higher depressive mood in early adolescence that decreased linearly over time. The high marijuana use and low depressive mood (HL) group, starting marijuana use early and increasing over time, reported depressive mood similar to the LL group. The high marijuana use and high depressive mood (HH) group, mirroring the HL group’s use pattern, reported the highest depressive mood in early adolescence, continuing into young adulthood. Thus, the co-occurrence of high marijuana use and depressive mood from adolescence to young adulthood is linked to low self-control in adolescence. Conversely, high self-control is associated with low marijuana use and depression over time. |
| 24 | Meier et al., 2020 [43] | United States | Sample size = 506; aged 15–26 years | Longitudinal | To determine whether increases in recent and cumulative cannabis use are associated with increases in internalising problems from adolescence to young adulthood. | After adjusting for time-varying covariates, the study found that increases in cumulative years of weekly cannabis use, but not recent use, were linked to higher levels of depression symptoms and anxiety/depression problems. Specifically, each additional year of prior weekly cannabis use was associated with a slight increase in depression symptoms (b = 0.012, p = 0.005) and anxiety/depression problems (b = 0.009, p = 0.001). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baral, A.; Hanna, F.; Chimoriya, R.; Rana, K. Cannabis Use and Its Impact on Mental Health in Youth in Australia and the United States: A Scoping Review. Epidemiologia 2024, 5, 106-121. https://doi.org/10.3390/epidemiologia5010007
Baral A, Hanna F, Chimoriya R, Rana K. Cannabis Use and Its Impact on Mental Health in Youth in Australia and the United States: A Scoping Review. Epidemiologia. 2024; 5(1):106-121. https://doi.org/10.3390/epidemiologia5010007
Chicago/Turabian StyleBaral, Aayush, Fahad Hanna, Ritesh Chimoriya, and Kritika Rana. 2024. "Cannabis Use and Its Impact on Mental Health in Youth in Australia and the United States: A Scoping Review" Epidemiologia 5, no. 1: 106-121. https://doi.org/10.3390/epidemiologia5010007
APA StyleBaral, A., Hanna, F., Chimoriya, R., & Rana, K. (2024). Cannabis Use and Its Impact on Mental Health in Youth in Australia and the United States: A Scoping Review. Epidemiologia, 5(1), 106-121. https://doi.org/10.3390/epidemiologia5010007