
Microbiology of Maxillary Sinus Infections: Systematic Review on the Relationship of Infectious Sinus Pathology with Oral Pathology



Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Isolated Micro-Organisms
2.5. Selection of Studies
2.6. Statistical Analysis
3. Results
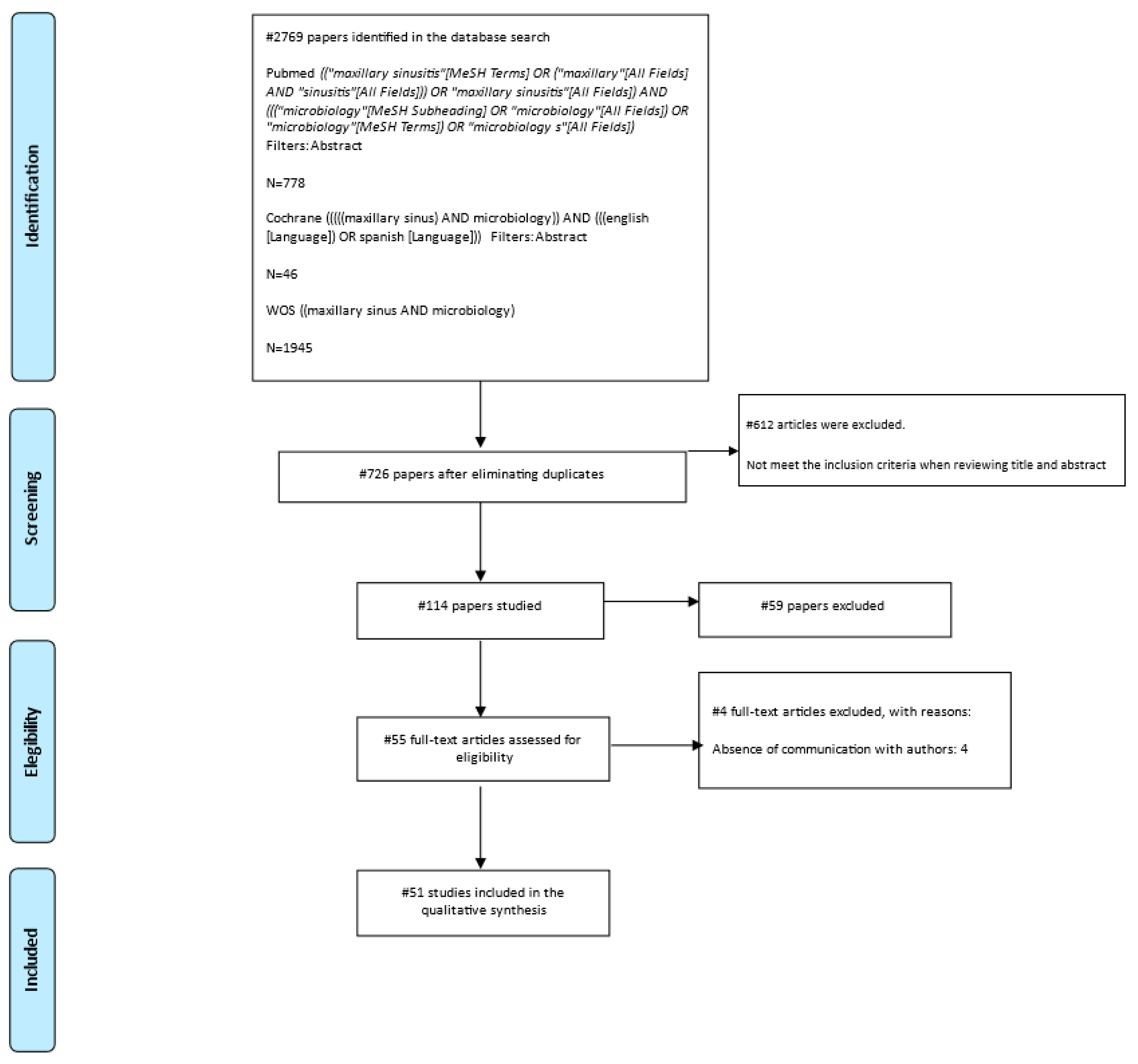
3.1. Study Selection and Characteristics
3.2. Results of Individual Studies
Isolated Micro-Organisms
4. Discussion
4.1. Limitations
4.2. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, N.A.; Ferguson, B.J. Odontogenic sinusitis: An ancient but under-appreciated cause of maxillary sinusitis. Curr. Opin. Otolaryngol. Head Neck Surg. 2012, 20, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Heider, C.C.; Ribalta, L.G.; Bacigalupe, R.D.; Krauss, K.M. Rinosinusitis maxilar crónica de origen dental. Rev. Otorrinolaringol. Cirugía Cabeza Cuello 2014, 74, 12–20. [Google Scholar] [CrossRef] [Green Version]
- Kretzschmar, D.P.; Kretzschmar, C.J.L. Rhinosinusitis: Review from a dental perspective. Oral Surgery Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2003, 96, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Novoa, R.R.; Sepúlveda, A.I.; Munzenmayer, B.J.; Schmidt, T. Resultados clínicos e imagenológicos en pacientes con rinosinusitis crónica odontogénica. Rev. Otorrinolaringol. Cirugía Cabeza Cuello 2020, 80, 147–156. [Google Scholar] [CrossRef]
- Mehra, P.; Jeong, D. Maxillary Sinusitis of Odontogenic Origin. Curr. Allergy Asthma Rep. 2009, 9, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Guzmán-Romero, A.K.; Macías-Fernández, B. Rinosinusitis odontogénica: Abordaje actual y comunicación de un caso Odontogenic rhinosi-nusitis: Current approach and a case report. An. Otorrinolaringol. Mex. 2017, 62, 55–64. [Google Scholar]
- Little, R.E.; Long, C.M.; Loehrl, T.A.; Poetker, D.M. Odontogenic sinusitis: A review of the current literature. Laryngoscope Investig. Otolaryngol. 2018, 3, 110–114. [Google Scholar] [CrossRef]
- Bischhoffshausen, K.V.; Teuber, C.; Tapia, S.; Callejas, C.; Ramírez, H.; Vargas, A. Diagnóstico y tratamiento de la sinusitis maxilar odontogénica. Rev. Otorrinolaringol. Cirugía Cabeza Cuello 2019, 79, 357–365. [Google Scholar] [CrossRef]
- Escapa, I.F.; Chen, T.; Huang, Y.; Gajare, P.; Dewhirst, F.E.; Lemon, K.P. New Insights into Human Nostril Microbiome from the Expanded Human Oral Microbiome Database (eHOMD): A Resource for the Microbiome of the Human Aerodigestive Tract. Msystems 2018, 3, e00187-18. [Google Scholar] [CrossRef] [Green Version]
- Drettner, B.; Lindholm, C.-E. The Borderline between Acute Rhinitis and Sinusitis. Acta Oto-Laryngol. 1967, 64, 508–513. [Google Scholar] [CrossRef]
- Berg, O.; Bergstedt, H.; Carenfelt, C.; Lind, M.G.; Perols, O. Discrimination of purulent from nonpurulent maxillary sinusitis: Clinical and radio-graphic diagnosis. Ann. Otol. Rhinol. Laryngol. 1981, 90, 272–275. [Google Scholar] [CrossRef]
- Carenfelt, C.; Lundberg, C.; Nord, C.E.; Wretlind, B. Bacteriology of Maxillary Sinusitis in Relation to Quality of the Retained Secretion. Acta Otolaryngol. 1978, 86, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Brook, I. The role of anaerobic bacteria in sinusitis. Anaerobe 2006, 12, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalcioglu, M.T.; Durmaz, B.; Aktaş, E.; Ozturan, O.; Durmaz, R. Bacteriology of Chronic Maxillary Sinusitis and Normal Maxillary Sinuses: Using Culture and Multiplex Polymerase Chain Reaction. Am. J. Rhinol. 2003, 17, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Greval, R.S.; Khurana, S.; Shobha, R.; Sharma, S.K. Anaerobic infection in chronic maxillary sinusitis. Indian J. Med. Sci. 1993, 47, 201–203. [Google Scholar]
- Penttilä, M.; Savolainen, S.; Kiukaanniemi, H.; Forsblom, B.; Jousimies-Somer, H. Bacterial findings in acute maxillary sinusitis-European study. Acta Otolaryngol. Suppl. 1997, 117, 165–168. [Google Scholar] [CrossRef]
- Hoyt, W.H., III. Bacterial patterns found in surgery patients with chronic sinusitis. J. Am. Osteopath. Assoc. 1992, 92, 205, 209–212. [Google Scholar] [CrossRef]
- Puglisi, S.; Privitera, S.; Maiolino, L.; Serra, A.; Garotta, M.; Blandino, G.; Speciale, A. Bacteriological findings and antimicrobial resistance in odontogenic and non-odontogenic chronic maxillary sinusitis. J. Med. Microbiol. 2011, 60, 1353–1359. [Google Scholar] [CrossRef]
- Brook, I. Microbiology of Acute Sinusitis of Odontogenic Origin Presenting with Periorbital Cellulitis in Children. Ann. Otol. Rhinol. Laryngol. 2007, 116, 386–388. [Google Scholar] [CrossRef]
- Brook, I. Microbiology of Acute and Chronic Maxillary Sinusitis Associated with an Odontogenic Origin. Laryngoscope 2005, 115, 823–825. [Google Scholar] [CrossRef] [Green Version]
- Zirk, M.; Dreiseidler, T.; Pohl, M.; Rothamel, D.; Buller, J.; Peters, F.; Zöller, J.E.; Kreppel, M. Odontogenic sinusitis maxillaris: A retrospective study of 121 cases with surgical inter-vention. J. Cranio-Maxillofac. Surg. 2017, 45, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Brook, I.; Hausfeld, J.N. Microbiology of Acute and Chronic Maxillary Sinusitis in Smokers and Nonsmokers. Ann. Otol. Rhinol. Laryngol. 2011, 120, 707–712. [Google Scholar] [CrossRef]
- Varzhapetian, S.; Makarenko, O.; Sydoryako, A.; Baleha, M.; Bunyatyan, K. Aerobic Microflora in the Pathogenesis of Maxillary Sinusitis after the Treatment of Caries Complications. Georgian Med. News 2019, 42–46. [Google Scholar]
- Moungthong, G.; Suwas, A.; Jaruchida, S.; Chantaratchada, S.; Phonphok, Y.; Rangsin, R. Prevalence of etiologic bacteria and be-ta-lactamase-producing bacteria in acute and chronic maxillary sinusitis at Phramongkutklao Hospital. J. Med. Assoc. Thai 2005, 88, 478–483. [Google Scholar]
- Brook, I.; Foote, P.A.; Hausfeld, J.N. Increase in the frequency of recovery of meticillin-resistant Staphylococcus aureus in acute and chronic maxillary sinusitis. J. Med. Microbiol. 2008, 57, 1015–1017. [Google Scholar] [CrossRef] [PubMed]
- Ivanchenko, O.A.; Karpishchenko, S.A.; Kozlov, R.S.; Krechikova, O.I.; Otvagin, I.V.; Sopko, O.N.; Piskunov, G.Z.; Lopatin, A.S. The microbiome of the maxillary sinus and middle nasal meatus in chronic rhinosinusitis. Rhinology 2016, 54, 68–74. [Google Scholar] [CrossRef]
- Nigro, J.F.; Nigro, C.E.; Marone, S.A.; Voegels, R.L. Microbiology of the maxillary and ethmoid sinuses in patients with chronic rhi-nosinusitis submitted to functional endoscopic sinus surgery. Braz. J. Otorhinolaryngol. 2006, 72, 217–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartog, B.; Degener, J.E.; van Benthem, P.P.G.; Hordijk, G.J. Microbiology of Chronic Maxillary Sinusitis in Adults: Isolated Aerobic and Anaerobic Bacteria and their Susceptibility to Twenty Antibiotics. Acta Otolaryngol. 1995, 115, 672–677. [Google Scholar] [CrossRef]
- Zurak, K.; Vagić, D.; Drvis, P.; Potocnik, C.P.; Dzidic, S.; Kalogjera, L. Bacterial colonization and granulocyte activation in chronic maxillary sinusitis in asthmatics and non-asthmatics. J. Med. Microbiol. 2009, 58, 1231–1235. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, K.; Yoo, J.-B.; Song, J.-W.; Yoon, J.-H. Bacteriological findings and antimicrobial susceptibility in chronic sinusitis with nasal polyp. Acta Otolaryngol. 2006, 126, 489–497. [Google Scholar] [CrossRef]
- Mantovani, K.; Bisanha, A.A.; Demarco, R.C.; Tamashiro, E.; Martinez, R.; Anselmo-Lima, W.T. Maxillary sinuses microbiology from patients with chronic rhinosinusitis. Braz. J. Otorhinolaryngol. 2010, 76, 548–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joniau, S.; Vlaminck, S.; Van Landuyt, H.; Kuhweide, R.; Dick, C. Microbiology of Sinus Puncture versus Middle Meatal Aspiration in Acute Bacterial Maxillary Sinusitis. Am. J. Rhinol. 2005, 19, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Jiang, R.-S.; Hsu, C.-Y.; Jang, J.-W. Bacteriology of the maxillary and ethmoid sinuses in chronic sinusitis. J. Laryngol. Otol. 1998, 112, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Almadori, G.; Bastianini, L.; Bistoni, F.; Maurizi, M.; Ottaviani, F.; Paludetti, G.; Scuteri, F. Microbial flora of nose and paranasal sinuses in chronic maxillary sinusitis. Rhinology 1986, 24, 257–264. [Google Scholar]
- Antila, J.; Suonpää, J.; Lehtonen, O.P. Bacteriological evaluation of 194 adult patients with acute frontal sinusitis and findings of simultaneous maxillary sinusitis. Acta Otolaryngol. Suppl. 1997, 529, 162–164. [Google Scholar] [CrossRef]
- Kamau, J.K.; Macharia, I.M.; Odhiambo, P.A. Bacteriology of chronic maxillary sinusitis at Kenyatta National Hospital, Nairobi. East Afr. Med. J. 2001, 78, 343–345. [Google Scholar] [CrossRef] [Green Version]
- Jiang, R.-S.; Lin, J.-F.; Hsu, C.-Y. Bacteriology of Chronic Maxillary Sinusitis in Relation to Sinoscopic Appearance. Am. J. Rhinol. 2002, 16, 249–253. [Google Scholar] [CrossRef]
- Şener, B.; Hasçelik, G.; Önerci, M.; Tunçkanat, F. Evaluation of the microbiology of chronic sinusitis. J. Laryngol. Otol. 1996, 110, 547–550. [Google Scholar] [CrossRef]
- Hamory, B.H.; Sande, M.A.; Sydnor, J.A.; Seale, D.L.; Gwaltney, J.J.M. Etiology and Antimicrobial Therapy of Acute Maxillary Sinusitis. J. Infect. Dis. 1979, 139, 197–202. [Google Scholar] [CrossRef]
- Arias Irimia, Ó.; Barona Dorado, C.; Santos Marino, J.; Martínez Rodríguez, N.; Martínez González, J.M. Meta-analisis of the etiology of odontogenic maxillary sinusitis. Med. Oral Patol. Oral Cirugía Bucal 2010, 15, 3–6. [Google Scholar]
- Paju, S.; Bernstein, J.M.; Haase, E.M.; Scannapieco, F.A. Molecular analysis of bacterial flora associated with chronically inflamed maxillary sinuses. J. Med. Microbiol. 2003, 52, 591–597. [Google Scholar] [CrossRef]
- Savolainen, S.; Jousimies-Somer, H.; Kleemola, M.; Ylikoski, J. Serological evidence of viral or Mycoplasma pneumoniae infection in acute maxillary sinusitis. Eur. J. Clin. Microbiol. Infect. Dis. 1989, 8, 131–135. [Google Scholar] [CrossRef]
- Erkan, M.; Özcan, M.; Arslan, S.; Soysal, V.; Bozdemir, K.; Haghighi, N. Bacteriology of Antrum in Children with Chronic Maxillary Sinusitis. Scand. J. Infect. Dis. 1996, 28, 283–285. [Google Scholar] [CrossRef] [PubMed]
- Erkan, M.; Aslan, T.; Ozcan, M.; Koç, N. Bacteriology of antrum in adults with chronic maxillary sinusitis. Laryngoscope 1994, 104, 321–324. [Google Scholar] [CrossRef] [PubMed]
- Aher, A.R.; Gujarathi, U.P.; Shinde, K.J. Incidence of fungal infections in chronic maxillary sinusitis. Indian J. Otolaryngol. Head Neck Surg. 2000, 52, 122–124. [Google Scholar] [CrossRef]
- Sindet-Pedersen, S.; Skoglund, L.A.; Hvidegaard, T.; Holst, E. A study of operative treatment and bacteriological examination of persistent oro-antral fistulas. Int. J. Oral Surg. 1983, 12, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Ylikoski, J.; Savolainen, S.; Jousimies-Somer, H. The Bacteriology of Acute Maxillary Sinusitis. ORL 1989, 51, 175–181. [Google Scholar] [CrossRef]
- Savolainen, S.; Ylikoski, J.; Jousimes-Somer, H. Predictive value of nasal bacterial culture for etiological agents in acute maxillary sinusitis. Rhinology 1987, 25, 49–55. [Google Scholar]
- Snyman, J.; Claassen, A.J.; Botha, P.L. A microbiological study of acute maxillary sinusitis in Bloemfontein. South Afr. Med. J. 1988, 74, 444–445. [Google Scholar]
- Su, W.-Y.; Liu, C.; Hung, S.-Y.; Tsai, W.-F. Bacteriological Study in Chronic Maxillary Sinusitis. Laryngoscope 1983, 93, 931–934. [Google Scholar] [CrossRef]
- Brorson, J.E.; Axelsson, A.; Holm, S.E. Serological Studies in Acute Maxillary Sinusitis. Acta Otolaryngol. 1976, 82, 415–419. [Google Scholar] [CrossRef]
- Karma, P.; Jokipii, L.; Sipila, P.; Luotonen, J.; Jokipii, A.M.M. Bacteria in Chronic Maxillary Sinusitis. Arch. Otolaryngol. Neck Surg. 1979, 105, 386–390. [Google Scholar] [CrossRef]
- Berg, O.; Carenfelt, C.; Kronvall, G. Bacteriology of Maxillary Sinusitis in Relation to Character of Inflammation and Prior Treatment. Scand. J. Infect. Dis. 1988, 20, 511–516. [Google Scholar] [CrossRef]
- Brown, C.A.; Paisner, H.M.; Biel, M.A.; Levinson, R.M.; Sigel, M.E.; Garvis, G.E.; Tedford, T.M. Evaluation of the Microbiology of Chronic Maxillary Sinusitis. Ann. Otol. Rhinol. Laryngol. 1998, 107, 942–945. [Google Scholar] [CrossRef] [PubMed]
- Yassin-Kassab, A.; Bhargava, P.; Tibbetts, R.J.; Do, Z.H.G.; Peterson, E.I.; Craig, J.R. Comparison of bacterial maxillary sinus cultures between odontogenic sinusitis and chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2020, 11, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.R.; Tataryn, R.W. Diagnosing odontogenic sinusitis of endodontic origin: A multidisciplinary literature review. Am. J. Otolaryngol. Head Neck Med. Surgery 2021, 42, 102925. [Google Scholar] [CrossRef] [PubMed]
- Taschieri, S.; Torretta, S.; Corbella, S.; Del Fabbro, M.; Francetti, L.; Lolato, A.; Capaccio, P. Pathophysiology of sinusitis of odontogenic origin. J. Investig. Clin. Dent. 2015, 8, e12202. [Google Scholar] [CrossRef]
- Olwoch, I.P. Microbiology of acute complicated bacterial sinusitis at the University of the Witwatersrand. S. Afr. Med. J. 2010, 100, 529–533. [Google Scholar] [CrossRef] [Green Version]
- Pokorny, A.; Tataryn, R. Clinical and radiologic findings in a case series of maxillary sinusitis of dental origin. Int. Forum Allergy Rhinol. 2013, 3, 973–979. [Google Scholar] [CrossRef]
- Longhini, A.B.; Ferguson, B.J. Clinical aspects of odontogenic maxillary sinusitis: A case series. Int. Forum Allergy Rhinol. 2011, 1, 409–415. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| N | % (CI 95%) | |
|---|---|---|
| Total sinuses | 7051 | |
| Total patients | 6415 | |
| Males | 3080 | 48% |
| Females | 3335 | 52% |
| Children | 319 | |
| Mean age | 33.82 | |
| Origin of sinusitis | ||
| Dental | 259 | 4% |
| 17 | 7% |
| 9 | 3% |
| 3 | 1% |
| 3 | 1% |
| 35 | 14% |
| 6 | 2% |
| 16 | 6% |
| 1 | 0% |
| 14 | 5% |
| 8 | 3% |
| 20 | 8% |
| 12 | 5% |
| 4 | 2% |
| Not specific * | 6156 | 96% |
| Mean Percentage (%) | Dispersion Percentage (SD) | Number of Underlying Articles | |
|---|---|---|---|
| Dental caries | 74.4 | 25.1 | 9 |
| Implant-related * | 23.9 | 13.4 | 2 |
| Sinus lift | 8.2 | 11.0 | 3 |
| Periodontitis | 6.7 | 3.6 | 2 |
| Mean Percentage (%) Relative Prevalence (CI 95%) | Studies Supporting the Finding | |
|---|---|---|
| Proportion of G1 infections out of total sinus infections | 24.21% (17.8–30.6) | 51 |
| Fusobacterium | 14.60% (10.7–18.5) | 17 |
| Prevotellas | 27.03% (20.6–33.5) | 19 |
| Porphyromonas | 7.37% (4.4–10.4) | 10 |
| Veillonellas | 14.06% (8.0–20.2) | 19 |
| Actinomyces | 21.16% (8.8–51.1) | 8 |
| Eubacterium | 9.06% (0.5–17.6) | 13 |
| Peptostreptococcus | 35.22% (27.4–43.0) | 26 |
| Propionibacterium | 17.09% (9.8–29.4) | 23 |
| St. Viridans | 39.89% (24.4–55.4) | 18 |
| Enterococcus | 16.88% (4.0–29.8) | 8 |
| Proportion of G2 infections out of total sinus infections | 63.51% (57.9–69.2) | 51 |
| Bacteroides | 15.65% (9.1–22.2) | 25 |
| Clostridium | 4.55% (2.5–6.6) | 10 |
| Staphylococcus aureus | 20.10% (2.6–37.6) | 43 |
| Klebsiella | 4.74% (3.2–6.3) | 26 |
| Streptococcus | 23.63% (18.2–29.0) | 40 |
| St. pyogenes | 8.62% (4.1–13.1) | 18 |
| Proteus | 5.84% (3.1–8.6) | 18 |
| Pseudomonas | 6.54% (3.9–9.2) | 26 |
| E. coli | 3.99% (2.5–5.5) | 27 |
| H. influenzae | 29% (21.0–37.1) | 43 |
| Neiserias | 6.40% (3.4–9.4) | 22 |
| Enterobacter | 6.18% (2.6–9.8) | 12 |
| Moraxellas | 6.82% (3.7–10.0) | 15 |
| Proportion of G3 infections out of total sinus infections | 12.27% (8.1–16.5) | 51 |
| St. pneumoniae | 20.02% (10.0–30.02) | 45 |
| Citrobacter spp. | 2.71% (1.4–4.2) | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Areizaga-Madina, M.; Pardal-Peláez, B.; Montero, J. Microbiology of Maxillary Sinus Infections: Systematic Review on the Relationship of Infectious Sinus Pathology with Oral Pathology. Oral 2023, 3, 134-145. https://doi.org/10.3390/oral3010012
Areizaga-Madina M, Pardal-Peláez B, Montero J. Microbiology of Maxillary Sinus Infections: Systematic Review on the Relationship of Infectious Sinus Pathology with Oral Pathology. Oral. 2023; 3(1):134-145. https://doi.org/10.3390/oral3010012
Chicago/Turabian StyleAreizaga-Madina, María, Beatriz Pardal-Peláez, and Javier Montero. 2023. "Microbiology of Maxillary Sinus Infections: Systematic Review on the Relationship of Infectious Sinus Pathology with Oral Pathology" Oral 3, no. 1: 134-145. https://doi.org/10.3390/oral3010012
APA StyleAreizaga-Madina, M., Pardal-Peláez, B., & Montero, J. (2023). Microbiology of Maxillary Sinus Infections: Systematic Review on the Relationship of Infectious Sinus Pathology with Oral Pathology. Oral, 3(1), 134-145. https://doi.org/10.3390/oral3010012