
Oral Squamous Cell Carcinoma Mimicking Medication-Related Osteonecrosis of the Jaws (MRONJ): A Case Series

 ,
, 
 , and
, and 
Abstract
:1. Introduction
2. Case Presentation
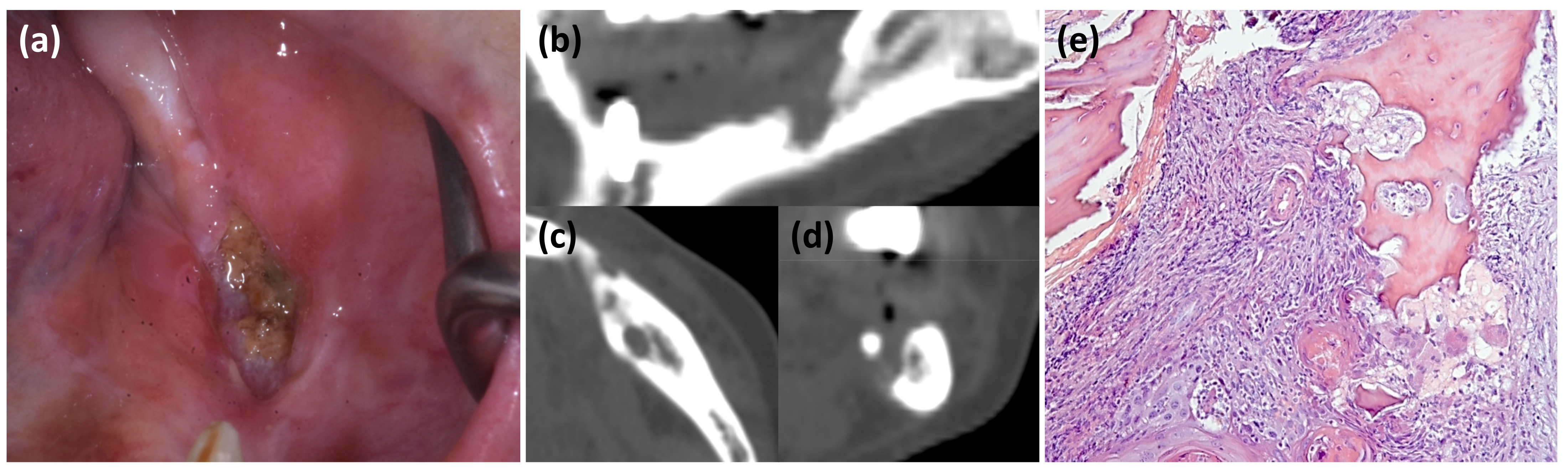
2.1. Clinical Case 1
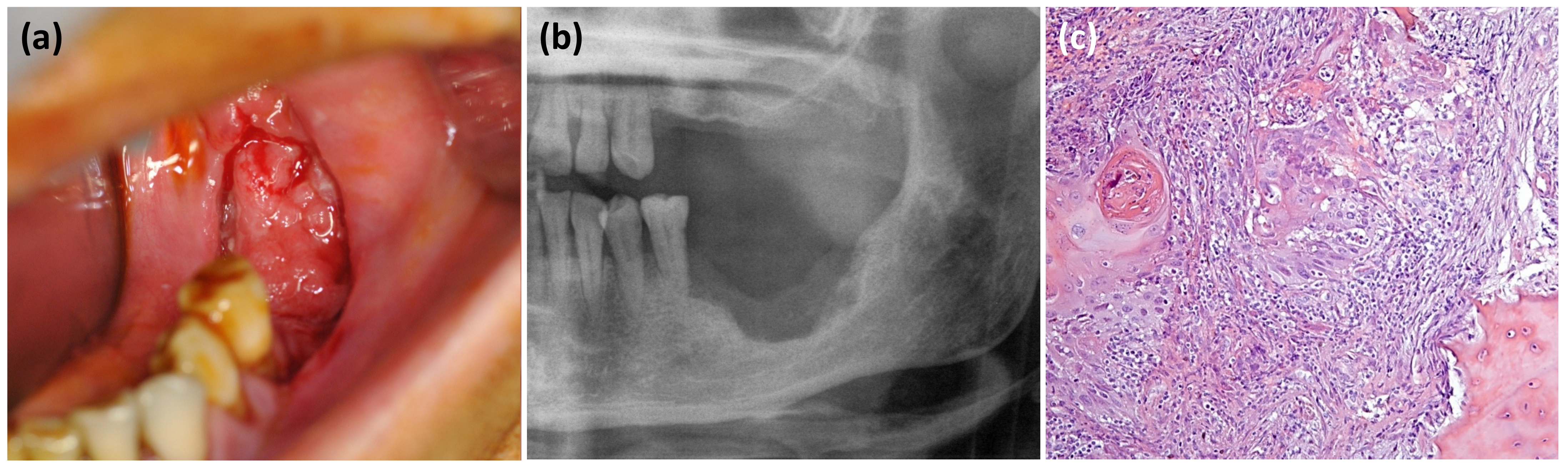
2.2. Clinical Case 2
2.3. Clinical Case 3
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bedogni, A.; Campisi, G.; Fusco, V. Medication Related Osteonecrosis of the Jaw (MRONJ); Qeios: London, UK, 2018. [Google Scholar]
- Campisi, G.; Mauceri, R.; Bertoldo, F.; Bettini, G.; Biasotto, M.; Colella, G.; Consolo, U.; Di Fede, O.; Favia, G.; Fusco, V.; et al. Medication-related osteonecrosis of jaws (MRONJ) prevention and diagnosis: Italian consensus update 2020. Int. J. Environ. Res. Public Health 2020, 17, 5998. [Google Scholar] [CrossRef]
- Campisi, G.; Bedogni, A.; Fusco, V. Raccomandazioni Clinico-Terapeutiche Sull’osteonecrosi Delle Ossa Mascellari (ONJ) Farmaco-Relata E Sua Prevenzione; Srl, N.D.F., Ed.; Palermo University Press: Palermo, Italy, 2020; ISBN 978-88-5509-148-0. [Google Scholar]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw—2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef] [PubMed]
- Campisi, G.; Fedele, S.; Fusco, V.; Pizzo, G.; Di Fede, O.; Bedogni, A. Epidemiology, clinical manifestations, risk reduction and treatment strategies of jaw osteonecrosis in cancer patients exposed to antiresorptive agents. Futur. Oncol. 2014, 10, 257–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bedogni, A.; Saia, G.; Ragazzo, M.; Bettini, G.; Capelli, P.; D’Alessandro, E.; Nocini, P.F.; Lo Russo, L.; Lo Muzio, L.; Blandamura, S. Bisphosphonate-associated osteonecrosis can hide jaw metastases. Bone 2007, 41, 942–945. [Google Scholar] [CrossRef] [PubMed]
- Gander, T.; Obwegeser, J.A.; Zemann, W.; Grätz, K.W.; Jacobsen, C. Malignancy mimicking bisphosphonate-associated osteonecrosis of the jaw: A case series and literature review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Tocaciu, S.; Breik, O.; Lim, B.; Angel, C.; Rutherford, N. Diagnostic dilemma between medication-related osteonecrosis and oral squamous cell carcinoma in a mandibular lytic lesion. Br. J. Oral Maxillofac. Surg. 2017, 55, e53–e57. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: A growing epidemic. J. Oral Maxillofac. Surg. 2003, 61, 1115–1117. [Google Scholar] [CrossRef]
- Yarom, N.; Shapiro, C.L.; Peterson, D.E.; Van Poznak, C.H.; Bohlke, K.; Ruggiero, S.L.; Migliorati, C.A.; Khan, A.; Morrison, A.; Anderson, H.; et al. Medication-related osteonecrosis of the jaw: MASCC/ISOO/ASCO clinical practice guideline. J. Clin. Oncol. 2019, 37, 2270–2290. [Google Scholar] [CrossRef] [PubMed]
- Fusco, V.; Santini, D.; Armento, G.; Tonini, G.; Campisi, G. Osteonecrosis of jaw beyond antiresorptive (bone-targeted) agents: New horizons in oncology. Expert Opin. Drug Saf. 2016, 15, 925–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedele, S.; Bedogni, G.; Scoletta, M.; Favia, G.; Colella, G.; Agrillo, A.; Bettini, G.; Di Fede, O.; Oteri, G.; Fusco, V.; et al. Up to a quarter of patients with osteonecrosis of the jaw associated with antiresorptive agents remain undiagnosed. Br. J. Oral Maxillofac. Surg. 2015, 53, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Arduino, P.G.; Scully, C.; Chiusa, L.; Broccoletti, R. Oral squamous cell carcinoma arising in a patient after hematopoietic stem cell transplantation with bisphosphonate-related osteonecrosis of the jaws. Case Rep. Dent. 2015, 2015, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Terenzi, V.; Cassoni, A.; Coiante, E.; Spadoni, D.; Della Rocca, C.; Pernazza, A.; Valentini, V. The possible contemporary presence of BRONJ and oral squamous cell carcinoma. Oral Oncol. 2018, 83, 160–161. [Google Scholar] [CrossRef] [PubMed]
- Carlson, E.R.; Fleisher, K.E.; Ruggiero, S.L. Metastatic cancer identified in osteonecrosis specimens of the jaws in patients receiving intravenous bisphosphonate medications. J. Oral Maxillofac. Surg. 2013, 71, 2077–2086. [Google Scholar] [CrossRef] [PubMed]
- Scully, C.; Bagan, J.V.; Hopper, C.; Epstein, J.B. Oral cancer: Current and future diagnostic techniques. Am. J. Dent. 2008, 21, 199–209. [Google Scholar] [PubMed]
- Carreras-Torras, C.; Gay-Escoda, C. Techniques for early diagnosis of oral squamous cell carcinoma: Systematic review. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e305–e315. [Google Scholar] [CrossRef] [PubMed]
- Cristaldi, M.; Mauceri, R.; Di Fede, O.; Giuliana, G.; Campisi, G.; Panzarella, V. Salivary Biomarkers for Oral Squamous Cell Carcinoma Diagnosis and Follow-Up: Current Status and Perspectives; Frontiers Media S.A.: Lausanne, Switzerland, 2019; Volume 10. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Shared Clinical Criteria | Unshared Clinical Criteria | |
|---|---|---|
| MRONJ |
|
|
| OSCC |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mauceri, R.; Toro, C.; Panzarella, V.; Iurato Carbone, M.; Rodolico, V.; Campisi, G. Oral Squamous Cell Carcinoma Mimicking Medication-Related Osteonecrosis of the Jaws (MRONJ): A Case Series. Oral 2021, 1, 326-331. https://doi.org/10.3390/oral1040032
Mauceri R, Toro C, Panzarella V, Iurato Carbone M, Rodolico V, Campisi G. Oral Squamous Cell Carcinoma Mimicking Medication-Related Osteonecrosis of the Jaws (MRONJ): A Case Series. Oral. 2021; 1(4):326-331. https://doi.org/10.3390/oral1040032
Chicago/Turabian StyleMauceri, Rodolfo, Corrado Toro, Vera Panzarella, Martina Iurato Carbone, Vito Rodolico, and Giuseppina Campisi. 2021. "Oral Squamous Cell Carcinoma Mimicking Medication-Related Osteonecrosis of the Jaws (MRONJ): A Case Series" Oral 1, no. 4: 326-331. https://doi.org/10.3390/oral1040032
APA StyleMauceri, R., Toro, C., Panzarella, V., Iurato Carbone, M., Rodolico, V., & Campisi, G. (2021). Oral Squamous Cell Carcinoma Mimicking Medication-Related Osteonecrosis of the Jaws (MRONJ): A Case Series. Oral, 1(4), 326-331. https://doi.org/10.3390/oral1040032