
Effect of Aging of Orthodontic Aligners in Different Storage Media on Force and Torque Generation: An In Vitro Study

 ,
,  and
and
Abstract
:Highlights
- Aging effect of saliva on mechanical properties of aligners is insignificant.
- In artificial aging, artificial saliva or deionized water have similar effect.
- The experimental studies of aligners have limitations.
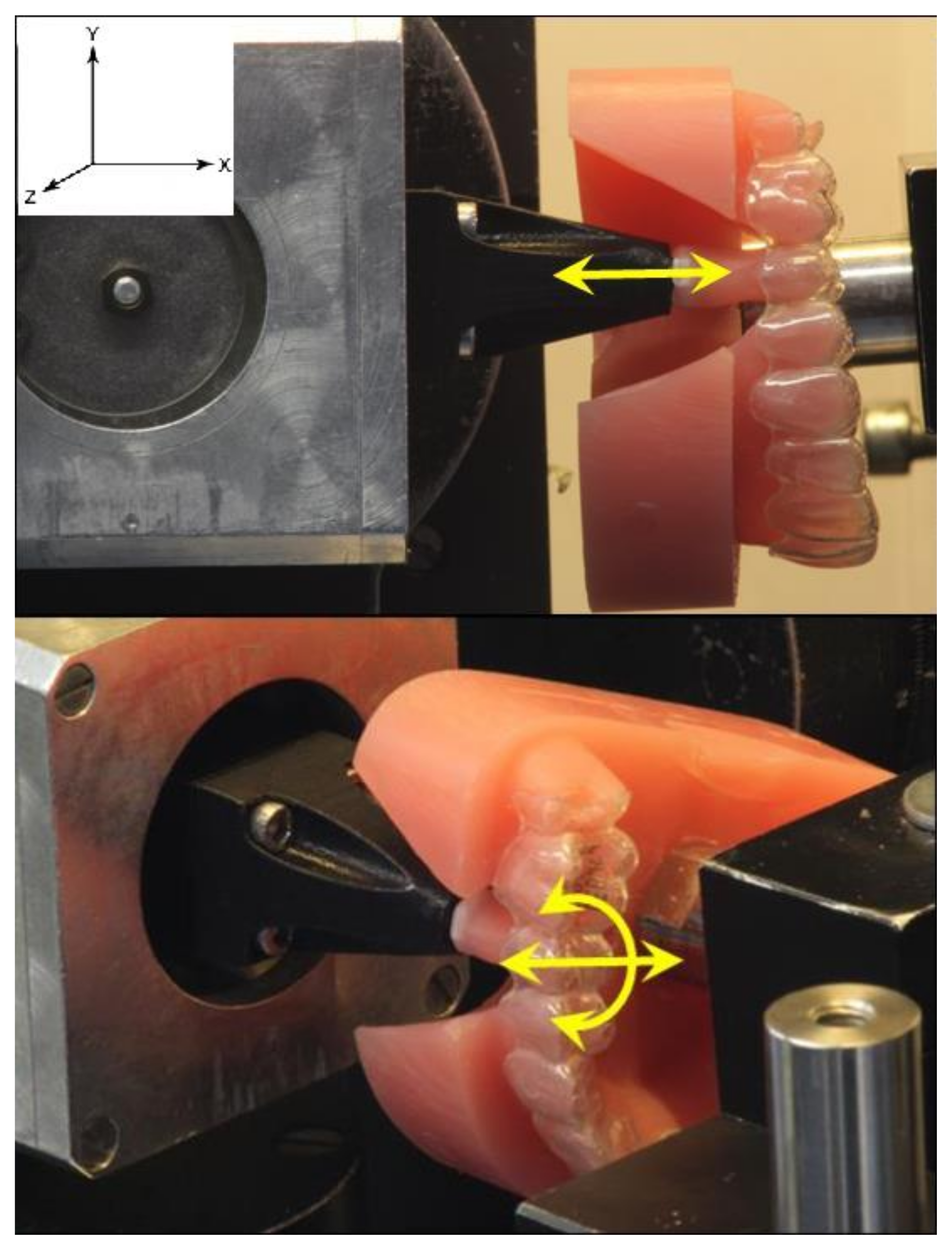
- Force generation by aligner is direction dependent.
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- The influence of artificial saliva only (as an approximation of natural saliva) on the mechanical properties of an aligner can be classified as insignificant, but other studies on the combined effect of saliva together with the aligner deformation over the 14 days use are needed;
- No significant difference between the forces/torques of the aligners stored in distilled water and those stored in artificial saliva, which means that the effect of the type of used medium for aging of aligners in vitro is insignificant; and
- Generation of forces and torques by aligner is direction-dependent due to tooth morphology.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Compliance with Ethics Requirements
References
- Ojima, K.; Kau, C.H. A perspective in accelerated orthodontics with aligner treatment. Semin. Orthod. 2017, 23, 76–82. [Google Scholar] [CrossRef]
- Pereira, D.; Machado, V.; Botelho, J.; Proença, L.; Mendes, J.J.; Delgado, A.S. Comparison of Pain Perception between Clear Aligners and Fixed Appliances: A Systematic Review and Meta-Analysis. Appl. Sci. 2020, 10, 4276. [Google Scholar] [CrossRef]
- Didier, V.F.; Almeida-Pedrin, R.R.; Oltramari, P.V.P.; Fernandes, T.M.F.; Dos Santos, L.L.; Conti, A.C. Influence of orthodontic appliance design on employment hiring preferences. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Elshazly, T.M.; Keilig, L.; Alkabani, Y.; Ghoneima, A.; Abuzayda, M.; Talaat, S.; Bourauel, C.P. Primary Evaluation of Shape Recovery of Orthodontic Aligners Fabricated from Shape Memory Polymer (A Typodont Study). Dent. J. 2021, 9, 31. [Google Scholar] [CrossRef] [PubMed]
- Elshazly, T.M.; Keilig, L.; Salvatori, D.; Chavanne, P.; Aldesoki, M.; Bourauel, C. Effect of Trimming Line Design and Edge Extension of Orthodontic Aligners on Force Transmission: An in vitro Study. J. Dent. 2022, 125, 104276. [Google Scholar] [CrossRef] [PubMed]
- Elshazly, T.M.; Keilig, L.; Aldesoki, M.; Ghoneima, A.; Abuzayda, M.; Talaat, W.; Talaat, S.; Bourauel, C.P. Computer-aided finite element model for biomechanical analysis of orthodontic aligners. Clin. Oral Investig. 2022, 27, 115–124. [Google Scholar] [CrossRef]
- Elshazly, T.M.; Keilig, L.; Alkabani, Y.; Ghoneima, A.; Abuzayda, M.; Talaat, W.; Talaat, S.; Bourauel, C.P. Potential Application of 4D Technology in Fabrication of Orthodontic Aligners. Front. Mater. 2022, 8, 586. [Google Scholar] [CrossRef]
- Hahn, W.; Fialka-Fricke, J.; Dathe, H.; Fricke-Zech, S.; Zapf, A.; Gruber, R.; Kubein-Meesenburg, D.; Sadat-Khonsari, R. Initial forces generated by three types of thermoplastic appliances on an upper central incisor during tipping. Eur. J. Orthod. 2009, 31, 625–631. [Google Scholar] [CrossRef]
- Hahn, W.; Dathe, H.; Fialka-Fricke, J.; Fricke-Zech, S.; Zapf, A.; Kubein-Meesenburg, D.; Sadat-Khonsari, R. Influence of thermoplastic appliance thickness on the magnitude of force delivered to a maxillary central incisor during tipping. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 12.e1–12.e7. [Google Scholar] [CrossRef]
- Upadhyay, M.; Arqub, S.A. Biomechanics of clear aligners: Hidden truths & first principles. J. World Fed. Orthod. 2021, 11, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, M.; Nanda, R. Biomechanics in orthodontics. Esthet. Biomech. Orthod. 2014, 152, 74–89. [Google Scholar]
- Lombardo, L.; Martines, E.; Mazzanti, V.; Arreghini, A.; Mollica, F.; Siciliani, G. Stress relaxation properties of four orthodontic aligner materials: A 24-h in vitro study. Angle Orthod. 2016, 87, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Janda, R. Organische Polymere: Chemie und Physik, Teil 1. Quintessenz Zahntech. 2008, 34, 190. [Google Scholar]
- Fang, D.; Zhang, N.; Chen, H.; Bai, Y. Dynamic stress relaxation of orthodontic thermoplastic materials in a simulated oral environment. Dent. Mater. J. 2013, 32, 946–951. [Google Scholar] [CrossRef]
- Vardimon, A.D.; Robbins, D.; Brosh, T. In-vivo von Mises strains during Invisalign treatment. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Schuster, S.; Eliades, G.; Zinelis, S.; Eliades, T.; Bradley, T.G. Structural conformation and leaching from in vitro aged and retrieved Invisalign appliances. Am. J. Orthod. Dentofac. Orthop. 2004, 126, 725–728. [Google Scholar] [CrossRef]
- Pazzini, L.; Cerroni, L.; Pasquantonio, G.; Pecora, A.; Mussi, V.; Rinaldi, A.; Mecheri, B.; Licoccia, S.; Maiolo, L. Mechanical properties of ‘two generations’ of teeth aligners: Change analysis during oral permanence. Dent. Mater. J. 2018, 37, 835–842. [Google Scholar] [CrossRef]
- Kwon, J.-S.; Lee, Y.-K.; Lim, B.-S.; Lim, Y.-K. Force delivery properties of thermoplastic orthodontic materials. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 228–234. [Google Scholar] [CrossRef]
- Ihssen, B.A.; Willmann, J.H.; Nimer, A.; Drescher, D. Effect of in vitro aging by water immersion and thermocycling on the mechanical properties of PETG aligner material. J. Orofac. Orthop. Kieferorthopädie 2019, 80, 292–303. [Google Scholar] [CrossRef]
- Hiller, D. Elastizitaet und Dimensionsstabilitaet von Druckformfolien vor und nach Temperaturwechselbelastung. Ph.D. Thesis, Charité-Universitätsmedizin Berlin, Berlin, Germany, 2018. [Google Scholar] [CrossRef]
- Lombardo, L.; Arreghini, A.; Ramina, F.; Huanca Ghislanzoni, L.T.; Siciliani, G. Predictability of orthodontic movement with orthodontic aligners: A retrospective study. Prog. Orthod. 2017, 18, 35. [Google Scholar] [CrossRef]
- Drake, C.T.; McGorray, S.P.; Dolce, C.; Nair, M.; Wheeler, T.T. Orthodontic tooth movement with clear aligners. ISRN Dent. 2012, 2012, 657973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nang, D. Veraenderung der Materialeigenschaften Kieferorthopaedischer Korrekturschienen durch Kuenstliche Alterung; Universitaets-und Landesbibliothek Bonn: Bonn, Germany, 2022; Available online: https://hdl.handle.net/20.500.11811/9790 (accessed on 6 May 2022).
- Geis-Gerstorfer, J.; Weber, H. Der Einfluss von Kaliumrhodanid auf das Korrosionsverhalten edelmetallfreier Dentallegierungen. Dtsch Zahnärztl 1985, 40, 87–91. [Google Scholar]
- Bourauel, C.; Drescher, D.; Thier, M. An experimental apparatus for the simulation of three-dimensional movements in orthodontics. J. Biomed. Eng. 1992, 14, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Drescher, D.; Bourauel, C.; Thier, M. Application of the orthodontic measurement and simulation system (OMSS) in orthodontics. Eur. J. Orthod. 1991, 13, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.A.; Bourauel, C. Forces and moments generated by removable thermoplastic aligners: Incisor torque, premolar derotation, and molar distalization. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Ryokawa, H.; Miyazaki, Y.; Fujishima, A.; Miyazaki, T.; Maki, K. The mechanical properties of dental thermoplastic materials in a simulated intraoral environment. Orthod. Waves 2006, 65, 64–72. [Google Scholar] [CrossRef]
- Elshazly, T.M.; Bourauel, C.; Sherief, D.I.; El-Korashy, D.I. Evaluation of Two Resin Composites Having Different Matrix Compositions. Dent. J. 2020, 8, 76. [Google Scholar] [CrossRef] [PubMed]
- Elshazly, T.M.; Bourauel, C.; Aboushelib, M.N.; Sherief, D.I.; El-Korashy, D.I. The polymerization efficiency of a bulk-fill composite based on matrix-modification technology. Restor. Dent. Endod. 2020, 45, e32. [Google Scholar] [CrossRef]
- Elshazly, T.M. Werkstoffwissenschaftliche Untersuchung eines Gefüllten, Matrixmodifizierten Zahnärztlichen Komposits; Universitäts-und Landesbibliothek Bonn: Bonn, Germany, 2021; Available online: https://hdl.handle.net/20.500.11811/8926 (accessed on 18 February 2021).
- Luft, S.I. Materialtechnische Untersuchungen an Selbstligierenden und Konventionellen Brackets; Universitäts-und Landesbibliothek Bonn: Bonn, Germany, 2008; Available online: https://hdl.handle.net/20.500.11811/3804 (accessed on 25 October 2008).
- Eliades, T.; Bourauel, C. Intraoral aging of orthodontic materials: The picture we miss and its clinical relevance. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 403–412. [Google Scholar] [CrossRef]
- Proffit, W.R.; Fields, H.W.; Sarver, D.M.; Ackerman, J.L. Contemporary Orthodontics; Mosby Inc.: St. Louis, MO, USA, 2000. [Google Scholar]
- Fiorelli, G.; Melsen, B. Biomechanics in orthodontics. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 134–135. [Google Scholar] [CrossRef]
- Wichelhaus, A.; Sander, C.; Sander, F.G. Development and biomechanical investigation of a new compound palatal arch. J. Orofac. Orthop. Kieferorthopädie 2004, 65, 104–122. [Google Scholar] [CrossRef]
- Kahl-Nieke, B. Einführung in die Kieferorthopädie: Diagnostik, Behandlungsplanung, Therapie: Mit 10 Tabellen; Deutscher Ärzteverlag: Köln, Germany, 2010. [Google Scholar]
- Sander, C.; Sander, F.M.; Sander, F.G. The derotation of premolars and canines with NiTi elements. J. Orofac. Orthop. Der Kieferorthopädie 2006, 67, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Erfurth-Jach, T.F. Biomechanische Untersuchungen an thermoplastisch geformten Schienen. Ph.D. Thesis, Georg-August-Universität Göttingen, Göttingen, Germany, 2012. [Google Scholar] [CrossRef]
- Barbagallo, L.J.; Jones, A.S.; Petocz, P.; Darendeliler, M.A. Physical properties of root cementum: Part 10. Comparison of the effects of invisible removable thermoplastic appliances with light and heavy orthodontic forces on premolar cementum. A microcomputed-tomography study. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Elkholy, F.; Panchaphongsaphak, T.; Kilic, F.; Schmidt, F.; Lapatki, B.G. Forces and moments delivered by PET-G aligners to an upper central incisor for labial and palatal translation. J. Orofac. Orthop. 2015, 76, 460–475. [Google Scholar] [CrossRef] [PubMed]
- Elkholy, F.; Schmidt, F.; Jäger, R.; Lapatki, B.G. Forces and moments delivered by novel, thinner PET-G aligners during labiopalatal bodily movement of a maxillary central incisor: An in vitro study. Angle Orthod. 2016, 86, 883–890. [Google Scholar] [CrossRef]
- Elkholy, F.; Mikhaiel, B.; Schmidt, F.; Lapatki, B.G. Mechanical load exerted by PET-G aligners during mesial and distal derotation of a mandibular canine. J. Orofac. Orthop. 2017, 78, 361–370. [Google Scholar] [CrossRef]
- Elkholy, F.; Schmidt, F.; Jäger, R.; Lapatki, B.G. Forces and moments applied during derotation of a maxillary central incisor with thinner aligners: An in-vitro study. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 407–415. [Google Scholar] [CrossRef]
- Engelke, B. Kraft-und Drehmomentabgabe Thermoplastisch Geformter Schienen bei Frontzahnderotation vor und nach Alterungssimulation. Ph.D. Thesis, Georg-August-Universität Göttingen, Göttingen, Germany, 2010. [Google Scholar] [CrossRef]
- Barbagallo, L.J.; Shen, G.; Jones, A.S.; Swain, M.V.; Petocz, P.; Darendeliler, M.A. A novel pressure film approach for determining the force imparted by clear removable thermoplastic appliances. Ann. Biomed. Eng. 2008, 36, 335–341. [Google Scholar] [CrossRef]
- Elshazly, T.; Salvatori, D.; Bourauel, C.; Elattar, H.; Alkabani, Y. Effect of Thickness and Material Type of Orthodontic Aligners on Force Transmission: An in Vitro Study Using Pressure-Sensitive Films. SSRN 2022, 4270102. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | Molecular Formula | Concentration (mg/L) |
|---|---|---|
| Sodium Chloride | NaCl | 400 |
| Potassium Chloride | KCl | 400 |
| Calcium Chloride Dihydrate | CaCl2·2H2O | 795 |
| Sodium Hydrogen Phosphate 1-Hydrate | NaH2PO4·H2O | 690 |
| Potassium Rhodanide | KSCN | 300 |
| Sodium Sulfide | Na2S·9H2O | 1.67 [normal with 5H2O] |
| Urea | CH4N2O | 1000 |
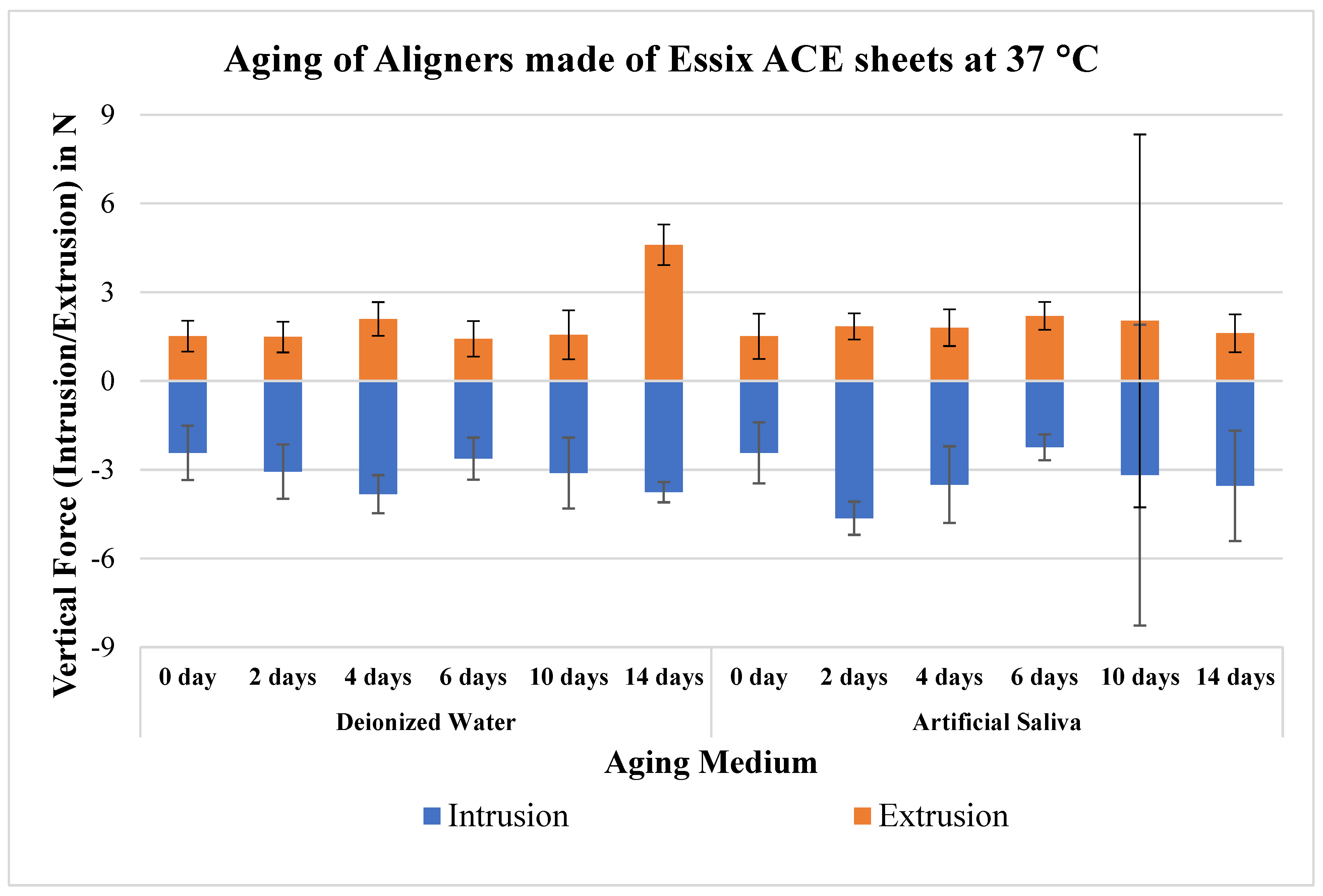
| Intrusion Force (N) | p-Value | Extrusion Force (N) | p-Value | |||
|---|---|---|---|---|---|---|
| Aging | Deionized Water | Artificial Saliva | Deionized Water | Artificial Saliva | ||
| 0 day | −2.4 ± 0.9 A | −2.4 ± 0.9 B | - | 1.5 ± 0.5 A | 1.5 ± 0.5 A | - |
| 2 days | −3.1 ± 0.6 Ab | −4.6 ± 0.7 Aa | * p < 0.05 | 1.5 ± 0.6 Aa | 1.9 ± 0.6 Aa | 0.121 |
| 14 days | −3.8 ± 5.1 Aa | −3.6 ± 1.9 ABa | 0.899 | 4.6 ± 6.3 Aa | 1.6 ± 0.6 Aa | 0.322 |
| p-value | 0.899 | * p < 0.05 | 0.899 | 0.899 | ||
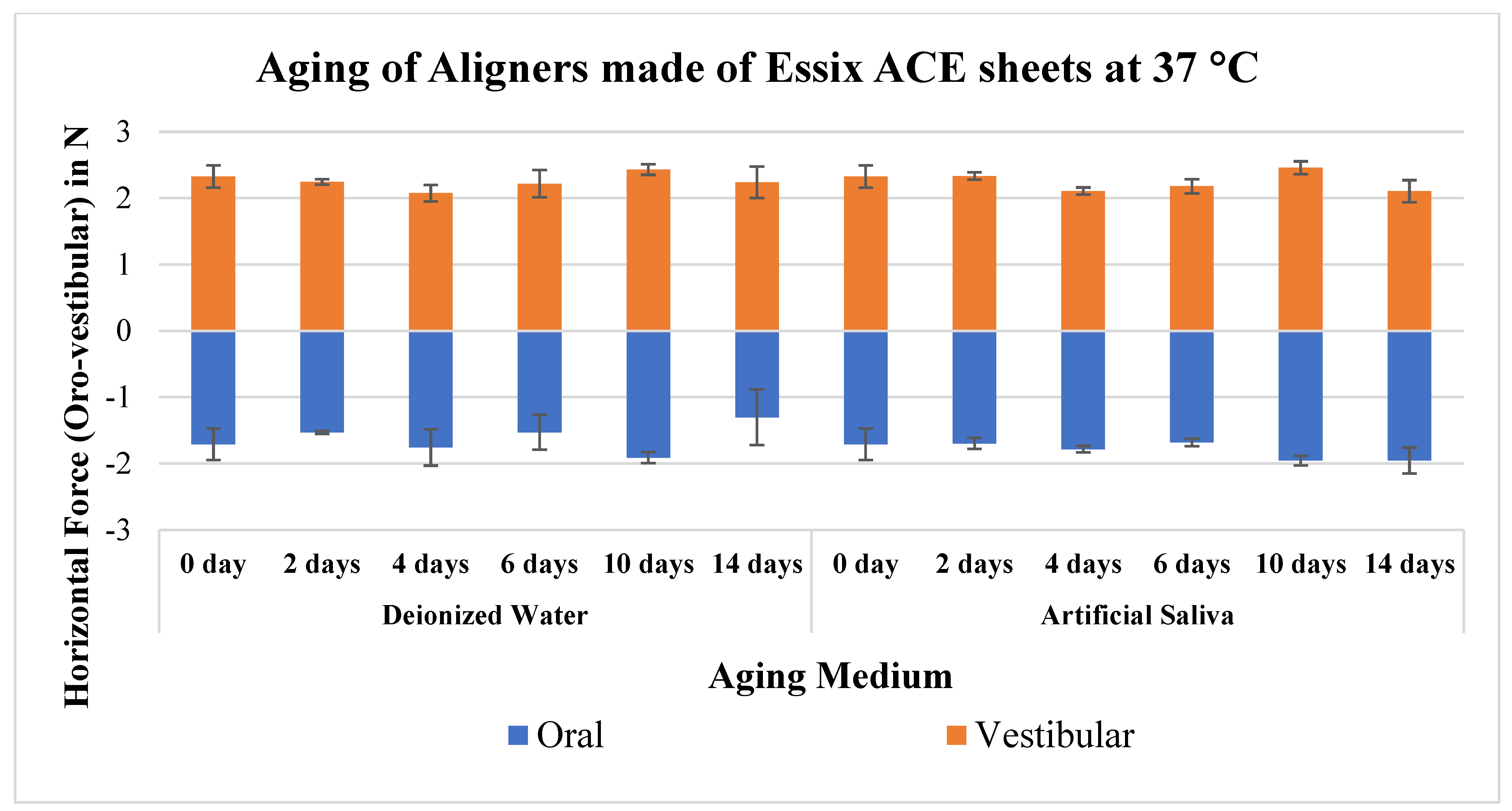
| Oral Force (N) | p-Value | Vestibular Force (N) | p-Value | |||
| Aging | Deionized Water | Artificial Saliva | Deionized Water | Artificial Saliva | ||
| 0 day | −1.7 ± 0.2 A | −1.7 ± 0.2 A | - | 2.3 ± 0.2 A | 2.3 ± 0.2 A | - |
| 2 days | −1.5 ± 0.0 Ab | −1.7 ± 0.1 Aa | * p < 0.05 | 2.2 ± 0.0 Ab | 2.3 ± 0.1 ABa | * p < 0.05 |
| 14 days | −1.3 ± 0.4 Ab | −2.0 ± 0.2 Aa | * p < 0.05 | 2.2 ± 0.2 Aa | 2.1 ± 0.2 Ba | 0.336 |
| p-value | 0.899 | 0.899 | 0.899 | * p < 0.05 | ||
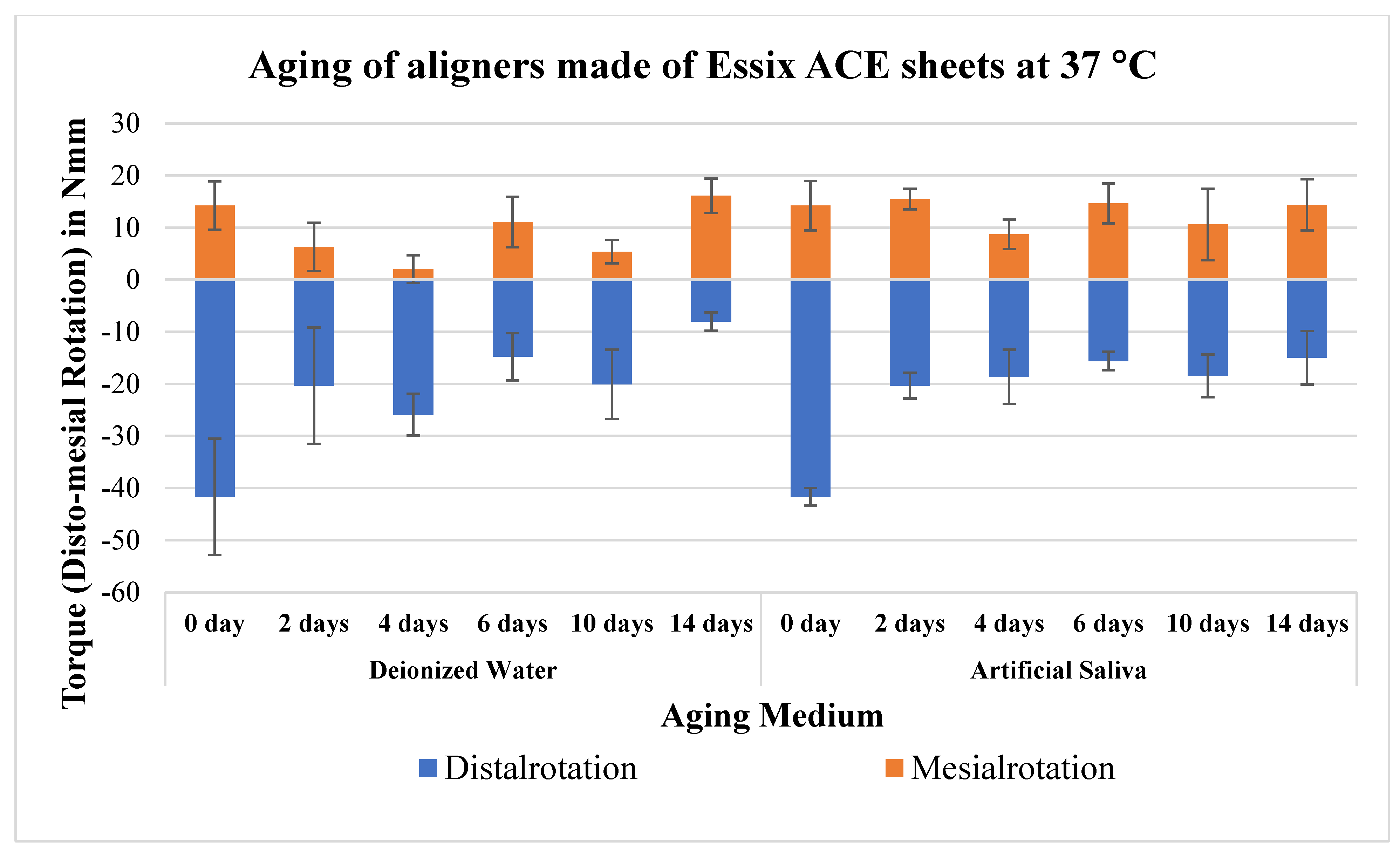
| Distalrotation Torque (Nmm) | p-Value | Mesialrotation Torque (Nmm) | p-Value | |||
| Aging | Deionized Water | Artificial Saliva | Deionized Water | Artificial Saliva | ||
| 0 day | −41.7 ± 11.2 A | −41.7 ± 11.2 A | - | 14.2 ± 4.7 A | 14.2 ± 4.7 A | - |
| 2 days | −20.4 ± 4.0 Ba | −20.3 ± 4.6 Ba | 0.899 | 6.3 ± 2.7 Bb | 15.5 ± 4.8 Aa | * p < 0.05 |
| 14 days | −8.1 ± 4.1 Bb | −15.0 ± 5.1 Ba | * p < 0.05 | 16.1 ± 6.9 Aa | 14.4 ± 4.9 Aa | 0.674 |
| p-value | * p < 0.05 | * p < 0.05 | * p < 0.05 | 0.899 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elshazly, T.M.; Nang, D.; Golkhani, B.; Elattar, H.; Bourauel, C. Effect of Aging of Orthodontic Aligners in Different Storage Media on Force and Torque Generation: An In Vitro Study. Oral 2023, 3, 67-76. https://doi.org/10.3390/oral3010007
Elshazly TM, Nang D, Golkhani B, Elattar H, Bourauel C. Effect of Aging of Orthodontic Aligners in Different Storage Media on Force and Torque Generation: An In Vitro Study. Oral. 2023; 3(1):67-76. https://doi.org/10.3390/oral3010007
Chicago/Turabian StyleElshazly, Tarek M., Diva Nang, Bijan Golkhani, Hanaa Elattar, and Christoph Bourauel. 2023. "Effect of Aging of Orthodontic Aligners in Different Storage Media on Force and Torque Generation: An In Vitro Study" Oral 3, no. 1: 67-76. https://doi.org/10.3390/oral3010007
APA StyleElshazly, T. M., Nang, D., Golkhani, B., Elattar, H., & Bourauel, C. (2023). Effect of Aging of Orthodontic Aligners in Different Storage Media on Force and Torque Generation: An In Vitro Study. Oral, 3(1), 67-76. https://doi.org/10.3390/oral3010007