Ionizing Radiation Mediates Dose Dependent Effects Affecting the Healing Kinetics of Wounds Created on Acute and Late Irradiated Skin

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procurement of Animals and Ethics Approval
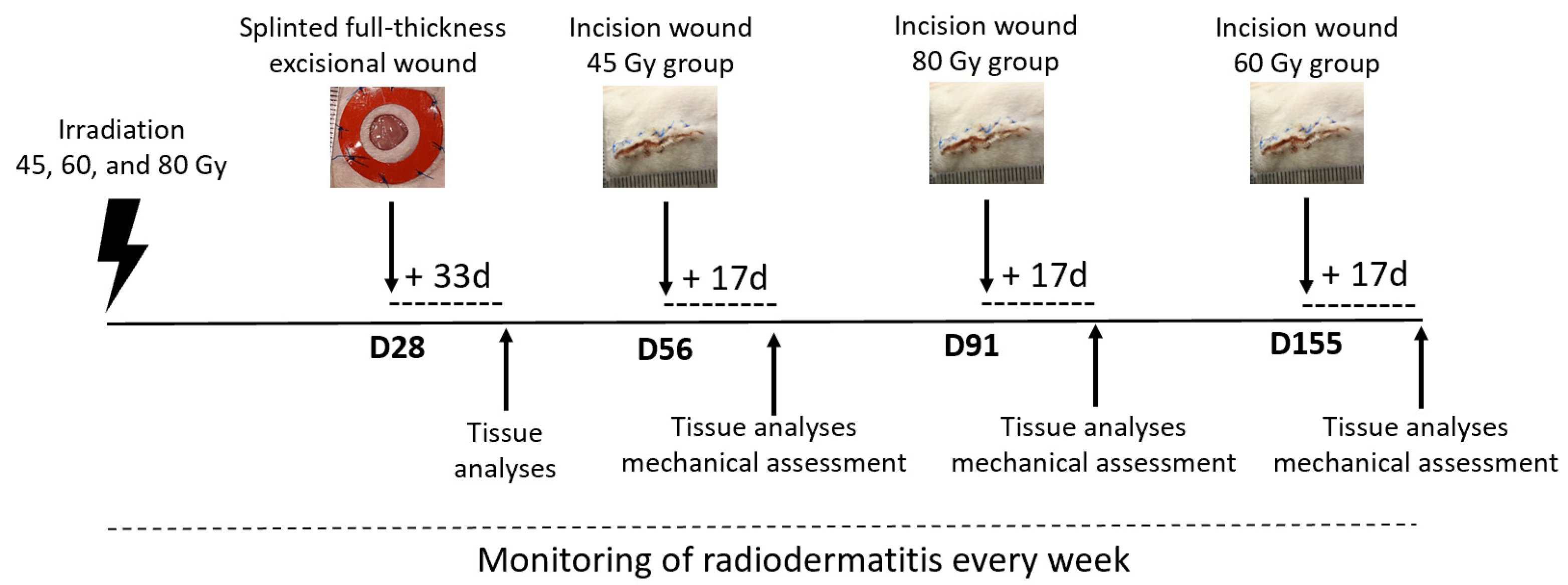
2.2. Irradiation Protocol and Experimental Design
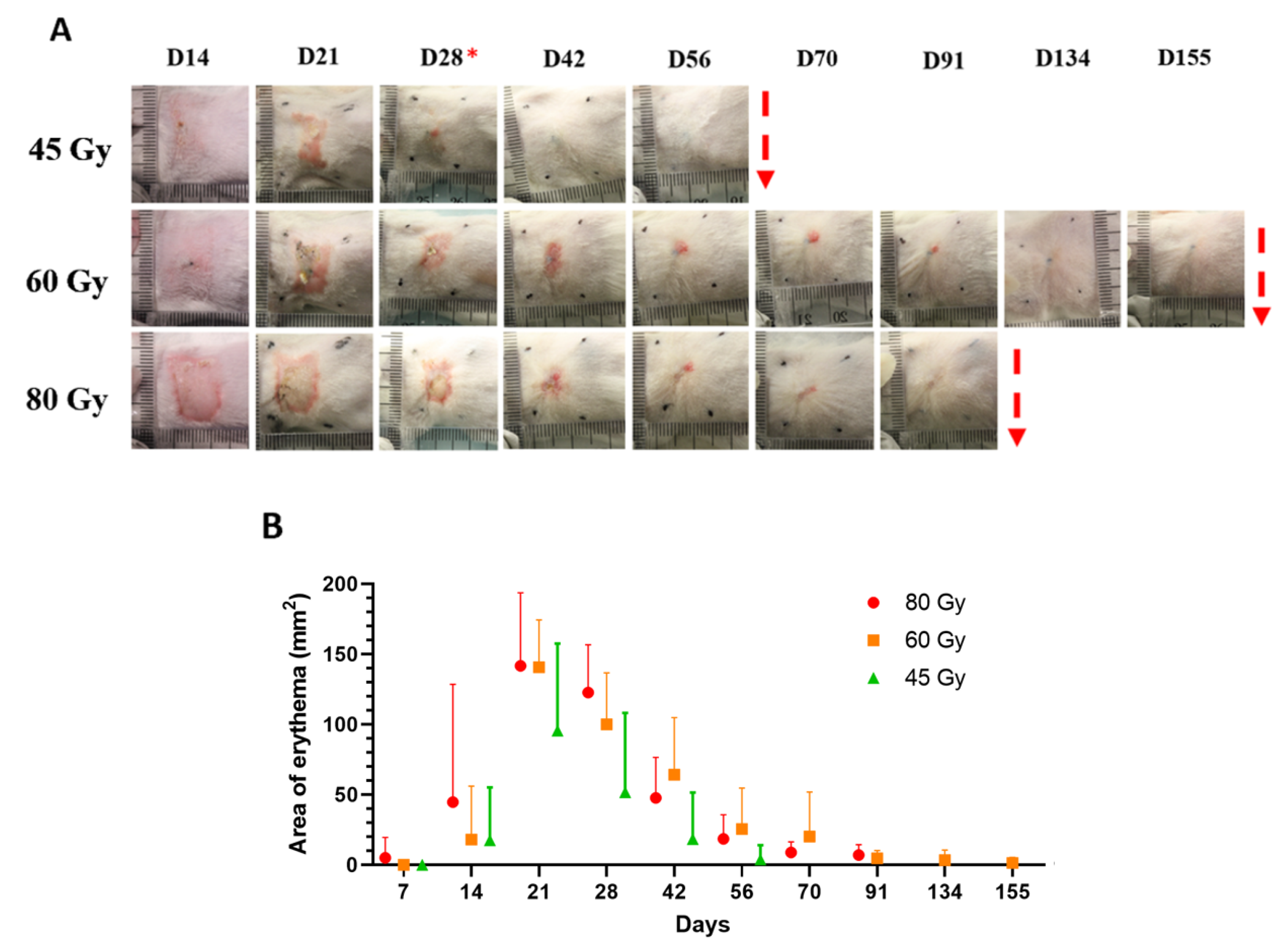
2.3. Monitoring of Radiodermatitis Progression
2.4. Histological Analyses
2.5. Immunolabeling on Tissue Cryosections and Related Analyses
2.6. Surgical Procedures on Animals
2.7. Macroscopic Imaging of the Wounds for Measurements and Scoring Analyses
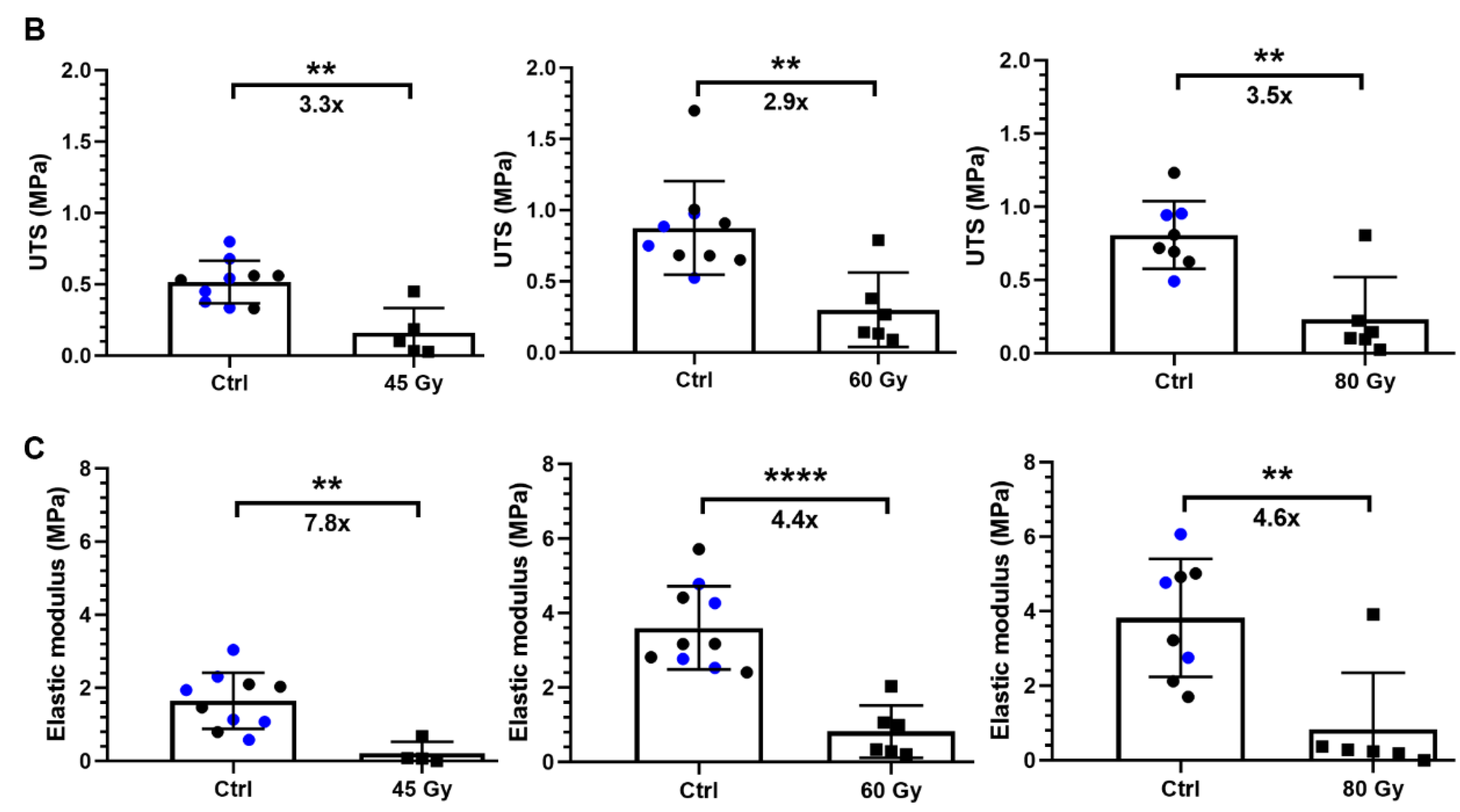
2.8. Evaluation of the Mechanical Properties of Skin after Incisional Surgery
2.9. Statistical Analyses
3. Results
3.1. Skin Toxicity Evolves over Time and Is Dose Dependent
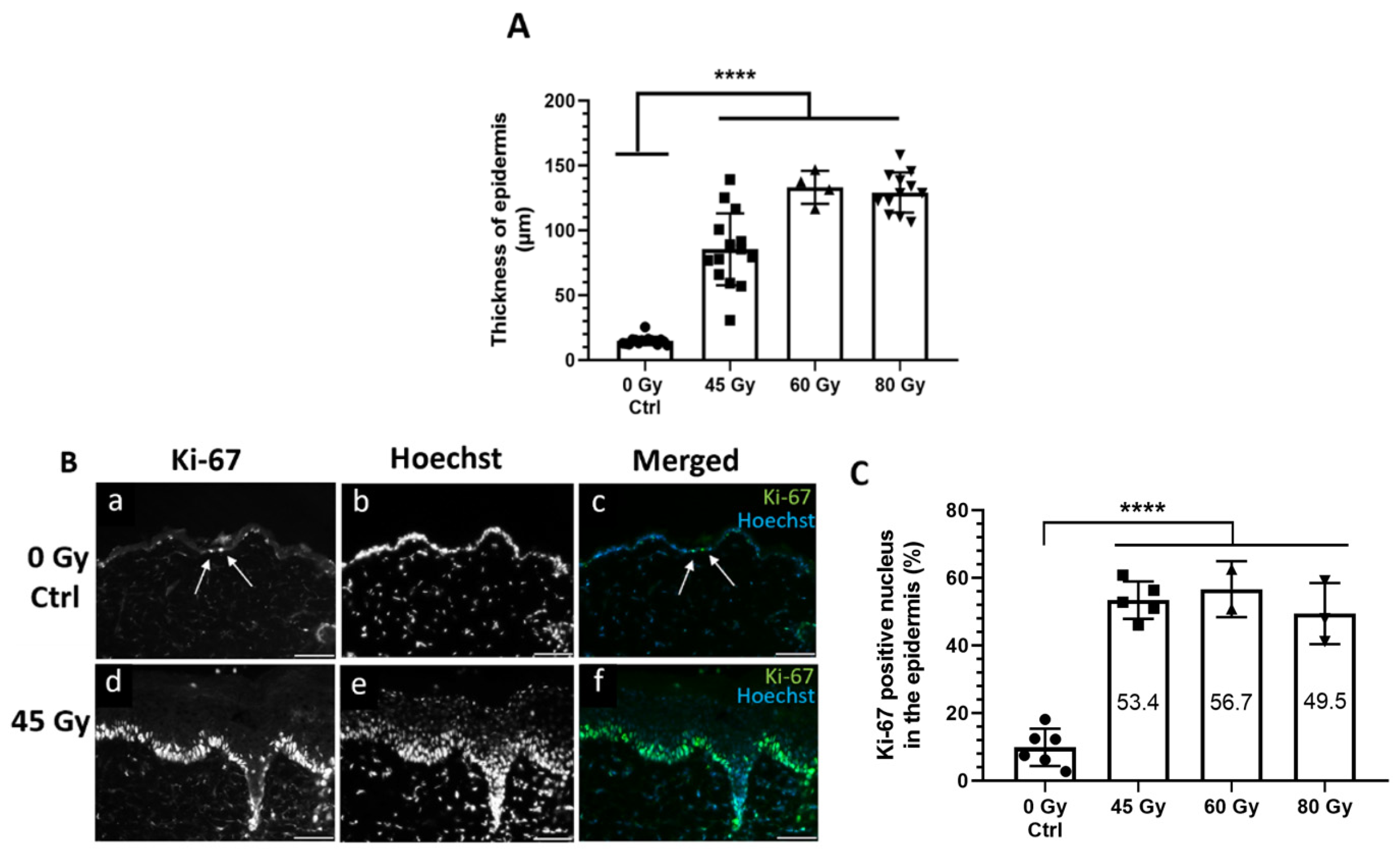
3.2. Acute Effects: Epidermal Thickness and Proliferative Status Are Increased in Murine Irradiated Epidermis 28 Days after Irradiation
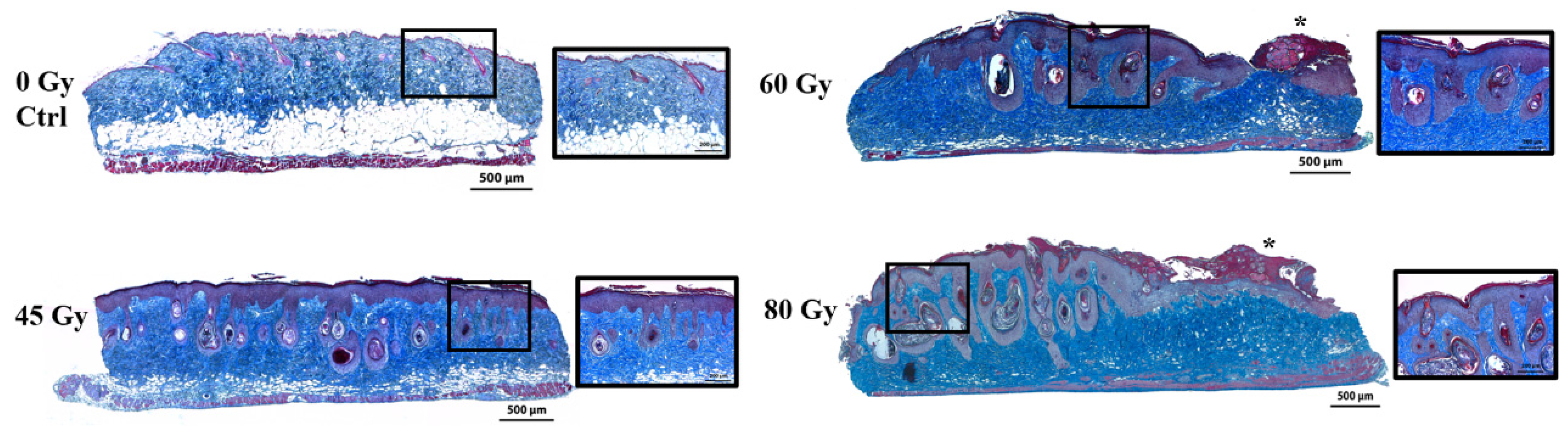
3.3. Evidence of Dermal Damage and dWAT Thinning 28 Days after Irradiation
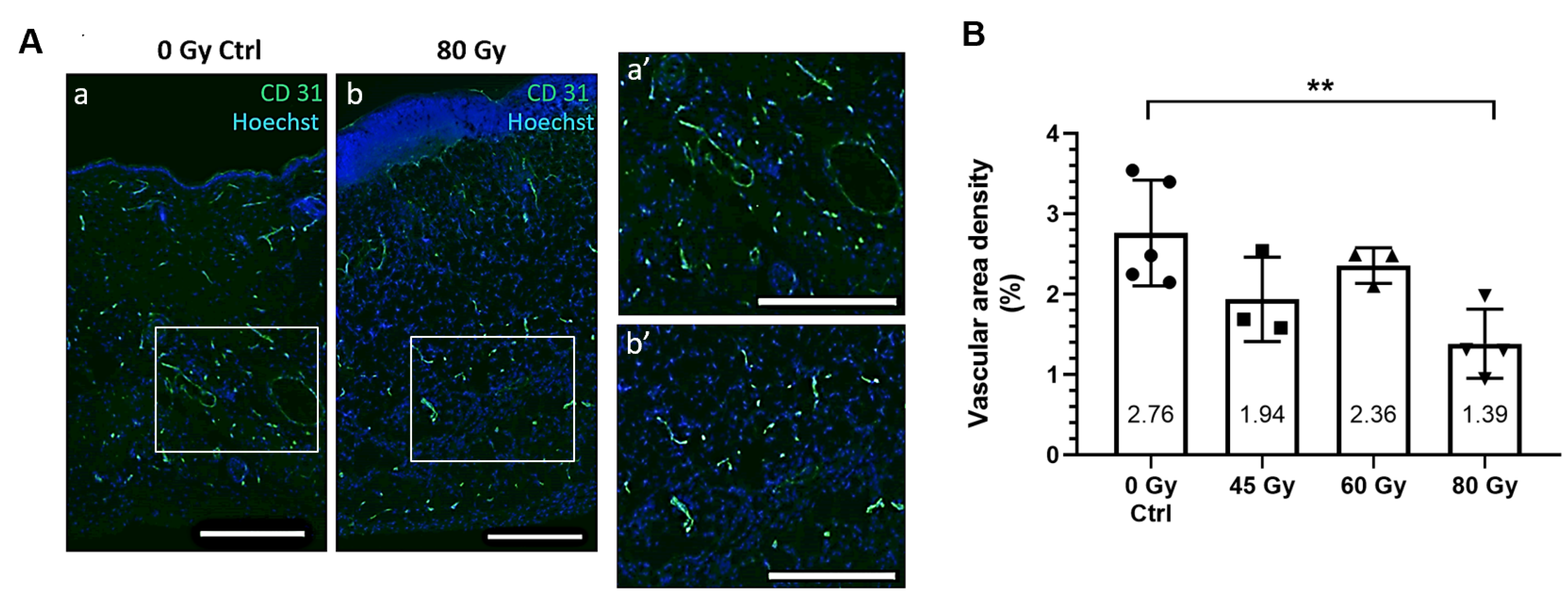
3.4. Capillary Vessels Are Altered in Irradiated Skin
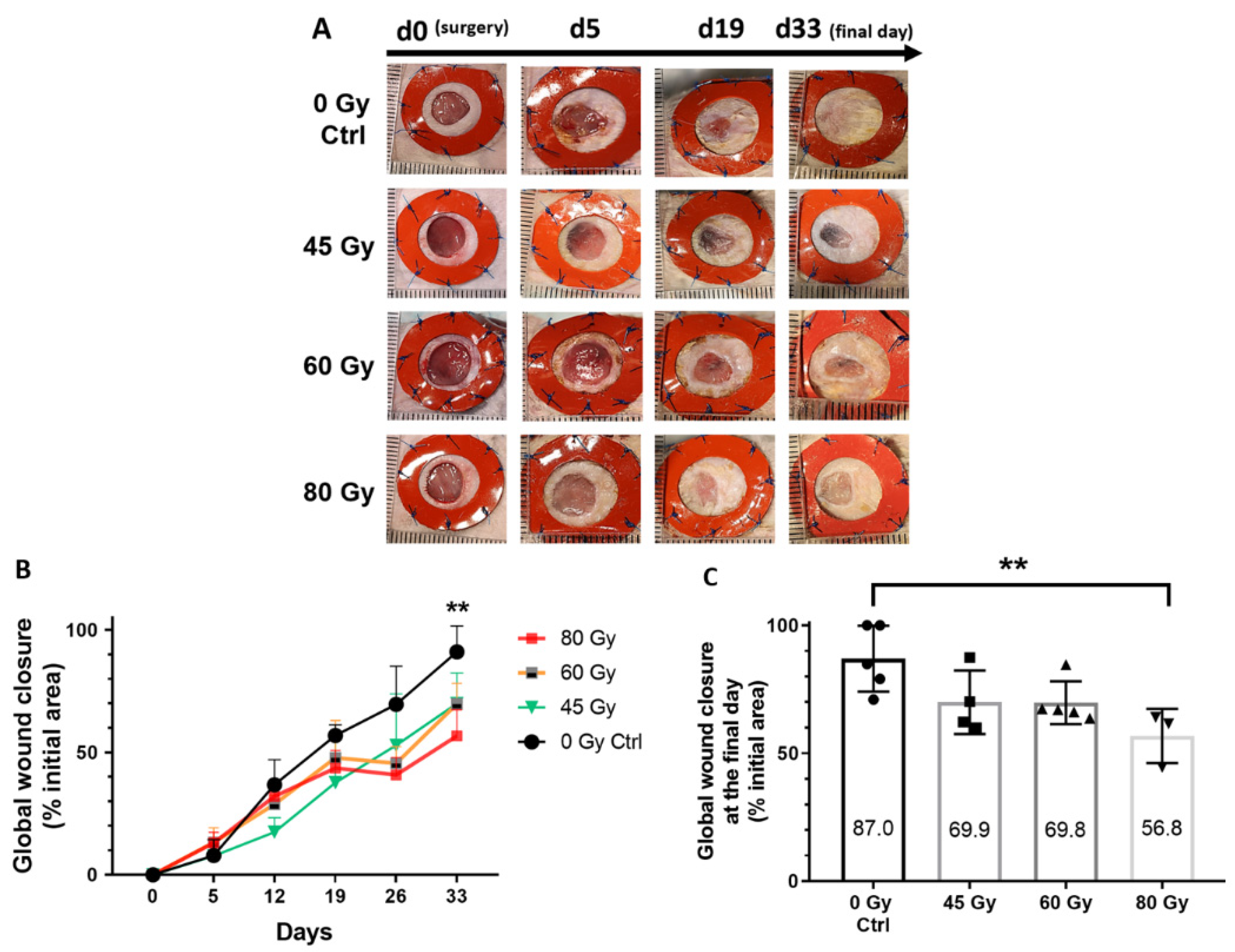
3.5. Delayed Healing Kinetics of Excisional Wounds Created on Irradiated Skin in the Acute Stage of Radiodermatitis
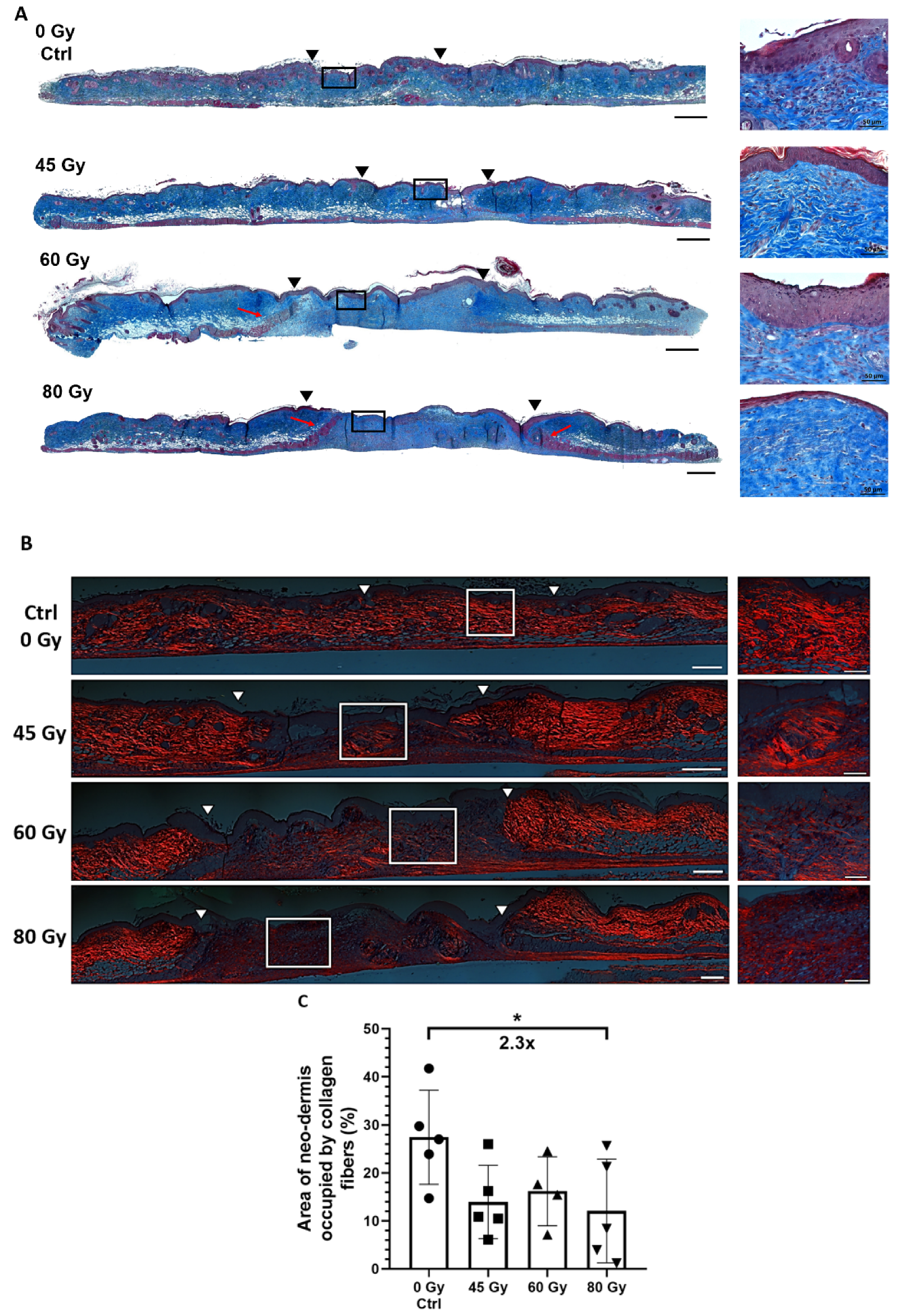
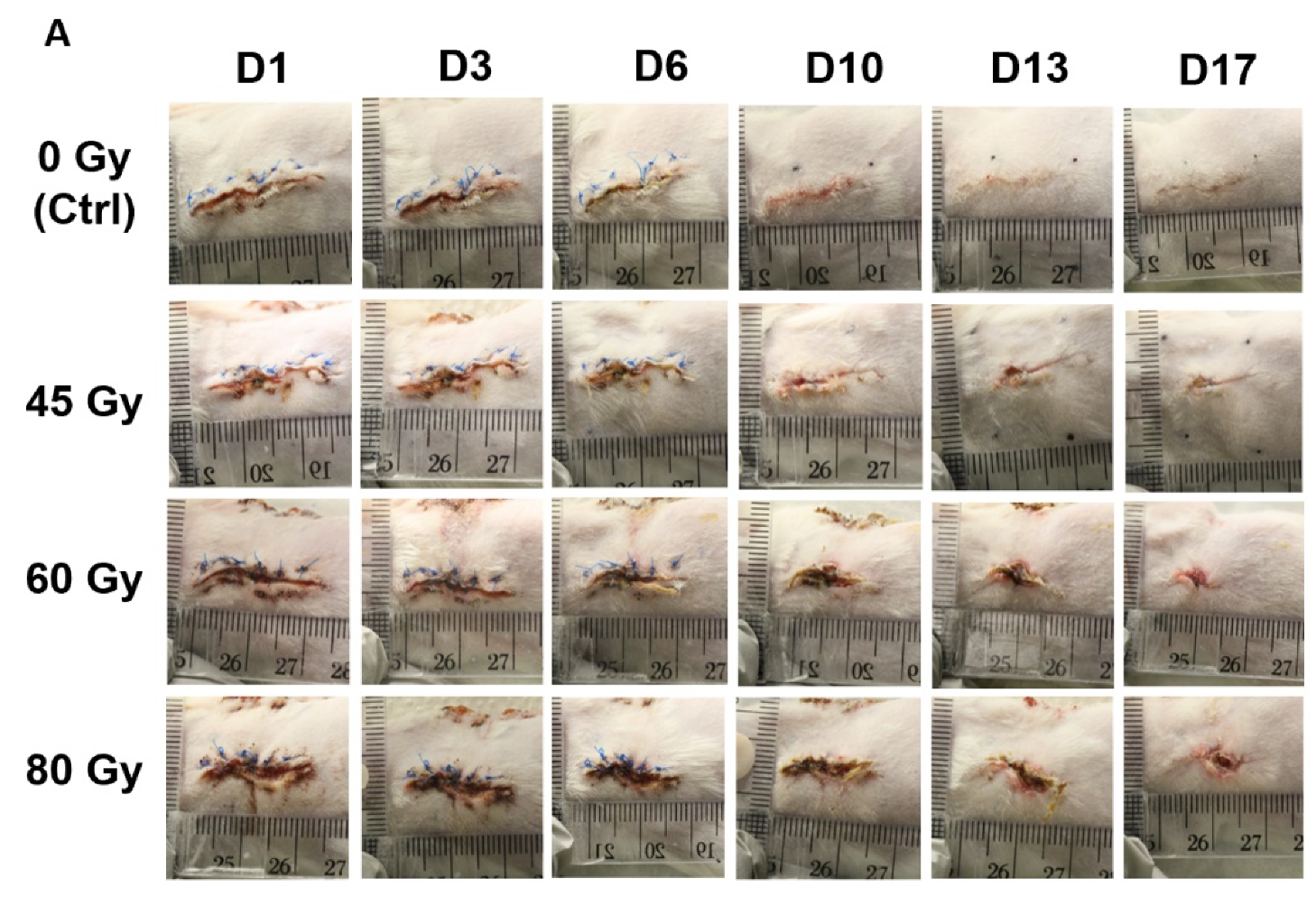
3.6. Healing of Incisional Wounds Created in Late Stages Irradiated Skin after Visual Resorption of Radiodermatitis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Delaney, G.; Jacob, S.; Featherstone, C.; Barton, M. The role of radiotherapy in cancer treatment: Estimating optimal utilization from a review of evidence-based clinical guidelines. Cancer 2005, 104, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Baskar, R.; Lee, K.A.; Yeo, R.; Yeoh, K.W. Cancer and radiation therapy: Current advances and future directions. Int. J. Med. Sci. 2012, 9, 193–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maddocks-Jennings, W.; Wilkinson, J.M.; Shillington, D. Novel approaches to radiotherapy-induced skin reactions: A literature review. Complement. Ther. Clin. Pr. 2005, 11, 224–231. [Google Scholar] [CrossRef] [PubMed]
- McQuestion, M. Evidence-based skin care management in radiation therapy: Clinical update. Semin. Oncol. Nurs. 2011, 27, e1–e17. [Google Scholar] [CrossRef]
- Salvo, N.; Barnes, E.; van Draanen, J.; Stacey, E.; Mitera, G.; Breen, D.; Giotis, A.; Czarnota, G.; Pang, J.; De Angelis, C. Prophylaxis and management of acute radiation-induced skin reactions: A systematic review of the literature. Curr. Oncol. 2010, 17, 94–112. [Google Scholar]
- Singh, M.; Alavi, A.; Wong, R.; Akita, S. Radiodermatitis: A Review of Our Current Understanding. Am. J. Clin. Dermatol. 2016, 17, 277–292. [Google Scholar] [CrossRef]
- Mendelsohn, F.A.; Divino, C.M.; Reis, E.D.; Kerstein, M.D. Wound care after radiation therapy. Adv. Ski. Wound Care 2002, 15, 216–224. [Google Scholar] [CrossRef]
- Brown, K.R.; Rzucidlo, E. Acute and chronic radiation injury. J. Vasc. Surg. 2011, 53, 15S–21S. [Google Scholar] [CrossRef]
- Lataillade, J.J.; Doucet, C.; Bey, E.; Carsin, H.; Huet, C.; Clairand, I.; Bottollier-Depois, J.F.; Chapel, A.; Ernou, I.; Gourven, M.; et al. New approach to radiation burn treatment by dosimetry-guided surgery combined with autologous mesenchymal stem cell therapy. Regen. Med. 2007, 2, 785–794. [Google Scholar] [CrossRef] [Green Version]
- Bey, E.; Duhamel, P.; Lataillade, J.J.; de Revel, T.; Carsin, H.; Gourmelon, P. Treatment of radiation burns with surgery and cell therapy. A report of two cases. Bull. Acad. Natl. Med. 2007, 191, 971–978, discussion 979. [Google Scholar]
- Ryan, J.L. Ionizing radiation: The good, the bad, and the ugly. J. Investig. Dermatol. 2012, 132, 985–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ejaz, A.; Greenberger, J.S.; Rubin, P.J. Understanding the mechanism of radiation induced fibrosis and therapy options. Pharmacol. Ther. 2019, 204, 107399. [Google Scholar] [CrossRef] [PubMed]
- Ejaz, A.; Epperly, M.W.; Hou, W.; Greenberger, J.S.; Rubin, J.P. Adipose-Derived Stem Cell Therapy Ameliorates Ionizing Irradiation Fibrosis via Hepatocyte Growth Factor-Mediated Transforming Growth Factor-beta Downregulation and Recruitment of Bone Marrow Cells. Stem Cells 2019, 37, 791–802. [Google Scholar] [CrossRef]
- Martin, M.; Lefaix, J.; Delanian, S. TGF-beta1 and radiation fibrosis: A master switch and a specific therapeutic target? Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 277–290. [Google Scholar] [CrossRef]
- Milliat, F.; Francois, A.; Isoir, M.; Deutsch, E.; Tamarat, R.; Tarlet, G.; Atfi, A.; Validire, P.; Bourhis, J.; Sabourin, J.C.; et al. Influence of endothelial cells on vascular smooth muscle cells phenotype after irradiation: Implication in radiation-induced vascular damages. Am. J. Pathol. 2006, 169, 1484–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, A.M.; O’Sullivan, B.; Turcotte, R.; Bell, R.; Catton, C.; Chabot, P.; Wunder, J.; Hammond, A.; Benk, V.; Kandel, R.; et al. Late radiation morbidity following randomization to preoperative versus postoperative radiotherapy in extremity soft tissue sarcoma. Radiother. Oncol. 2005, 75, 48–53. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, B.; Davis, A.M.; Turcotte, R.; Bell, R.; Catton, C.; Chabot, P.; Wunder, J.; Kandel, R.; Goddard, K.; Sadura, A.; et al. Preoperative versus postoperative radiotherapy in soft-tissue sarcoma of the limbs: A randomised trial. Lancet 2002, 359, 2235–2241. [Google Scholar] [CrossRef]
- Tumerdem-Ulug, B.; Kuran, I.; Ozden, B.C.; Mete, O.; Kemikler, G.; Aktas, S.; Calik, B. Does hyperbaric oxygen administration before or after irradiation decrease side effects of irradiation on implant sites? Ann. Plast. Surg. 2011, 67, 62–67. [Google Scholar] [CrossRef]
- Vandeweyer, E.; Deraemaecker, R. Radiation therapy after immediate breast reconstruction with implants. Plast. Reconstr. Surg. 2000, 106, 56–58, discussion 59–60. [Google Scholar] [CrossRef]
- Forman, D.L.; Chiu, J.; Restifo, R.J.; Ward, B.A.; Haffty, B.; Ariyan, S. Breast reconstruction in previously irradiated patients using tissue expanders and implants: A potentially unfavorable result. Ann. Plast. Surg. 1998, 40, 360–363, discussion 363–364. [Google Scholar] [CrossRef]
- Bernstein, E.F.; Salomon, G.D.; Harisiadis, L.; Talbot, T.; Harrington, F.; Russo, A.; Uitto, J. Collagen gene expression and wound strength in normal and radiation-impaired wounds. A model of radiation-impaired wound healing. J. Dermatol. Surg. Oncol. 1993, 19, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Gorodetsky, R.; McBride, W.H.; Withers, H.R. Assay of radiation effects in mouse skin as expressed in wound healing. Radiat. Res. 1988, 116, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Mustoe, T.A.; Pierce, G.F.; Thomason, A.; Gramates, P.; Sporn, M.B.; Deuel, T.F. Accelerated healing of incisional wounds in rats induced by transforming growth factor-beta. Science 1987, 237, 1333–1336. [Google Scholar] [CrossRef] [PubMed]
- Mustoe, T.A.; Purdy, J.; Gramates, P.; Deuel, T.F.; Thomason, A.; Pierce, G.F. Reversal of impaired wound healing in irradiated rats by platelet-derived growth factor-BB. Am. J. Surg. 1989, 158, 345–350. [Google Scholar] [CrossRef]
- Tibbs, M.K. Wound healing following radiation therapy: A review. Radiother. Oncol. 1997, 42, 99–106. [Google Scholar] [CrossRef]
- Jagetia, G.C.; Rajanikant, G.K. Effect of curcumin on radiation-impaired healing of excisional wounds in mice. J. Wound Care 2004, 13, 107–109. [Google Scholar] [CrossRef]
- El-Hamoly, T.; El-Denshary, E.S.; Saad, S.M.; El-Ghazaly, M.A. 3-aminobenzamide, a poly (ADP ribose) polymerase inhibitor, enhances wound healing in whole body gamma irradiated model. Wound Repair Regen. 2015, 23, 672–684. [Google Scholar] [CrossRef]
- Galiano, R.D.; Michaels, J.T.; Dobryansky, M.; Levine, J.P.; Gurtner, G.C. Quantitative and reproducible murine model of excisional wound healing. Wound Repair Regen. 2004, 12, 485–492. [Google Scholar] [CrossRef]
- Morissette Martin, P.; Maux, A.; Laterreur, V.; Mayrand, D.; Gagné, V.L.; Moulin, V.J.; Fradette, J. Enhancing repair of full-thickness excisional wounds in a murine model: Impact of tissue-engineered biological dressings featuring human differentiated adipocytes. Acta Biomater. 2015, 22, 39–49. [Google Scholar] [CrossRef]
- Michaels, J.T.; Churgin, S.S.; Blechman, K.M.; Greives, M.R.; Aarabi, S.; Galiano, R.D.; Gurtner, G.C. db/db mice exhibit severe wound-healing impairments compared with other murine diabetic strains in a silicone-splinted excisional wound model. Wound Repair Regen. 2007, 15, 665–670. [Google Scholar] [CrossRef]
- Werier, J.; Ferguson, P.; Bell, R.; Hill, R.; Wunder, J.; O’Sullivan, B.; Kandel, R. Model of radiation-impaired healing of a deep excisional wound. Wound Repair Regen. 2006, 14, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.P.; Brown, S.L.; Georges, G.E.; Hauer-Jensen, M.; Hill, R.P.; Huser, A.K.; Kirsch, D.G.; Macvittie, T.J.; Mason, K.A.; Medhora, M.M.; et al. Animal models for medical countermeasures to radiation exposure. Radiat. Res. 2010, 173, 557–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hegedus, F.; Mathew, L.M.; Schwartz, R.A. Radiation dermatitis: An overview. Int. J. Dermatol. 2017, 56, 909–914. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.J.; Webster, J.; Chung, B.; Marquart, L.; Ahmed, M.; Garantziotis, S. Prevention and treatment of acute radiation-induced skin reactions: A systematic review and meta-analysis of randomized controlled trials. BMC Cancer 2014, 14, 53. [Google Scholar] [CrossRef] [Green Version]
- Iacovelli, N.A.; Galaverni, M.; Cavallo, A.; Naimo, S.; Facchinetti, N.; Iotti, C.; Fallai, C.; Orlandi, E. Prevention and treatment of radiation-induced acute dermatitis in head and neck cancer patients: A systematic review. Future Oncol. 2018, 14, 291–305. [Google Scholar] [CrossRef]
- Lin, L.C.; Que, J.; Lin, L.K.; Lin, F.C. Zinc supplementation to improve mucositis and dermatitis in patients after radiotherapy for head-and-neck cancers: A double-blind, randomized study. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 745–750. [Google Scholar] [CrossRef]
- Vadarli, G.; Angelo-Khattar, M. A Fibroblast-Derived Human Growth Factor Preparation for the Management of Acute Radiodermatitis: A Case Report. Int. Med. Case Rep. J. 2020, 13, 691–696. [Google Scholar] [CrossRef]
- Landry, Y.; Le, O.; Mace, K.A.; Restivo, T.E.; Beausejour, C.M. Secretion of SDF-1alpha by bone marrow-derived stromal cells enhances skin wound healing of C57BL/6 mice exposed to ionizing radiation. J. Cell. Mol. Med. 2010, 14, 1594–1604. [Google Scholar] [CrossRef]
- Huang, S.P.; Huang, C.H.; Shyu, J.F.; Lee, H.S.; Chen, S.G.; Chan, J.Y.; Huang, S.M. Promotion of wound healing using adipose-derived stem cells in radiation ulcer of a rat model. J. Biomed. Sci. 2013, 20, 51. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.S.; Park, B.S.; Sung, J.H.; Yang, J.M.; Park, S.B.; Kwak, S.J.; Park, J.S. Wound healing effect of adipose-derived stem cells: A critical role of secretory factors on human dermal fibroblasts. J. Dermatol. Sci. 2007, 48, 15–24. [Google Scholar] [CrossRef]
- Rehman, J.; Traktuev, D.; Li, J.; Merfeld-Clauss, S.; Temm-Grove, C.J.; Bovenkerk, J.E.; Pell, C.L.; Johnstone, B.H.; Considine, R.V.; March, K.L. Secretion of angiogenic and antiapoptotic factors by human adipose stromal cells. Circulation 2004, 109, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, G.; Fox, J.; Ashton, B.; Middleton, J. Concise review: Mesenchymal stem cells: Their phenotype, differentiation capacity, immunological features, and potential for homing. Stem Cells 2007, 25, 2739–2749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Junqueira, L.C.; Bignolas, G.; Brentani, R.R. Picrosirius staining plus polarization microscopy, a specific method for collagen detection in tissue sections. Histochem. J. 1979, 11, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Classen, J.; Paulsen, F.; Hehr, T.; Bamberg, M.; Budach, W. Effect of gemcitabine on acute and late radiation toxicity of skin and underlying soft tissues to single-dose irradiation in a nude mice model. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 197–205. [Google Scholar] [CrossRef]
- Dombrowsky, A.C.; Schauer, J.; Sammer, M.; Blutke, A.; Walsh, D.W.M.; Schwarz, B.; Bartzsch, S.; Feuchtinger, A.; Reindl, J.; Combs, S.E.; et al. Acute Skin Damage and Late Radiation-Induced Fibrosis and Inflammation in Murine Ears after High-Dose Irradiation. Cancers 2019, 11, 727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thames, H.D., Jr.; Withers, H.R.; Peters, L.J.; Fletcher, G.H. Changes in early and late radiation responses with altered dose fractionation: Implications for dose-survival relationships. Int. J. Radiat. Oncol. Biol. Phys. 1982, 8, 219–226. [Google Scholar] [CrossRef]
- Cosset, J.M.; Mornex, F.; Eschwege, F. Hypofractionation and radiotherapy: “The eternal return”. Cancer Radiother. 2013, 17, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Aldinger, K.A.; Sokoloff, G.; Rosenberg, D.M.; Palmer, A.A.; Millen, K.J. Genetic variation and population substructure in outbred CD-1 mice: Implications for genome-wide association studies. PLoS ONE 2009, 4, e4729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Festing, M.F. Evidence should trump intuition by preferring inbred strains to outbred stocks in preclinical research. ILAR J. 2014, 55, 399–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hymes, S.R.; Strom, E.A.; Fife, C. Radiation dermatitis: Clinical presentation, pathophysiology, and treatment 2006. J. Am. Acad. Dermatol. 2006, 54, 28–46. [Google Scholar] [CrossRef] [PubMed]
- Sheng, X.; Zhou, Y.; Wang, H.; Shen, Y.; Liao, Q.; Rao, Z.; Deng, F.; Xie, L.; Yao, C.; Mao, H.; et al. Establishment and characterization of a radiation-induced dermatitis rat model. J. Cell. Mol. Med. 2019, 23, 3178–3189. [Google Scholar] [CrossRef] [PubMed]
- Joiner, M.C.; Marples, B.; Lambin, P.; Short, S.C.; Turesson, I. Low-dose hypersensitivity: Current status and possible mechanisms. Int. J. Radiat. Oncol. Biol. Phys. 2001, 49, 379–389. [Google Scholar] [CrossRef]
- Sivan, V.; Vozenin-Brotons, M.C.; Tricaud, Y.; Lefaix, J.L.; Cosset, J.M.; Dubray, B.; Martin, M.T. Altered proliferation and differentiation of human epidermis in cases of skin fibrosis after radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 385–393. [Google Scholar] [CrossRef]
- Liu, K.; Kasper, M.; Trott, K.R. Changes in keratinocyte differentiation during accelerated repopulation of the irradiated mouse epidermis. Int. J. Radiat. Biol. 1996, 69, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Turesson, I.; Nyman, J.; Qvarnstrom, F.; Simonsson, M.; Book, M.; Hermansson, I.; Sigurdardottir, S.; Johansson, K.A. A low-dose hypersensitive keratinocyte loss in response to fractionated radiotherapy is associated with growth arrest and apoptosis. Radiother. Oncol. 2010, 94, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Liao, W.; Hei, T.K.; Cheng, S.K. Radiation-Induced Dermatitis is Mediated by IL17-Expressing gammadelta T Cells. Radiat. Res. 2017, 187, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Koh, T.J.; DiPietro, L.A. Inflammation and wound healing: The role of the macrophage. Expert Rev. Mol. Med. 2011, 13, e23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wynn, T.A.; Vannella, K.M. Macrophages in Tissue Repair, Regeneration, and Fibrosis. Immunity 2016, 44, 450–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marangoni, R.G.; Lu, T.T. The roles of dermal white adipose tissue loss in scleroderma skin fibrosis. Curr. Opin. Rheumatol. 2017, 29, 585–590. [Google Scholar] [CrossRef]
- Marangoni, R.G.; Korman, B.D.; Wei, J.; Wood, T.A.; Graham, L.V.; Whitfield, M.L.; Scherer, P.E.; Tourtellotte, W.G.; Varga, J. Myofibroblasts in murine cutaneous fibrosis originate from adiponectin-positive intradermal progenitors. Arthritis Rheumatol. 2015, 67, 1062–1073. [Google Scholar] [CrossRef] [PubMed]
- Shook, B.A.; Wasko, R.R.; Mano, O.; Rutenberg-Schoenberg, M.; Rudolph, M.C.; Zirak, B.; Rivera-Gonzalez, G.C.; Lopez-Giraldez, F.; Zarini, S.; Rezza, A.; et al. Dermal Adipocyte Lipolysis and Myofibroblast Conversion Are Required for Efficient Skin Repair. Cell Stem Cell 2020, 26, 880–895.e6. [Google Scholar] [CrossRef] [PubMed]
- Sugihara, T.; Hattori, Y.; Yamamoto, Y.; Qi, F.; Ichikawa, R.; Sato, A.; Liu, M.Y.; Abe, K.; Kanno, M. Preferential impairment of nitric oxide-mediated endothelium-dependent relaxation in human cervical arteries after irradiation. Circulation 1999, 100, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Venkatesulu, B.P.; Mahadevan, L.S.; Aliru, M.L.; Yang, X.; Bodd, M.H.; Singh, P.K.; Yusuf, S.W.; Abe, J.I.; Krishnan, S. Radiation-Induced Endothelial Vascular Injury: A Review of Possible Mechanisms. JACC Basic Transl. Sci. 2018, 3, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Langley, R.E.; Bump, E.A.; Quartuccio, S.G.; Medeiros, D.; Braunhut, S.J. Radiation-induced apoptosis in microvascular endothelial cells. Br. J. Cancer 1997, 75, 666–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabrys, D.; Greco, O.; Patel, G.; Prise, K.M.; Tozer, G.M.; Kanthou, C. Radiation effects on the cytoskeleton of endothelial cells and endothelial monolayer permeability. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 1553–1562. [Google Scholar] [CrossRef]
- Jourdan, M.M.; Lopez, A.; Olasz, E.B.; Duncan, N.E.; Demara, M.; Kittipongdaja, W.; Fish, B.L.; Mader, M.; Schock, A.; Morrow, N.V.; et al. Laminin 332 deposition is diminished in irradiated skin in an animal model of combined radiation and wound skin injury. Radiat. Res. 2011, 176, 636–648. [Google Scholar] [CrossRef] [Green Version]
- Madden, J.W.; Peacock, E.E., Jr. Studies on the biology of collagen during wound healing. I. Rate of collagen synthesis and deposition in cutaneous wounds of the rat. Surgery 1968, 64, 288–294. [Google Scholar]
- Zomer, H.D.; Trentin, A.G. Skin wound healing in humans and mice: Challenges in translational research. J. Dermatol. Sci. 2018, 90, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Lynch, B.; Bonod-Bidaud, C.; Ducourthial, G.; Affagard, J.S.; Bancelin, S.; Psilodimitrakopoulos, S.; Ruggiero, F.; Allain, J.M.; Schanne-Klein, M.C. How aging impacts skin biomechanics: A multiscale study in mice. Sci. Rep. 2017, 7, 13750. [Google Scholar] [CrossRef] [Green Version]
- Reiser, K.M. Influence of age and long-term dietary restriction on enzymatically mediated crosslinks and nonenzymatic glycation of collagen in mice. J. Gerontol. 1994, 49, B71–B79. [Google Scholar] [CrossRef]
- Delanian, S.; Martin, M.; Bravard, A.; Luccioni, C.; Lefaix, J.L. Abnormal phenotype of cultured fibroblasts in human skin with chronic radiotherapy damage. Radiother. Oncol. 1998, 47, 255–261. [Google Scholar] [CrossRef]
- Miller, J.P.; Borde, B.H.; Bordeleau, F.; Zanotelli, M.R.; LaValley, D.J.; Parker, D.J.; Bonassar, L.J.; Pannullo, S.C.; Reinhart-King, C.A. Clinical doses of radiation reduce collagen matrix stiffness. APL Bioeng. 2018, 2, 031901. [Google Scholar] [CrossRef] [PubMed]
- Gu, Q.; Wang, D.; Gao, Y.; Zhou, J.; Peng, R.; Cui, Y.; Xia, G.; Qing, Q.; Yang, H.; Liu, J.; et al. Expression of MMP1 in surgical and radiation-impaired wound healing and its effects on the healing process. J. Environ. Pathol. Toxicol. Oncol. 2002, 21, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Dewael, S.; Vandevoort, M.; Fabre, G.; Nanhekhan, L. Immediate versus delayed autologous breast reconstruction: A retrospective matched cohort study of irradiated patients. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 1769–1775. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dose | Day 56 | Day 91 | Day 155 |
|---|---|---|---|
| 45 Gy | 6/7 (86%) | NA | NA |
| 60 Gy | 1/7 (14%) | 2/7 (29%) | 6/7 (86%) |
| 80 Gy | 0/8 (0%) | 2/8 (25%) * | NA |
| Healing Quality of the Scarring on the Final Day (Day 17) | |||||
|---|---|---|---|---|---|
| Dose (Gy) Number of Animals | Shedding Time of Scabs | Redness Scoring/3 | Contraction/Waviness Scoring/3 | Non-Union of the Margins Scoring/3 | Full Macroscopic Recovery (%) |
| 0 Gy Ctrl n = 7 | Day 10 | 0/3 | 0.6/3 | 0/3 | 100% (Day 15) |
| 45 Gy n = 4 | Day 13 | 0.7/3 | 1.2/3 | 0.9/3 | 0% |
| 60 Gy n = 6 | Day 16 | 1.8/3 | 2.0/3 | 1.8/3 | 0% |
| 80 Gy n = 6 | Day 15 | 2.1/3 | 2.5/3 | 2.1/3 | 0% |
| UTS Values for Intact Non-Wounded Age-Matched Murine Skin (MPa) (Age in Weeks) (Skin Thickness in µm) | Recovery for Normal Skin Incision (%) (Raw Values in MPa) | Recovery for Irradiated Skin Incision (%) (Raw Values in MPa) |
|---|---|---|
| 5.31 ± 1.14 (22) (1.07 ± 0.09) | 9.80% (0.52 ± 0.16) | 45 Gy: 3.00% (0.16 ± 0.17) |
| 3.37 ± 1.53 (36) (1.25 ± 0.13) | 26.10% (0.88 ± 0.33) | 60 Gy: 8.90% (0.30 ± 0.26) |
| 4.04 ± 0.38 (27) (1.10 ± 0.07) | 20.10% (0.81 ± 0.23) | 80 Gy: 5.70% (0.23 ± 0.29) |
| Modulus of Elasticity for Intact Non-Wounded Age-Matched Murine Skin (MPa) (Age in Weeks) (Skin Thickness in µm) | Recovery for Normal Skin Incision (%) (Raw Values in MPa) | Recovery for Irradiated Skin Incision (%) (Raw Values in MPa) |
|---|---|---|
| 8.35 ± 1.25 (22) (1.07 ± 0.09) | 19.80% (1.65 ± 0.77) | 45 Gy: 2.50% (0.21± 0.32) |
| 9.51± 6.05 (36) (1.25 ± 0.13) | 38.00% (3.61 ± 1.12) | 60 Gy: 8.60% (0.82 ± 0.70) |
| 11.29 ± 2.30 (27) (1.10 ± 0.07) | 33.80% (3.82 ± 1.58) | 80 Gy: 7.40% (0.83 ± 1.52) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diaz, C.; Hayward, C.J.; Safoine, M.; Paquette, C.; Langevin, J.; Galarneau, J.; Théberge, V.; Ruel, J.; Archambault, L.; Fradette, J. Ionizing Radiation Mediates Dose Dependent Effects Affecting the Healing Kinetics of Wounds Created on Acute and Late Irradiated Skin. Surgeries 2021, 2, 35-57. https://doi.org/10.3390/surgeries2010004
Diaz C, Hayward CJ, Safoine M, Paquette C, Langevin J, Galarneau J, Théberge V, Ruel J, Archambault L, Fradette J. Ionizing Radiation Mediates Dose Dependent Effects Affecting the Healing Kinetics of Wounds Created on Acute and Late Irradiated Skin. Surgeries. 2021; 2(1):35-57. https://doi.org/10.3390/surgeries2010004
Chicago/Turabian StyleDiaz, Candice, Cindy J. Hayward, Meryem Safoine, Caroline Paquette, Josée Langevin, Josée Galarneau, Valérie Théberge, Jean Ruel, Louis Archambault, and Julie Fradette. 2021. "Ionizing Radiation Mediates Dose Dependent Effects Affecting the Healing Kinetics of Wounds Created on Acute and Late Irradiated Skin" Surgeries 2, no. 1: 35-57. https://doi.org/10.3390/surgeries2010004
APA StyleDiaz, C., Hayward, C. J., Safoine, M., Paquette, C., Langevin, J., Galarneau, J., Théberge, V., Ruel, J., Archambault, L., & Fradette, J. (2021). Ionizing Radiation Mediates Dose Dependent Effects Affecting the Healing Kinetics of Wounds Created on Acute and Late Irradiated Skin. Surgeries, 2(1), 35-57. https://doi.org/10.3390/surgeries2010004