
Digital Subtraction Angiography (DSA) Technical and Diagnostic Aspects in the Study of Lower Limb Arteries

 ,
,  , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Digital Subtraction Angiography Technique
2.1. Pre-Procedural Evaluation
2.2. Angiography Technique
3. Angiographic Findings
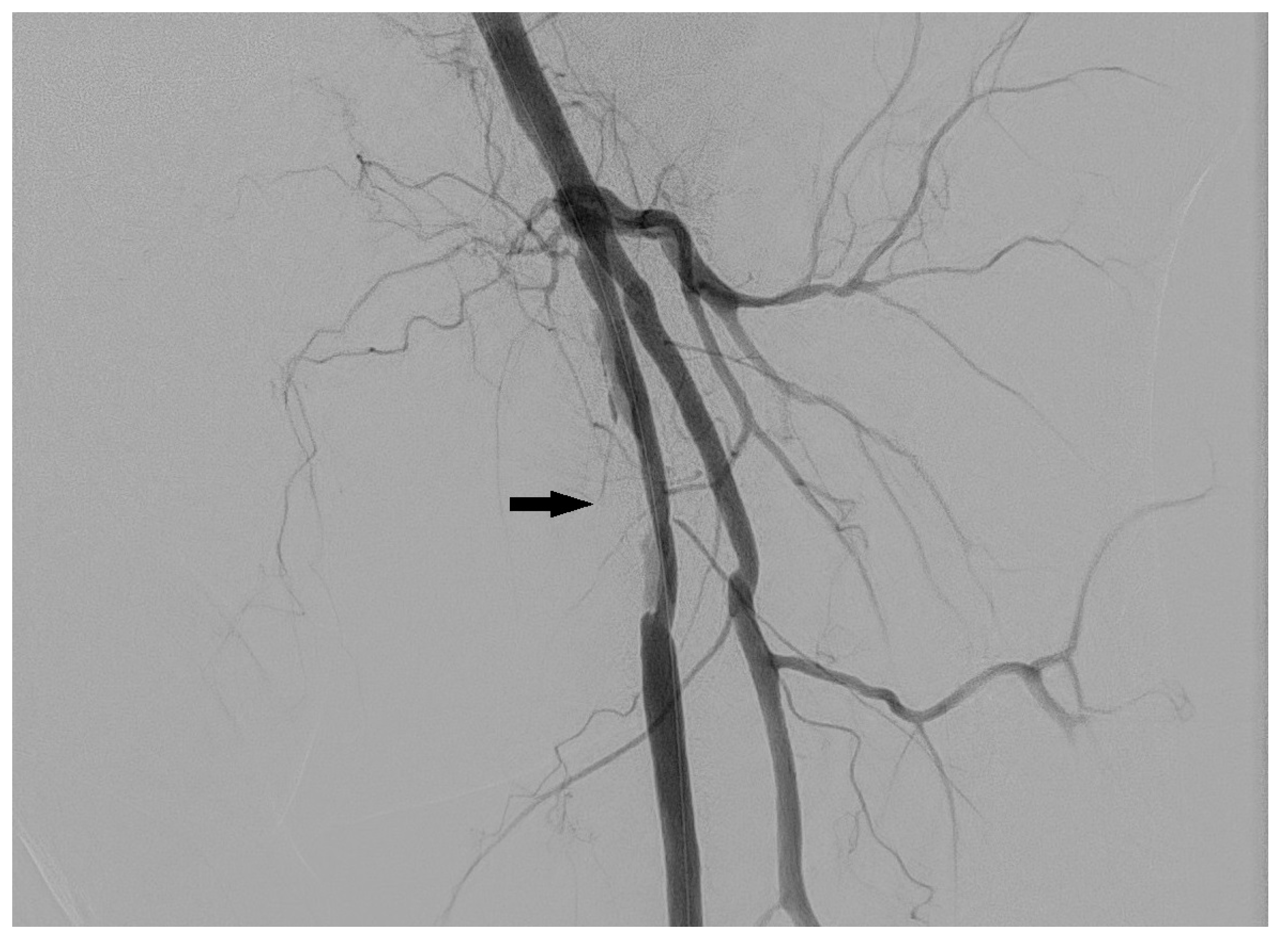
3.1. Stenosis and Occlusion
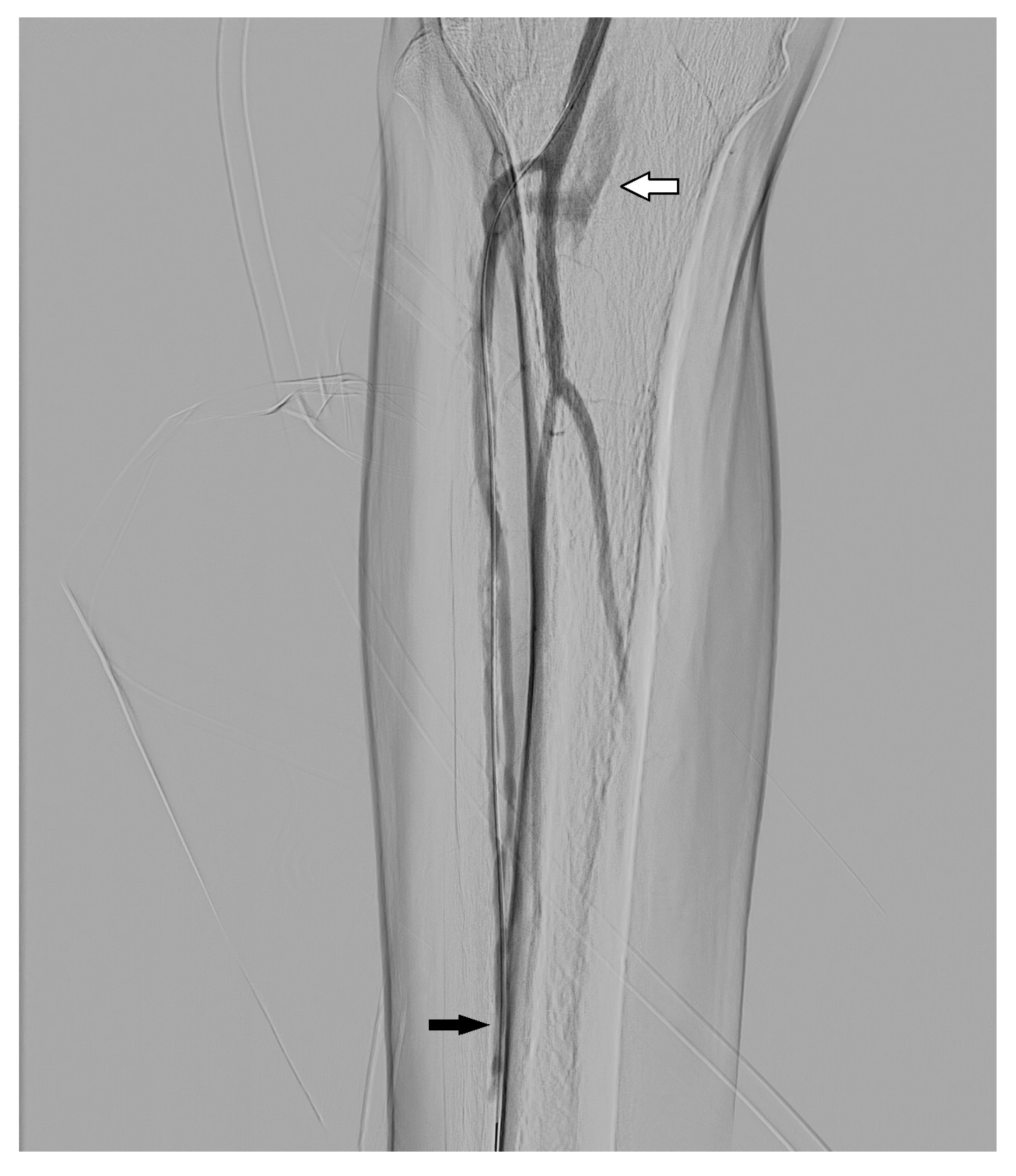
3.2. Dissection
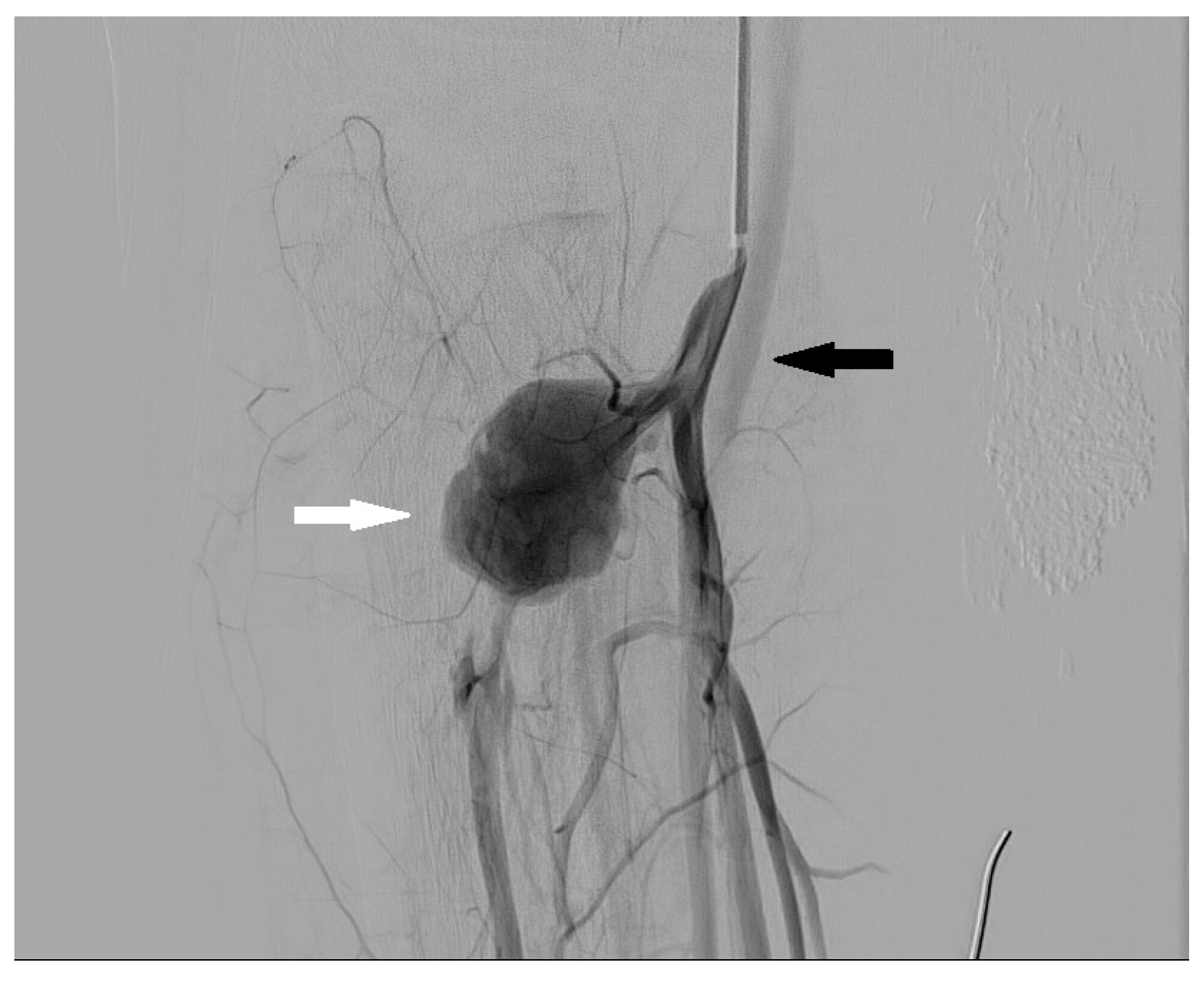
3.3. Arteriovenous Fistula
3.4. Aneurysm and Pseudoaneurysm
4. Risks of DSA
4.1. Percutaneous Arterial Access-Related Complications
4.2. Contrast Medium-Related Risks
4.3. Radiation Dose
5. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dua, A.; Lee, C.J. Epidemiology of Peripheral Arterial Disease and Critical Limb Ischemia. Tech. Vasc. Interv. Radiol. 2016, 19, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Levin, D.C.; Rao, V.M.; Parker, L.; Frangos, A.J.; Sunshine, J.H. The effect of the introduction of MR and CT angiography on the utilization of catheter angiography for peripheral arterial disease. J. Am. Coll. Radiol. 2007, 4, 457–460. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.C.; Levin, D.C.; Parker, L.; Rao, V.M. Have CT and MR Angiography Replaced Catheter Angiography in Diagnosing Peripheral Arterial Disease? J. Am. Coll. Radiol. 2015, 12, 909–914. [Google Scholar] [CrossRef] [PubMed]
- Heijenbrok-Kal, M.H.; Kock, M.C.; Hunink, M.G. Lower extremity arterial disease: Multidetector CT angiography meta-analysis. Radiology 2007, 245, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Fotiadis, N.; Kyriakides, C.; Bent, C.; Vorvolakos, T.; Matson, M. 64-section CT angiography in patients with critical limb ischaemia and severe claudication: Comparison with digital subtractive angiography. Clin. Radiol. 2011, 66, 945–952. [Google Scholar] [CrossRef]
- Al-Rudaini, H.E.A.; Han, P.; Liang, H. Comparison Between Computed Tomography Angiography and Digital Subtraction Angiography in Critical Lower Limb Ischemia. Curr. Med. Imaging Rev. 2019, 15, 496–503. [Google Scholar] [CrossRef]
- Willmann, J.K.; Baumert, B.; Schertler, T.; Wildermuth, S.; Pfammatter, T.; Verdun, F.R.; Seifert, B.; Marincek, B.; Böhm, T. Aortoiliac and lower extremity arteries assessed with 16-detector row CT angiography: Prospective comparison with digital subtraction angiography. Radiology 2005, 236, 1083–1093. [Google Scholar] [CrossRef] [Green Version]
- Collins, R.; Burch, J.; Cranny, G.; Aguiar-Ibáñez, R.; Craig, D.; Wright, K.; Berry, E.; Gough, M.; Kleijnen, J.; Westwood, M. Duplex ultrasonography, magnetic resonance angiography, and computed tomography angiography for diagnosis and assessment of symptomatic, lower limb peripheral arterial disease: Systematic review. BMJ 2007, 334, 1257. [Google Scholar] [CrossRef] [Green Version]
- Sun, Z. Digital Variance Angiography: A Promising Alternative Technology to Traditional Angiography for Improvement of Image Quality with Reduction of Radiation and Contrast Medium Doses. Cardiovasc. Interv. Radiol. 2021, 44, 460–461. [Google Scholar] [CrossRef]
- Weiss, C.R.; Azene, E.M.; Majdalany, B.S.; AbuRahma, A.F.; Collins, J.D.; Francois, C.; Gerhard-Herman, M.D.; Gornik, H.L.; Moriarty, J.M.; Norton, P.T.; et al. ACR Appropriateness Criteria® Sudden Onset of Cold, Painful Leg. J. Am. Coll. Radiol 2017, 14, S307–S313. [Google Scholar] [CrossRef]
- Kaufman, S.L.; Chang, R.; Kadir, S.; Mitchell, S.E.; White, R.I., Jr. Intraarterial digital subtraction angiography in diagnostic arteriography. Radiology 1984, 151, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Jeans, W.D. The development and use of digital subtraction angiography. Br. J. Radiol. 1990, 63, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.P.; Cragg, A.H.; Berbaum, K.S.; Nakagawa, N. Comparison of the efficacy of digital subtraction and film-screen angiography of the lower limb: Prospective study in 50 patients. Am. J. Roentgenol. 1992, 158, 431–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pomposelli, F. Arterial imaging in patients with lower extremity ischemia and diabetes mellitus. J. Vasc. Surg. 2010, 52, 81S–91S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, K.K.; Hawkins, I.F. Jr. Angiography of the lower extremity in atherosclerotic vascular disease. Current techniques. Surg. Clin. N. Am. 1992, 72, 767–789. [Google Scholar] [CrossRef]
- Cohen, M.I.; Vogelzang, R.L. A comparison of techniques for improved visualization of the arteries of the distal lower extremity. Am. J. Roentgenol. 1986, 147, 1021–1024. [Google Scholar] [CrossRef] [Green Version]
- Hoh, B.L.; Ogilvy, C.S. Endovascular treatment of cerebral vasospasm: Transluminal balloon angioplasty, intra-arterial papaverine, and intra-arterial nicardipine. Neurosurg. Clin. N. Am. 2005, 16, 501–516. [Google Scholar] [CrossRef]
- El-Zammar, Z.M.; Latorre, J.G.; Wang, D.; Satyan, S.; Elnour, E.; Kamel, A.; Devasenapathy, A.; Lodi, Y.M. Intra-arterial vasodilator use during endovascular therapy for acute ischemic stroke might improve reperfusion rate. Ann. N. Y. Acad. Sci 2012, 1268, 134–140. [Google Scholar] [CrossRef]
- Cina, A.; Steri, L.; Barbieri, P.; Contegiacomo, A.; Amodeo, E.M.; Di Stasi, C.; Morasca, A.; Romualdi, D.; Ciccarone, F.; Manfredi, R. Optimizing the Angiography Protocol to Reduce Radiation Dose in Uterine Artery Embolization: The Impact of Digital Subtraction Angiographies on Radiation Exposure. Cardiovasc. Interv. Radiol. 2022, 45, 249–254. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis--an inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.; TASC II Working Group; Bell, K.; Caporusso, J.; Durand-Zaleski, T.; et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Eur. J. Vasc. Endovasc. Surg. 2007, 33, S1–S75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hentsch, A.; Aschauer, M.A.; Balzer, J.O.; Brossmann, J.; Busch, H.P.; Davis, K.; Douek, P.; Ebner, F.; Van Engelshoven, J.M.A.; Gregor, M.; et al. Gadobutrol-enhanced moving-table magnetic resonance angiography in patients with peripheral vascular disease: A prospective, multi-centre blinded comparison with digital subtraction angiography. Eur. Radiol. 2003, 13, 2103–2114. [Google Scholar] [CrossRef] [PubMed]
- American College of Radiology. Manual on contrast media. Available online: http://www.acr.org/Quality-Safety/Resources/Contrast-Manual (accessed on 16 August 2022).
- Miller, D.L.; Balter, S.; Dixon, R.G.; Nikolic, B.; Bartal, G.; Cardella, J.F.; Dauer, L.T.; Stecker, M.S.; Society of Interventional Radiology Standards of Practice Committee. Quality improvement guidelines for recording patient radiation dose in the medical record for fluoroscopically guided procedures. J. Vasc. Interv. Radiol. 2012, 23, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Bartal, G.; Vano, E.; Paulo, G.; Miller, D.L. Management of patient and staff radiation dose in interventional radiology: Current concepts. Cardiovasc. Interv. Radiol. 2014, 37, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Bastian, M.B.; König, A.M.; Viniol, S.; Gyánó, M.; Szöllősi, D.; Góg, I.; Kiss, J.P.; Osvath, S.; Szigeti, K.; Mahnken, A.H.; et al. Digital Variance Angiography in Lower-Limb Angiography with Metal Implants. Cardiovasc. Interv. Radiol. 2021, 44, 452–459. [Google Scholar] [CrossRef]
- Gyánó, M.; Góg, I.; Óriás, V.I.; Ruzsa, Z.; Nemes, B.; Csobay-Novák, C.; Oláh, Z.; Nagy, Z.; Merkely, B.; Szigeti, K.; et al. Kinetic Imaging in Lower Extremity Arteriography: Comparison to Digital Subtraction Angiography. Radiology 2019, 290, 246–253. [Google Scholar] [CrossRef]
- Óriás, V.I.; Gyánó, M.; Góg, I.; Szöllősi, D.; Veres, D.S.; Nagy, Z.; Csobay-Novák, C.; Zoltán, O.; Kiss, J.P.; Osváth, S.; et al. Digital Variance Angiography as a Paradigm Shift in Carbon Dioxide Angiography. Investig. Radiol. 2019, 54, 428–436. [Google Scholar] [CrossRef]
- Gyánó, M.; Csobay-Novák, C.; Berczeli, M.; Góg, I.; Kiss, J.P.; Szigeti, K.; Osváth, S.; Nemes, B. Initial Operating Room Experience with Digital Variance Angiography in Carbon Dioxide-Assisted Lower Limb Interventions: A Pilot Study. Cardiovasc. Interv. Radiol. 2020, 43, 1226–1231. [Google Scholar] [CrossRef]
- Kagadis, G.C.; Tsantis, S.; Gatos, I.; Spiliopoulos, S.; Katsanos, K.; Karnabatidis, D. 2D perfusion DSA with an open-source, semi-automated, color-coded software for the quantification of foot perfusion following infrapopliteal angioplasty: A feasibility study. Eur. Radiol. Exp. 2020, 4, 47. [Google Scholar] [CrossRef]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Posa, A.; Tanzilli, A.; Barbieri, P.; Steri, L.; Arbia, F.; Mazza, G.; Longo, V.; Iezzi, R. Digital Subtraction Angiography (DSA) Technical and Diagnostic Aspects in the Study of Lower Limb Arteries. Radiation 2022, 2, 376-386. https://doi.org/10.3390/radiation2040028
Posa A, Tanzilli A, Barbieri P, Steri L, Arbia F, Mazza G, Longo V, Iezzi R. Digital Subtraction Angiography (DSA) Technical and Diagnostic Aspects in the Study of Lower Limb Arteries. Radiation. 2022; 2(4):376-386. https://doi.org/10.3390/radiation2040028
Chicago/Turabian StylePosa, Alessandro, Alessandro Tanzilli, Pierluigi Barbieri, Lorenzo Steri, Francesco Arbia, Giulia Mazza, Valentina Longo, and Roberto Iezzi. 2022. "Digital Subtraction Angiography (DSA) Technical and Diagnostic Aspects in the Study of Lower Limb Arteries" Radiation 2, no. 4: 376-386. https://doi.org/10.3390/radiation2040028
APA StylePosa, A., Tanzilli, A., Barbieri, P., Steri, L., Arbia, F., Mazza, G., Longo, V., & Iezzi, R. (2022). Digital Subtraction Angiography (DSA) Technical and Diagnostic Aspects in the Study of Lower Limb Arteries. Radiation, 2(4), 376-386. https://doi.org/10.3390/radiation2040028