
Return to Driving after Elective Foot and Ankle Surgery: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
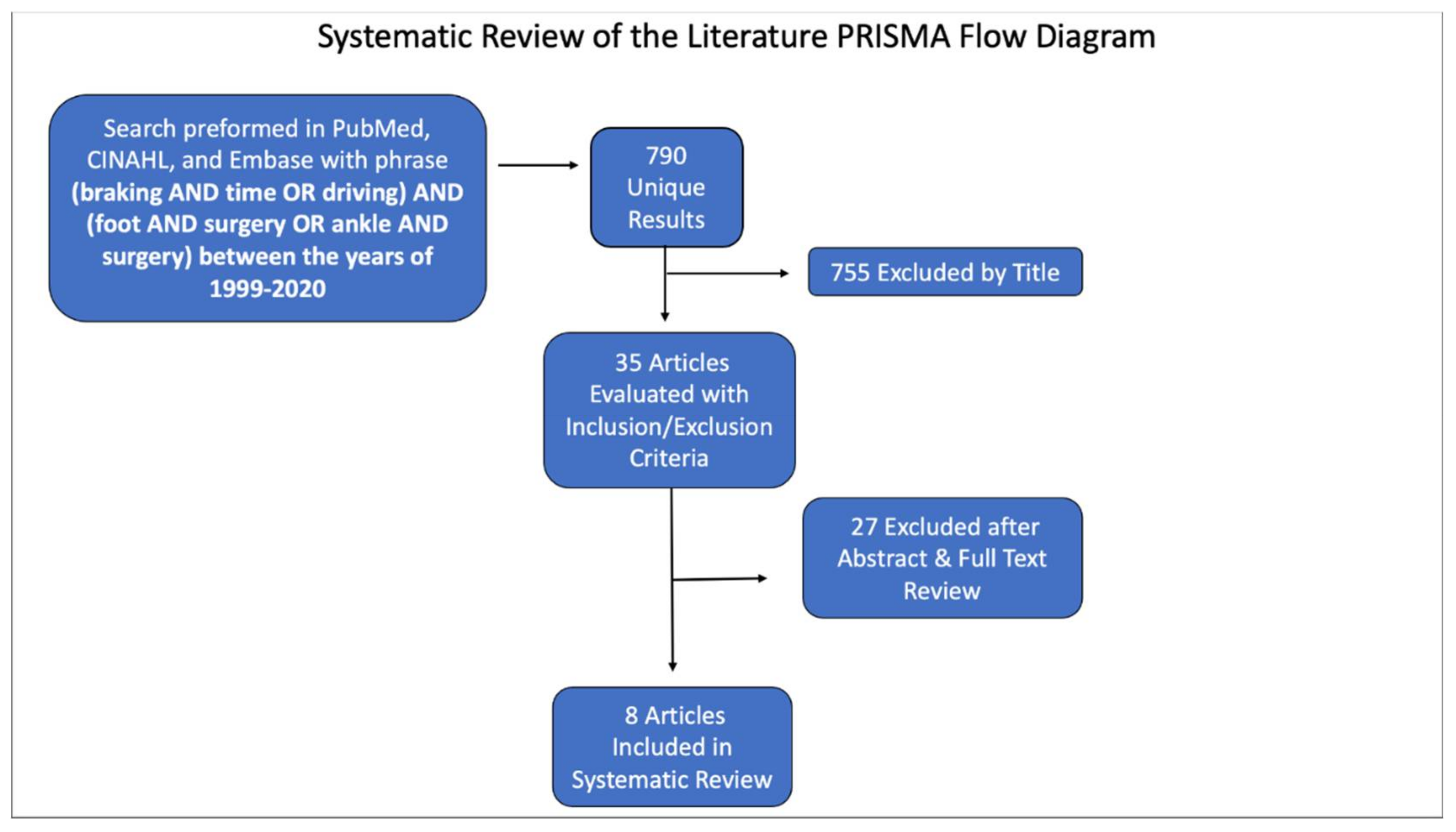
2.1. Literature Review
2.2. Eligibility
2.3. Data Extraction and Analysis
3. Results
3.1. Study Details
3.2. Population and Control Group
3.3. Method of Evaluation
3.4. Objective Observer-Reported Outcomes
3.5. Subjective Patient-Reported Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Humbyrd, C.J.; Sugarman, J. Ethical Considerations Related to Impaired Driving after Orthopaedic Injuries. J. Bone Jt. Surg. 2016, 98, e60. [Google Scholar] [CrossRef] [PubMed]
- Sittapairoj, T.; Anthony, C.A.; Rungprai, C.; Gao, Y.; Barg, A.; Phisitkul, P. Brake Reaction Time after Ankle and Subtalar Arthroscopy. Arthrosc. J. Arthrosc. Relat. Surg. 2017, 33, 2231–2237. [Google Scholar] [CrossRef] [PubMed]
- Egol, K.A.; Sheikhazadeh, A.; Mogatederi, S.; Barnett, A.; Koval, K.J. Lower-Extremity Function for Driving an Automobile after Operative Treatment of Ankle Fracture. J. Bone Jt. Surg. 2003, 85, 1185–1189. [Google Scholar] [CrossRef] [PubMed]
- Egol, K.A.; Sheikhazadeh, A.; Koval, K.J. Braking Function after Complex Lower Extremity Trauma. J. Trauma Inj. Infect. Crit. Care 2008, 65, 1435–1438. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.J.; McClain, W.D.; Dowd, T.C. Patient Safety Driving after Foot and Ankle Surgery. Orthop. Clin. N. Am. 2018, 49, 527–539. [Google Scholar] [CrossRef]
- DiSilvestro, K.J.; Santoro, A.J.; Tjoumakaris, F.P.; Levicoff, E.A.; Freedman, K.B. When Can I Drive after Orthopaedic Surgery? A Systematic Review. Clin. Orthop. Relat. Res. 2016, 474, 2557–2570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, M. “How Long Does It Take to Stop?” Methodological Analysis of Driver Perception-Brake Times. Transp. Hum. Factors 2000, 2, 195–216. [Google Scholar] [CrossRef]
- Dammerer, D.; Braito, M.; Biedermann, R.; Ban, M.; Giesinger, J.; Haid, C.; Liebensteiner, M.C.; Kaufmann, G. Effect of surgical shoes on brake response time after first metatarsal osteotomy—A prospective cohort study. J. Orthop. Surg. Res. 2016, 11, 14. [Google Scholar] [CrossRef] [Green Version]
- Holt, G.; Kay, M.; McGrory, R.; Kumar, C.S. Emergency Brake Response Time after First Metatarsal Osteotomy. J. Bone Jt. Surg. 2008, 90, 1660–1664. [Google Scholar] [CrossRef] [PubMed]
- Jeng, C.L.; Lin, J.S.; Amoyal, K.; Campbell, J.; Myerson, M.S. Driving Brake Reaction Time Following Right Ankle Arthrodesis. Foot Ankle Int. 2011, 32, 896–899. [Google Scholar] [CrossRef] [PubMed]
- Liebensteiner, M.C.; Braito, M.; Giesinger, J.M.; Fuchs, A.; Putzer, D.; Schuh, R.; Haid, C.; Kaufmann, G. Driving ability after right-sided ankle arthroscopy—A prospective Study. Injury 2016, 47, 762–765. [Google Scholar] [CrossRef] [PubMed]
- McDonald, E.; Shakked, R.; Daniel, J.; Pedowitz, D.I.; Winters, B.S.; Reb, C.; Lynch, M.-K.; Raikin, S.M. Driving after Hallux Valgus Surgery. Foot Ankle Int. 2017, 38, 982–986. [Google Scholar] [CrossRef] [PubMed]
- McDonald, E.L.; Pedowitz, D.I.; Shakked, R.J.; Fuchs, D.J.; Winters, B.S.; Daniel, J.N.; Raikin, S.M. When Is It Safe to Drive after Total Ankle Arthroplasty? Clin. Orthop. Relat. Res. 2020, 478, 8–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwienbacher, S.; Aghayev, E.; Hofmann, U.K.; Jordan, M.; Marmotti, A.; Röder, C.; Ipach, I. Driving and emergency braking may be impaired after tibiotalar joint arthrodesis: Conclusions after a case series. Int. Orthop. 2015, 39, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Sansosti, L.E.; Greene, T.; Hasenstein, T.; Berger, M.; Meyr, A.J. U. S. State Driving Regulations Relevant to Foot and Ankle Surgeons. J. Foot Ankle Surg. 2017, 56, 522–542. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.W.L.; Yam, M.; Chan, M.L.; Kwek, E.B.K. Return to car driving is safe 6 weeks after operative treatment of right ankle fractures. Arch. Orthop. Trauma Surg. 2018, 138, 1691–1697. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Procedure | Experimental Group | Control Group | Average MINORS Score |
|---|---|---|---|---|
| Dammerer et al. [8] | Hallux valgus | 42 patients | No control group | 13 |
| Holt et al. [9] | Hallux valgus | 28 patients | 28 age-, gender-, and driving-frequency-matched volunteers | 19.5 |
| Jeng et al. [10] | Ankle arthrodesis | 10 patients | 10 age-matched volunteers | 16 |
| Liebensteiner et al. [11] | Ankle arthroscopy | 19 patients | No control group | 15 |
| McDonald et al. [12] | Hallux valgus | 60 patients | 20 age- and gender-matched volunteers | 18 |
| McDonald et al. [13] | Total ankle arthroplasty | 59 patients | 20 age- and gender- matched volunteers | 19 |
| Schwienbacher et al. [14] | Ankle arthrodesis and other foot joint arthrodesis | 12 patients with ankle arthrodesis 12 patients with other foot joint arthrodeses | 17 volunteers | 16 |
| Sittapairoj et al. [2] | Ankle arthroscopy | 17 patients | 19 age-matched volunteers | 17 |
| Study | Control Mean BRT (ms) | 2-Week Mean BRT (ms) | p-Value | 6-Week Mean BRT (ms) | p-Value |
|---|---|---|---|---|---|
| Liebensteiner et al. [11] | 606, pre-op baseline | 606 | Not significant ♦ | 596 | Not significant ♦ |
| Sittapairoj et al. [2] | 550, healthy control | 570 | p = 0.84 | N/A | N/A |
| Study | Control Mean BRT (ms) | 6-Week Mean BRT (ms) | p-Value |
|---|---|---|---|
| McDonald et al. [13] | 547, healthy control | 620 passing group * (n = 54) 1120 failing group * (n = 5) | <0.001 @ |
| Study | Control Mean BRT (ms) | 6-Month Mean BRT (ms) | p-Value | 12-Month Mean BRT (ms) | p-Value |
|---|---|---|---|---|---|
| Schweinbacher et al. [14] | 475.7, healthy control | 596.2 other foot joint arthrodesises | 1 μ | N/A | N/A |
| 729.7 ankle arthrodesis | 0.026 μ | ||||
| Jeng et al. [10] | 330, healthy control | N/A | N/A | 420 | 0.03 λ |
| Study | Control Mean BRT (ms) | 2-Week Mean BRT (ms) | p-Value | 6-Week Mean BRT (ms) | p-Value |
|---|---|---|---|---|---|
| Dammerer et al. [8] | 712, pre-op baseline with no orthosis | 804 with Hallux Valgus Shoe | <0.001 # | 750 with Hallux Valgus Shoe | 0.003 δ |
| 811 with Forefoot Relief Shoe | <0.001 δ | ||||
| 841 with Forefoot Relief Shoe | <0.001 # | ||||
| 769 with no orthosis | <0.001 δ | ||||
| Holt et al. [9] | 806, pre-op baseline | 850 | 0.791 # | 684 | <0.001 δ |
| McDonald et al. [12] | 550, healthy control | N/A | N/A | 640 passing group * (n = 51) 1360 failing group * (n = 9) | 0.02 @ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lundy, A.; Piscoya, A.; Rodkey, D.; Bedrin, M.; Eckel, T. Return to Driving after Elective Foot and Ankle Surgery: A Systematic Review. Osteology 2022, 2, 121-128. https://doi.org/10.3390/osteology2030014
Lundy A, Piscoya A, Rodkey D, Bedrin M, Eckel T. Return to Driving after Elective Foot and Ankle Surgery: A Systematic Review. Osteology. 2022; 2(3):121-128. https://doi.org/10.3390/osteology2030014
Chicago/Turabian StyleLundy, Alexander, Andres Piscoya, Daniel Rodkey, Michael Bedrin, and Tobin Eckel. 2022. "Return to Driving after Elective Foot and Ankle Surgery: A Systematic Review" Osteology 2, no. 3: 121-128. https://doi.org/10.3390/osteology2030014
APA StyleLundy, A., Piscoya, A., Rodkey, D., Bedrin, M., & Eckel, T. (2022). Return to Driving after Elective Foot and Ankle Surgery: A Systematic Review. Osteology, 2(3), 121-128. https://doi.org/10.3390/osteology2030014