
Patients’ Perspective on Barriers to Utilization of a Diabetic Retinopathy Screening Service

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Design and Sampling Techniques
2.3. Inclusion and Exclusion Criteria
2.4. Data Collection Procedure
2.5. Data Management and Analysis
3. Results
3.1. Sociodemographic Features of the Respondents
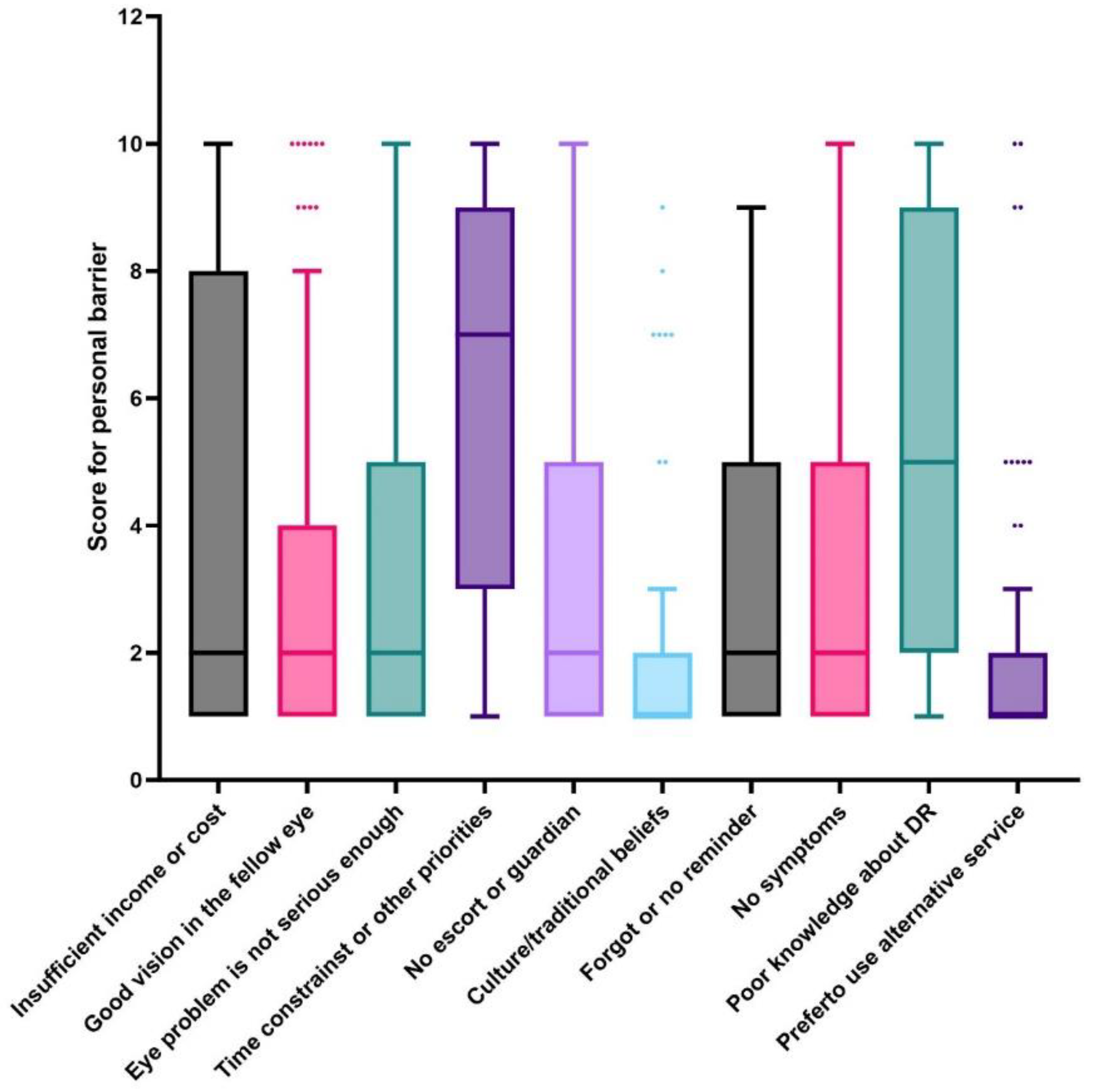
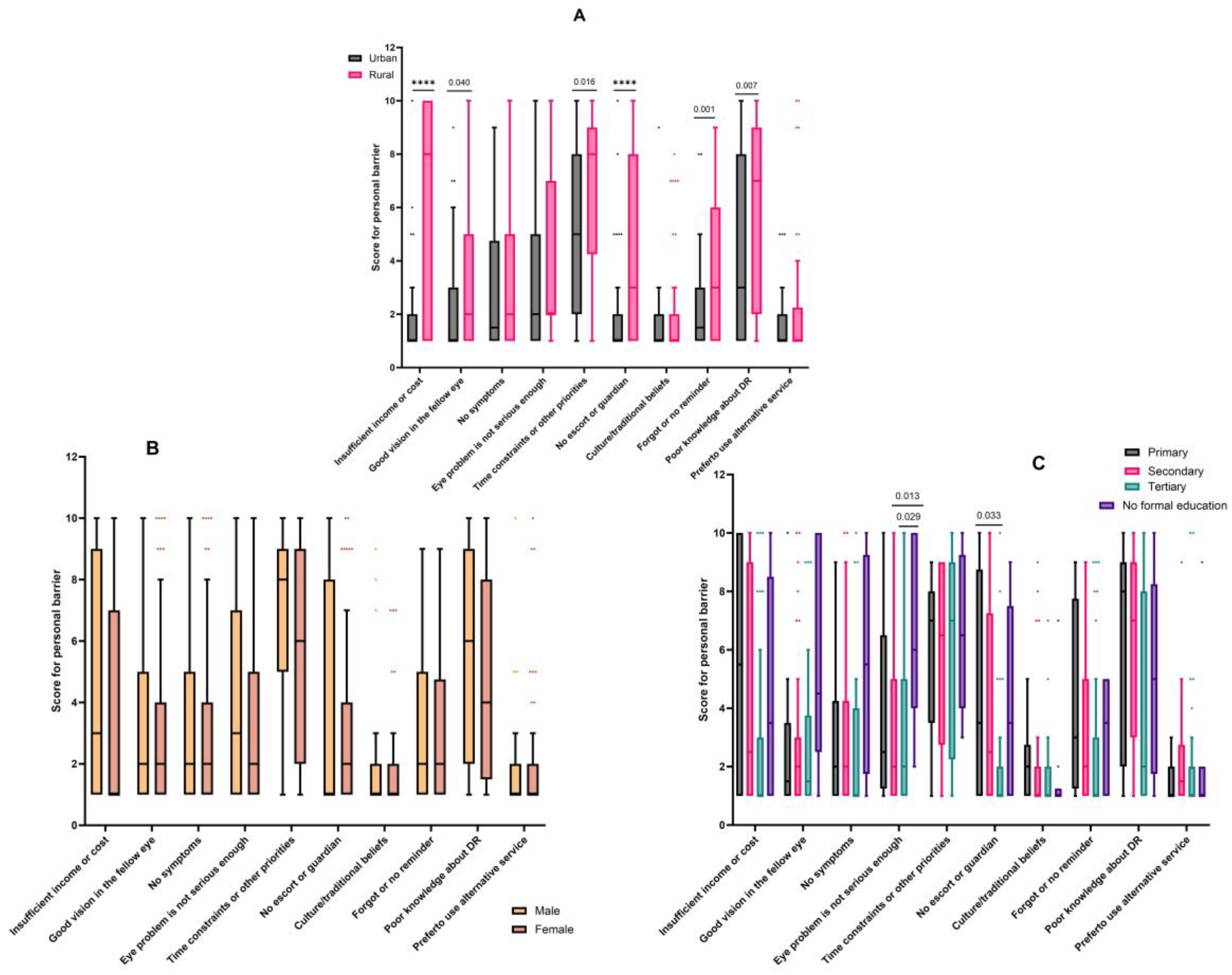
3.2. Personal Barriers
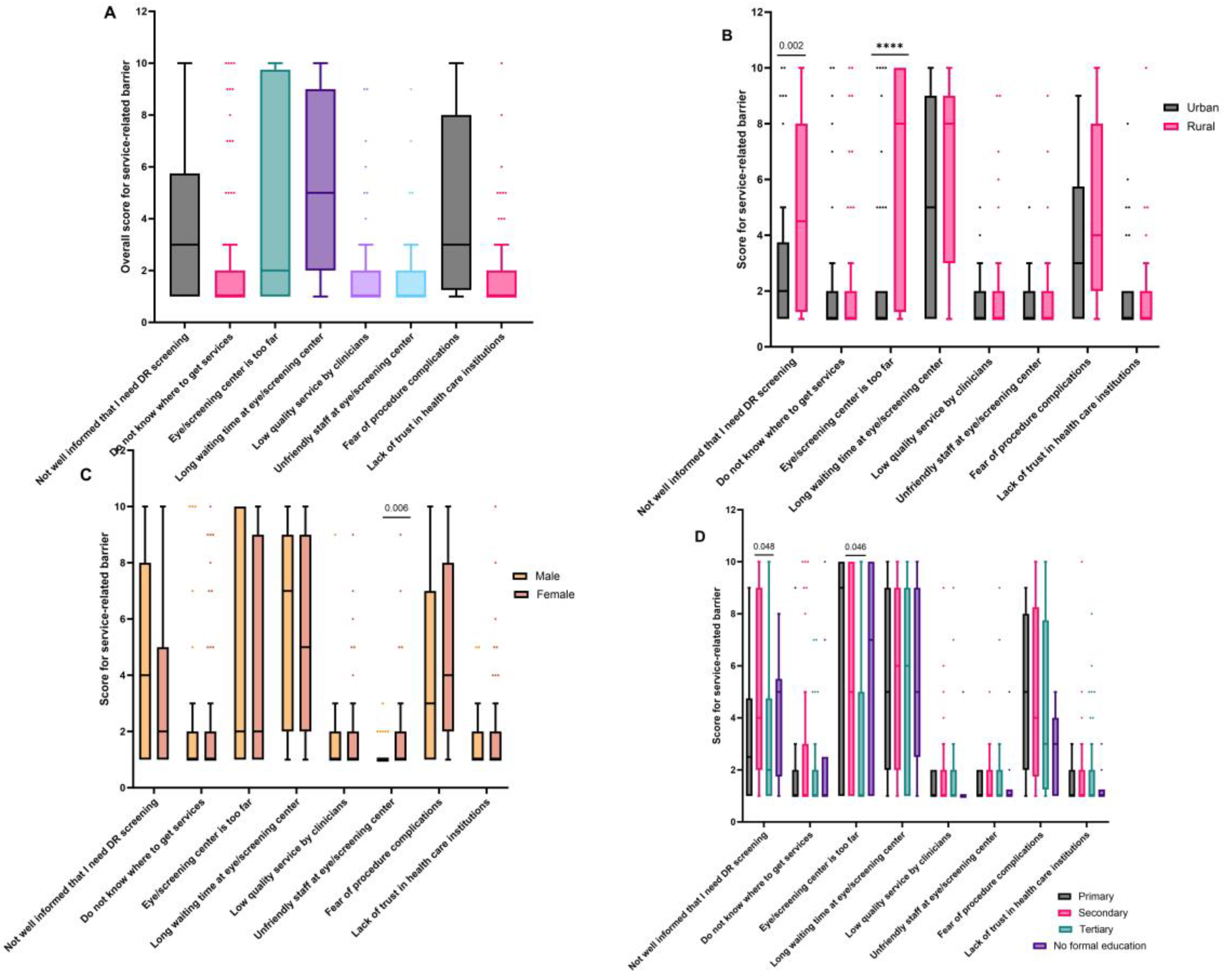
3.3. Service-Related Barriers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Simó-Servat, O.; Hernández, C.; Simó, R. Diabetic Retinopathy in the Context of Patients with Diabetes. Ophthalmic Res. 2019, 62, 211–217. [Google Scholar] [CrossRef]
- Jenkins, A.J.; Joglekar, M.V.; Hardikar, A.A.; Keech, A.C.; O’Neal, D.N.; Januszewski, A.S. Biomarkers in diabetic retinopathy. Rev. Diabet. Stud. 2015, 12, 159–195. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Lo, A.C.Y. Diabetic retinopathy: Pathophysiology and treatments. Int. J. Mol. Sci. 2018, 19, 1816. [Google Scholar] [CrossRef]
- Hammes, H.P. Diabetic retinopathy: Hyperglycaemia, oxidative stress and beyond. Diabetologia 2018, 61, 29–38. [Google Scholar] [CrossRef]
- Kang, Q.; Yang, C. Oxidative stress and diabetic retinopathy: Molecular mechanisms, pathogenetic role and therapeutic implications. Redox Biol. 2020, 37, 101799. [Google Scholar] [CrossRef] [PubMed]
- Heng, L.Z.; Comyn, O.; Peto, T.; Tadros, C.; Ng, E.; Sivaprasad, S.; Hykin, P.G. Diabetic retinopathy: Pathogenesis, clinical grading, management and future developments. Diabet. Med. 2013, 30, 640–650. [Google Scholar] [CrossRef]
- Rodríguez, M.L.; Pérez, S.; Mena-Mollá, S.; Desco, M.C.; Ortega, Á.L. Oxidative Stress and Microvascular Alterations in Diabetic Retinopathy: Future Therapies. Oxid. Med. Cell. Longev. 2019, 2019, 4940825. [Google Scholar] [CrossRef]
- Al Ghamdi, A.H. Clinical Predictors of Diabetic Retinopathy Progression; A Systematic Review. Curr. Diabetes Rev. 2019, 16, 242–247. [Google Scholar] [CrossRef]
- Chen, X.D.; Gardner, T.W. A critical review: Psychophysical assessments of diabetic retinopathy. Surv. Ophthalmol. 2021, 66, 213–230. [Google Scholar] [CrossRef]
- Jampol, L.M.; Glassman, A.R.; Sun, J. Evaluation and Care of Patients with Diabetic Retinopathy. N. Engl. J. Med. 2020, 382, 1629–1637. [Google Scholar] [CrossRef]
- Burnett, A.; Lee, L.; D’Esposito, F.; Wabulembo, G.; Cama, A.; Guldan, G.; Nelisse, M.; Koim, S.P.; Keys, D.; Poffley, A.J.; et al. Rapid assessment of avoidable blindness and diabetic retinopathy in people aged 50 years and older in the National Capital District of Papua New Guinea. Br. J. Ophthalmol. 2019, 103, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Pacific Eye Institute. Diabetes Retinal Screening, Grading and Management Guidelines for Use in Pacific Island Nations, 2010; Diabetes Work Group, Fred Hollows Found Pacific Eye Institute: Auckland, New Zealand, 2010; pp. 1–37. Available online: https://www.worlddiabetesfoundation.org/sites/default/files/WDF08-386%20Pacific%20Island%20Ret%20Screen%20Guidelines.pdf (accessed on 20 July 2023).
- Owusu-afriyie, B.; Baimur, I.; Gende, T.; Baia, T. Prevalence of Risk Factors of Retinal Diseases among Patients in Madang Province, Papua New Guinea. Int. J. Clin. Pract. 2022, 2022, 6120908. [Google Scholar] [CrossRef]
- Alwazae, M.; Al Adel, F.; Alhumud, A.; Almutairi, A.; Alhumidan, A.; Elmorshedy, H. Barriers for Adherence to Diabetic Retinopathy Screening among Saudi Adults. Cureus 2019, 11, e6454. [Google Scholar] [CrossRef] [PubMed]
- Kashim, R.M.; Newton, P.; Ojo, O. Diabetic Retinopathy Screening: A Systematic Review on Patients’ Non-Attendance. Int. J. Environ. Res. Public. Health 2018, 15, 157. [Google Scholar] [CrossRef] [PubMed]
- Watson, M.J.G.; McCluskey, P.J.; Grigg, J.R.; Kanagasingam, Y.; Daire, J.; Estai, M. Barriers and facilitators to diabetic retinopathy screening within Australian primary care. BMC Fam. Pract. 2021, 22, 239. [Google Scholar] [CrossRef] [PubMed]
- Bruggeman, B.; Zimmerman, C.; LaPorte, A.; Stalvey, M.; Filipp, S.L.; Gurka, M.J.; Silverstein, J.H.; Jacobsen, L.M. Barriers to retinopathy screening in youth and young adults with type 1 diabetes. Pediatr. Diabetes 2021, 22, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Fairless, E.; Nwanyanwu, K. Barriers to and Facilitators of Diabetic Retinopathy Screening Utilization in a High-Risk Population. J. Racial Ethn. Health Disparities 2019, 6, 1244–1249. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.L.; Stafford, L.K.; McLaughlin, S.A.; Boyko, E.J.; Vollset, S.E.; Smith, A.E.; Dalton, B.E.; Duprey, J.; Cruz, J.A.; Hagins, H.; et al. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2023, 402, 203–234. [Google Scholar] [CrossRef]
- World Health Organization. Eye Care Indicator Menu (ECIM): A Tool for Monitoring Strategies and Actions for Eye Care Provision. 2022. Available online: http://apps.who.int/ (accessed on 21 July 2023).
- Teo, Z.L.; Tham, Y.C.; Yu, M.; Chee, M.L.; Rim, T.H.; Cheung, N.; Bikbov, M.M.; Wang, Y.X.; Tang, Y.; Lu, Y.; et al. Global Prevalence of Diabetic Retinopathy and Projection of Burden through 2045: Systematic Review and Meta-analysis. Ophthalmology 2021, 128, 1580–1591. [Google Scholar] [CrossRef]
- Sabanayagam, C.; Banu, R.; Chee, M.L.; Lee, R.; Wang, Y.X.; Tan, G.; Jonas, J.B.; Lamoureux, E.L.; Cheng, C.-Y.; Klein, B.E.K.; et al. Incidence and progression of diabetic retinopathy: A systematic review. Lancet Diabetes Endocrinol. 2019, 7, 140–149. [Google Scholar] [CrossRef]
- Owusu-Afriyie, B.; Caleb, A.; Kube, L.; Gende, T. Knowledge and Awareness of Diabetes and Diabetic Retinopathy among Patients Seeking Eye Care Services in Madang Province, Papua New Guinea. J. Ophthalmol. 2022, 2022, 7674928. [Google Scholar] [CrossRef]
- Xiao, B.; Mercer, G.D.; Jin, L.; Lee, H.L.; Chen, T.; Wang, Y.; Liu, Y.; Denniston, A.K.; Egan, C.A.; Li, J.; et al. Outreach screening to address demographic and economic barriers to diabetic retinopathy care in rural China. PLoS ONE 2022, 17, e0266380. [Google Scholar] [CrossRef] [PubMed]
- Malerbi, F.K.; Andrade, R.E.; Morales, P.H.; Stuchi, J.A.; Lencione, D.; de Paulo, J.V.; Carvalho, M.P.; Nunes, F.S.; Rocha, R.M.; Ferraz, D.A.; et al. Diabetic Retinopathy Screening Using Artificial Intelligence and Handheld Smartphone-Based Retinal Camera. J. Diabetes Sci. Technol. 2022, 16, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Rajalakshmi, R.; Arulmalar, S.; Usha, M.; Prathiba, V.; Kareemuddin, K.S.; Anjana, R.M.; Mohan, V. Validation of smartphone based retinal photography for diabetic retinopathy screening. PLoS ONE 2015, 10, e0138285. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.H.; Kyaw, B.M.; Smith, H.; Tan, C.S.; Car, L.T. Use of Smartphones to Detect Diabetic Retinopathy: Scoping Review and Meta-Analysis of Diagnostic Test Accuracy Studies. J. Med. Internet Res. 2020, 22, e16658. [Google Scholar] [CrossRef] [PubMed]
- Bilong, Y.; Katte, J.C.; Koki, G.; Kagmeni, G.; Obama, O.P.N.; Fofe, H.R.N.; Mvilongo, C.; Nkengfack, O.; Bimbai, A.M.; Sobngwi, E.; et al. Validation of smartphone-based retinal photography for diabetic retinopathy screening. Ophthalmic Surg. Lasers Imaging Retin. 2019, 50, S18–S22. [Google Scholar] [CrossRef] [PubMed]
- Harrison, W.W.; Bearse, M.A.; Ng, J.S.; Jewell, N.P.; Barez, S.; Burger, D.; Schneck, M.E.; Adams, A.J. Multifocal electroretinograms predict onset of diabetic retinopathy in adult patients with diabetes. Investig. Ophthalmol. Vis. Sci. 2011, 52, 772–777. [Google Scholar] [CrossRef]
- Zagst, A.J.; Smith, J.D.; Wang, R.; Harrison, W.W. Foveal avascular zone size and mfERG metrics in diabetes and prediabetes: A pilot study of the relationship between structure and function. Doc. Ophthalmol. 2023, 147, 99–107. [Google Scholar] [CrossRef]
- Russell, J.F.; Al-khersan, H.; Shi, Y.; Scott, N.L.; Hinkle, J.W.; Fan, K.C.; Lyu, C.; Feuer, W.J.; Gregori, G.; Rosenfeld, P.J. Retinal Non-Perfusion in Proliferative Diabetic Retinopathy Before and After Panretinal Photocoagulation Assessed by Wide Field OCT Angiography. Am. J. Ophthalmol. 2020, 213, 177–185. [Google Scholar] [CrossRef]
- Kyei, S.; Asare, F.A.; Assan, J.K.; Zaabaar, E.; Assiamah, F.; Obeng, E.O.; Asiedu, K. Efficacy of intravitreal bevacizumab on diabetic macular oedema in an African population. Ir. J. Med. Sci. 2023. [Google Scholar] [CrossRef]
- Sun, Z.; Yang, D.; Tang, Z.; Ng, D.S.; Cheung, C.Y. Optical coherence tomography angiography in diabetic retinopathy: An updated review. Eye 2021, 35, 149–161. [Google Scholar] [CrossRef]
- Chua, J.; Sim, R.; Tan, B.; Wong, D.; Yao, X.; Liu, X.; Ting, D.S.W.; Schmidl, D.; Ang, M.; Garhöfer, G.; et al. Optical coherence tomography angiography in diabetes and diabetic retinopathy. J. Clin. Med. 2020, 9, 1723. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.J.; D’Alessio, D.A.; Fradkin, J.; Kernan, W.N.; Mathieu, C.; Mingrone, G.; Rossing, P.; Tsapas, A.; Wexler, D.J.; Buse, J.B. Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2018, 61, 2461–2498. [Google Scholar] [CrossRef]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; et al. Management of hyperglycaemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2022, 65, 1925–1966. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Glycemic targets: Standards of medical care in diabetes. Diabetes Care 2022, 42, S61–S70. [Google Scholar]
- Agrawal, L.; Azad, N.; Bahn, G.D.; Reaven, P.D.; Hayward, R.A.; Reda, D.J.; Emanuele, N.V.; Abraira, C.; Duckworth, W.C.; Hayden, C.T.; et al. Intensive glycemic control improves long-term renal outcomes in type 2 diabetes in the veterans affairs diabetes trial (VADT). Diabetes Care 2019, 42, E181–E182. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Hisland, L.; Grenet, G.; Gueyffier, F.; Cornu, C.; Jaafari, N.; Boussageon, R. Reappraisal of the efficacy of intensive glycaemic control on microvascular complications in patients with type 2 diabetes: A meta-analysis of randomised control-trials. Therapies 2022, 77, 413–423. [Google Scholar] [CrossRef]
- Xu, H.; Li, X.; Adams, H.; Kubena, K.; Guo, S. Etiology of metabolic syndrome and dietary intervention. Int. J. Mol. Sci. 2019, 20, 128. [Google Scholar] [CrossRef]
- Umpierrez, G.E.; PKovatchev, B. Glycemic Variability: How to Measure and Its Clinical Implication for Type 2 Diabetes. Am. J. Med. Sci. 2018, 356, 518–527. [Google Scholar] [CrossRef]
- Sherwani, S.I.; Khan, H.A.; Ekhzaimy, A.; Masood, A.; Sakharkar, M.K. Significance of HbA1c test in diagnosis and prognosis of diabetic patients. Biomark. Insights 2016, 11, 95–104. [Google Scholar] [CrossRef]
- Martinez, M.; Santamarina, J.; Pavesi, A.; Musso, C.; Umpierrez, G.E. Glycemic variability and cardiovascular disease in patients with type 2 diabetes. BMJ Open Diabetes Res. Care 2021, 9, e002032. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Respondents; n (%) |
|---|---|
| Gender | |
| Male | 39 (37.5) |
| Female | 65 (62.5) |
| Residential Location | |
| Urban | 48 (46.2) |
| Rural | 56 (53.8) |
| Age Group (years) | |
| 21–30 | 4 (3.8) |
| 31–40 | 14 (13.5) |
| 41–50 | 30 (28.8) |
| 51–60 | 33 (31.7) |
| 61–70 | 20 (19.2) |
| Above 70 years | 3 (2.9) |
| Level of Education | |
| Primary | 16 (15.4) |
| Secondary | 34 (32.7) |
| Tertiary | 44 (42.3) |
| No formal education | 10 (9.6) |
| Residential Province | |
| Madang | 89 (85.6) |
| Simbu | 4 (3.8) |
| East New Britain | 2 (1.9) |
| Milne Bay | 2 (1.9) |
| Jiwaka | 2 (1.9) |
| Others a | 4 (3.8) |
| Not reported | 1 (1.0) |
| Primary Occupation | |
| Farmer | 23 (22.1) |
| Retail trader/self employed | 14 (13.5) |
| Teacher/lecturer | 12 (11.5) |
| Housewife | 11 (10.6) |
| Manager/director | 9 (8.7) |
| Health worker | 7 (6.7) |
| Secretary | 7 (6.7) |
| Others b | 21 (20.2) |
| Expected Year of DR Screening | |
| 2017 | 10 (9.6) |
| 2018 | 15 (14.4) |
| 2019 | 22 (21.2) |
| 2020 | 44 (42.3) |
| 2021 | 13 (12.5) |
| Category of Nonadherence | |
| First DR screening appointment | 37 (35.6) |
| Follow-up visits/reviews | 58 (55.8) |
| Taking Any Diabetes Treatment/Medication | |
| Yes | 38 (36.5) |
| No | 66 (63.5) |
| Diabetes Medication | |
| Metformin | 27 (26.0) |
| Daonil | 6 (5.8) |
| Herbs and traditional remedy | 3 (2.9) |
| Insulin | 1 (1.0) |
| Nifedipine | 1 (1.0) |
| Reasons For Not Taking Diabetes Treatment | |
| No reason | 32 (30.8) |
| Diet | 21 (20.2) |
| Managing other comorbidity first | 6 (5.8) |
| Poor access to a health facility | 3 (2.9) |
| Financial constraint | 2 (1.9) |
| Side effect of medication | 1 (1.0) |
| Poor understanding of the treatment plan | 1 (1.0) |
| Personal Barriers | Respondents; n (%) |
|---|---|
| Insufficient income or cost | 54 (51.9) |
| Good vision in the fellow eye | 58 (55.8) |
| Eye problem is not serious enough | 73 (70.2) |
| Time constraints or other priorities | 90 (86.5) |
| No escort or guardian to help | 56 (53.8) |
| Culture/traditional beliefs | 34 (32.7) |
| Forgot or no reminder | 62 (59.6) |
| No symptoms | 57 (54.8) |
| Poor knowledge about DR | 80 (76.9) |
| Prefer to use alternative service | 42 (40.3) |
| Service-related Barriers | Respondents; n (%) |
| Not well informed that I need DR screening | 68 (65.4) |
| Do not know where to get services | 36 (34.6) |
| Eye/screening center is too far | 58 (55.8) |
| Long waiting time at eye/screening center | 81 (77.9) |
| Low quality service by clinicians | 32 (30.8) |
| Unfriendly staff at eye/screening center | 33 (31.7) |
| Fear of procedure complications | 78 (75.0) |
| Lack of trust in healthcare institutions | 38 (36.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Owusu-Afriyie, B.; Gende, T.; Tapilas, M.; Zimbare, N.; Kewande, J. Patients’ Perspective on Barriers to Utilization of a Diabetic Retinopathy Screening Service. Diabetology 2023, 4, 393-405. https://doi.org/10.3390/diabetology4030033
Owusu-Afriyie B, Gende T, Tapilas M, Zimbare N, Kewande J. Patients’ Perspective on Barriers to Utilization of a Diabetic Retinopathy Screening Service. Diabetology. 2023; 4(3):393-405. https://doi.org/10.3390/diabetology4030033
Chicago/Turabian StyleOwusu-Afriyie, Bismark, Theresa Gende, Martin Tapilas, Nicholas Zimbare, and Jeffrey Kewande. 2023. "Patients’ Perspective on Barriers to Utilization of a Diabetic Retinopathy Screening Service" Diabetology 4, no. 3: 393-405. https://doi.org/10.3390/diabetology4030033
APA StyleOwusu-Afriyie, B., Gende, T., Tapilas, M., Zimbare, N., & Kewande, J. (2023). Patients’ Perspective on Barriers to Utilization of a Diabetic Retinopathy Screening Service. Diabetology, 4(3), 393-405. https://doi.org/10.3390/diabetology4030033