

Diabetes Management in Danish Primary School: A Survey of Experiences of Parents of Children with Type 1 Diabetes

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
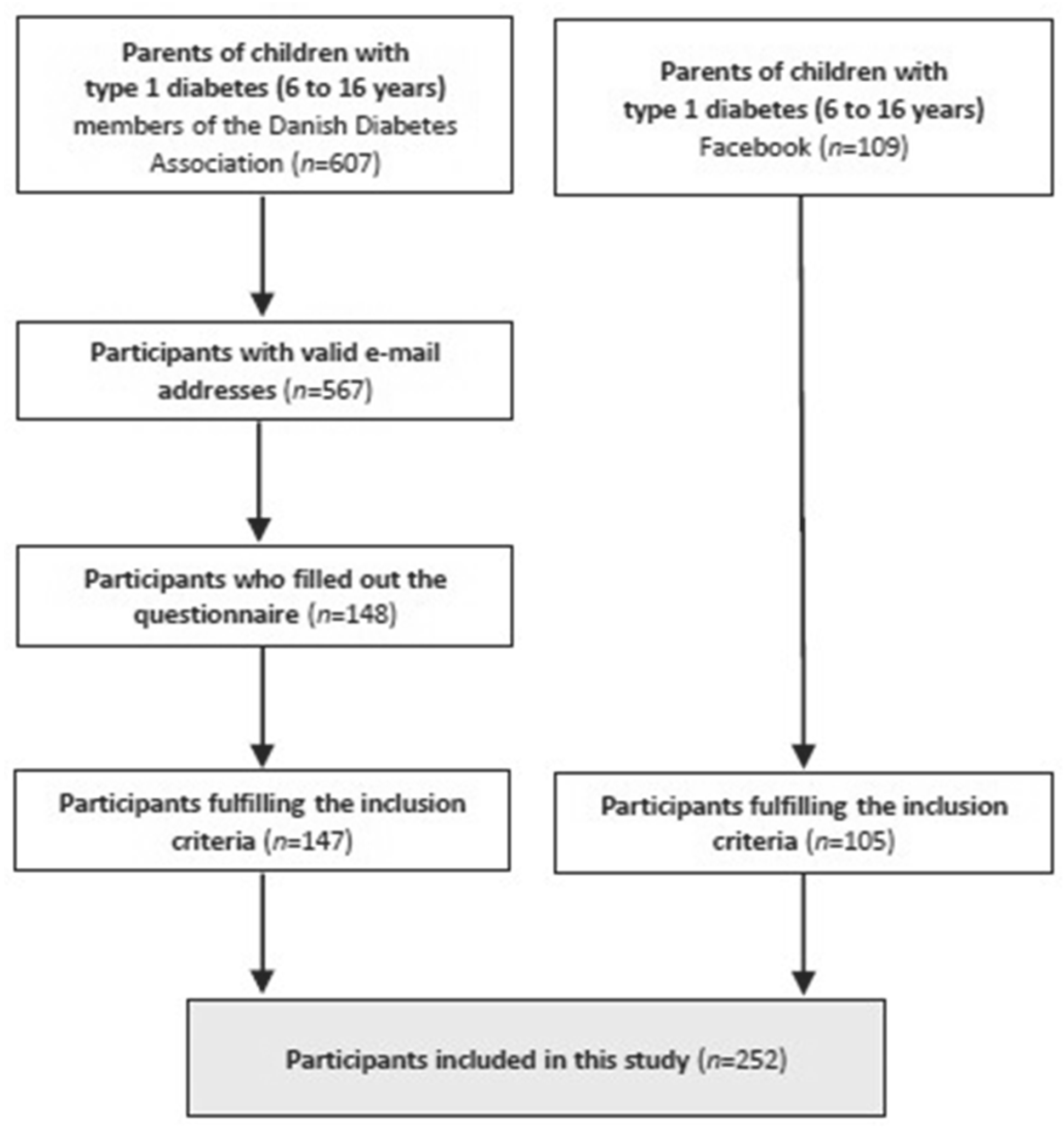
3.1. Study Population
3.2. Diabetes Care in School
3.3. Indicators of Mental Health and Well-Being in School
3.4. Being a Parent of a Child with T1D
3.5. Subgroup Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Parents (n = 252) | The Danish Population (30–54 Years) * | |
| Females | 88.9 | 49.6 |
| 30–34 years | 6.3 | 19.6 |
| 35–39 years | 9.5 | 17.8 |
| 40–44 years | 31.7 | 19.4 |
| 45–49 years | 34.9 | 21.3 |
| 50–54 years | 14.7 | 22.0 |
| Above 55 years | 2.4 | - |
| Primary and lower secondary | 1.6 | 15.5 |
| Vocational education and training | 7.6 | 32.9 |
| General upper secondary | 4.0 | 5.6 |
| Short-cycle programs | 10.8 | 6.4 |
| Medium-cycle programs | 56.4 | 21.1 |
| Long-cycle programs | 18.8 | 17.2 |
| Other | 0.8 | 1.3 |
| Employed | 88.0 | 81.1 |
| Unemployed | 6.8 | 16.2 |
| Other | 5.2 | 2.7 |
| Capital Region of Denmark | 22.6 | 34.0 |
| Region Zealand | 20.2 | 14.1 |
| Region of Southern Denmark | 23.4 | 20.2 |
| Central Denmark Regions | 21.8 | 22.3 |
| North Denmark Region | 12.1 | 9.5 |
References
- Diabetes Control and Complications Trial Research Group. The Effect of Intensive Treatment of Diabetes on the Development and Progression of Long-Term Complications in Insulin-Dependent Diabetes Mellitus. N. Engl. J. Med. 1993, 329, 977–986. [Google Scholar] [CrossRef] [PubMed]
- Diabetes Control and Complications Trial Research Group. Effect of intensive diabetes treatment on the development and progression of long-term complications in adolescents with insulin-dependent diabetes mellitus: Diabetes Control and Complications Trial. J. Pediatr. 1994, 125, 177–188. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, A.M.; Lindgren, S.; Mengeling, M.A.; Tsalikian, E.; Engvall, J.C. Factors associated with academic achievement in children with type 1 diabetes. Diabetes Care 2003, 26, 112–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCarthy, A.M.; Lindgren, S.; Mengeling, M.A.; Tsalikian, E.; Engvall, J.C. Effects of diabetes on learning in children. Pediatrics 2002, 109, e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindkvist, E.B.; Thorsen, S.U.; Paulsrud, C.; Thingholm, P.R.; Eriksen, T.L.M.; Gaulke, A.; Skipper, N.; Svensson, J. Association of type 1 diabetes and educational achievement in 16–20-year-olds: A Danish nationwide register study. Diabet. Med. 2021, 39, e14673. [Google Scholar] [CrossRef]
- Knight, M.F.; Perfect, M.M.; Madison, F. Glycemic control influences on academic performance in youth with Type 1 diabetes. Sch. Psychol. 2019, 34, 646–655. [Google Scholar] [CrossRef]
- Bratina, N.; Forsander, G.; Annan, F.; Wysocki, T.; Pierce, J.; Calliari, L.E.; Parcaud, D.; Adolfsson, P.; Dovc, K.; Middlehurst, A.; et al. ISPAD Clinical Practice Consensus Guidelines 2018: Management and support of children and adolescents with type 1 diabetes in school. Pediatr. Diabetes 2018, 19, 287–301. [Google Scholar] [CrossRef]
- Lange, K.; Jackson, C.; Deeb, L. Diabetes care in schools—The disturbing facts. Pediatr. Diabetes 2009, 10, 28–36. [Google Scholar] [CrossRef]
- Piaget, J.; Inhelder, B. La Psychologie de L’enfant; Presses Universitaires de France: Paris, France, 1968. [Google Scholar]
- Christie, D. How do children and adolescents understand their diabetes? Pract. Diabetes 2019, 36, 117a–120a. [Google Scholar] [CrossRef]
- Mahapatra, S. Development of Planning Behaviour and Decision Making Ability of Children. J. Educ. Practice. 2016, 7, 74–77. [Google Scholar]
- Kelo, M.; Martikainen, M.; Eriksson, E. Self-care of school-age children with diabetes: An integrative review. J. Adv. Nurs. 2011, 67, 2096–2108. [Google Scholar] [CrossRef]
- Global Self-Care Federation. What Is Self-Care? Available online: https://www.selfcarefederation.org/what-is-self-care (accessed on 5 May 2022).
- The Danish Diabetes Association. Skolebørn og Diabetes (EN: School Children and Diabetes). 2007. Available online: https://diabetes.dk/forskning/for-fagfolk/projekter-og-undersogelser#anchor-id-undersoegelser-fra-arkivet-skoleboern-og-diabetes (accessed on 28 April 2022).
- Ducat, L.; Philipson, L.H.; Anderson, B.J. The Mental Health Comorbidities of Diabetes. JAMA 2014, 312, 691–692. [Google Scholar] [CrossRef]
- Ministry of Children and Education. Regler om Inklusion (EN: Rules of Inclusion). Available online: https://www.uvm.dk/folkeskolen/laering-og-laeringsmiljoe/inklusion/regler-om-inklusion (accessed on 28 April 2022).
- Kingod, N.; Grabowski, D. In a vigilant state of chronic disruption: How parents with a young child with type 1 diabetes negotiate events and moments of uncertainty. Sociol Health Illn. 2020, 42, 1473–1487. [Google Scholar] [CrossRef]
- The Danish Health Data Authority. Udvalgte Kroniske Sygdomme og Svære Psykiske Lidelser (EN: Selected Chronic Diseases and Severe Mental Disorders). 2021. Available online: https://www.esundhed.dk/Registre/Udvalgte-kroniske-sygdomme-og-svaere-psykiske-lidelser (accessed on 17 January 2022).
- Särnblad, S.; Berg, L.; Detlofsson, I.; Jönsson, A.; Forsander, G. Diabetes management in Swedish schools: A national survey of attitudes of parents, children, and diabetes teams. Pediatr. Diabetes 2014, 15, 550–556. [Google Scholar] [CrossRef]
- Särnblad, S.; Åkesson, K.; Fernström, L.; Ilvered, R.; Forsander, G. Improved diabetes management in Swedish schools: Results from two national surveys. Pediatr. Diabetes 2016, 18, 463–469. [Google Scholar] [CrossRef]
- Statistics Denmark. StatBank. 2022. Available online: https://www.dst.dk/en (accessed on 12 January 2022).
- Smith, L.B.; Terry, A.; Bollepalli, S.; Rechenberg, K. School-Based Management of Pediatric Type 1 Diabetes: Recommendations, Advances, and Gaps in Knowledge. Curr. Diab. Rep. 2019, 19, 37. [Google Scholar] [CrossRef]
- Hawkes, P.H.; McDarby, V.; Cody, D. Fear of hypoglycemia in parents of children with type 1 diabetes. J. Paediatr. Child Health 2014, 50, 639–642. [Google Scholar] [CrossRef]
- Haugstvedt, A.; Wentzel-Larsen, T.; Graue, M.; Søvik, O.; Rokne, B. Fear of hypoglycaemia in mothers and fathers of children with Type 1 diabetes is associated with poor glycaemic control and parental emotional distress: A population-based study. Diabet. Med. 2010, 27, 72–78. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, F.L.; Denham, S.; Heh, V.; Wapner, A.; Shubrook, J. Experiences of Children and Adolescents with type 1 diabetes in school: Survey of children, parents and schools. Diabetes Spectr. 2010, 23, 47–55. [Google Scholar] [CrossRef] [Green Version]
- McCollum, D.C.; Mason, O.; Codd, M.B.; O’Grady, M.J. Management of type 1 diabetes in primary schools in Ireland: A cross-sectional survey. Ir. J. Med. Sci. 2018, 188, 835–841. [Google Scholar] [CrossRef]
- Eriksen, T.L.M.; Gaulke, A.; Skipper, N.; Svensson, J. The impact of childhood health shocks on parental labor supply. J. Health Econ. 2021, 78, 102486. [Google Scholar] [CrossRef] [PubMed]

| Parents (n = 252) | The Danish Population (30–54 Years) * | |
|---|---|---|
| Females | 88.9 | 49.6 |
| 30–39 years | 15.8 | 37.4 |
| 40–49 years | 66.6 | 40.7 |
| 50–54 years | 14.7 | 22.2 |
| Above 55 years | 2.4 | - |
| Compulsory education 1 | 1.6 | 15.5 |
| Secondary education 2 | 11.6 | 38.5 |
| Post-secondary education 3 | 86.0 | 44.7 |
| Employed | 88.0 | 81.1 |
| Unemployed | 6.8 | 16.2 |
| Children with Type 1 Diabetes (n = 252) | The Danish Population (6–16 Years) * | |
|---|---|---|
| Females | 56.3 | 48.7 |
| 6–8 years | 9.8 | 27.8 |
| 9–11 years | 29.9 | 30.9 |
| 12–14 years | 43.5 | 32.0 |
| 15–16 years | 16.8 | 9.3 |
| Municipal school | 73.1 | 78.7 |
| Private or free school | 24.5 | 18.4 |
| Boarding school | 1.2 | 1.3 |
| Other school | 1.2 | 1.6 |
| 0. to 3. grade | 25.4 | 36.1 |
| 4. to 6. grade | 42.0 | 31.8 |
| 7. to 9. grade | 32.6 | 32.1 |
| 0–5 years at diabetes debut | 33.4 | - |
| 6–8 years at diabetes debut | 30.6 | - |
| 9–12 years at diabetes debut | 31.8 | - |
| ≥13 years at diabetes debut | 4.1 | - |
| Does the Child Have a Designated Staff Member Responsible for Support in Diabetes Self-Care during School Hours? | Children <12 Years (n = 98) | Children ≥12 Years (n = 146) | Total (n = 244) |
|---|---|---|---|
| Yes | 51.0 | 13.0 | 28.3 |
| No | 37.8 | 63.0 | 52.9 |
| No, but previously yes | 11.2 | 24.0 | 18.9 |
| (n = 239) | To a Great Extent | To Some Extent | To a Lesser Extent | Not at All | p | ||
|---|---|---|---|---|---|---|---|
| To what extent do you experience good parent–school cooperation? Designated staff member YES Designated staff member NO | 41.4 69.7 30.6 | 35.1 22.7 39.9 | 17.2 7.6 20.8 | 6.3 0.0 8.7 | <0.001 *** | ||
| … the school engaging in having a student with diabetes? Designated staff member YES Designated staff member NO | 28.0 54.5 17.9 | 33.1 33.3 32.9 | 25.5 10.6 31.2 | 13.4 1.5 17.9 | <0.001 *** | ||
| … that the school is meeting the child’s individual need in relation to diabetes? Designated staff member YES Designated staff member NO | 34.3 63.6 23.1 | 30.5 19.7 34.7 | 26.4 15.2 30.6 | 8.8 1.5 11.6 | <0.001 *** | ||
| Comfortable | Slightly Comfortable | Neither Nor | Slightly Uncomfortable | Un- comfortable | Do Not Know | p | |
| How comfortable are you with the school’s ability in managing diabetes during school hours? (n = 237) Designated staff member YES Designated staff member NO | 38.8 69.7 26.9 | 17.3 15.2 18.1 | 11.8 3.0 15.2 | 15.2 10.6 17.0 | 14.3 1.5 19.3 | 2.5 0.0 3.5 | <0.001 *** |
| … the designated school staff member’s ability in managing diabetes during school hours? (n = 66) | 77.3 | 12.1 | 6.1 | 1.5 | 1.5 | 1.5 | - |
| (n = 233) | All the Time | Often | Now and Then | Rarely | Never | Do Not Know | p |
| How often do you experience that your child is excluded from school events due to diabetes? | 1.3 | 3.9 | 12.4 | 15.0 | 64.8 | 2.6 | 0.81 |
| … is unwantedly left alone in managing diabetes? Designated staff member YES Designated staff member NO | 4.7 0.0 6.5 | 15.0 4.6 19.0 | 23.2 20.0 24.4 | 28.8 30.8 28.0 | 26.2 44.6 19.0 | 2.1 0.0 3.0 | <0.001 *** |
| (n = 231) | To a Great Extent | To Some Extent | To a Lesser Extent | Not at All | p | ||
|---|---|---|---|---|---|---|---|
| To what extent do you experience your child as being happy in school? | 55.8 | 30.3 | 11.3 | 2.6 | 0.35 | ||
| … as feeling comfortable in school? Designated staff member YES Designated staff member NO | 58.9 73.8 53.0 | 29.0 21.5 31.9 | 10.4 4.6 12.7 | 1.7 0.0 2.4 | 0.022 * | ||
| … as being concerned about life with diabetes? | 24.2 | 46.3 | 22.5 | 6.9 | 0.77 | ||
| … as being offered support in school to cope with psychological challenges of diabetes? Designated staff member YES Designated staff member NO | 9.5 16.9 6.6 | 18.2 24.6 15.7 | 23.4 23.1 23.5 | 48.9 35.4 54.2 | 0.014 * | ||
| (n = 231) | All the Time | Often | Now and Then | Rarely | Never | Do Not Know | p |
| As a consequence of diabetes, how often do you experience your child as feeling excluded? | 0.4 | 12.1 | 27.7 | 32.5 | 26.0 | 1.3 | 0.15 |
| … is your child absent from school? | 0.4 | 7.8 | 31.6 | 45.5 | 14.7 | 0.0 | 0.32 |
| (n = 229) | To a Great Extent | To Some Extent | To a Lesser Extent | Not at All | p | ||
|---|---|---|---|---|---|---|---|
| To what extent do you feel comfortable having your child in school? Designated staff member YES Designated staff member NO | 50.7 60.0 47.0 | 37.6 36.9 37.8 | 7.4 3.1 9.1 | 4.4 0.0 6.1 | 0.049 * | ||
| … do you experience lack of support to the child negatively affecting your work life? | 14.0 | 32.3 | 30.1 | 23.6 | 0.32 | ||
| … do you experience it challenging to be parent of a child with diabetes? | 50.2 | 34.5 | 14.4 | 0.9 | 0.14 | ||
| (n = 229) | All the Time | Often | Now and Then | Rarely | Never | Do Not Know | p |
| How often are you concerned about your child’s risk of low blood sugar? | 16.6 | 31.9 | 33.6 | 15.3 | 2.2 | 0.4 | 0.49 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iken, M.K.; Mateu, N.C.; Johansen, L.B.; Pilgaard, K.A.; Mouritsen, A.K.; Schou, A.J.; Høst, L.S.; Nannsen, A.Ø.; Kristensen, K.; Hangaard, S.; et al. Diabetes Management in Danish Primary School: A Survey of Experiences of Parents of Children with Type 1 Diabetes. Diabetology 2023, 4, 108-118. https://doi.org/10.3390/diabetology4010012
Iken MK, Mateu NC, Johansen LB, Pilgaard KA, Mouritsen AK, Schou AJ, Høst LS, Nannsen AØ, Kristensen K, Hangaard S, et al. Diabetes Management in Danish Primary School: A Survey of Experiences of Parents of Children with Type 1 Diabetes. Diabetology. 2023; 4(1):108-118. https://doi.org/10.3390/diabetology4010012
Chicago/Turabian StyleIken, Mia K., Nuri C. Mateu, Lise B. Johansen, Kasper A. Pilgaard, Annette K. Mouritsen, Anders J. Schou, Line S. Høst, Anne Ø. Nannsen, Kurt Kristensen, Stine Hangaard, and et al. 2023. "Diabetes Management in Danish Primary School: A Survey of Experiences of Parents of Children with Type 1 Diabetes" Diabetology 4, no. 1: 108-118. https://doi.org/10.3390/diabetology4010012
APA StyleIken, M. K., Mateu, N. C., Johansen, L. B., Pilgaard, K. A., Mouritsen, A. K., Schou, A. J., Høst, L. S., Nannsen, A. Ø., Kristensen, K., Hangaard, S., Madsen, M., & Grabowski, D. (2023). Diabetes Management in Danish Primary School: A Survey of Experiences of Parents of Children with Type 1 Diabetes. Diabetology, 4(1), 108-118. https://doi.org/10.3390/diabetology4010012