
Trans-Esophageal Echocardiography of the Descending Aorta and Celiac Trunk as an Intraoperative Monitoring for Median Arcuate Ligament Syndrome (MALS) Treatment: Technique Proposal and Two Case Reports

 ,
,  , , and
, , and 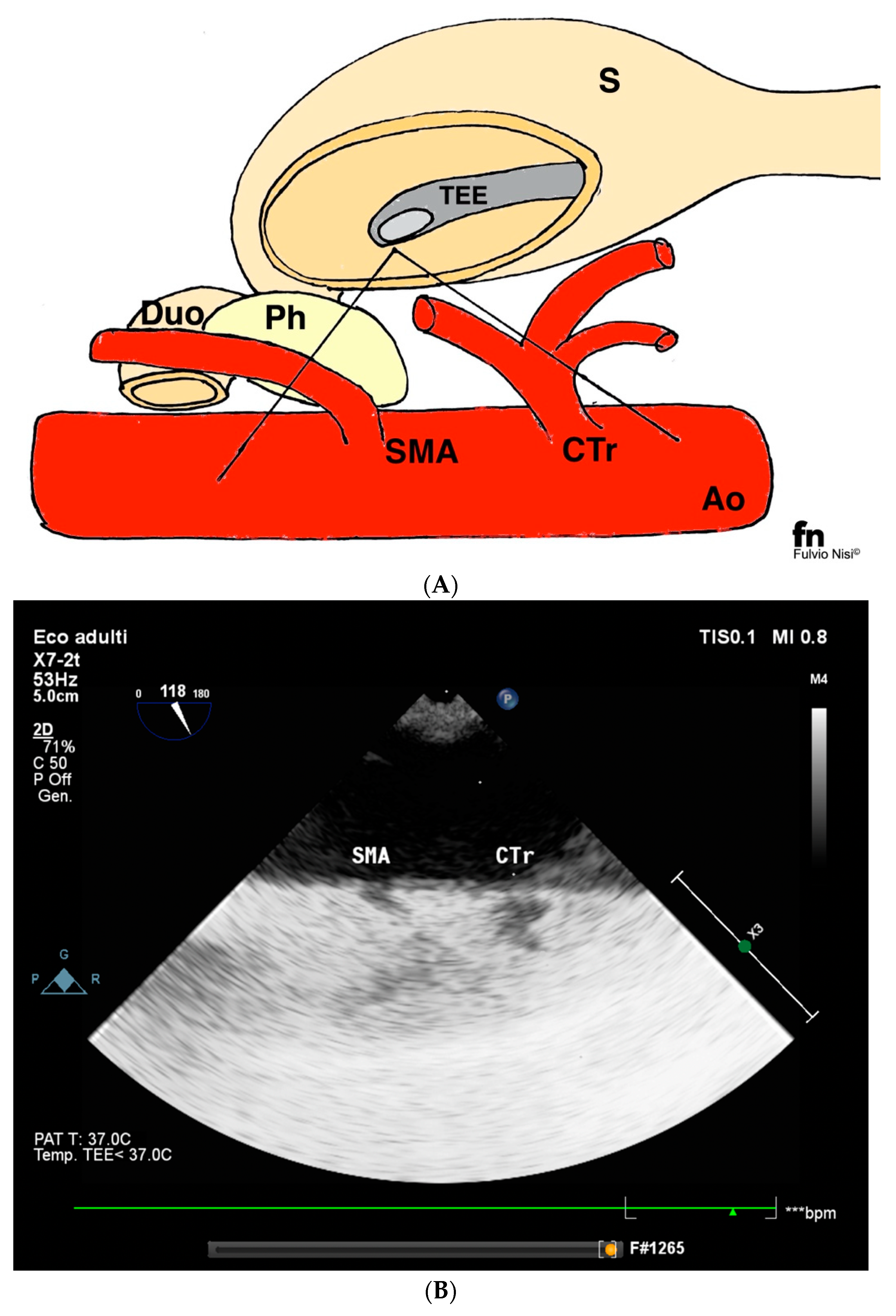{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
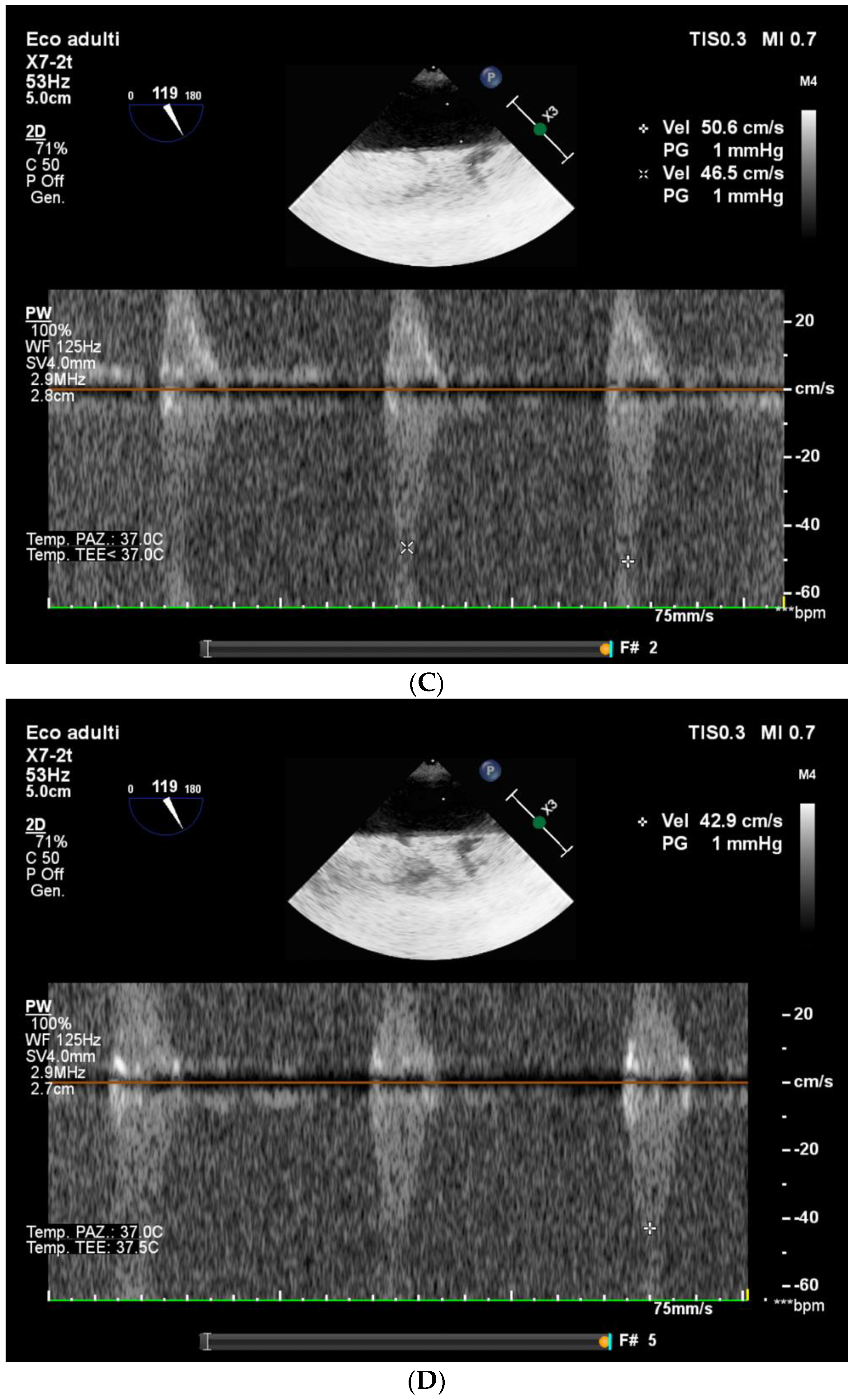
2.1. Technique Description
2.2. Case Report 1
2.3. Case Report 2
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, E.N.; Lamb, K.; Relles, D.; Moudgill, N.; DiMuzio, P.J.; Eisenberg, J.A. Median arcuate ligament syndrome-Review of this rare disease. JAMA Surg. 2016, 151, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, S.; Chaudhary, M. Median arcuate ligament syndrome (Dunbar syndrome). Cardiovasc. Diagn. Ther. 2021, 11, 1172–1176. [Google Scholar] [CrossRef] [PubMed]
- Dyches, R.P.; Eaton, K.J.; Smith, H.F. The Roles of Celiac Trunk Angle and Vertebral Origin in Median Arcuate Ligament Syndrome. Diagnostics 2020, 10, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodall, R.; Langridge, B.; Onida, S.; Ellis, M.; Lane, T.; Davies, A.H. Median arcuate ligament syndrome. J. Vasc. Surg. 2020, 71, 2170–2176. [Google Scholar] [CrossRef] [PubMed]
- Romero-Velez, G.; Barajas-Gamboa, J.S.; Pantoja, J.P.; Corcelles, R.; Rodriguez, J.; Navarrete, S.; Park, W.M.; Kroh, M. A nationwide analysis of median arcuate ligament release between 2010 and 2020: A NSQIP Study. Surg. Endosc. 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sultan, S.A.; Acharya, Y.; Mustafa, M.; Hynes, N. Two Decades of Experience with Chronic Mesenteric Ischaemia and Median Arcuate Ligament Syndrome in a Tertiary Referral Centre: A Parallel Longitudinal Comparative Study. Cureus 2021, 13, e20726. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, H.; Hiraki, S.; Sakamoto, N.; Yaguchi, Y.; Kumano, I.; Yoshida, K.; Matsumoto, Y.; Akase, T.; Horiguchi, H.; Ono, S.; et al. Laparoscopic Treatment for Median Arcuate Ligament Syndrome: The Usefulness of Intraoperative Doppler Ultrasound to Confirm the Decompression of the Celiac Artery. Surg. Laparosc. Endosc. Percutan. Tech. 2012, 22, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Hahn, R.T.; Abraham, T.; Adams, M.S.; Bruce, C.J.; Glas, K.E.; Lang, R.M.; Reeves, S.T.; Shanewise, J.S.; Siu, S.C.; Stewart, W.; et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: Recommendations from the American society of echocardiography and the society of cardiovascular anesthesiologists. Anesth. Analg. 2014, 118, 21–68. [Google Scholar] [CrossRef] [PubMed]
- Orihashi, K.; Matsuura, Y.; Sueda, T.; Shikata, H.; Morita, S.; Hirai, S.; Sueshiro, M.; Okada, K. Abdominal aorta and visceral arteries visualized with transesophageal echocardiography during operations on the aorta. J. Thorac. Cardiovasc. Surg. 1998, 115, 945–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frazin, L.J. Transesophageal echocardiographic detection of thoracic aorta dissection extending into the celiac artery. J. Am. Soc. Echocardiogr. 2003, 16, 1186–1187. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Nagaraja, P.; Gopal, D.; Manjunath, V.; Nagesh, K.S.; Manjunatha, N.; Patel, G.P.; Mishra, S.K. Feasibility of measuring superior mesenteric artery blood flow during cardiac surgery under hypothermic cardiopulmonary bypass using transesophageal echocardiography: An observational study. Ann. Card. Anaesth. 2016, 19, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Moral, S.; Avegliano, G.; Cuéllar, H.; Ballesteros, E.; Rodríguez-Palomares, J.; Teixidó, G.; Galian, L.; Gutiérrez, L.; Evangelista, A. Usefulness of Transesophageal Echocardiography in the Evaluation of Celiac Trunk and Superior Mesenteric Artery Involvement in Acute Aortic Dissection. J. Am. Soc. Echocardiogr. 2021, 34, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Coppalini, G.; Giustiniano, E.; Nisi, F.; Castoro, C.; Civilini, E.; Cecconi, M. Intraoperative trans-esophageal echographic evaluation of the celiac artery flow after arcuate ligament resection in a case of Dunbar Syndrome. A case report. JCIMCR 2021, 2, 1137. [Google Scholar] [CrossRef]
- Duran, M.; Simon, F.; Ertas, N.; Schelzig, H.; Floros, N. Open vascular treatment of median arcuate ligament syndrome. BMC Surg. 2017, 17, 95. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, K.; Hungness, E.S.; Pearson, E.G.; Soper, N.J. Laparoscopic treatment of celiac artery compression syndrome: Case series and review of current treatment modalities. J. Gastrointest. Surg. 2009, 13, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Bayati, I.A.; Gajendran, M.; Davis, B.R.; Diaz, J.R.; McCallum, R.W. Median Arcuate Ligament Syndrome Clinical Presentation, Pathophysiology, and Management: Description of Four Cases. Gastrointest. Disord. 2021, 3, 44–50. [Google Scholar] [CrossRef]
- López-Pardo, F.; Gómez-Navarro, C.; Peiró, J.; Alcázar, M.; Villa, M.; Retegui, G. Transesophageal Echocardiographic Detection of Aortic Dissection with Reentry Site at the Level of the Celiac Artery. Echocardiography 2005, 22, 279–281. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Jariwala, N.; Frazin, L. Should the celiac artery be used as an anatomical marker for the descending thoracic aorta during transesophageal echocardiography? Echocardiography 2016, 33, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Klimas, A.; Lemmer, A.; Bergert, H.; Brodhun, M.; Scholbach, T.; Großer, K. Laparoscopic treatment of celiac artery compression syndrome in children and adolescents. VASA 2015, 44, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Okobi, O.E.; Afuda, B.A.; Boms, M.; Ekpemiro, C.U.; Umeh, N.J.; Nnaji, C.G.; Onyechi, N.P.; Faderin, O.G.; Chiji-Aguma, J.C.; Stephen, E.; et al. Median Arcuate Ligament Syndrome: Management and Literature Review. Cureus 2022, 14, e28889. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lubian, M.; Nisi, F.; Giustiniano, E.; Ripani, U.; Piccioni, F.; Cecconi, M. Trans-Esophageal Echocardiography of the Descending Aorta and Celiac Trunk as an Intraoperative Monitoring for Median Arcuate Ligament Syndrome (MALS) Treatment: Technique Proposal and Two Case Reports. Surgeries 2023, 4, 17-25. https://doi.org/10.3390/surgeries4010003
Lubian M, Nisi F, Giustiniano E, Ripani U, Piccioni F, Cecconi M. Trans-Esophageal Echocardiography of the Descending Aorta and Celiac Trunk as an Intraoperative Monitoring for Median Arcuate Ligament Syndrome (MALS) Treatment: Technique Proposal and Two Case Reports. Surgeries. 2023; 4(1):17-25. https://doi.org/10.3390/surgeries4010003
Chicago/Turabian StyleLubian, Marta, Fulvio Nisi, Enrico Giustiniano, Umberto Ripani, Federico Piccioni, and Maurizio Cecconi. 2023. "Trans-Esophageal Echocardiography of the Descending Aorta and Celiac Trunk as an Intraoperative Monitoring for Median Arcuate Ligament Syndrome (MALS) Treatment: Technique Proposal and Two Case Reports" Surgeries 4, no. 1: 17-25. https://doi.org/10.3390/surgeries4010003
APA StyleLubian, M., Nisi, F., Giustiniano, E., Ripani, U., Piccioni, F., & Cecconi, M. (2023). Trans-Esophageal Echocardiography of the Descending Aorta and Celiac Trunk as an Intraoperative Monitoring for Median Arcuate Ligament Syndrome (MALS) Treatment: Technique Proposal and Two Case Reports. Surgeries, 4(1), 17-25. https://doi.org/10.3390/surgeries4010003