
Fasting during Ramadan: A Comprehensive Review for Primary Care Providers



Abstract
:1. Introduction
2. What Is Ramadan?
3. Do All Muslims Have to Fast during Ramadan?
4. What Do Muslims Eat during Ramadan?
5. Physiology of the Fast
6. Metabolic Effects of Ramadan Fasting
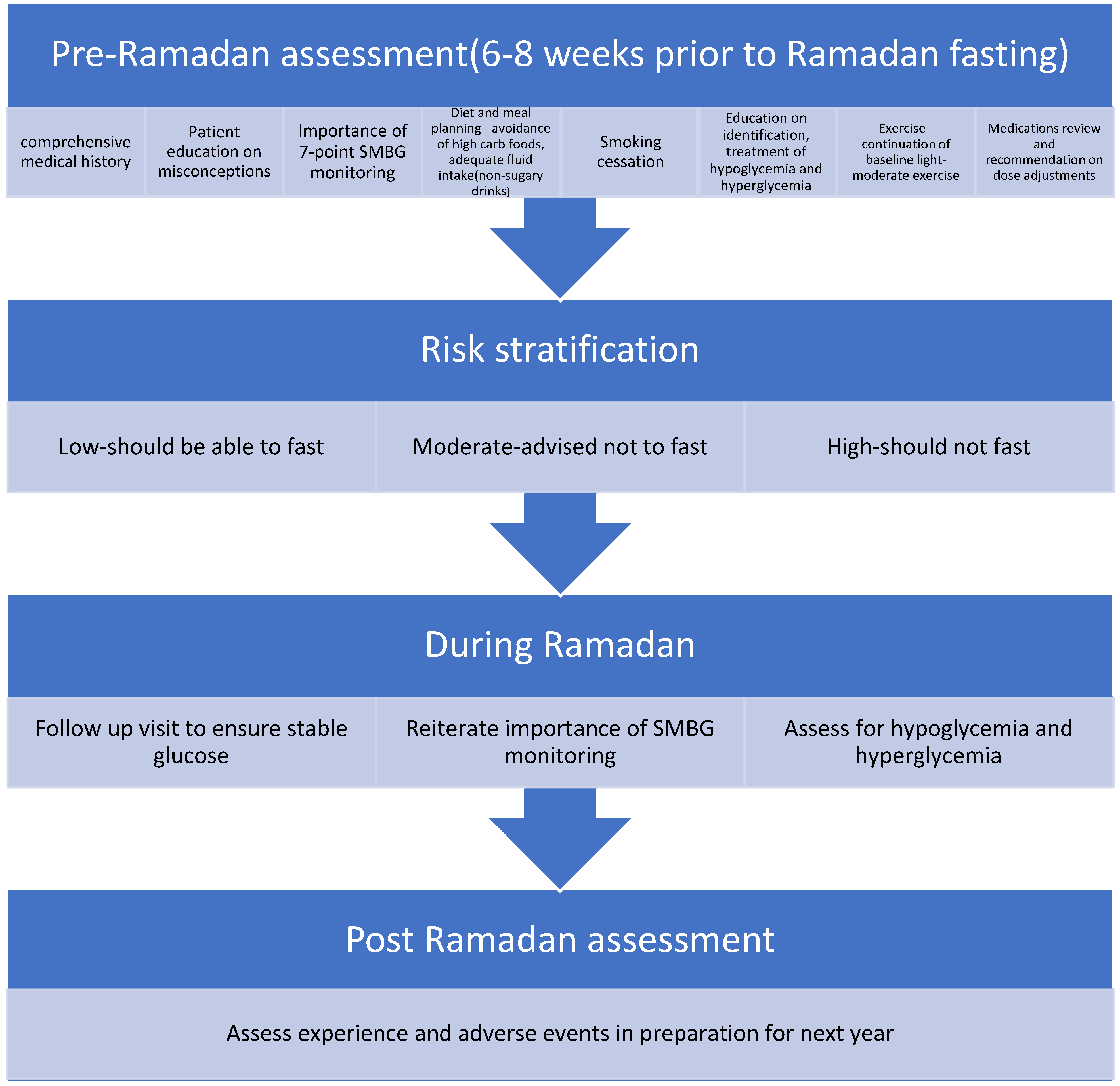
7. Pre-Ramadan Visit
8. Risk Stratification
9. Clearing Patient/Family Misconceptions about Diabetes during Ramadan
10. Knowing When Patients Should Break the Fast
11. Monitoring Blood Glucose
12. Diabetes Medications
13. Insulin
14. Sulfonylureas
15. Metformin
16. Incretin-Based Therapies
17. SGLT2 Inhibitors
18. Alpha-Glucosidase Inhibitors
19. Thiazolidinedione
20. Meglitinides
21. Emergency Room Visits and Hospitalizations
22. Conclusion and Future Applications
23. Take Home Points
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Diabetes Federation and the DAR International Alliance. Diabetes and Ramadan: Practical Guidelines; International Diabetes Federation: Brussels, Belgium, 2021. Available online: www.idf.org/guidelines/diabetes-in-ramadanandwww.daralliance (accessed on 1 January 2022).
- Yılmaz, T.E.; Başara, E.; Yılmaz, T.; Kasım, İ.; Özkara, A. Approaches and awareness of family physicians on diabetes management during Ramadan. Int. J. Clin. Pract. 2021, 75, e14205. [Google Scholar] [CrossRef] [PubMed]
- Beshyah, W.S.; Beshyah, S.A. Bibliometric analysis of the literature on Ramadan fasting and diabetes in the past three decades (1989–2018). Diabetes Res. Clin. Pract. 2019, 151, 313–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karamat, M.A.; Syed, A.; Hanif, W. Review of diabetes management and guidelines during Ramadan. J. R. Soc. Med. 2010, 103, 139–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghani, F. Most Muslims Say They Fast During Ramadan; Pew Research Center: Washington, DC, USA. Available online: https://www.pewresearch.org/fact-tank/2013/07/09/global-median-of-93-of-muslims-say-they-fast-during-ramadan (accessed on 1 January 2022).
- Salti, I.; Bénard, E.; Detournay, B.; Bianchi-Biscay, M.; Le Brigand, C.; Voinet, C.; Jabbar, A. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: Results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care 2004, 27, 2306–2311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quran Word for Word Translation. Available Online Quran word for Word Translation. Available online: https://islamicstudies.info/quran/wordtranslation.php?ch=2&v=183 (accessed on 1 January 2022).
- Al-Arouj, M.; Bouguerra, R.; Buse, J.; Hafez, S.; Hassanein, M.; Ibrahim, M.A.; Ismail-Beigi, F.; El-Kebbi, I.; Khatib, O.; Kishawi, S.; et al. Recommendations for management of diabetes during Ramadan. Diabetes Care 2005, 28, 2305–2311. [Google Scholar] [CrossRef] [Green Version]
- Al-Arouj, M.; Assaad-Khalil, S.; Buse, J.; Fahdil, I.; Fahmy, M.; Hafez, S.; Hassanein, M.; Ibrahim, M.A.; Kendall, D.; Kishawi, S.; et al. Recommendations for Management of Diabetes during Ramadan: Update. Diabetes Care 2010, 33, 1895–1902. [Google Scholar] [CrossRef] [Green Version]
- Hassanein, M.; Al-Arouj, M.; Hamdy, O.; Bebakar, W.M.W.; Jabbar, A.; Al-Madani, A.; Hanif, W.; Lessan, N.; Basit, A.; Tayeb, K.; et al. Diabetes and Ramadan: Practical guidelines. Diabetes Res. Clin. Pract. 2017, 126, 303–316. [Google Scholar] [CrossRef] [Green Version]
- Tootee, A.; Larijani, B. Ramadan fasting and diabetes, latest evidence and technological advancements: 2021 update. J. Diabetes Metab. Disord. 2021, 20, 1085–1091. [Google Scholar] [CrossRef]
- Lamine, F.; Bouguerra, R.; Jabrane, J.; Marrakchi, Z.; Ben Rayana, M.C.; Ben Slama, C.; Gaigi, S. Food intake and high density lipoprotein cholesterol levels changes during ramadan fasting in healthy young subjects. Tunis. Med. 2006, 84, 647–650. [Google Scholar]
- Alkaabi, J.M.; Al-Dabbagh, B.; Ahmad, S.; Saadi, H.F.; Gariballa, S.; Ghazali, M.A. Glycemic indices of five varieties of dates in healthy and diabetic subjects. Nutr. J. 2011, 10, 59. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.H.; Chowdhury, T.A.; Hussain, S.; Syed, A.; Karamat, A.; Helmy, A.; Waqar, S.; Ali, S.; Dabhad, A.; Seal, S.T.; et al. Ramadan and Diabetes: A Narrative Review and Practice Update. Diabetes Ther. 2020, 11, 2477–2520. [Google Scholar] [CrossRef] [PubMed]
- Hassanein, M.; Afandi, B.; Ahmedani, M.Y.; Alamoudi, R.M.; Alawadi, F.; Bajaj, H.S.; Basit, A.; Bennakhi, A.; El Sayed, A.A.; Hamdy, O.; et al. Diabetes and Ramadan: Practical guidelines 2021. Diabetes Res. Clin. Pract. 2022, 185, 109185. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee; Draznin, B.; Aroda, V.R.; Bakris, G.; Benson, G.; Brown, F.M.; Freeman, R.; Green, J.; Huang, E.; Isaacs, D. 6. Glycemic Targets: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45 (Suppl. S1), S83–S96. [Google Scholar] [CrossRef]
- Van Cauter, E.; Polonsky, K.S.; Scheen, A.J. Roles of circadian rhythmicity and sleep in human glucose regulation. Endocr. Rev. 1997, 18, 716–738. [Google Scholar] [CrossRef] [Green Version]
- Aldawi, N.; Darwiche, G.; Abusnana, S.; Elbagir, M.; Elgzyri, T. Initial increase in glucose variability during Ramadan fasting in non-insulin-treated patients with diabetes type 2 using continuous glucose monitoring. Libyan J. Med. 2019, 14, 1535747. [Google Scholar] [CrossRef]
- Patterson, R.E.; Sears, D.D. Metabolic Effects of Intermittent Fasting. Annu. Rev. Nutr. 2017, 37, 371–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Barha, N.S.; Aljaloud, K.S. The Effect of Ramadan Fasting on Body Composition and Metabolic Syndrome in Apparently Healthy Men. Am. J. Mens Health 2019, 13, 1–8. [Google Scholar] [CrossRef]
- Ongsara, S.; Boonpol, S.; Prompalad, N.; Jeenduang, N. The Effect of Ramadan Fasting on Biochemical Parameters in Healthy Thai Subjects. J. Clin. Diagn. Res. 2017, 11, BC14–BC18. [Google Scholar] [CrossRef]
- Adawi, M.; Watad, A.; Brown, S.; Aazza, K.; Aazza, H.; Zouhir, M.; Sharif, K.; Ghanayem, K.; Farah, R.; Mahagna, H.; et al. Ramadan Fasting Exerts Immunomodulatory Effects: Insights from a Systematic Review. Front. Immunol. 2017, 8, 1144. [Google Scholar] [CrossRef] [Green Version]
- Feizollahzadeh, S.; Rasuli, J.; Kheirouri, S.; Alizadeh, M. Augmented plasma adiponectin after prolonged fasting during ramadan in men. Health Promot. Perspect. 2014, 4, 77–81, Published 12 July 2014. [Google Scholar] [CrossRef]
- Ibrahim, M.; Abu Al Magd, M.; Annabi, F.A.; Assaad-Khalil, S.; Ba-Essa, E.M.; Fahdil, I.; Karadeniz, S.; Meriden, T.; Misha’L, A.A.; Pozzilli, P.; et al. Recommendations for management of diabetes during Ramadan: Update 2015. BMJ Open Diabetes Res. Care. 2015, 3, e000108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ibn Taymiyyah, I. The Nature of Fasting; Darussalam: Riyadh, Saudi Arabia, 2000. [Google Scholar]
- How to Treat Low Blood Sugar (Hypoglycemia). Available online: www.cdc.gov/diabetes/basics/low-blood-sugar-treatment.html (accessed on 1 April 2022).
- Hypoglycemia Resources for Healthcare Professionals. Available online: www.diabeteseducator.org/practice/practice-tools/diabetes-management-tools/hypoglycemia-resources (accessed on 1 April 2022).
- Almalki, M.H.; Hussen, I.; Khan, S.A.; Almaghamsi, A.; Alshahrani, F. Assessment of Ramadan Education and Knowledge Among Diabetic Patients. Clin. Med. Insights Endocrinol. Diabetes 2018, 11, 1179551417751611, Published 10 January 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowker, S.L.; Mitchell, C.G.; Majumdar, S.R.; Toth, E.L.; Johnson, J.A. Lack of insurance coverage for testing supplies is associated with poorer glycemic control in patients with type 2 diabetes. Can. Med. Assoc. J. 2004, 171, 39–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- How to Get Unlimited Test Strips and Personal Diabetes Coaching. 2019. diaTribe. Available online: https://diatribe.org/how-get-unlimited-test-strips-and-personal-diabetes-coaching (accessed on 1 April 2022).
- Al-Arouj, M.; Hassoun, A.A.; Medlej, R.; Pathan, M.F.; Shaltout, I.; Chawla, M.S.; Hristoskova, S.; DiTommaso, S.; Kadwa, M.Y. The effect of vildagliptin relative to sulphonylureas in Muslim patients with type 2 diabetes fasting during Ramadan: The VIRTUE study. Int. J. Clin. Pract. 2013, 67, 957–963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassanein, M.; Abdallah, K.; Schweizer, A. A double-blind, randomized trial, including frequent patient-physician contacts and Ramadan-focused advice, assessing vildagliptin and gliclazide in patients with type 2 diabetes fasting during Ramadan: The STEADFAST study. Vasc. Health Risk Manag. 2014, 10, 319–326, Published 28 May 2014. [Google Scholar] [CrossRef] [Green Version]
- Hassanein, M.; Hanif, W.; Malik, W.; Kamal, A.; Geransar, P.; Lister, N.; Andrews, C.; Barnett, A. Comparison of the dipeptidyl peptidase-4 inhibitor vildagliptin and the sulphonylurea gliclazide in combination with metformin, in Muslim patients with type 2 diabetes mellitus fasting during Ramadan: Results of the VECTOR study. Curr. Med. Res. Opin. 2011, 27, 1367–1374. [Google Scholar] [CrossRef]
- Brady, E.M.; Davies, M.J.; Gray, L.J.; Saeed, M.; Smith, D.; Hanif, W.; Khunti, K. A randomized controlled trial comparing the GLP-1 receptor agonist liraglutide to a sulphonylurea as add on to metformin in patients with established type 2 diabetes during Ramadan: The Treat 4 Ramadan Trial. Diabetes Obes. Metab. 2014, 16, 527–536. [Google Scholar] [CrossRef]
- Loh, H.H.; Lim, L.L.; Loh, H.S.; Yee, A. Safety of Ramadan fasting in young patients with type 1 diabetes: A systematic review and meta-analysis. J. Diabetes Investig. 2019, 10, 1490–1501. [Google Scholar] [CrossRef]
- Bin-Abbas, B.S. Insulin pump therapy during Ramadan fasting in type 1 diabetic adolescents. Ann. Saudi Med. 2008, 28, 305–306. [Google Scholar] [CrossRef]
- Elbarbary, N.S. Effectiveness of the low-glucose suspend feature of insulin pump during fasting during Ramadan in type 1 diabetes mellitus. Diabetes Metab. Res. Rev. 2016, 32, 623–633. [Google Scholar] [CrossRef]
- Aravind, S.R.; Al Tayeb, K.; Ismail, S.B.; Shehadeh, N.; Kaddaha, G.; Liu, R.; Balshaw, R.; Lesnikova, N.; Heisel, O.; Girman, C.J.; et al. Hypoglycaemia in sulphonylurea-treated subjects with type 2 diabetes undergoing Ramadan fasting: A five-country observational study. Curr. Med. Res. Opin. 2011, 27, 1237–1242. [Google Scholar] [CrossRef] [PubMed]
- Hassanein, M.; Bashier, A.; Randeree, H.; Abouelmagd, M.; AlBaker, W.; Afandi, B.; Abu Hijleh, O.; Shaltout, I.; Ei-Sharkawy, M.; Dagdelen, S.; et al. Use of SGLT2 inhibitors during Ramadan: An expert panel statement. Diabetes Res. Clin. Pract. 2020, 169, 108465. [Google Scholar] [CrossRef] [PubMed]
- Kast, R.E. Acarbose related diarrhea: Increased butyrate upregulates prostaglandin E. Inflamm. Res. 2002, 51, 117–118. [Google Scholar] [CrossRef] [PubMed]
- Ruling on Injections and Intravenous Fluids for One Who Is Fasting, and the Impact of the Intention (Niyyah) on Invalidating the Fast. Available online: https://islamqa.info/en/answers/250660/ruling-on-injections-and-intravenous-fluids-for-one-who-is-fasting-and-the-impact-of-the-intention-niyyah-on-invalidating-the-fast (accessed on 1 January 2022).




{kind=link}
{kind=link}
{kind=link}
| Risk Factors | Score |
|---|---|
| Diabetes type and duration | |
| Type 1 diabetes | 1 |
| Type 2 diabetes | 0 |
| Duration of diabetes | |
| Duration ≥ 10 years | 1 |
| Duration < 10 years | 0 |
| History of hypoglycemia and hypoglycemia unawareness | |
| Hypoglycemia unawareness | 6.5 |
| Recent severe hypoglycemia | 5.5 |
| Recurrent hypoglycemia | 3.5 |
| Hypoglycemia < once a week | 1 |
| No hypoglycemia | 0 |
| Glycemic control | |
| A1c > 9% | 2 |
| A1c 7.5–9% | 1 |
| A1c < 7.5% | 0 |
| Type of Treatment | |
| Multiple daily premixed insulin regimen | 3 |
| Basal bolus regimen/Insulin pump | 2.5 |
| Once daily premixed insulin | 2 |
| Basal insulin only | 1.5 |
| Older generation sulfonylureas (Glibenclamide) | 1 |
| Second generation sulfonylureas(SU) or Repaglinide | 0.5 |
| Non-insulin and non-SU agents | 0 |
| Self-monitoring of blood glucose(SMBG) | |
| No adequate SMBG checks | 2 |
| Suboptimal SMBG checks | 1 |
| Adequate SMBG checks | 0 |
| Occurrence of Diabetic ketoacidosis/Hyperglycemic hyperosmolar state | |
| In last 3 months | 3 |
| In the last 6 month | 2 |
| In the last 12 months | 1 |
| None | 0 |
| Cardiovascular complications/co-morbidities | |
| Unstable | 6.5 |
| Stable | 2 |
| None | 0 |
| Renal complications/co-morbidities | |
| GFR < 30 mL/min/Stage 4 CKD | 6.5 |
| GFR 30–44 mL/min/Stage 3b CKD | 4 |
| GFR 45–59 mL/min/Stage 3a CKD | 2 |
| GFR ≥ 60 mL/min | 0 |
| Pregnancy | |
| Blood glucose not within target range | 6.5 |
| Blood glucose within target range | 3.5 |
| Not pregnant | 0 |
| Frailty and cognitive function | |
| Impaired cognition or Frail | 6.5 |
| >70 year without home support | 3.5 |
| None | 0 |
| Physical labor | |
| High intense | 4 |
| Moderate intense | 2 |
| None | 0 |
| Prior Ramadan experience | |
| Negative experience | 1 |
| No particular experience | 0 |
| Fasting hours based on location | |
| ≥16 h | 1 |
| <16 h | 0 |
| Score 0–3 Low risk | Should be able to fast |
| Score 3.5–6 Moderate risk | Advised not to fast |
| Score > 6 High risk | Should not fast |
| Misconception | Reality Supported by Evidence |
|---|---|
| Pricking my fingers and drawing blood to check blood glucose breaks my fast | Taking small amounts of blood for medical testing does not break the fast [24,25] |
| Injecting insulin breaks my fast (This includes insulin pumps) | Injected medications that provide no caloric contribution do not break the fast [24,25] |
| I cannot abstain from fasting or break my fast due to complications from my diabetes | Muslims facing acute or chronic illness that places their wellbeing at jeopardy can avoid fasting or break a fast [24,25] |
| Study | Study Design | Conclusions |
|---|---|---|
| VIRTUE | RCT of 1300 participants in Asia and the Middle East who fasted during Ramadan—684 treated with Vildagliptin and 631 treated with Sulfonylurea therapy in addition to Metformin and/or lifestyle change. | Fewer participants experienced hypoglycemic events in the Vildagliptin study arm compared to the Sulfonylurea study arm (5.4% vs. 19.8% p < 0.001). An increased proportion of participants in the Sulfonylurea arm experienced adverse events consisting mostly of hypoglycemic events compared to the Vildagliptin arm (22.8% vs. 10.2%). Vildagliptin may thus be a safer option than Sulfonylurea in managing type 2 diabetes during Ramadan fasting [31] |
| STEADFAST | Double Blind RCT of 557 participants with type 2 diabetes who fasted during Ramadan randomized to receive either Vildagliptin or Gliclazide plus Metformin. | Vildagliptin is safe for use by type 2 diabetes during Ramadan and is associated with lower risk of hypoglycemic events compared to Gliclazide (3.0% vs. 7.0%, respectively p = 0.039) [32] |
| VECTOR | RCT of 72 participants with type 2 diabetes who fasted during Ramadan—30 participants took Vildagliptin and 41 took Gliclazide in addition to Metformin therapy | No participants in the Vildagliptin arm experienced a hypoglycemic event compared to 35 hypoglycemic events in the Gliclazide arm [34]. Vildagliptin lowered the mean HbA1c from 7.6% to 7.2% compared to no effect at baseline HbA1c 7.2% in the Gliclazide arm [33] |
| Treat Ramadan 4 Trial | RCT of 99 participants with type 2 diabetes who fasted in Ramadan—randomly assigned to Liraglutide or Sulfonylurea. | Significant weight loss and diastolic blood pressure were observed in the Liraglutide arm compared to Sulfonylurea arm. No episodes of severe hypoglycemia occurred in either group, but the Sulfonylurea arm reported instances of blood glucose falling below threshold of 3.9 mmol/L more than Liraglutide group [34]. |
| Type of Insulin | Dosing Frequency | Recommended Change |
|---|---|---|
| Basal insulin (insulin glargine/NPH/Degludec/Detemir) | Once daily | Reduce dose by 15–30% and Take at Iftar (sunset meal) |
| Basal insulin (insulin glargine/NPH/Degludec/Detemir) | Twice daily | Take usual morning dose at Iftar (sunset meal), Reduce evening dose by 50% and Take at Suhoor (pre-dawn meal) |
| Short-acting insulin/Bolus insulin | Take normal dose at Iftar (sunset meal), Skip lunch time dose and Reduce Suhoor (pre-dawn meal) dose by 25–50% |
| Pre-Sunset, Pre-Dawn Blood Glucose | Rapid- or Short-Acting Insulin Dose Adjustment |
|---|---|
| >250 mg/dL | Increase dose by 20% |
| >180 mg/dL | Increase dose by 10% |
| 100–180 mg/dL | No change |
| <100 mg/dL or symptoms of hypoglycemia | Reduce dose by 10% |
| <70 mg/dL | Reduce dose by 20% and preferably avoid fast |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, S.; Khokhar, N.; Shubrook, J.H. Fasting during Ramadan: A Comprehensive Review for Primary Care Providers. Diabetology 2022, 3, 276-291. https://doi.org/10.3390/diabetology3020019
Ahmed S, Khokhar N, Shubrook JH. Fasting during Ramadan: A Comprehensive Review for Primary Care Providers. Diabetology. 2022; 3(2):276-291. https://doi.org/10.3390/diabetology3020019
Chicago/Turabian StyleAhmed, Sumera, Natasha Khokhar, and Jay H. Shubrook. 2022. "Fasting during Ramadan: A Comprehensive Review for Primary Care Providers" Diabetology 3, no. 2: 276-291. https://doi.org/10.3390/diabetology3020019
APA StyleAhmed, S., Khokhar, N., & Shubrook, J. H. (2022). Fasting during Ramadan: A Comprehensive Review for Primary Care Providers. Diabetology, 3(2), 276-291. https://doi.org/10.3390/diabetology3020019