
Adenosquamous Carcinomas and Mucinous Adenocarcinoma of the Minor Salivary Glands: Immunohistochemical and Molecular Insights

Abstract
:1. Introduction
2. Materials and Methods
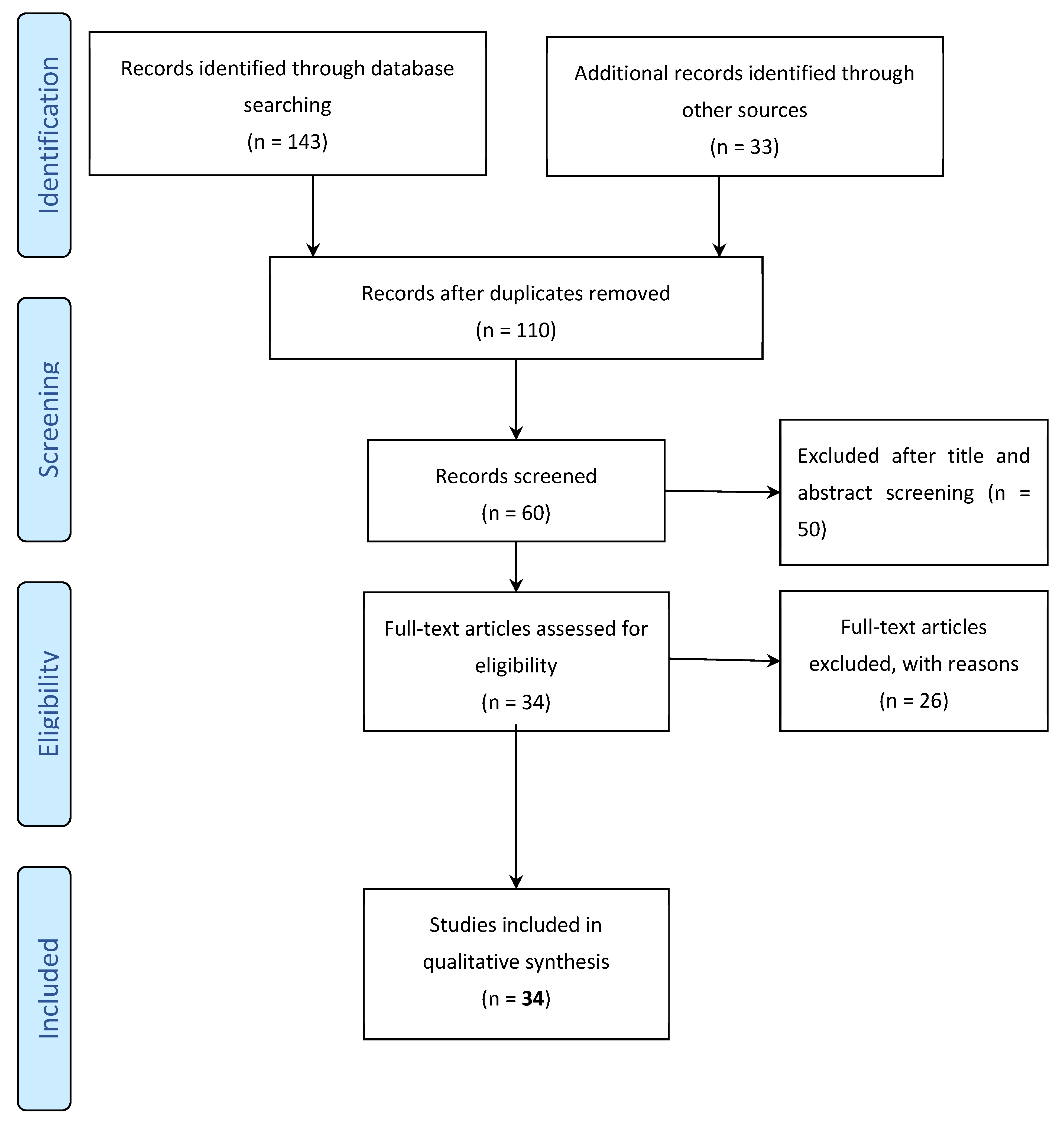
2.1. Reviewing the Literature
- All research papers must be original research articles that explore cases empirically.
- All articles must be published in English.
- All articles must investigate the diagnosed case molecularly.
- All articles must justify the diagnosis of the lesion.
- All published cases must include adequate clinical and histologic descriptions.
- All published cases must report information about the patient survival.
- Reporting molecular or immunohistochemical investigations, or both. is recommended.
- Articles that include an abstract only.
- Studies that reviewed previous works without reporting new cases.
- Studies that investigated major salivary gland lesions or extra-salivary neoplasms.
2.2. Collating Molecular Findings in Non-Salivary ASCs and MACs
3. Results
3.1. Immunohistochemical and Molecular Findings in Salivary ASCs and MACs
3.2. Morphologic Difference in Different Sites
3.3. Molecular Profiling of ASCs and MACs and Relevant Pathways

4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- White, V.; Hyrcza, M.; Lennerz, J.K.; Thierauf, J.; Lokuhetty, D.; Cree, I.A.; Indave, B. Mucoepidermoid carcinoma (MEC) and adenosquamous carcinoma (ASC), the same or different entities? Mod. Pathol. 2022, 35, 1484–1493. [Google Scholar] [CrossRef] [PubMed]
- Toyooka, S.; Yatabe, Y.; Tokumo, M.; Ichimura, K.; Asano, H.; Tomii, K.; Aoe, M.; Yanai, H.; Date, H.; Mitsudomi, T.; et al. Mutations of epidermal growth factor receptor and K-ras genes in adenosquamous carcinoma of the lung. Int. J. Cancer 2006, 118, 1588–1590. [Google Scholar] [CrossRef] [PubMed]
- Tochigi, N.; Dacic, S.; Nikiforova, M.; Cieply, K.M.; Yousem, S.A. Adenosquamous carcinoma of the lung a microdissection study of KRAS and EGFR mutational and amplification status in a Western patient population. Am. J. Clin. Pathol. 2011, 135, 783–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, S.M.; Kang, H.J.; Shin, J.H.; Kim, H.; Shin, D.H.; Kim, S.K.; Kim, J.H.; Chung, K.Y.; Kim, S.K.; Chang, J. Identical epidermal growth factor receptor mutations in adenocarcinomatous and squamous cell carcinomatous components of adenosquamous carcinoma of the lung. Cancer 2007, 109, 581–587. [Google Scholar] [CrossRef]
- Kass, J.I.; Lee, S.C.; Abberbock, S.; Seethala, R.R.; Duvvuri, U. Adenosquamous carcinoma of the head and neck: Molecular analysis using CRTC-MAML FISH and survival comparison with paired conventional squamous cell carcinoma. Laryngoscope 2015, 125, E371–E376. [Google Scholar] [CrossRef]
- Clauditz, T.S.; Gontarewicz, A.; Bokemeyer, C.; Sauter, G.; Knecht, R.; Münscher, A.; Wilczak, W. Abundant expression of mTOR kinase in salivary gland tumors–potentials as therapy target? J. Oral Pathol. Med. 2013, 42, 769–773. [Google Scholar] [CrossRef]
- Parente, P.; Covelli, C.; Parrella, P.; Latiano, T.P.; Fiordelisi, F.; Pellico, M.T.; Maiello, E.; Graziano, P. Intestinal adenosquamous carcinoma with a synchronous skin metastasis: A immunohistochemical and molecular analysis. Int. J. Color. Dis. 2020, 35, 337–341. [Google Scholar] [CrossRef]
- Martinho, O.; Gonçalves, A.; Moreira, M.A.R.; Ribeiro, L.F.J.; Queiroz, G.S.; Schmitt, F.C.; Reis, R.M.; Longatto-Filho, A. KIT activation in uterine cervix adenosquamous carcinomas by KIT/SCF autocrine/paracrine stimulation loops. Gynecol. Oncol. 2008, 111, 350–355. [Google Scholar] [CrossRef]
- Solakoglu Kahraman, D.; Diniz, G.; Sayhan, S.; Ayaz, D.; Uncel, M.; Karadeniz, T.; Akman, T.; Ozdemir, A. Differences in the ARID-1 alpha expressions in squamous and adenosquamous carcinomas of uterine cervix. APMIS 2015, 123, 847–850. [Google Scholar] [CrossRef]
- Bataillon, G.; Fuhrmann, L.; Girard, E.; Menet, E.; Laé, M.; Capovilla, M.; Treilleux, I.; Arnould, L.; Penault-Llorca, F.; Rouzier, R.; et al. High rate of PIK3CA mutations but no TP53 mutations in low-grade adenosquamous carcinoma of the breast. Histopathology 2018, 73, 273–283. [Google Scholar] [CrossRef]
- Stolnicu, S.; Hoang, L.; Hanko-Bauer, O.; Barsan, I.; Terinte, C.; Pesci, A.; Aviel-Ronen, S.; Kiyokawa, T.; Alvarado-Cabrero, I.; Oliva, E.; et al. Cervical adenosquamous carcinoma: Detailed analysis of morphology, immunohistochemical profile, and clinical outcomes in 59 cases. Mod. Pathol. 2019, 32, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Alos, L.; Castillo, M.; Nadal, A.; Caballero, M.; Mallofre, C.; Palacin, A.; Cardesa, A. Adenosquamous carcinoma of the head and neck: Criteria for diagnosis in a study of 12 cases. Histopathology 2004, 44, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Huo, Z.; Wu, H.; Li, J.; Li, S.; Wu, S.; Liu, Y.; Luo, Y.; Cao, J.; Zeng, X.; Liang, Z. Primary pulmonary mucoepidermoid carcinoma: Histopathological and moleculargenetic studies of 26 cases. PLoS ONE 2015, 10, e0143169. [Google Scholar] [CrossRef] [PubMed]
- Uramoto, H.; Yamada, S.; Hanagiri, T. Immunohistochemical staining with DeltaNp63 is useful for distinguishing the squamous cell component of adenosquamous cell carcinoma of the lung. Anticancer Res. 2010, 30, 4717–4720. [Google Scholar] [PubMed]
- Prabhakar, M.C.; Sabarinath, B.K.; Sivapathasundharam, B.; Vasanthakumar, V. Adenosquamous carcinoma of the tongue: A case report and an overview of histogenetic concepts. J. Oral Maxillofac. Pathol. 2020, 24, S110–S114. [Google Scholar] [CrossRef]
- WHO. WHO Classification of Tumours Editorial Board. Head and Neck Tumours, 5th ed.; WHO classification of tumours series; International Agency for Research on Cancer: Lyon, France, 2022; Volume 9.
- Simpson, R.H.W. Salivary Duct Carcinoma: New Developments-Morphological Variants Including Pure In Situ High Grade Lesions; Proposed Molecular Classification. Head Neck Pathol. 2013, 7, 48–58. [Google Scholar] [CrossRef] [Green Version]
- Wong, F.K.; Zumsteg, Z.S.; Langevin, C.-J.; Ali, N.; Maclary, S.; Balzer, B.L.; Ho, A.S. Mucinous Carcinoma with Neuroendocrine Differentiation of Salivary Gland Origin. Head Neck Pathol. 2017, 11, 249–255. [Google Scholar] [CrossRef] [Green Version]
- Simpson, R.H.W.; Prasad, A.R.; Lewis, J.E.; Skálová, A.; David, L. Mucin-rich variant of salivary duct carcinoma: A clinicopathologic and immunohistochemical study of four cases. Am. J. Surg. Pathol. 2003, 27, 1070–1079. [Google Scholar] [CrossRef]
- Lastra, R.R.; Park, K.J.; Kenneth Schoolmeester, J. Invasive stratified mucin-producing carcinoma and stratified mucin-producing intraepithelial lesion (SMILE) 15 cases presenting a spectrum of cervical neoplasia with description of a distinctive variant of invasive adenocarcinoma. Am. J. Surg. Pathol. 2016, 40, 262–269. [Google Scholar] [CrossRef]
- Agaimy, A.; Baněčková, M.; Ihrler, S.; Mueller, S.K.; Franchi, A.; Hartmann, A.; Stoehr, R.; Skálová, A. ALK Rearrangements Characterize 2 Distinct Types of Salivary Gland Carcinomas: Clinicopathologic and Molecular Analysis of 4 Cases and Literature Review. Am. J. Surg. Pathol. 2021, 45, 1166–1178. [Google Scholar] [CrossRef]
- Wang, K.; McDermott, J.D.; Schrock, A.B.; Elvin, J.A.; Gay, L.; Karam, S.D.; Raben, D.; Somerset, H.; Ali, S.M.; Ross, J.S.; et al. Comprehensive genomic profiling of salivary mucoepidermoid carcinomas reveals frequent BAP1, PIK3CA, and other actionable genomic alterations. Ann. Oncol. 2017, 28, 748–753. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, M.; Tanaka, A.; Hamao, A.; Kitada, M.; Fukuda, F.; Suzuki, S.; Kebusa, Y.; Yamamoto, Y.; Sakashita, H.; Kusama, K. Expression of cytokeratins in oral adenosquamous carcinoma: Specific detection of individual cytokeratins by monoclonal antibodies. Asian J. Oral Maxillofac. Surg. 2002, 14, 232–239. [Google Scholar] [CrossRef]
- Keelawat, S.; Liu, C.Z.; Roehm, P.C.; Barnes, L. Adenosquamous carcinoma of the upper aerodigestive tract: A clinicopathologic study of 12 cases and review of the literature. Am. J. Otolaryngol.-Head Neck Med. Surg. 2002, 23, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Sheahan, P.; Fitzgibbon, J.; Lee, G.; O’Leary, G. Adenosquamous carcinoma of the tongue in a 22-year-old female: Report of a case with immunohistochemistry. Eur. Arch. Oto-Rhino-Laryngol. 2003, 260, 509–512. [Google Scholar] [CrossRef] [PubMed]
- Morita, N.; Yabuta, T.; Todo, K.; Kimoto, N. Adenosquamous carcinoma of the tongue. Asian J. Oral Maxillofac. Surg. 2005, 17, 277–279. [Google Scholar] [CrossRef]
- Shinhar, S.Y.; Heckathorn, C.L. Adenosquamous carcinoma of the nasal cavity. Ear Nose Throat J. 2008, 87, 612–614. [Google Scholar] [CrossRef] [Green Version]
- Masand, R.P.; El-Mofty, S.K.; Ma, X.J.; Luo, Y.; Flanagan, J.J.; Lewis, J.S. Adenosquamous Carcinoma of the Head and Neck: Relationship to Human Papillomavirus and Review of the Literature. Head Neck Pathol. 2011, 5, 108–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fonseca, F.P.; Ramos, L.M.A.; Vargas, P.A.; de Almeida, O.P.; Lopes, M.A.; Santos-Silva, A.R. Oral adenosquamous carcinoma: Evidence that it arises from the surface mucosal epithelium. Histopathology 2012, 61, 321–323. [Google Scholar] [CrossRef]
- Pandilla, R.; Kotapalli, V.; Gowrishankar, S.; Chigurupati, M.; Patnaik, S.; Uppin, S.; Rao, S.; Kalidindi, N.; Regulagadda, S.; Sundaram, C.; et al. Distinct genetic aberrations in oesophageal adeno and squamous carcinoma. Eur. J. Clin. Investig. 2013, 43, 1233–1239. [Google Scholar] [CrossRef]
- Ishida, M.; Iwai, M.; Kagotani, A.; Iwamoto, N.; Okabe, H. Adenosquamous carcinoma of the tongue: A case report with review of the literature. Int. J. Clin. Exp. Pathol. 2014, 7, 1809–1813. [Google Scholar]
- Bhattacharyya, I.; Chehal, H.K.; McNally, S.J.; Cohen, D.M.; Islam, N.M. Adenosquamous carcinoma of the oral cavity: An unusual epithelial malignancy. A report of two cases and review of literature. J. Oral Maxillofac. Surg. Med. Pathol. 2015, 27, 126–130. [Google Scholar] [CrossRef]
- Magalhaes, M.A.O.; Irish, J.C.; Weinreb, I.; Perez-Ordonez, B. Adenosquamous Carcinoma of Hypopharynx with Intestinal-Phenotype. Head Neck Pathol. 2015, 9, 114–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sravya, T.; Rao, G.; Kumar, M.; Sudheerkanth, K. Oral adenosquamous carcinoma: Report of a rare entity with a special insight on its histochemistry. J. Oral Maxillofac. Pathol. 2016, 20, 548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miura, K.I.; Shiraishi, T.; Ohba, S.; Asahina, I. Importance of diagnosis and initial treatment strategy for adenosquamous carcinoma of the tongue: A case report and literature review. Oral Maxillofac. Surg. Cases 2017, 3, 102–106. [Google Scholar] [CrossRef]
- Satomi, T.; Kohno, M.; Hasagawa, O.; Enomoto, A.; Abukawa, H.; Chikazu, D.; Yoshida, M.; Matsubayashi, J.; Nagao, T. Adenosquamous carcinoma of the tongue: Clinicopathologic study and review of the literature. Odontology 2017, 105, 127–135. [Google Scholar] [CrossRef]
- Kikuta, S.; Todoroki, K.; Seki, N.; Kusukawa, J. Adenosquamous Carcinoma in the Midline Dorsum of the Tongue: A Rare Case Report. J. Oral Maxillofac. Surg. 2018, 76, 2131–2135. [Google Scholar] [CrossRef]
- Rawal, Y.; Anderson, K. Adenosquamous Carcinoma of the Tongue. Head Neck Pathol. 2018, 12, 576–579. [Google Scholar] [CrossRef]
- Eguchi, T.; Basugi, A.; Kanai, I.; Miyata, Y.; Suzuki, T.; Hamada, Y. Adenosquamous carcinoma development as a recurrence of squamous cell carcinoma in the oral floor: A case report. Medicine 2019, 98, e17688. [Google Scholar] [CrossRef]
- Gao, Y.; Di, P.; Peng, X.; Yu, G.; Sun, K. Mucinous adenocarcinoma of salivary glands. Zhonghua Kou Qiang Yi Xue Za Zhi = Zhonghua Kouqiang Yixue Zazhi = Chin. J. Stomatol. 2002, 37, 356–358. [Google Scholar]
- Notani, K.-I.; Iizuka, T.; Yamazaki, Y.; Henmi, T.; Sugiura, C.; Kohgo, T.; Fukuda, H. Mucinous adenocarcinoma of probable minor salivary gland origin. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2002, 94, 738–740. [Google Scholar] [CrossRef]
- Abecasis, J.; Viana, G.; Pissarra, C.; Pereira, T.; Fonseca, I.; Soares, J. Adenocarcinomas of the nasal cavity and paranasal sinuses: A clinicopathological and immunohistochemical study of 14 cases. Histopathology 2004, 45, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Shumway, A.; Kalmar, J.; Steiner, R.; Allen, C. Mucinous Adenocarcinoma of the Palate: Report of a Case and Review of the Literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 103, e23–e24. [Google Scholar] [CrossRef]
- Ide, F.; Mishima, K.; Tanaka, A.; Saito, I.; Kusama, K. Mucinous adenocarcinoma of minor salivary glands: A high-grade malignancy prone to lymph node metastasis. Virchows Arch. A Pathol. Anat. Histopathol. 2009, 454, 55–60. [Google Scholar] [CrossRef]
- Seoane, J.; Varela-Centelles, P.; López-Niño, J.; Vazquez, I.; Abdulkader, I.; García-Caballero, T. Gingival mucinous adenocarcinoma of a minor salivary gland. J. Periodontol. 2010, 81, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Uchida, K.; Oga, A.; Mano, T.; Nagatsuka, H.; Ueyama, Y.; Sasaki, K. Screening for DNA copy number aberrations in mucinous adenocarcinoma arising from the minor salivary gland: Two case reports. Cancer Genet. Cytogenet. 2010, 203, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Slova, D.; Mondolfi, A.P.; Moisini, I.; Levi, G.; Urken, M.; Zevallos, J.; Mansoor, S.; Khorsandi, A.; Bloch, D.; Vidhun, R.; et al. Colonic-Type Adenocarcinoma of the Base of the Tongue: A Case Report of a Rare Neoplasm. Head Neck Pathol. 2012, 6, 250–254. [Google Scholar] [CrossRef] [Green Version]
- Bhat, S.P.; Prasad, K.H.L.; Bhat, V.S.; Aroor, R. Primary Mucinous Carcinoma of Buccal Mucosa: A Rare Case Report. Indian J. Surg. Oncol. 2014, 5, 249–251. [Google Scholar] [CrossRef] [Green Version]
- Mezmezian, M.; Spreafico, H.; Glembocki, A.; Carassai, M. Primary mucinous adenocarcinoma of minor salivary glands of the palate: Case report and literature review. J. Oral Maxillofac. Surg. Med. Pathol. 2015, 27, 446–449. [Google Scholar] [CrossRef]
- De Benedittis, M.; Palmiotto, A.; Turco, M.; Petruzzi, M.; Cortelazzi, R. Salivary mucinous adenocarcinoma of the mandible. Odontology 2017, 105, 257–261. [Google Scholar] [CrossRef]
- Petersson, F.; Michal, M.; Ptáková, N.; Skalova, A.; Michal, M. Salivary gland mucinous adenocarcinoma with minor (Mammary Analogue) secretory and low-grade in situ carcinoma components sharing the same ETV6-RET translocation and with no other molecular genetic aberrations detected on NGS analysis. Appl. Immunohistochem. Mol. Morphol. 2020, 28, E54–E57. [Google Scholar] [CrossRef]
- Aoki, T.; Kondo, Y.; Karakida, K.; Naito, H.; Kajiwara, H.; Ota, Y. A mucinous adenocarcinoma of the lip with elevated serum carcinoembryonic antigen levels: A case report. Oral Maxillofac. Surg. 2020, 24, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Rooper, L.M.; Argyris, P.P.; Thompson, L.D.R.; Gagan, J.; Westra, W.H.; Jordan, R.C.; Koutlas, I.G.; Bishop, J.A. Salivary Mucinous Adenocarcinoma Is a Histologically Diverse Single Entity with Recurrent AKT1 E17K Mutations: Clinicopathologic and Molecular Characterization with Proposal for a Unified Classification. Am. J. Surg. Pathol. 2021, 45, 1337–1347. [Google Scholar] [CrossRef] [PubMed]
- Vassella, E.; Langsch, S.; Dettmer, M.S.; Schlup, C.; Neuenschwander, M.; Frattini, M.; Gugger, M.; Schäfer, S.C. Molecular profiling of lung adenosquamous carcinoma: Hybrid or genuine type? Oncotarget 2015, 6, 23905–23916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shu, C.; Cheng, H.; Wang, A.; Mansukhani, M.M.; Powell, C.A.; Halmos, B.; Borczuk, A.C. Thymidylate synthase expression and molecular alterations in adenosquamous carcinoma of the lung. Mod. Pathol. 2013, 26, 239–246. [Google Scholar] [CrossRef] [Green Version]
- Brody, J.R.; Costantino, C.L.; Potoczek, M.; Cozzitorto, J.; McCue, P.; Yeo, C.J.; Hruban, R.H.; Witkiewicz, A.K. Adenosquamous carcinoma of the pancreas harbors KRAS2, DPC4 and TP53 molecular alterations similar to pancreatic ductal adenocarcinoma. Mod. Pathol. 2009, 22, 651–659. [Google Scholar] [CrossRef] [Green Version]
- Fonseca-Silva, T.; de Oliveira Santos, C.C.; Bonan, P.R.F.; Martelli-Junior, H.; de Almeida, O.P.; Roy, A.; De-Paula, A.M.B.; Guimarães, A.L.S. Primary Oral Mucinous Adenocarcinoma in minor salivary gland. Indian J. Dent. 2013, 4, 237–240. [Google Scholar] [CrossRef]
- Cipriani, N.A.; Lusardi, J.J.; Mcelherne, J.; Pearson, A.T.; Olivas, A.D.; Fitzpatrick, C.; Lingen, M.W.; Blair, E.A. Mucoepidermoid Carcinoma: A Comparison of Histologic Grading Systems and Relationship to MAML2 Rearrangement and Prognosis. Am. J. Surg. Pathol. 2019, 43, 885–897. [Google Scholar] [CrossRef]
- Han, H.; Luo, X.D.; Shao, L.Q. A population-based analysis of adenosquamous carcinoma of the salivary gland. Gland Surg. 2021, 10, 645–655. [Google Scholar] [CrossRef]
- Kenmotsu, H.; Serizawa, M.; Koh, Y.; Isaka, M.; Takahashi, T.; Taira, T.; Ono, A.; Maniwa, T.; Takahashi, S.; Mori, K.; et al. Prospective genetic profiling of squamous cell lung cancer and adenosquamous carcinoma in Japanese patients by multitarget assays. BMC Cancer 2014, 14, 786. [Google Scholar] [CrossRef] [Green Version]
- Hirose, S.; Murakami, N.; Takahashi, K.; Kuno, I.; Takayanagi, D.; Asami, Y.; Matsuda, M.; Shimada, Y.; Yamano, S.; Sunami, K.; et al. Genomic alterations in STK11 can predict clinical outcomes in cervical cancer patients. Gynecol. Oncol. 2020, 156, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Cros, J.; Sbidian, E.; Hans, S.; Roussel, H.; Scotte, F.; Tartour, E.; Brasnu, D.; Laurent-Puig, P.; Bruneval, P.; Blons, H.; et al. Expression and mutational status of treatment-relevant targets and key oncogenes in 123 malignant salivary gland tumours. Ann. Oncol. 2013, 24, 2624–2629. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Song, B.; Guo, S.; Li, G.; Jin, G. Identification of germline and somatic mutations in pancreatic adenosquamous carcinoma using whole exome sequencing. Cancer Biomark. 2020, 27, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Bishop, J.A.; Koduru, P.; Veremis, B.M.; Oliai, B.R.; Weinreb, I.; Rooper, L.M.; Dickson, B.C.; Demicco, E.G. SS18 Break-Apart Fluorescence In Situ Hybridization is a Practical and Effective Method for Diagnosing Microsecretory Adenocarcinoma of Salivary Glands. Head Neck Pathol. 2021, 15, 723–726. [Google Scholar] [CrossRef]
- Luo, W.; Lindley, S.W.; Lindley, P.H.; Krempl, G.A.; Seethala, R.R.; Fung, K.M. Mammary analog secretory carcinoma of salivary gland with high-grade histology arising in hard palate, report of a case and review of literature. Int. J. Clin. Exp. Pathol. 2014, 7, 9008–9022. [Google Scholar]
- Skalova, A.; Vanecek, T.; Martinek, P.; Weinreb, I.; Stevens, T.M.; Simpson, R.H.W.; Hyrcza, M.; Rupp, N.J.; Baneckova, M.; Michal, M.; et al. Molecular profiling of mammary analog secretory carcinoma revealed a subset of tumors harboring a novel ETV6-RET translocation: Report of 10 cases. Am. J. Surg. Pathol. 2018, 42, 234–246. [Google Scholar] [CrossRef] [Green Version]
- Panaccione, A.; Zhang, Y.; Mi, Y.; Yarbrough, W.G.; Ivanov, S.V.; Mitani, Y.; El-Naggar, A.K.; Yan, G.; Prasad, M.L.; McDonald, W.H.; et al. Chromosomal abnormalities and molecular landscape of metastasizing mucinous salivary adenocarcinoma. Oral Oncol. 2017, 66, 38–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kikuchi, K.; Fukunaga, S.; Ide, F.; Hoshino, M.; Inoue, H.; Miyazaki, Y.; Li, T.J.; Kusama, K. Primary intestinal-type adenocarcinoma of the buccal mucosa: A case report and literature review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2019, 127, e61–e70. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Refs. | Dx | Cases | Morphology | Mucin | Positive IHC | Molecular | Exclusion |
|---|---|---|---|---|---|---|---|---|
| Fukudaet al., 2002 | [23] | ASC | 4 | AC + SCC | Y | CK14 | No | Not Adenoid SCC |
| Keelawatet al., 2002 | [24] | ASC | 5 | AC + SCC | Y | No | No | Not Adenoid SCC, not MEC |
| Sheahanet al., 2003 | [25] | ASC | 1 | AC + SCC | Y | CK7 CAM5.2 | No | Not given |
| Alos et al., 2004 | [12] | ASC | 5 | AC + SCC | Y | CEA, CK7 CAM5.2 | Aneuploid ASCs | Not MEC |
| Moritaet al., 2005 | [26] | ASC | 1 | AC + SCC | Y | No | No | Not given |
| Shinharet al., 2008 | [27] | ASC | 1 | AC + SCC | Y | No | No | Not given |
| Masand et al., 2011 | [28] | ASC | 4 | AC + SCC | Y | No | For HPV | Adenoid SCC included |
| Fonsecaet al., 2012 | [29] | ASC | 1 | AC + SCC | Y | CEA, CK7/8/18 | No | Not given |
| Pandilla et al., 2013 | [30] | ASC | 1 | AC + SCC | Y | β-catenin | APC c.4315delC mutation | Not given |
| Ishidaet al., 2014 | [31] | ASC | 1 | AC + SCC | Y | CEA, HCK, CK7, CA19-9 | No | Not given |
| Bhattacharyya et al., 2015 | [32] | ASC | 2 | AC + SCC | Y | No | No | Not MEC, not SCC with mucoserous invasion, not adenoid SCC |
| Kass et al., 2015 | [5] | ASC | 42 | AC + SCC | Y | No | -ve for MAML2 | Not MEC |
| Magalhaeset al., 2015 | [33] | ASC | 1 | AC + SCC | Y | CEA, CK7/20, EMA, CDX2 CAM5.2 | No | Not AC, NOS |
| Sravyaet al., 2016 | [34] | ASC | 1 | AC + SCC | Y | 34βE12 | No | Not MEC, not basaloid SCC, not adenoid SCC |
| Miuraet al., 2017 | [35] | ASC | 1 | AC + SCC | Y | 34βE12, CK7, CAM5.2 | No | Not given |
| Satomiet al., 2017 | [36] | ASC | 1 | AC + SCC | Y | CEA, CK7 | No | Not given |
| Kikutaet al., 2018 | [37] | ASC | 1 | AC + SCC | Y | CK7/CK20 | No | ? Cribriform AC * |
| Rawal et al., 2018 | [38] | ASC | 1 | AC + SCC | Y | CEA, CK7, CAM5.2 | No | Not given |
| Eguchi et al., 2019 | [39] | ASC | 1 | AC + SCC | Y | CEA, CK7, p53 | No | Not given |
| Prabhakar et al., 2020 | [15] | ASC | 1 | AC + recurrent SCC | Y | Pancytokeratin | No | Not adenoid SCC |
| Gao et al., 2002 | [40] | MAC | 1 | MAC + features | Y | CK7 | No | Not given |
| Notani et al., 2002 | [41] | MAC | 1 | Classic MAC | Y | CK7 | No | Not given |
| Abecasis et al., 2004 | [42] | MAC | 2 | Classic MAC | Y | CK7, CK20, synaptophysin; | No | Not given |
| Shumway et al., 2007 | [43] | MAC | 1 | Classic MAC | Y | CK7 | No | Not given |
| Ide et al., 2009 | [44] | MAC | 1 | Classic MAC | Y | CEA, HCK, CK7/20, EMA | No | Not given |
| Seoane et al., 2010 | [45] | MAC | 1 | Classic MAC | Y | CK AE1/AE3/CK8, CK18, S100 | No | Not given |
| Uchida et al., 2010 | [46] | MAC | 4 | Classic MAC | Y | No | MDM2 AURKA | Not given |
| Slova et al., 2012 | [47] | MAC | 1 | Colonic type adenocarcinoma + mucin | Y | AE1/AE3, CAM5.2, CK7, CK20, EMA | No | Not given |
| Bhat et al., 2014 | [48] | MAC | 1 | MAC | Y | No | No | Not given |
| Mezmezian et al., 2015 | [49] | MAC | 1 | MAC + eosinophil | Y | CK7, CK19, EMA, CEA | No | Mucinous metastatic carcinoma |
| De Benedittis et al., 2017 | [50] | MAC | 1 | MAC + features | Y | CK7/8 | No | Not given |
| Petersson et al., 2020 | [51] | MAC | 1 | In a hybrid tumor | Y | Mammaglobin | ETV6 RET | MASC dominant |
| Aoki et al., 2020 | [52] | MAC | 1 | Classic MAC | Y | CK7, CEA | No | Not given |
| Rooper et al., 2021 | [53] | MAC | 4 | MAC + features | Y | CK7 | AKT1 E17K | Not intraductal papillary mucinous ca. |
| ASC | MAC | HG-MEC | Corresponding Pathway | |
|---|---|---|---|---|
| ABCB1 | + | Energy Metabolism | ||
| ACE2 | + | A-beta Uptake and Degradation | ||
| AKT1 | + | Energy Metabolism; PI3K/Akt Signaling | ||
| ARRB1 | + | Tyrosine Kinases; Wnt/Hedgehog/Notch | ||
| BCL2 | + | Apoptosis Signaling Pathway | ||
| CA9 | + | Angiogenesis | ||
| CD274 | + | NF-kappaB Signaling | ||
| CDX2 | + | Wnt/Hedgehog/Notch | ||
| CHST4 | + | O-linked Glycosylation of Mucins | ||
| EGFR | + | + | Akt Signaling Pathway; Jak/STAT Signaling Pathway; MAPK Signaling: Mitogens; mTOR Signaling | |
| EPHB1 | + | ErbB2-ErbB3 Heterodimers Pathway | ||
| ERBB2 | + | + | Akt Pathway Apoptosis Pathway MAPK Pathway NF-kappaB Pathway | |
| FZD1 | + | Neural Stem Cells and Lineage-Specific Markers; Wnt Signaling Pathways | ||
| HNF4A | + | TGF-beta Signaling Pathways | ||
| IGF1 | + | IGF1R Signaling Cascade | ||
| IGF1R | + | IGF1R Signaling Cascade | ||
| KDR | + | Akt Pathway Apoptosis Pathway NF-kappaB Pathway VEGF Pathway | ||
| KIT | + | + | NF-kappaB Signaling; Tyrosine Kinases | |
| KRAS | + | + | + | PI3K-Akt-mTOR Pathway TGF-beta Pathway Insulin Pathway |
| KRT5 | + | Cytoskeletal Signaling | ||
| MIR205 | + | miRNA-Mediated Gene Silencing | ||
| MIR373 | + | Endoderm Differentiation Pathways | ||
| MLH1 | + | Cell Cycle/DNA Damage | ||
| MUC1 | + | + | EGF Pathway; ILK Signaling | |
| MUC16 | + | + | O-linked Glycosylation of Mucins | |
| MUC2 | + | NTHi-Induced Signaling | ||
| MUC4 | + | Cell Adhesion | ||
| MUC5AC | + | Mucin Expression in CF | ||
| MUC6 | + | C-type Lectin Receptors (CLRs) | ||
| NRG1 | + | Apoptosis and Survival Role of CDK5 in Neuronal Death and Survival | ||
| PDGFRA | + | Akt Pathway; Apoptosis Pathway | ||
| PIK3CA | + | + | EMT Pathway PI3K-Akt-mTOR Pathway TLR Pathway | |
| PMS1 | + | DNA Mismatch Repair | ||
| PMS2 | + | DNA Mismatch Repair | ||
| PTEN | + | + | Cytoskeleton Remodeling FAK Signaling; Apoptosis Pathway PI3K-Akt-mTOR Pathway | |
| RET | + | + | G-protein Signaling_H-RAS Regulation Pathway | |
| ROR2 | + | Wnt Pathway | ||
| SLC3A2 | + | Energy Metabolism | ||
| SMAD4 | + | TGF-beta Signaling Pathways; Th17 Differentiation | ||
| SMARCB1 | + | AMPK Enzyme Complex Pathway; BRCA1 Pathway; Chromatin Remodeling (Acetylation); Glucocorticoid Receptor Signaling | ||
| STK11 | + | mTOR Signaling | ||
| TGFA | + | Angiogenesis; Tyrosine Kinases | ||
| TGFBR2 | + | Akt Pathway Apoptosis Pathway NF-kappaB Pathway TGF-beta Pathway | ||
| TP53 | + | Akt Pathway Apoptosis Pathway MAPK Pathway mTOR Pathway | ||
| TP63 | + | + | Development Notch Signaling Pathway; DNA Damage | |
| TRAK1 | + | O-linked glycosylation | ||
| UPF1 | + | Translational Control | ||
| VEGFA | + | Cell adhesion_Plasmin Signaling; Cytoskeleton Remodeling FAK Signaling; VEGF Signaling and Activation | ||
| WNT5A | + | EMT Pathway; Wnt Pathway; GSK3 Signaling |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khalele, B.; Laforga, J.B.; Kajo, K.; Kajová Macháleková, K. Adenosquamous Carcinomas and Mucinous Adenocarcinoma of the Minor Salivary Glands: Immunohistochemical and Molecular Insights. J. Mol. Pathol. 2022, 3, 273-285. https://doi.org/10.3390/jmp3040023
Khalele B, Laforga JB, Kajo K, Kajová Macháleková K. Adenosquamous Carcinomas and Mucinous Adenocarcinoma of the Minor Salivary Glands: Immunohistochemical and Molecular Insights. Journal of Molecular Pathology. 2022; 3(4):273-285. https://doi.org/10.3390/jmp3040023
Chicago/Turabian StyleKhalele, Bacem, Juan B. Laforga, Karol Kajo, and Katarína Kajová Macháleková. 2022. "Adenosquamous Carcinomas and Mucinous Adenocarcinoma of the Minor Salivary Glands: Immunohistochemical and Molecular Insights" Journal of Molecular Pathology 3, no. 4: 273-285. https://doi.org/10.3390/jmp3040023
APA StyleKhalele, B., Laforga, J. B., Kajo, K., & Kajová Macháleková, K. (2022). Adenosquamous Carcinomas and Mucinous Adenocarcinoma of the Minor Salivary Glands: Immunohistochemical and Molecular Insights. Journal of Molecular Pathology, 3(4), 273-285. https://doi.org/10.3390/jmp3040023