
Facial Swelling in the Presence of a COVID-19 Diagnosis: Case Report


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
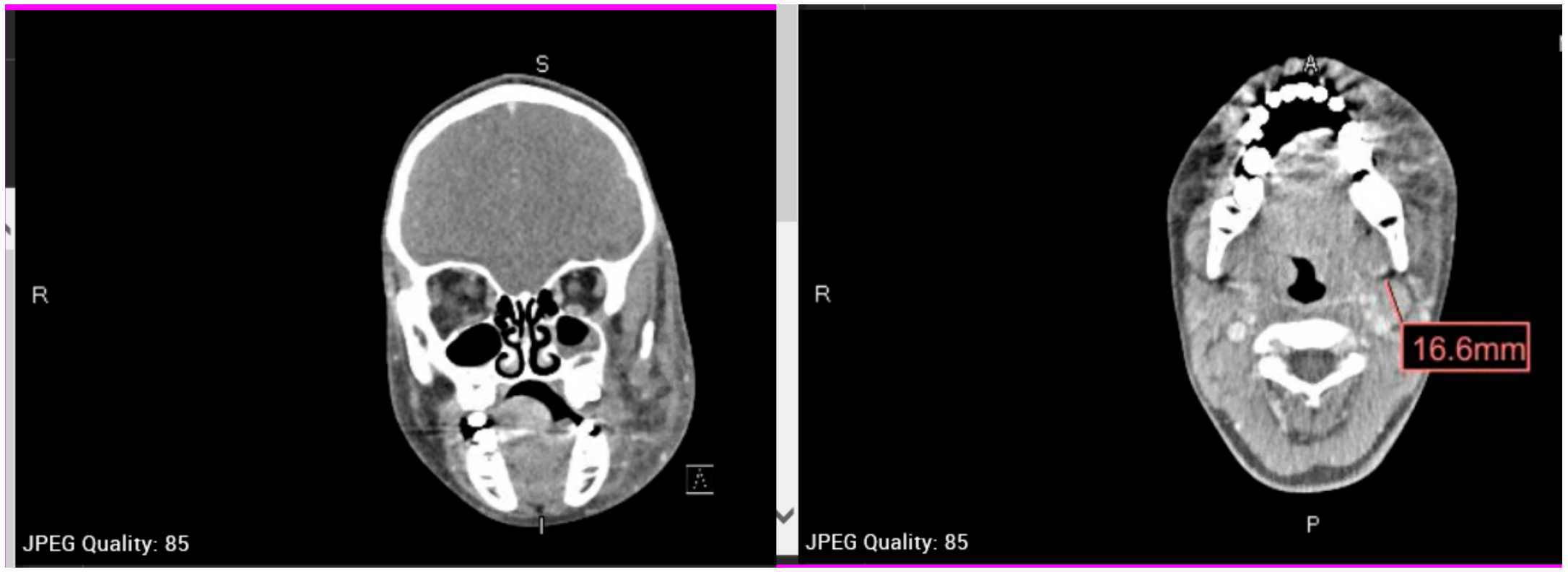
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fini, M.B. What dentists need to know about COVID-19. Oral Oncol. 2020, 105, 104741. [Google Scholar] [CrossRef] [PubMed]
- CDC. COVID Data Tracker. Updated 2020 October 26. Available online: https://covid.cdc.gov/covid-data-tracker/#cases_totalcases (accessed on 26 October 2020).
- Hartnett, K.P.; Kite-Powell, A.; Devies, J.; Coletta, M.A.; Boehmer, T.K.; Adjemian, J.; Gundlapalli, A.V.; National Syndromic Surveillance Program Community of Practice. Impact of the COVID-19 Pandemic on Emergency Department Visits—United States, January 1, 2019–May 30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Carey, M.; American Dental Association (ADA). HPI Poll Examines Impact of COVID-19 on Dental Practices. ADA News. 1 April 2020. Available online: https://www.ada.org/en/publications/ada-news/2020-archive/april/hpi-poll-examines-impact-of-covid-19-on-dental-practices (accessed on 5 August 2020).
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics. Children and COVID-19: State-Level Data Report. Critical Updates on COVID-19. Updated 22 October 2020. Available online: https://services.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/ (accessed on 26 October 2020).
- Henry, B.M.; Benoit, S.W.; de Oliveira, M.H.S.; Hsieh, W.C.; Benoit, J.; Ballout, R.A.; Plebani, M.; Lippi, G. Laboratory abnormalities in children with mild and severe coronavirus disease 2019 (COVID-19): A pooled analysis and review. Clin. Biochem. 2020, 81, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Liao, B.; Cheng, L.; Peng, X.; Xu, X.; Li, Y.; Hu, T.; Li, J.; Zhou, X.; Ren, B. The microbial coinfection in COVID-19. Appl. Microbiol. Biotechnol. 2020, 104, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Netea, M.G.; Giamarellos-Bourboulis, E.J.; Domínguez-Andrés, J.; Curtis, N.; Van Crevel, R.; Van De Veerdonk, F.L.; Bonten, M. Trained Immunity: A Tool for Reducing Susceptibility to and the Severity of SARS-CoV-2 Infection. Cell 2020, 181, 969–977. [Google Scholar] [CrossRef] [PubMed]
- Brandão, T.B.; Gueiros, L.A.; Melo, T.S.; Prado-Ribeiro, A.C.; Nesrallah, A.C.F.A.; Prado, G.V.B.; Santos-Silva, A.R.; Migliorati, C.A. Oral lesions in patients with SARS-CoV-2 infection: Could the oral cavity be a target organ? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, e45–e51. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, J.A.; Normando, A.G.C.; Da Silva, R.L.C.; De Paula, R.M.; Cembranel, A.C.; Santos-Silva, A.R.; Guerra, E.N.S. Oral mucosal lesions in a COVID-19 patient: New signs or secondary manifestations? Int. J. Infect. Dis. 2020, 97, 326–328. [Google Scholar] [CrossRef] [PubMed]
- Behl, T.; Kaur, I.; Bungau, S.; Kumar, A.; Uddin, M.S.; Kumar, C.; Pal, G.; Shrivastava, K.; Zengin, G.; Arora, S. The dual impact of ACE2 in COVID-19 and ironical actions in geriatrics and pediatrics with possible therapeutic solutions. Life Sci. 2020, 257, 118075. [Google Scholar] [CrossRef] [PubMed]
- American Dental Association (ADA). COVID-19 State Mandates & Recommendations. Updated 8 August 2020. Available online: https://success.ada.org/en/practice-management/patients/covid-19-state-mandates-and-recommendations (accessed on 26 October 2020).
- Minnesota Department of Health. COVID-19 Aerosol-Generating Procedures and Patients with Suspected or Confirmed COVID-19. Updated 22 July 2020. Available online: https://www.health.state.mn.us/diseases/coronavirus/hcp/aerosol.pdf (accessed on 27 October 2020).
- Livingston, E.H.; Desai, A.; Berkwits, M. Sourcing Personal Protective Equipment during the COVID-19 Pandemic. JAMA 2020, 323, 1912–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamorro-Petronacci, C.; Carreras-Presas, C.M.; Sanz-Marchena, A.; A Rodríguez-Fernández, M.; Suárez-Quintanilla, J.M.; Rivas-Mundiña, B.; Suárez-Quintanilla, J.; Pérez-Sayáns, M. Assessment of the Economic and Health-Care Impact of COVID-19 (SARS-CoV-2) on Public and Private Dental Surgeries in Spain: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 5139. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Zhou, Y.; Liu, X.; Tan, J. The impact of the COVID-19 epidemic on the utilization of emergency dental services. J. Dent. Sci. 2020, 15, 564–567. [Google Scholar] [CrossRef] [PubMed]
- Ajeigbe, T.; Ria, B.; Wates, E.; Mattine, S. Severe parapharyngeal abscess that developed significant complications: Management during the COVID-19 pandemic. BMJ Case Rep. 2020, 13, e236449. [Google Scholar] [CrossRef] [PubMed]
- Taşlıdere, B.; Mehmetaj, L.; Özcan, A.B.; Gülen, B.; Taşlıdere, N. Melkersson-Rosenthal Syndrome Induced by COVID-19. Am. J. Emerg. Med. 2021, 41, 262.e5–262.e7. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fleagle, J.; Lorch, M. Facial Swelling in the Presence of a COVID-19 Diagnosis: Case Report. Oral 2021, 1, 102-107. https://doi.org/10.3390/oral1020010
Fleagle J, Lorch M. Facial Swelling in the Presence of a COVID-19 Diagnosis: Case Report. Oral. 2021; 1(2):102-107. https://doi.org/10.3390/oral1020010
Chicago/Turabian StyleFleagle, Jenelle, and Margarita Lorch. 2021. "Facial Swelling in the Presence of a COVID-19 Diagnosis: Case Report" Oral 1, no. 2: 102-107. https://doi.org/10.3390/oral1020010
APA StyleFleagle, J., & Lorch, M. (2021). Facial Swelling in the Presence of a COVID-19 Diagnosis: Case Report. Oral, 1(2), 102-107. https://doi.org/10.3390/oral1020010