
Optimal Assessment of Metastatic Breast Carcinoma: The Value of Cytopathology Combined with Molecular Analysis


Abstract
:1. Introduction
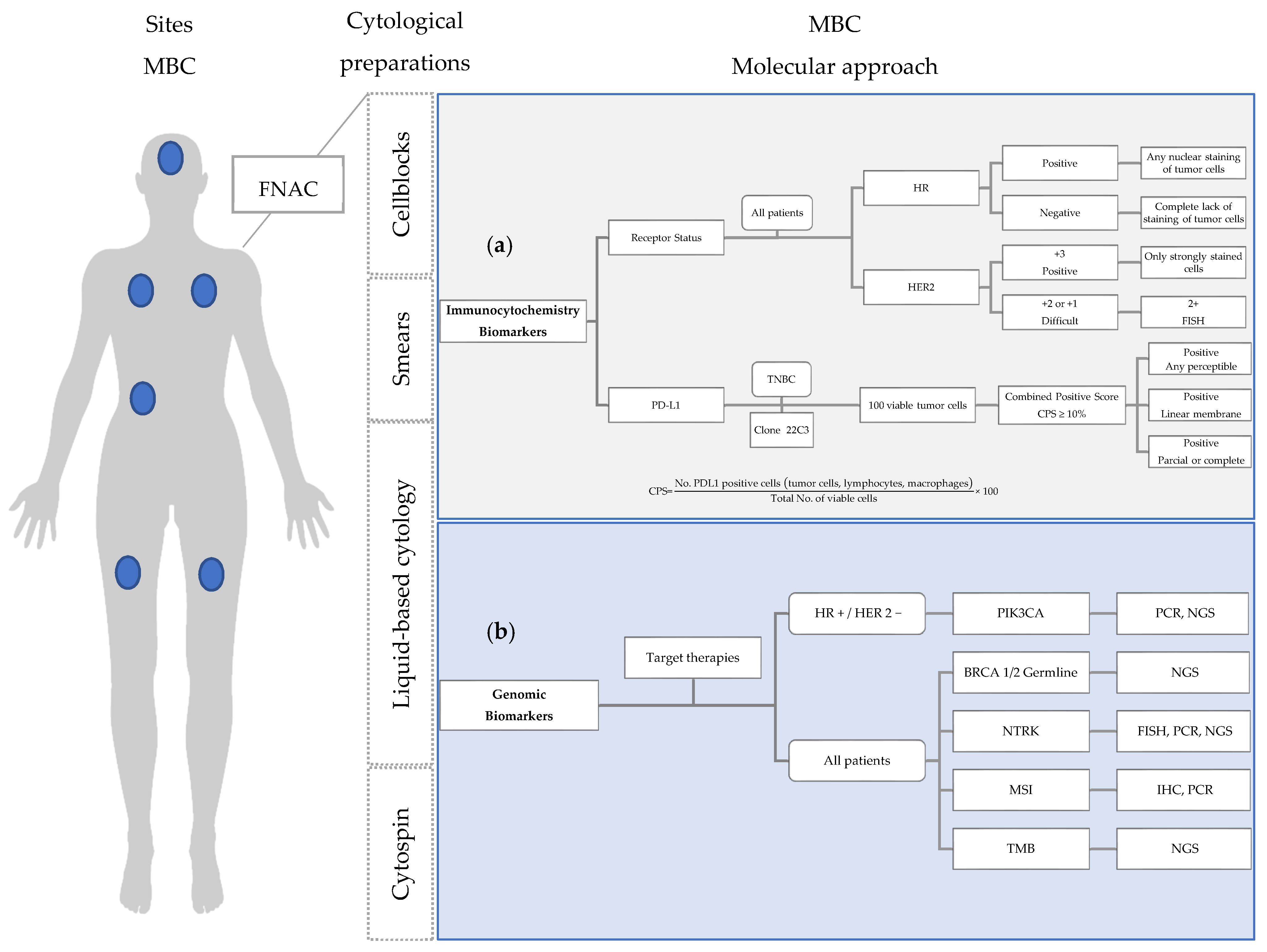
2. Metastatic Breast Cancer: Molecular Cytological Approach
2.1. Immunocytochemistry Biomarkers: Receptor Status

{kind=link}
| Study (Author, Year; Type of Study) | Number (Articles or Cases; Period) | Discordance Rates PBC vs. MBC |
|---|---|---|
| Aurilio et al., 2014 [20] Meta-analysis | 48 articles From 1983 to 2011 | ER: 20% PR: 33% HER2: 8% |
| Yeung et al., 2016 [17] Review | 47 articles From 1988 to 2012 | ER: 14% PR: 21% HER2: 10% |
| Nakayama et al., 2016 [21] Prospective | 20 paired cytology cases From 2015 | ER: 24% PR: 24% HER2: 5% |
| Pareja et al., 2017 [22] Prospective | 65 paired cytology cases From 2007 to 2009 | ER: 21.5% PR: 41.5% HER2: 3.1% |
| Schrijver et al., 2018 [23] Systematic review and meta-analysis | 39 articles From 1989 to 2016 | ER: 19.3% PR: 30.9% HER2: 10.3% |
| Matsui et al., 2019 [24] Prospective | 62 paired cytology cases From 2015 to 2016 | ER: 18.2% PR: 36.4% HER2: 8.2% |
| Sperduto et al., 2020 [25] Retrospective | 316 paired cases From 2006 and 2017 | ER: 22% PR: 26% HER2: 10% |
| Kotecha et al., 2021 [16] Systematic review and meta-analysis | 15 articles From 2007 to 2020 | ER: 17% PR: 23% HER2: 12% |
2.2. Immunocytochemistry Biomarkers: Program Death Ligand-1 (PD-L1)
2.3. Genomic Biomarkers
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Schiemann, W.P. Introduction to This Special Issue “Breast Cancer Metastasis. J. Cancer Metastasis Treat. 2020, 6, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loibl, S.; Poortmans, P.; Morrow, M.; Denkert, C.; Curigliano, G. Breast Cancer. Lancet 2021, 397, 1750–1769. [Google Scholar] [CrossRef] [PubMed]
- Martins, D.; Beca, F.; Schmitt, F. Metastatic Breast Cancer: Mechanisms and Opportunities for Cytology. Cytopathol. Off. J. Br. Soc. Clin. Cytol. 2014, 25, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Gennari, A.; André, F.; Barrios, C.H.; Cortés, J.; de Azambuja, E.; DeMichele, A.; Dent, R.; Fenlon, D.; Gligorov, J.; Hurvitz, S.A.; et al. ESMO Clinical Practice Guideline for the Diagnosis, Staging and Treatment of Patients with Metastatic Breast Cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 1475–1495. [Google Scholar] [CrossRef] [PubMed]
- Na, K.; Lee, J.-Y.; Sung, J.-Y.; Kim, G.M.; Koo, J.S.; Kim, H.-S. Comparative Clinicopathological and Cytomorphological Analyses of Peritoneal Carcinomatosis Associated with Metastatic Breast Carcinoma and Primary Peritoneal/Ovarian Carcinoma in Patients with a History of Breast Carcinoma. Virchows Arch. Int. J. Pathol. 2018, 473, 165–175. [Google Scholar] [CrossRef]
- Hölzel, D.; Eckel, R.; Bauerfeind, I.; Baier, B.; Beck, T.; Braun, M.; Ettl, J.; Hamann, U.; Kiechle, M.; Mahner, S.; et al. Improved Systemic Treatment for Early Breast Cancer Improves Cure Rates, Modifies Metastatic Pattern and Shortens Post-Metastatic Survival: 35-Year Results from the Munich Cancer Registry. J. Cancer Res. Clin. Oncol. 2017, 143, 1701–1712. [Google Scholar] [CrossRef]
- Cramer, H. Cytopathology of Metastatic Breast Cancer. Clin. Breast Cancer 2000, 1, 243–244. [Google Scholar] [CrossRef]
- Pinto, D.; Schmitt, F.C. Immunohistochemistry Applied to Breast Cytological Material. Pathobiology 2022, 89, 343–358. [Google Scholar] [CrossRef]
- Roy-Chowdhuri, S.; Dacic, S.; Ghofrani, M.; Illei, P.B.; Layfield, L.J.; Lee, C.; Michael, C.W.; Miller, R.A.; Mitchell, J.W.; Nikolic, B.; et al. Collection and Handling of Thoracic Small Biopsy and Cytology Specimens for Ancillary Studies: Guideline From the College of American Pathologists in Collaboration With the American College of Chest Physicians, Association for Molecular Pathology, American Society of Cytopathology, American Thoracic Society, Pulmonary Pathology Society, Papanicolaou Society of Cytopathology, Society of Interventional Radiology, and Society of Thoracic Radiology. Arch. Pathol. Lab. Med. 2020, 144, 933–958. [Google Scholar] [CrossRef]
- Van Poznak, C.; Somerfield, M.R.; Bast, R.C.; Cristofanilli, M.; Goetz, M.P.; Gonzalez-Angulo, A.M.; Hicks, D.G.; Hill, E.G.; Liu, M.C.; Lucas, W.; et al. Use of Biomarkers to Guide Decisions on Systemic Therapy for Women With Metastatic Breast Cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 2695–2704. [Google Scholar] [CrossRef] [PubMed]
- Gradishar, W.J.; Moran, M.S.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Anderson, B.; Burstein, H.J.; Chew, H.; Dang, C.; et al. Breast Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. JNCCN 2022, 20, 691–722. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.; Murata, Y.; Mori, K.; Yamashiro, K.; Kuraoka, K.; Ichihara, S.; Taguchi, K.; Suzuki, H.; Ito, M.; Yamashita, N. Evaluation of the HER2 and Hormone Receptor Status in Metastatic Breast Cancer Using Cell Blocks: A Multi-Institutional Study. Acta Cytol. 2018, 62, 288–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanber, Y.; Pusztaszeri, M.; Auger, M. Immunocytochemistry for Diagnostic Cytopathology-A Practical Guide. Cytopathol. Off. J. Br. Soc. Clin. Cytol. 2021, 32, 562–587. [Google Scholar] [CrossRef] [PubMed]
- Monaco, S.E.; Wu, Y.; Teot, L.A.; Cai, G. Assessment of Estrogen Receptor (ER), Progesterone Receptor (PR), and Human Epidermal Growth Factor Receptor 2 (HER2) Status in the Fine Needle Aspirates of Metastatic Breast Carcinomas. Diagn. Cytopathol. 2013, 41, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, R.; Tonse, R.; Rubens, M.; McDermott, M.W.; Odia, Y.; Appel, H.; Mehta, M.P. Systematic Review and Meta-Analysis of Breast Cancer Brain Metastasis and Primary Tumor Receptor Expression Discordance. Neuro-Oncol. Adv. 2021, 3, vdab010. [Google Scholar] [CrossRef]
- Yeung, C.; Hilton, J.; Clemons, M.; Mazzarello, S.; Hutton, B.; Haggar, F.; Addison, C.L.; Kuchuk, I.; Zhu, X.; Gelmon, K.; et al. Estrogen, Progesterone, and HER2/Neu Receptor Discordance between Primary and Metastatic Breast Tumours-a Review. Cancer Metastasis Rev. 2016, 35, 427–437. [Google Scholar] [CrossRef]
- Malmgren, J.A.; Mayer, M.; Atwood, M.K.; Kaplan, H.G. Differential Presentation and Survival of de Novo and Recurrent Metastatic Breast Cancer over Time: 1990–2010. Breast Cancer Res. Treat. 2018, 167, 579–590. [Google Scholar] [CrossRef] [Green Version]
- Amir, E.; Miller, N.; Geddie, W.; Freedman, O.; Kassam, F.; Simmons, C.; Oldfield, M.; Dranitsaris, G.; Tomlinson, G.; Laupacis, A.; et al. Prospective Study Evaluating the Impact of Tissue Confirmation of Metastatic Disease in Patients with Breast Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 587–592. [Google Scholar] [CrossRef]
- Aurilio, G.; Disalvatore, D.; Pruneri, G.; Bagnardi, V.; Viale, G.; Curigliano, G.; Adamoli, L.; Munzone, E.; Sciandivasci, A.; De Vita, F.; et al. A Meta-Analysis of Oestrogen Receptor, Progesterone Receptor and Human Epidermal Growth Factor Receptor 2 Discordance between Primary Breast Cancer and Metastases. Eur. J. Cancer 2014, 50, 277–289. [Google Scholar] [CrossRef]
- Nakayama, Y.; Nakagomi, H.; Omori, M.; Inoue, M.; Takahashi, K.; Maruyama, M.; Takano, A.; Furuya, K.; Amemiya, K.; Ishii, E.; et al. Benefits of Using the Cell Block Method to Determine the Discordance of the HR/HER2 Expression in Patients with Metastatic Breast Cancer. Breast Cancer 2016, 23, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Pareja, F.; Murray, M.P.; Des Jean, R.; Konno, F.; Friedlander, M.; Lin, O.; Edelweiss, M. Cytologic Assessment of Estrogen Receptor, Progesterone Receptor, and HER2 Status in Metastatic Breast Carcinoma. J. Am. Soc. Cytopathol. 2017, 6, 33–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrijver, W.A.M.E.; Suijkerbuijk, K.P.M.; van Gils, C.H.; van der Wall, E.; Moelans, C.B.; van Diest, P.J. Receptor Conversion in Distant Breast Cancer Metastases: A Systematic Review and Meta-Analysis. J. Natl. Cancer Inst. 2018, 110, 568–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsui, A.; Murata, Y.; Masuda, N.; Mori, K.; Takahashi, M.; Yamashiro, K.; Aogi, K.; Maeda, S.; Itou, M.; Ozaki, S.; et al. Clinical Significance of Evaluating Hormone Receptor and HER2 Protein Using Cell Block against Metastatic Breast Cancer: A Multi-Institutional Study. Oncotarget 2019, 10, 5680–5689. [Google Scholar] [CrossRef] [Green Version]
- Sperduto, P.W.; Mesko, S.; Li, J.; Cagney, D.; Aizer, A.; Lin, N.U.; Nesbit, E.; Kruser, T.J.; Chan, J.; Braunstein, S.; et al. Estrogen/Progesterone Receptor and HER2 Discordance between Primary Tumor and Brain Metastases in Breast Cancer and Its Effect on Treatment and Survival. Neuro-Oncology 2020, 22, 1359–1367. [Google Scholar] [CrossRef]
- Shabaik, A.; Lin, G.; Peterson, M.; Hasteh, F.; Tipps, A.; Datnow, B.; Weidner, N. Reliability of Her2/Neu, Estrogen Receptor, and Progesterone Receptor Testing by Immunohistochemistry on Cell Block of FNA and Serous Effusions from Patients with Primary and Metastatic Breast Carcinoma. Diagn. Cytopathol. 2011, 39, 328–332. [Google Scholar] [CrossRef]
- Kumar, S.K.; Gupta, N.; Rajwanshi, A.; Joshi, K.; Singh, G. Immunochemistry for Oestrogen Receptor, Progesterone Receptor and HER2 on Cell Blocks in Primary Breast Carcinoma. Cytopathol. Off. J. Br. Soc. Clin. Cytol. 2012, 23, 181–186. [Google Scholar] [CrossRef]
- Bueno Angela, S.P.; Viero, R.M.; Soares, C.T. Fine Needle Aspirate Cell Blocks Are Reliable for Detection of Hormone Receptors and HER-2 by Immunohistochemistry in Breast Carcinoma. Cytopathol. Off. J. Br. Soc. Clin. Cytol. 2013, 24, 26–32. [Google Scholar] [CrossRef]
- Ferguson, J.; Chamberlain, P.; Cramer, H.M.; Wu, H.H. ER, PR, and Her2 Immunocytochemistry on Cell-Transferred Cytologic Smears of Primary and Metastatic Breast Carcinomas: A Comparison Study with Formalin-Fixed Cell Blocks and Surgical Biopsies. Diagn. Cytopathol. 2013, 41, 575–581. [Google Scholar] [CrossRef]
- Francis, I.M.; Altemaimi, R.A.; Al-Ayadhy, B.; Alath, P.; Jaragh, M.; Mothafar, F.J.; Kapila, K. Hormone Receptors and Human Epidermal Growth Factor (HER2) Expression in Fine-Needle Aspirates from Metastatic Breast Carcinoma—Role in Patient Management. J. Cytol. 2019, 36, 94–100. [Google Scholar] [CrossRef]
- Beca, F.; Schmitt, F.C. Ancillary Tests in Breast Cytology: A Practical Guide. Acta Cytol. 2019, 63, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Verret, B.; Bottosso, M.; Hervais, S.; Pistilli, B. The Molecular Predictive and Prognostic Biomarkers in Metastatic Breast Cancer: The Contribution of Molecular Profiling. Cancers 2022, 14, 4203. [Google Scholar] [CrossRef] [PubMed]
- Iaccarino, A.; Salatiello, M.; Migliatico, I.; De Luca, C.; Gragnano, G.; Russo, M.; Bellevicine, C.; Malapelle, U.; Troncone, G.; Vigliar, E. PD-L1 and beyond: Immuno-Oncology in Cytopathology. Cytopathol. Off. J. Br. Soc. Clin. Cytol. 2021, 32, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Satturwar, S.; Girolami, I.; Munari, E.; Ciompi, F.; Eccher, A.; Pantanowitz, L. Program Death Ligand-1 Immunocytochemistry in Lung Cancer Cytological Samples: A Systematic Review. Diagn. Cytopathol. 2022, 50, 313–323. [Google Scholar] [CrossRef]
- Mansour, M.S.I.; Lindquist, K.E.; Seidal, T.; Mager, U.; Mohlin, R.; Tran, L.; Hejny, K.; Holmgren, B.; Violidaki, D.; Dobra, K.; et al. PD-L1 Testing in Cytological Non-Small Cell Lung Cancer Specimens: A Comparison with Biopsies and Review of the Literature. Acta Cytol. 2021, 65, 501–509. [Google Scholar] [CrossRef]
- Zhang, X. Molecular Classification of Breast Cancer. Arch. Pathol. Lab. Med. 2022. [Google Scholar] [CrossRef]
- Mosele, F.; Remon, J.; Mateo, J.; Westphalen, C.B.; Barlesi, F.; Lolkema, M.P.; Normanno, N.; Scarpa, A.; Robson, M.; Meric-Bernstam, F.; et al. Recommendations for the Use of Next-Generation Sequencing (NGS) for Patients with Metastatic Cancers: A Report from the ESMO Precision Medicine Working Group. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2020, 31, 1491–1505. [Google Scholar] [CrossRef]
- Dupain, C.; Masliah-Planchon, J.; Gu, C.; Girard, E.; Gestraud, P.; Du Rusquec, P.; Borcoman, E.; Bello, D.; Ricci, F.; Hescot, S.; et al. Fine-Needle Aspiration as an Alternative to Core Needle Biopsy for Tumour Molecular Profiling in Precision Oncology: Prospective Comparative Study of next-Generation Sequencing in Cancer Patients Included in the SHIVA02 Trial. Mol. Oncol. 2021, 15, 104–115. [Google Scholar] [CrossRef]
- Dinarvand, P.; Liu, C.; Roy-Chowdhuri, S. A Decade of Change: Trends in the Practice of Cytopathology at a Tertiary Care Cancer Centre. Cytopathology 2021, 32, 604–610. [Google Scholar] [CrossRef]
- Lee, H.-B.; Joung, J.-G.; Kim, J.; Lee, K.-M.; Ryu, H.S.; Lee, H.-O.; Moon, H.-G.; Park, W.-Y.; Noh, D.-Y.; Han, W. The Use of FNA Samples for Whole-Exome Sequencing and Detection of Somatic Mutations in Breast Cancer Surgical Specimens. Cancer Cytopathol. 2015, 123, 669–677. [Google Scholar] [CrossRef]
- Roy-Chowdhuri, S.; Chen, H.; Singh, R.R.; Krishnamurthy, S.; Patel, K.P.; Routbort, M.J.; Manekia, J.; Barkoh, B.A.; Yao, H.; Sabir, S.; et al. Concurrent Fine Needle Aspirations and Core Needle Biopsies: A Comparative Study of Substrates for next-Generation Sequencing in Solid Organ Malignancies. Mod. Pathol. 2017, 30, 499–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisapia, P.; Pepe, F.; Sgariglia, R.; Nacchio, M.; Russo, G.; Conticelli, F.; Girolami, I.; Eccher, A.; Bellevicine, C.; Vigliar, E.; et al. Next Generation Sequencing in Cytology. Cytopathol. Off. J. Br. Soc. Clin. Cytol. 2021, 32, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Souza da Silva, R.; Pinto, R.; Cirnes, L.; Schmitt, F. Tissue Management in Precision Medicine: What the Pathologist Needs to Know in the Molecular Era. Front. Mol. Biosci. 2022, 9, 983102. [Google Scholar] [CrossRef] [PubMed]
- Penault-Llorca, F.; Kerr, K.M.; Garrido, P.; Thunnissen, E.; Dequeker, E.; Normanno, N.; Patton, S.J.; Fairley, J.; Kapp, J.; de Ridder, D.; et al. Expert Opinion on NSCLC Small Specimen Biomarker Testing—Part 1: Tissue Collection and Management. Virchows Arch. 2022, 481, 335–350. [Google Scholar] [CrossRef]
- Janaki, N.; Harbhajanka, A.; Michael, C.W.; Bomeisl, P.; Wasman, J.; Atchley, M.; Miskiewicz, K.; Alouani, D.; Sadri, N. Comparison of Cytocentrifugation Supernatant Fluid and Formalin-Fixed Paraffin-Embedded Tissue for Targeted next-Generation Sequencing. Cancer Cytopathol. 2019, 127, 297–305. [Google Scholar] [CrossRef]
- Ruff, H.M.; Lou, S.K.; Hahn, E.; Grenier, S.; Stockley, T.L.; Boerner, S.L. Molecular Yield and Cytomorphologic Assessment of Fine Needle Aspiration Specimen Supernatants. J. Am. Soc. Cytopathol. 2022, 11, 142–153. [Google Scholar] [CrossRef]
- Pepe, F.; Pisapia, P.; Gristina, V.; Rocco, D.; Micheli, M.; Micheli, P.; Iaccarino, A.; Tufano, R.; Gragnano, G.; Russo, G.; et al. Tumor Mutational Burden on Cytological Samples: A Pilot Study. Cancer Cytopathol. 2021, 129, 460–467. [Google Scholar] [CrossRef]
- Bellevicine, C.; Malapelle, U.; Vigliar, E.; Pisapia, P.; Vita, G.; Troncone, G. How to Prepare Cytological Samples for Molecular Testing. J. Clin. Pathol. 2017, 70, 819–826. [Google Scholar] [CrossRef] [Green Version]
- Hong, R.; Xu, B. Breast Cancer: An up-to-Date Review and Future Perspectives. Cancer Commun. 2022, 42, 913–936. [Google Scholar] [CrossRef]
- Bertucci, F.; Ng, C.K.Y.; Patsouris, A.; Droin, N.; Piscuoglio, S.; Carbuccia, N.; Soria, J.C.; Dien, A.T.; Adnani, Y.; Kamal, M.; et al. Genomic Characterization of Metastatic Breast Cancers. Nature 2019, 569, 560–564. [Google Scholar] [CrossRef]
- Henry, N.L.; Somerfield, M.R.; Dayao, Z.; Elias, A.; Kalinsky, K.; McShane, L.M.; Moy, B.; Park, B.H.; Shanahan, K.M.; Sharma, P.; et al. Biomarkers for Systemic Therapy in Metastatic Breast Cancer: ASCO Guideline Update. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2022, 40, 3205–3221. [Google Scholar] [CrossRef] [PubMed]
- Danesi, R.; Fogli, S.; Indraccolo, S.; Del Re, M.; Dei Tos, A.P.; Leoncini, L.; Antonuzzo, L.; Bonanno, L.; Guarneri, V.; Pierini, A.; et al. Druggable Targets Meet Oncogenic Drivers: Opportunities and Limitations of Target-Based Classification of Tumors and the Role of Molecular Tumor Boards. ESMO Open 2021, 6, 100040. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Narayan, P.; Osgood, C.L.; Wedam, S.; Prowell, T.M.; Gao, J.J.; Shah, M.; Krol, D.; Wahby, S.; Royce, M.; et al. U.S. FDA Drug Approvals for Breast Cancer: A Decade in Review. Clin. Cancer Res. 2022, 28, 1072–1086. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, F.; Lozano, M.D. Molecular/Biomarker Testing in Lung Cytology: A Practical Approach. Diagn. Cytopathol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, A.G.; Tsao, M.S.; Beasley, M.B.; Borczuk, A.C.; Brambilla, E.; Cooper, W.A.; Dacic, S.; Jain, D.; Kerr, K.M.; Lantuejoul, S.; et al. The 2021 WHO Classification of Lung Tumors: Impact of Advances Since 2015. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2022, 17, 362–387. [Google Scholar] [CrossRef]

| Biomarker/Alteration | BC Subtypes | Detection | Prevalence | ESCAT/NCCN Category | FDA-Approved Agents [12] |
|---|---|---|---|---|---|
| HER2 Amplification | HER2+ | IHC, FISH | 15–20% | IA/1 | Trastuzumab, T-DM1, lapatinib, trastuzumab + pertuzumab, neratinib |
| BRCA 1, BRCA 2 Germline Mutation | All | NGS | 4% | IA/1 | Olaparib Talazoparib |
| BRCA 1, BRCA 2 Somatic Mutation | HER 2 low status | IHC | 3% | IIA/2A | Trastuzumab deruxtecan |
| PIK3CA Hotspot mutation | HR+/HER2− | PCR, NGS | 30–40% | IA/1 | Alpelisib + fulvestrant |
| MSI-H dMMR | All | IHC, PCR | 1% | IC/2A | Pembrolizumab Dostarlimab-gxly |
| NTRK Fusion | All | FISH, PCR, NGS | 1% | IC/2A | Larotrectinib Entrectinib |
| PD-L1 | TNBC | IHC | 20% | IA/1 | Pembrolizumab + chemotherapy |
| TMB-High (≥10 mut/mb) | All | NGS | 8–11% | IA/2A | Pembrolizumab |
| ESR1 Mutation (mechanism of resistance) | HER+ | NGS | 10% | IIA/1 | Fulvestrant |
| PTEN Mutation | NA | NGS | 7% | IIA/NA | NA |
| AKT1 Mutation | NA | NGS | 5% | IIB/NA | NA |
| NF1 Mutation (resistance biomarker) | NA | NGS | 6% | NA | NA |
| MDM2 Amplification | NA | NGS | ~1% | IIIA/NA | NA |
| ERBB3 Mutation | NA | NGS | 2% | IIIB/NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Souza da Silva, R.; Schmitt, F. Optimal Assessment of Metastatic Breast Carcinoma: The Value of Cytopathology Combined with Molecular Analysis. J. Mol. Pathol. 2022, 3, 329-338. https://doi.org/10.3390/jmp3040028
Souza da Silva R, Schmitt F. Optimal Assessment of Metastatic Breast Carcinoma: The Value of Cytopathology Combined with Molecular Analysis. Journal of Molecular Pathology. 2022; 3(4):329-338. https://doi.org/10.3390/jmp3040028
Chicago/Turabian StyleSouza da Silva, Ricella, and Fernando Schmitt. 2022. "Optimal Assessment of Metastatic Breast Carcinoma: The Value of Cytopathology Combined with Molecular Analysis" Journal of Molecular Pathology 3, no. 4: 329-338. https://doi.org/10.3390/jmp3040028
APA StyleSouza da Silva, R., & Schmitt, F. (2022). Optimal Assessment of Metastatic Breast Carcinoma: The Value of Cytopathology Combined with Molecular Analysis. Journal of Molecular Pathology, 3(4), 329-338. https://doi.org/10.3390/jmp3040028