
Influence of Cement Thickness on the Polymerization Shrinkage Stress of Adhesively Cemented Composite Inlays: Photoelastic and Finite Element Analysis

 , ,
, , 
Abstract
:1. Introduction
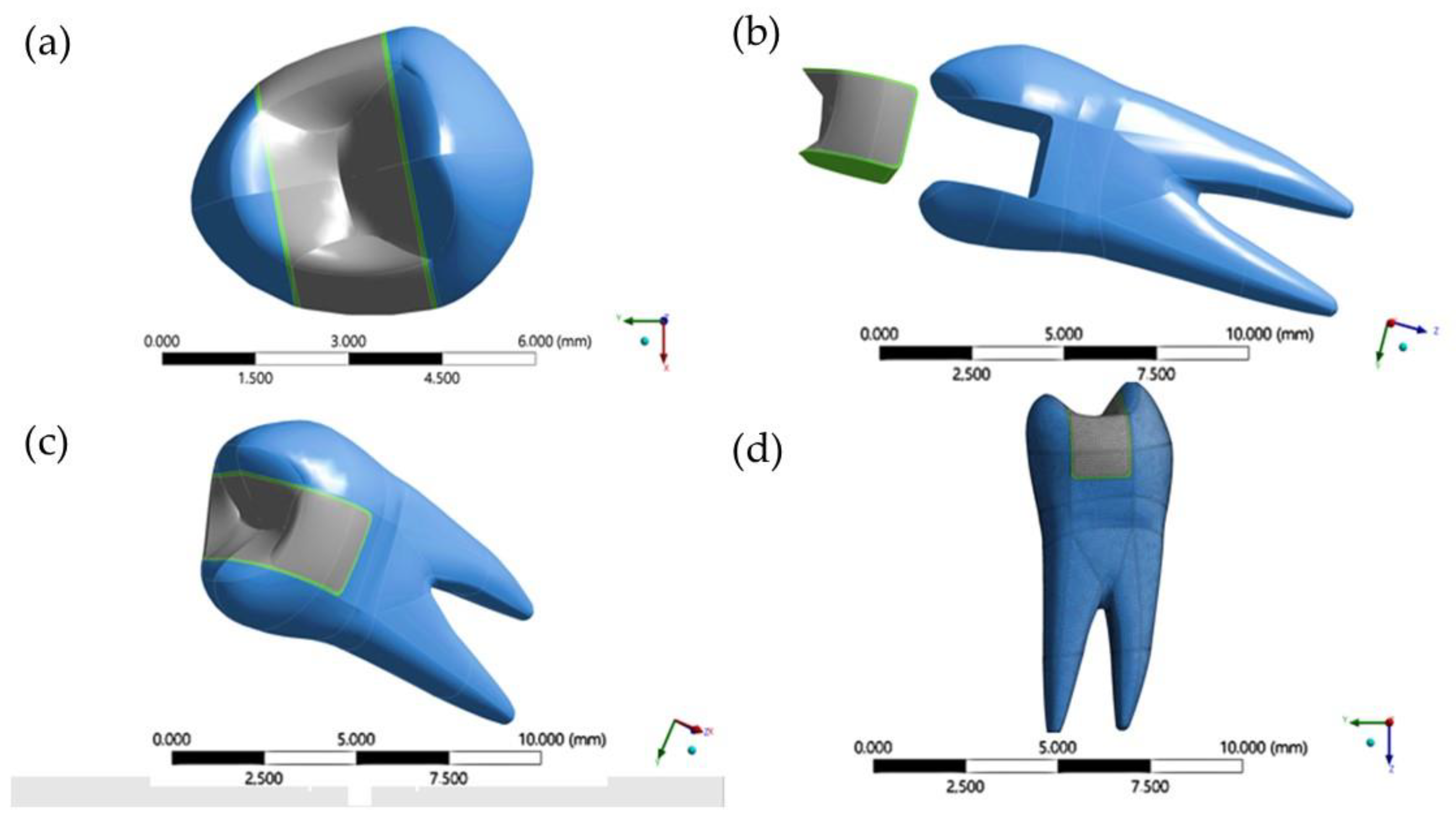
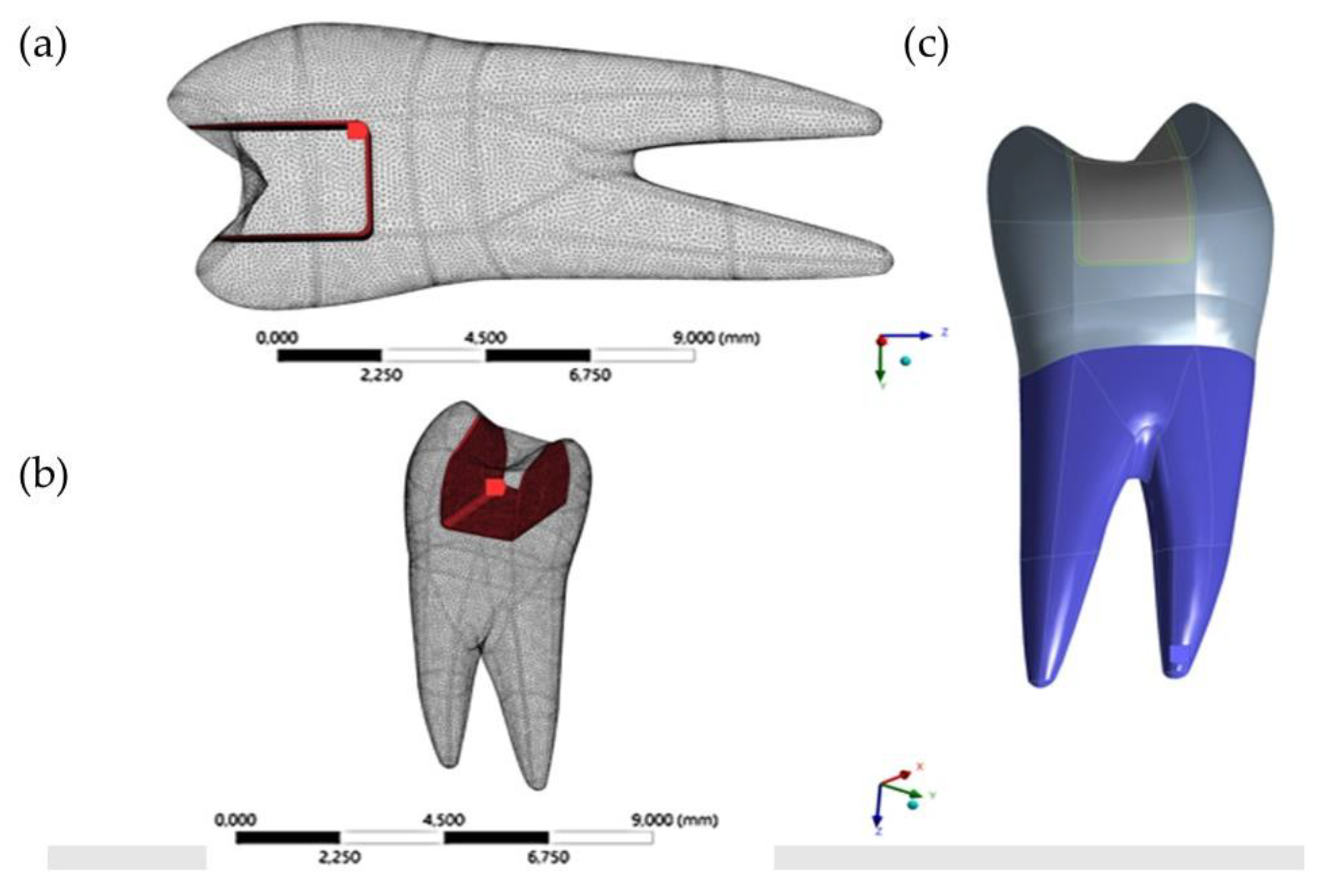
2. Materials and Methods
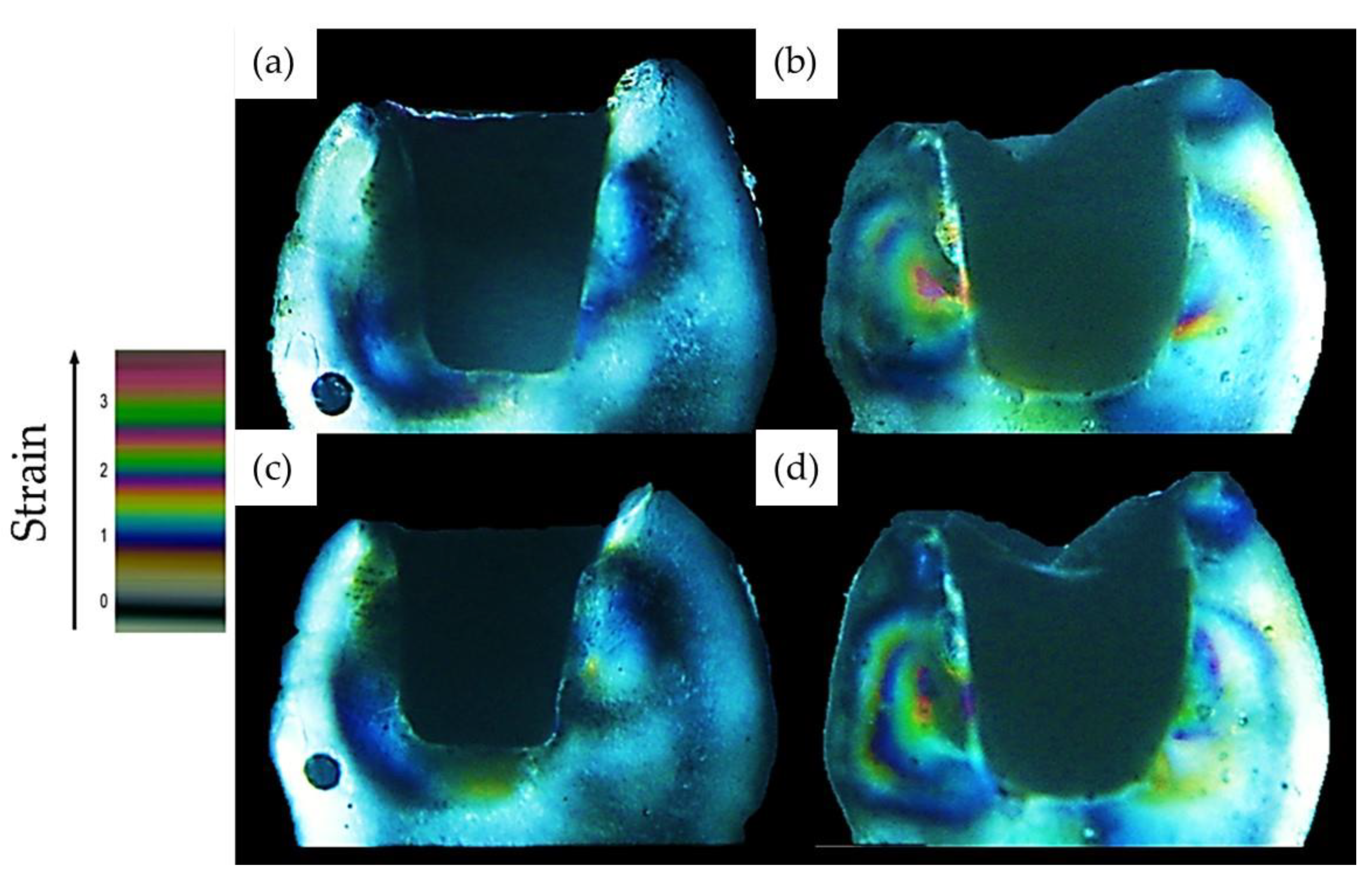
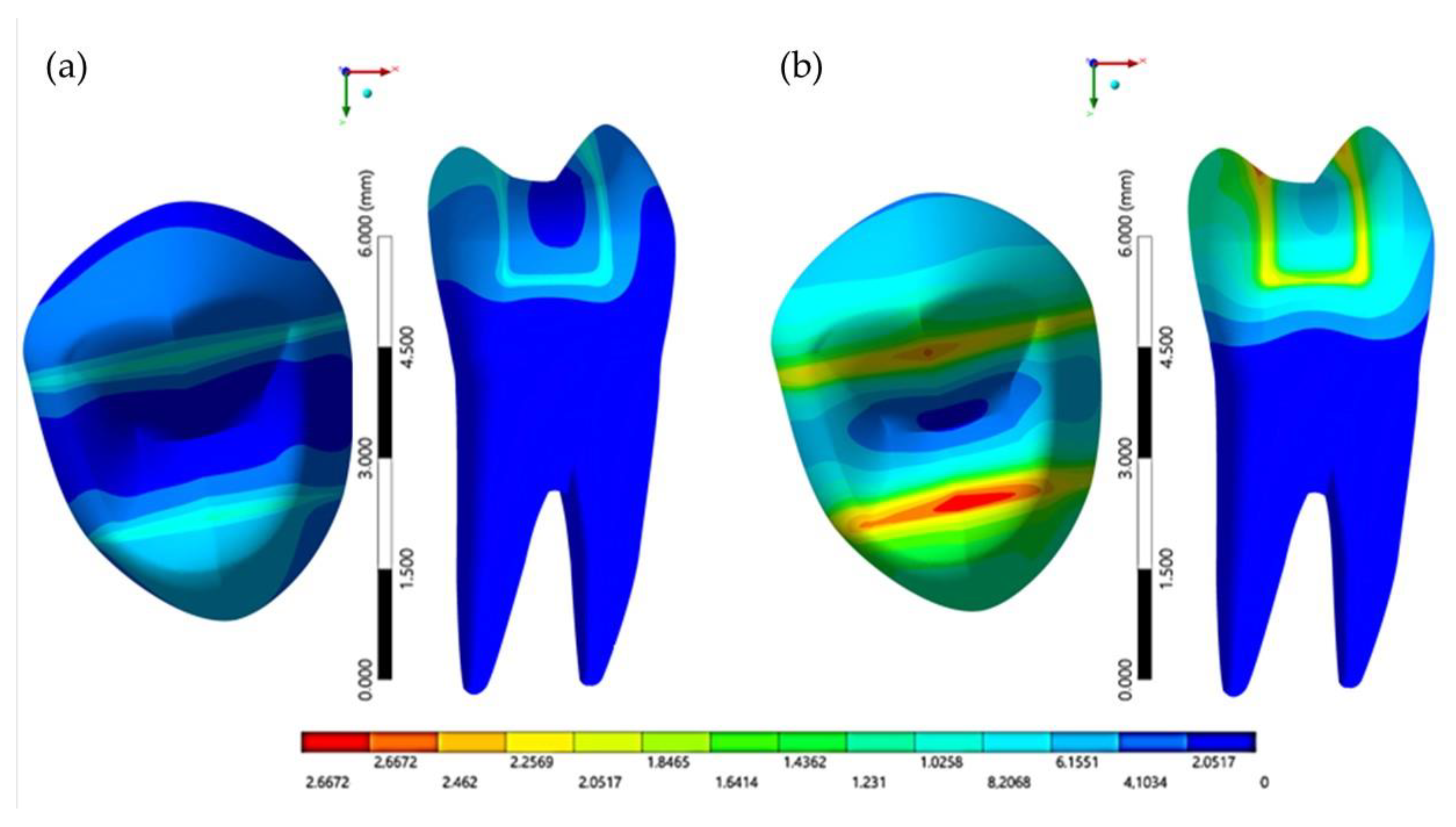
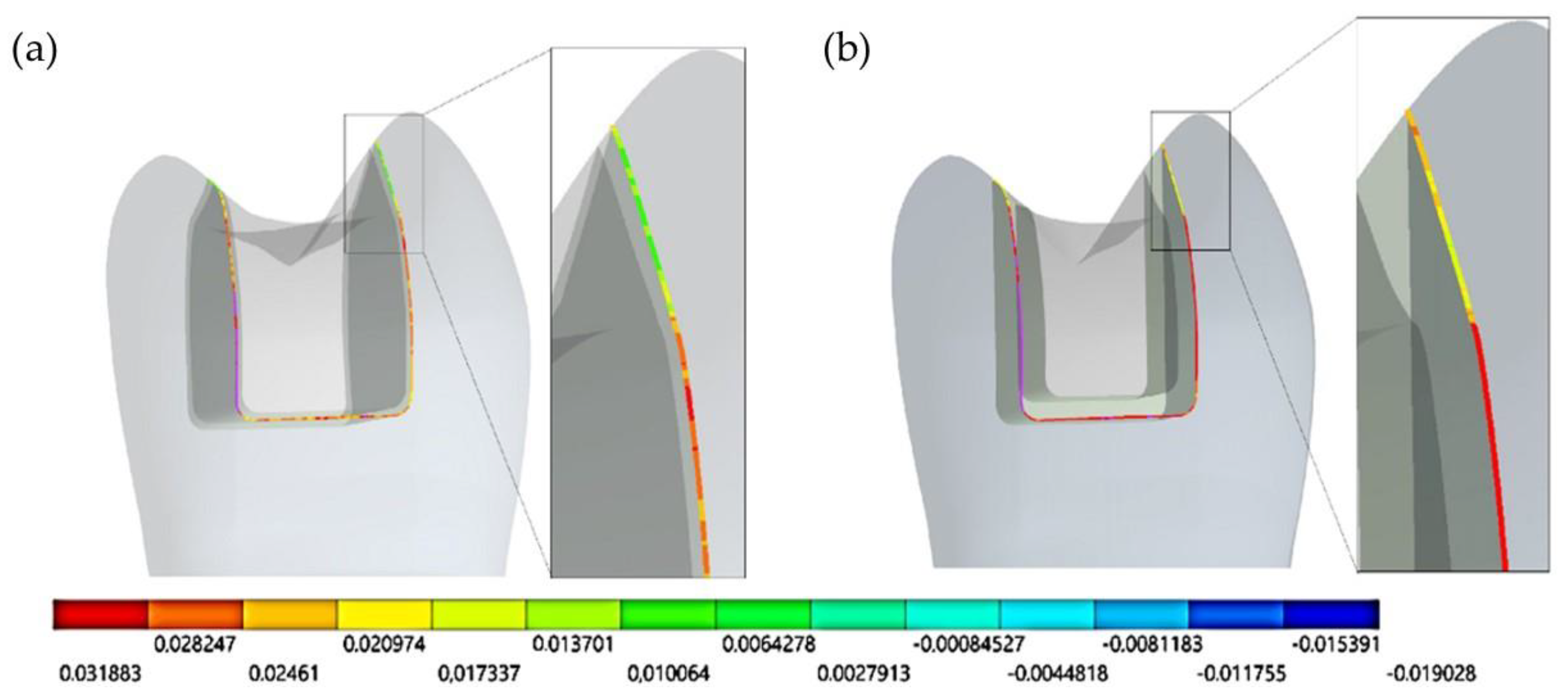
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Diaz-Arnold, A.M.; Vargas, M.A.; Haselton, D.R. Current status of luting agents for fixed prosthodontics. J. Prosthet. Dent. 1999, 81, 135–141. [Google Scholar] [CrossRef]
- de Matos, J.D.; Nakano, L.J.; Bottino, M.A.; de Jesus, R.H.; Maciel, L.C. Current considerations for dental ceramics and their respective union systems. Rev. Bras. Odontol. 2020, 77, e1768. [Google Scholar] [CrossRef]
- Menezes-Silva, R.; Velasco, S.R.; BRESCIANi, E.; Bastos, R.D.; Navarro, M.F. A prospective and randomized clinical trial evaluating the effectiveness of ART restorations with high-viscosity glass-ionomer cement versus conventional restorations with resin composite in Class II cavities of permanent teeth: Two-year follow-up. J. Appl. Oral Sci. 2021, 29, e20200609. [Google Scholar] [CrossRef]
- Ernst, C.P.; Meyer, G.R.; Klöcker, K.; Willershausen, B. Determination of polymerization shrinkage stress by means of a photoelastic investigation. Dent. Mater. 2004, 20, 313–321. [Google Scholar] [CrossRef]
- Charton, C.; Falk, V.; Marchal, P.; Pla, F.; Colon, P. Influence of Tg, viscosity and chemical structure of monomers on shrinkage stress in light-cured dimethacrylate-based dental resins. Dent. Mater. 2007, 23, 1447–1459. [Google Scholar] [CrossRef]
- Weinmann, W.; Thalacker, C.; Guggenberger, R. Siloranes in dental composites. Dent. Mater. 2005, 21, 68–74. [Google Scholar] [CrossRef]
- Feilzer, A.J.; De Gee, A.J.; Davidson, C.L. Increased wall-to-wall curing contraction in thin bonded resin layers. J. Dent. Res. 1989, 68, 48–50. [Google Scholar] [CrossRef]
- De Jager, N.; Pallav, P.; Feilzer, A.J. The influence of design parameters on the FEA-determined stress distribution in CAD-CAM produced all-ceramic dental crowns. Dent. Mater. 2005, 21, 242–251. [Google Scholar] [CrossRef]
- Ionescu, A.C.; Cazzaniga, G.; Ottobelli, M.; Ferracane, J.L.; Paolone, G.; Brambilla, E. In vitro biofilm formation on resin-based composites cured under different surface conditions. J. Dent. 2018, 77, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Ozyesil, A.G.; Usumez, A.; Gunduz, B. The efficiency of different light sources to polymerize composite beneath a simulated ceramic restauration. J. Prosthet. Dent. 2004, 91, 151–157. [Google Scholar] [CrossRef]
- Arrais, C.A.; Rueggeberg, F.A.; Waller, J.L.; de Goes, M.F.; Giannini, M. Effect of curing mode on the polymerization characteristics of dual-cured resin cement systems. J. Dent. 2008, 36, 418–426. [Google Scholar] [CrossRef]
- Marinho, M.L.; Strazzi-Sayhon, H.B.; Moraes, J.C.; Assunção, W.G.; Dos Santos, P.H. Degree of conversion of resin cements polymerized under different ceramic systems. Gen. Dent. 2020, 68, 44–49. [Google Scholar] [PubMed]
- Rullman, I.; Patyna, M.; Janssen, B.; Willershausen, B. Determination of polymerization shrinkage of different composites using a photoelastic method. Am. J. Dent. 2017, 30, 16–22. [Google Scholar] [PubMed]
- Rullmann, I.; Schattenberg, A.; Marx, M.; Willershausen, B.; Ernst, C.P. Photoelastic determination of polymerization shrinkage stress in low-shrinkage resin composites. Schweiz. Mon. Zahnmed. 2012, 122, 294–299. [Google Scholar]
- Schwertner, A.; Almeida, R.R.; Gonini, A., Jr.; Almeida, M.R. Photoelastic analysis of stress generated by Connecticut Intrusion Arch (CIA). Dent. Press J. Orthod. 2017, 22, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Kainose, K.; Nakajima, M.; Foxton, R.; Wakabayashi, N.; Tagami, J. Stress distribution in root filled teeth restored with various post and core techniques: Effect of post length and crown height. Int. Endod. J. 2015, 48, 1023–1032. [Google Scholar] [CrossRef]
- da Silva, J.V.; Martins, T.A.; Noritomi, P.Y. Scaffold informatics and biomimetic design: Three-dimensional medical reconstruction. Methods Mol. Biol. 2012, 868, 91–109. [Google Scholar] [PubMed]
- Kinomoto, Y.; Torii, M.; Takeshige, F.; Ebisu, S. Polymerization contraction stress of resin composite restorations in a model class I cavity configuration using photoelastic analysis. J. Esthet. Restor. Dent. 2000, 12, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Correia, A.; Andrade, M.R.; Tribst, J.; Borges, A.; Caneppele, T. Influence of bulk-fill restoration on polymerization shrinkage stress and marginal gap formation in Class V restorations. Oper. Dent. 2020, 45, E207–E216. [Google Scholar] [CrossRef] [PubMed]
- Versluis, A.; Tantbirojn, D.; Pintado, M.R.; DeLong, R.; Douglas, W.H. Residual shrinkage stress distributions in molars after composite restoration. Dent. Mater. 2004, 20, 554–564. [Google Scholar] [CrossRef]
- Borges, A.L.; Borges, A.B.; Xavier, T.A.; Bottino, M.C.; Platt, J.A. Impact of quantity of resin, C-factor, and geometry on resin composite polymerization shrinkage stress in Class V restorations. Oper. Dent. 2014, 39, 144–151. [Google Scholar] [CrossRef]
- Noritomi, P.; Xavier, T.; Silva, J. A comparison between BioCAD and some known methods for finite element model generation. In Innovative Developments in Virtual and Physical Prototyping; CRC Press: Boca Raton, FL, USA, 2011; pp. 685–690. ISBN 9780415684187. [Google Scholar]
- Campaner, L.M.; Silveira, M.P.; de Andrade, G.S.; Borges, A.L.; Bottino, M.A.; Dal Piva, A.M.; Lo Giudice, R.; Ausiello, P.; Tribst, J.P. Influence of polymeric restorative materials on the stress distribution in posterior fixed partial dentures: 3D finite element analysis. Polymers 2021, 13, 758. [Google Scholar] [CrossRef] [PubMed]
- de Andrade, G.S.; Pinto, A.B.; Tribst, J.P.; Chun, E.P.; Borges, A.L.; de Siqueira Ferreira Anzaloni Saavedra, G. Does overlay preparation design affect polymerization shrinkage stress distribution? A 3D FEA study. Comput. Methods Biomech. Biomed. Eng. 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ausiello, P.P.; Ciaramella, S.; Lanzotti, A.; Ventre, M.; Borges, A.L.; Tribst, J.P.; Dal Piva, A.; Garcia-Godoy, F. Mechanical behavior of Class I cavities restored by different material combinations under loading and polymerization shrinkage stress. A 3D-FEA study. Am. J. Dent. 2019, 32, 55–60. [Google Scholar] [PubMed]
- Scotti, N.; Coero Borga, F.A.; Alovisi, M.; Rota, R.; Pasqualini, D.; Berutti, E. Is fracture resistance of endodontically treated mandibular molars restored with indirect onlay composite restorations influenced by fibre post insertion? J. Dent. 2012, 40, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Kassis, C.; Khoury, P.; Mehanna, C.Z.; Baba, N.Z.; Bou Chebel, F.; Daou, M.; Hardan, L. Effect of Inlays, Onlays and Endocrown Cavity Design Preparation on Fracture Resistance and Fracture Mode of Endodontically Treated Teeth: An In Vitro Study. J. Prosthodont. 2020. [Google Scholar] [CrossRef]
- Abad-Coronel, C.; Naranjo, B.; Valdiviezo, P. Adhesive systems used in indirect restorations cementation: Review of the literature. Dent. J. 2019, 7, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collares, K.; Corrêa, M.B.; Laske, M.; Kramer, E.; Reiss, B.; Moraes, R.R.; Huysmans, M.C.; Opdam, N.J. A practice-based research network on the survival of ceramic inlay/onlay restorations. Dent. Mater. 2016, 32, 687–694. [Google Scholar] [CrossRef]
- D’Arcangelo, C.; Vanini, L.; Casinelli, M.; Frascaria, M.; De Angelis, F.; Vadini, M.; D’Amario, M. Adhesive cementation of indirect composite inlays and onlays: A literature review. Compend. Contin. Educ. Dent. 2015, 36, 570–577, quiz 578. [Google Scholar] [PubMed]
- Yoshihara, K.; Nagaoka, N.; Sonoda, A.; Maruo, Y.; Makita, Y.; Okihara, T.; Irie, M.; Yoshida, Y.; Van Meerbeek, B. Effectiveness and stability of silane coupling agent incorporated in ‘universal’ adhesives. Dent. Mater. 2016, 32, 1218–1225. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.Y.; Cho, G.Y.; Roh, B.D.; Shin, Y. Effect of curing mode on shear bond strength of self-adhesive cement to composite blocks. Materials 2016, 9, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dal Piva, A.M.; Tribst, J.P.; Jalkh, E.B.; Anami, L.C.; Bonfante, E.A.; Bottino, M.A. Minimal tooth preparation for posterior monolithic ceramic crowns: Effect on the mechanical behavior, reliability and translucency. Dent. Mater. 2021, 37, e140–e150. [Google Scholar] [CrossRef] [PubMed]
- Gomes de Carvalho, A.B.; de Andrade, G.S.; Mendes Tribst, J.P.; Grassi, E.D.; Ausiello, P.; Saavedra, G.D.; Bressane, A.; Marques de Melo, R.; Borges, A.L. Mechanical behavior of different restorative materials and onlay preparation designs in endodontically treated molars. Materials 2021, 14, 1923. [Google Scholar] [CrossRef] [PubMed]
- Ferracane, J.L.; Mitchem, J.C. Relationship between composite contraction stress and leakage in Class V cavities. Am. J. Dent. 2003, 16, 239–243. [Google Scholar] [PubMed]
- Kaisarly, D.; Gezawi, M.E. Polymerization shrinkage assessment of dental resin composites: A literature review. Odontology 2016, 104, 257–270. [Google Scholar] [CrossRef]
- da Rosa, H.C.; Marcondes, M.L.; de Souza, N.C.; Weber, J.B.; Spohr, A.M. Do resin cements influence the cuspal deflection of teeth restored with composite resin inlays? Acta Odontol. Latinoam. 2015, 28, 28–34. [Google Scholar]
- Salaverry, A.; Borges, G.A.; Mota, E.G.; Burnett Júnior, L.H.; Spohr, A.M. Effect of resin cements and aging on cuspal deflection and fracture resistance of teeth restored with composite resin inlays. J. Adhe. Dent. 2013, 15, 561–568. [Google Scholar]
- Dall Agnol, R.J.; Ghiggi, P.C.; Paranhos, M.P.; Borges, G.A.; Burnett, L.H., Jr.; Spohr, A.M. Influence of resin cements on cuspal deflection and fracture load of endodontically-treated teeth restored with composite inlays. Acta Odontol. Scand. 2013, 71, 664–670. [Google Scholar] [CrossRef]
- Sokolowski, G.; Krasowski, M.; Szczesio-Wlodarczyk, A.; Konieczny, B.; Sokolowski, J.; Bociong, K. The influence of cement layer thickness on the stress state of metal inlay restorations-photoelastic analysis. Materials 2021, 14, 599. [Google Scholar] [CrossRef]
- Braga, R.R.; Boaro, L.C.; Kuroe, T.; Azevedo, C.L.; Singer, J.M. Influence of cavity dimensions and their derivatives (volume and “C” factor) on shrinkage stress development and microleakage of composite restorations. Dent. Mater. 2006, 22, 818–823. [Google Scholar] [CrossRef]
- Hayashi, J.; Shimada, Y.; Tagami, J.; Sumi, Y.; Sadr, A. Real-time imaging of gap progress during and after composite polymerization. J. Dent. Res. 2017, 96, 992–998. [Google Scholar] [CrossRef]
- Ilie, N.; Jelen, E.; Clementino-Luedemann, T.; Hickel, R. Low-shrinkage composite for dental application. Dent. Mater. J. 2007, 26, 149–155. [Google Scholar] [CrossRef] [Green Version]
- Watts, D.C.; Satterthwaite, J.D. Axial shrinkage-stress depends upon both C-factor and composite mass. Dent. Mater. 2008, 24, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Craig, R.G.; el-Ebrashi, M.K.; LePeak, P.J.; Peyton, F.A. Experimental stress analysis of dental restorations. I. Two-dimensional photoelastic stress analysis of inlays. J. Prosthet. Dent. 1967, 17, 277–291. [Google Scholar] [CrossRef]
- Feilzer, A.J.; De Gee, A.J.; Davidson, C.L. Setting stress in composite resin in relation to configuration of the restoration. J. Dent. Res. 1987, 66, 1636–1639. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, R.; Powers, J. Restorative Materials. In Craig’s Restorative Dental Materials; Elsevier: Amsterdam, The Netherlands, 2019; pp. 135–170. ISBN 9780323478212. [Google Scholar]
- Rodrigues, F.P.; Silikas, N.; Watts, D.C.; Ballester, R.Y. Finite element analysis of bonded model Class I “restorations” after shrinkage. Dent. Mater. 2012, 28, 123–132. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Correia, A.M.; Tribst, J.P.; de Souza Matos, F.; Platt, J.A.; Caneppele, T.M.; Borges, A.L. Polymerization shrinkage stresses in different restorative techniques for non-carious cervical lesions. J. Dent. 2018, 76, 68–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tribst, J.P.; Dal Piva, A.M.; de Melo, R.M.; Borges, A.L.; Bottino, M.A.; Özcan, M. Short communication: Influence of restorative material and cement on the stress distribution of posterior resin-bonded fixed dental prostheses: 3D finite element analysis. J. Mech. Behav. Biomed. Mater. 2019, 96, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Kaisarly, D.; El Gezawi, M.; Nyamaa, I.; Rösch, P.; Kunzelmann, K.H. Effects of boundary condition on shrinkage vectors of a flowable composite in experimental cavity models made of dental substrates. Clin. Oral Investig. 2019, 23, 2403–2411. [Google Scholar] [CrossRef]
- Dal Piva, A.O.; Tribst, J.P.; Borges, A.L.; de Melo, R.M.; Bottino, M.A. Influence of substrate design for in vitro mechanical testing. J. Clin. Exp. Dent. 2019, 11, e119–e125. [Google Scholar] [CrossRef]
- Benazzi, S.; Nguyen, H.N.; Kullmer, O.; Hublin, J.J. Exploring the bio mechanics of taurodontism. J. Anat. 2015, 226, 180–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Harbi, F.; Kaisarly, D.; Bader, D.; El Gezawi, M. Marginal integrity of bulk versus incremental fill class II composite restorations. Oper. Dent. 2016, 41, 146–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Li, H.; Fok, S.L. A mathematical analysis of shrinkage stress development in dental composite restorations during resin polymerization. Dent. Mater. 2008, 24, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Tribst, J.P.; Dal Piva, A.M.; Ausiello, P.; Kalman, L. Influence of implant-abutment contact surfaces and prosthetic screw tightening on the stress concentration, fatigue life and microgap formation: A finite element analysis. Oral 2021, 1, 88–101. [Google Scholar] [CrossRef]
- Yeo, H.W.; Loo, M.Y.; Alkhabaz, M.; Li, K.C.; Choi, J.J.; Barazanchi, A. Bulk-fill direct restorative materials: An in vitro assessment of their physio-mechanical properties. Oral 2021, 1, 75–87. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Young’s Modulus (GPa) | Poisson’s Ratio | Volumetric Shrinkage (%) | References |
|---|---|---|---|---|
| Dentin | 18.0 | 0.23 | - | [18] |
| Enamel | 80.0 | 0.30 | - | [18] |
| Cement layer | 7.0 | 0.24 | 1.74 | [19] |
| Composite resin | 20 | 0.20 | - | [20] |
| Result | Cement Layer Model | |
|---|---|---|
| 100 μm | 400 μm | |
| Cusp displacement (mm) | 0.000107 | 0.00026 |
| Tooth stress (MPa) | 0.210 | 0.305 |
| Cement stress (MPa) | 0.261 | 0.270 |
| Restoration stress (MPa) | 0.203 | 0.270 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campaner, L.M.; Alves Pinto, A.B.; Demachkia, A.M.; Paes-Junior, T.J.d.A.; Pagani, C.; Borges, A.L.S. Influence of Cement Thickness on the Polymerization Shrinkage Stress of Adhesively Cemented Composite Inlays: Photoelastic and Finite Element Analysis. Oral 2021, 1, 168-180. https://doi.org/10.3390/oral1020017
Campaner LM, Alves Pinto AB, Demachkia AM, Paes-Junior TJdA, Pagani C, Borges ALS. Influence of Cement Thickness on the Polymerization Shrinkage Stress of Adhesively Cemented Composite Inlays: Photoelastic and Finite Element Analysis. Oral. 2021; 1(2):168-180. https://doi.org/10.3390/oral1020017
Chicago/Turabian StyleCampaner, Larissa Mendes, Alana Barbosa Alves Pinto, Amir Mohidin Demachkia, Tarcísio José de Arruda Paes-Junior, Clóvis Pagani, and Alexandre Luiz Souto Borges. 2021. "Influence of Cement Thickness on the Polymerization Shrinkage Stress of Adhesively Cemented Composite Inlays: Photoelastic and Finite Element Analysis" Oral 1, no. 2: 168-180. https://doi.org/10.3390/oral1020017
APA StyleCampaner, L. M., Alves Pinto, A. B., Demachkia, A. M., Paes-Junior, T. J. d. A., Pagani, C., & Borges, A. L. S. (2021). Influence of Cement Thickness on the Polymerization Shrinkage Stress of Adhesively Cemented Composite Inlays: Photoelastic and Finite Element Analysis. Oral, 1(2), 168-180. https://doi.org/10.3390/oral1020017