1. Introduction
Inherited bleeding disorders (IBD) are lifelong conditions that are associated with a wide range of bleeding manifestations. Von Willebrand disease (VWD) and Haemophilia are the most common types of IBD, corresponding to more than 95% of all IBD [
1].
Von Willebrand disease (VWD) is the most common IBD, with an estimated prevalence of 1% based on population screening [
2]. VWD is the result of a qualitative or quantitative defect in von Willebrand factors (VWF). The VWF protein stabilises factor VIII and enables platelet interaction with the blood vessel wall. Inherited VWD can be further divided into three subgroups. Type I represents the most common variant of von Willebrand’s disease, and accounts for approximately 80% of VWD cases. Type I VWD is characterised by a reduced quantity of circulating VWF, whereby the synthesis of VWF is normal, but the release of VWF multimers is inhibited. In type II VWD, there is a defect in the function rather than the amount of VWF. In type III cases, the most severe form of disease, the levels of VWF are negligible or undetectable [
3].
Haemophilia is an inherited X-linked chromosomal bleeding disorder, caused by deficiencies in factor VIII (haemophilia A) or factor IV (haemophilia B). Haemophilia is less common than VWD but is the most common severe IBD. Being X-linked, haemophilia typically affects males, while females are classified as carriers. Most carriers are asymptomatic, although some carriers may be symptomatic with clotting factor levels in the haemophiliac range, and experience bleeding episodes relative to their degree of clotting factor deficiency. In these instances, symptomatic carriers are classified as haemophiliac in line with the World Federation of Hemophilia guidelines [
4]. Patients with haemophilia may be on prophylactic factor regimens. This is via intravenous replacement of factor VIII or IX, with either purified plasma derived concentrates or recombinant factor concentrates. The dose, duration and frequency of treatment is dependent on the severity of bleeding. Haemophilia is defined as severe when plasma activity is <1 IU/dL (normal range 50–100); moderate if it ranges between 2–5 IU/dL and mild when ranging between 6–40 IU/dL [
5].
Good oral health for individuals with IBD is imperative, to minimize the risk of oral bleeding from gingival inflammation, periodontal disease and prevent the need for extraction of teeth. There is sufficient evidence that patients with a low bleeding risk may receive preventive and simple dental procedures in the community dental setting [
6]. Despite this, many dentists lack confidence and knowledge when treating patients with bleeding disorders. There is currently no protocol for delivery of oral health care to paediatric patients with IBD in Australia. Consequently, most of these patients are seen in hospital paediatric dental clinics. The purpose of this narrative review was to explore the management strategies and internationally established worldwide protocols on the oral health management for paediatric patients with IBD.
2. Materials and Methods
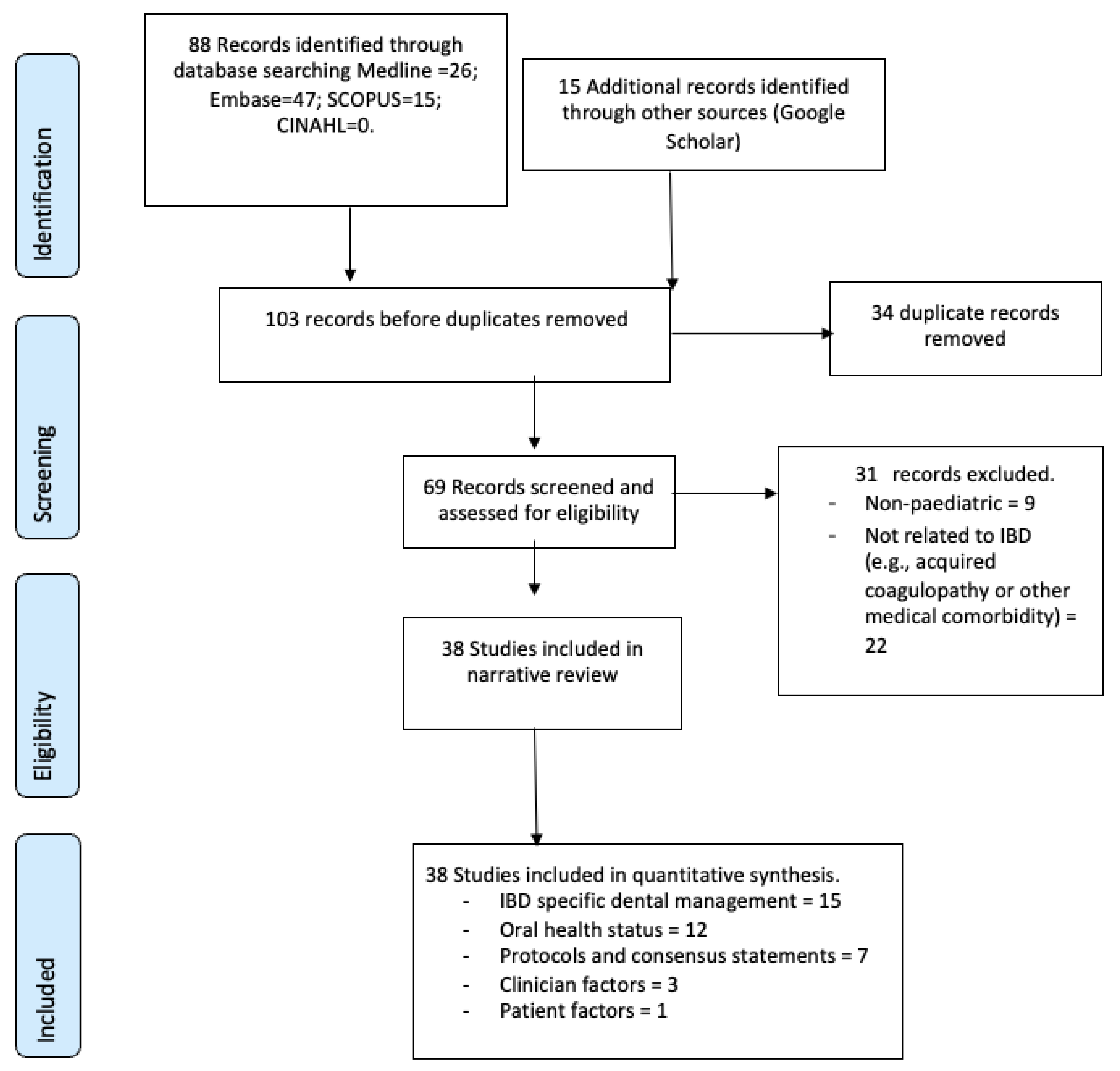
An electronic search of four databases up to July 2023 was undertaken using Medline (Ovid and PubMed), Embase (Ovid), Scopus and CINAHL. The search was undertaken using MeSH (Medical Subject Headings) terms listed in
Table 1 below. These terms were used in combination using ‘Boolean’ operators. Only articles published in English language were included. A university librarian experienced in undertaking literature reviews was consulted to ensure the relevance of individual search strategies. Hand searching of reference lists of selected articles chosen to be included were also explored to ensure relevant publications were also included (
Figure 1: PRISMA flow diagram).
Inclusion criteria: English language publications relating to the oral health outcomes, education, and management of paediatric patients with IBD. The key focus areas of this narrative review were the oral health status of paediatric patients with IBD, patient and clinician factors, IBD specific dental management, and protocols and consensus statements relating to models of care.
When no publications were identified on specific aspects of care in the paediatric population (such as patient and clinician barriers), publications with adult patients relating to the topic were included. Exclusion criteria: Patients with acquired bleeding disorders.
The search yielded 69 publications (
Table 2), with 38 included in the narrative review. All eligible studies were organised using EndNote X9 (The Thompson Corporation, NY, USA). Duplicate records and studies that appeared in more than one database were removed.
3. Results
Using an inductive thematic analysis, data extracted from the selected studies identified the following themes and subthemes:
- -
Oral health status.
- -
Patient factors.
- →
Barriers and enablers in accessing care.
- -
Clinician factors.
- →
Barriers and enablers in providing care.
- -
IBD specific management.
- →
Emergency and elective dental treatment.
- →
Anaesthesia and analgesia considerations.
- -
Protocols and consensus statements.
- →
Management in private practice.
- →
Models of shared care.
- →
Criteria for referral to tertiary centres.
4. Discussion
4.1. Access to Oral Health Care
It has been suggested that patients with a low bleeding risk may receive preventive and simple dental procedures in the community dental setting [
6]. Dentists who care for patients with IBD are required to understand their patient’s medical condition, severity, and response to previous treatment to formulate a safe dental treatment plan. The World Federation of Hemophilia ‘Guidelines for dental treatment of patients with inherited bleeding disorders’ [
14] outline that minor oral surgery, dental extractions and dental treatments that require the use of inferior alveolar nerve (IAN) block anaesthesia and/or anaesthesia via lingual infiltration, require referral to a hospital-based dental clinic [
14]. A similar consensus statement by Australian hospital dentists and specialists outlined the dental management of adult patients with IBD [
25]. Similarly, this Australian publication also detailed procedures including routine examinations, scaling, restorations, endodontic and prosthodontic treatment that requires buccal or palatal infiltration anaesthesia may be safely carried out in a community dental setting.
4.2. Patient and Clinician Barriers
Kalsi reported 40% of general dental practitioners (GDPs) surveyed in the United Kingdom reported feeling not comfortable treating patients with IBD in the general dental setting [
27]. This lack of confidence from oral health practitioners to provide care for patients with IBD carries the potential risk of poorer oral health outcomes and a risk of untreated disease, potentially requiring a greater level of intervention than may have been needed if recognised earlier.
Kalsi also surveyed 105 individuals with IBD regarding their experiences with accessing primary oral health care [
27]. Their results highlighted a range of primarily patient-related barriers rather than disease-related barriers. Only one-fifth of patients reported being refused treatment by a GDP, whereas almost half (45%) felt their dentist did not have the expertise to care for them.
4.3. Oral Health Outcomes
4.3.1. Oral Health Status and Oral Health Related Quality of Life
It is important that the maintenance of optimal oral health is prioritised in children with IBD. Despite numerous publications on the general medical health of children with IBD, very few have reported on the oral health profiles of these children. Research from the UK and Northern Ireland have demonstrated that children with haemophilia were reported to have a significantly lower prevalence of dental caries compared to their healthy matched controls [
39]. In contrast, two studies from Turkey and Poland respectively found poorer oral hygiene levels and dental status in haemophiliac children [
8,
29].
Salem in 2013 conducted a study investigating both the dental health status and oral health-related quality of life amongst children with IBD in Iran [
36]. Forty-six patients aged between 2–15 years old with IBD who were referred for treatment at a tertiary children’s hospital for comprehensive care; were matched for age and gender with forty-six fit and healthy children as a control. Twenty-six IBD patients (55%) reported a history of bleeding from the oral cavity, primarily during the time of dental eruption or primary tooth shedding, with the second most common reason for bleeding being trauma-induced bleeding particularly on the tongue. Spontaneous gingival bleeding and bleeding with toothbrushing was reassuringly not a main complaint amongst most participants. Salem found that more children with IBD were caries-free compared to their controls and this result was statistically significant, however there was no statistically significant difference in the permanent dentition. They found no difference in oral health related quality of life (OHRQoL) scores amongst children with IBD and their healthy counterparts.
4.3.2. Exfoliation and Eruption
Salem 2018 assessed the oral health status of 53 haemophiliac children and adolescents aged 2–15 years in Iran. They reported the highest rate of oral haemmorhage was associated with exfoliation of primary teeth and tooth eruption [
37]. It should be noted that natural dental exfoliation as well as assisted exfolation of primary teeth does not require haemostatic cover [
25].
4.4. Management in Private Practice
Formulation of a dental treatment plan for patients with IBD must consider not only the patients bleeding risk, but also the extent of treatment that is required, the location of treatment within the mouth, as well as the experience of the treating clinician [
25]. As previously discussed, non- or minimally-invasive dental treatments do not require adjustment of factor levels—such as intraoral radiographs, supra-gingival restorations, the use of local anaesthesia via infiltrations and supragingival scaling [
25]. For patients with IBD to be safely treated in the primary oral health care setting, effective communication pathways between the private dental practitioner and the patient’s specialist haematologist or haematology treatment centre (HTC) must exist. For patients identified as at being high bleeding risk and those who are undergoing a high bleeding risk procedure, a referral to a dental specialist tertiary centre should be made.
4.5. Models of Shared Care
Improving communication between hospital dental clinics and primary oral health care clinics in the community is an important step in establishing effective and financially viable pathways for the provision of oral health care for patients with IBD. The Royal London Hospital (RLH) is a major centre of care for children with IBD. RLH has established a pathway for oral health management of children with IBD [
21]. This pathway aims to redistribute patients to primary oral care services for patients identified as low risk that require routine dental treatment, so that the hospital services can be reserved for management of more complex dental treatment in higher risk individuals. In the RLH care pathway, there is a paediatric dental specialist (PDS) who plays a central role in attending haematology clinics. It is at this point that preventive advice is given, and the family is provided with a letter to their GDP detailing the current treatment guidelines and highlights the GDPs role in the provision of ongoing preventive dental care. This letter also provides contact information for the haemophilia team and PDS associated with the HTC. GDPs are encouraged to actively liaise with the haematologists and PDS to not only support the provision of primary dental care in the community, but also to directly refer patients that need high-bleeding risk or invasive procedures to be done within the hospital oral health service. Within this system, patients that require cover and those with severe IBD have their treatment within the specialist hospital dental service by a PDS [
21].
There is currently no pathway of care for paediatric patients with IBD in Australia or New Zealand. Consequently, in Australasia, hospital paediatric dental clinics see most of these patients, rather than a shared model of care such as in RLH. This is an important area of potential research to inform the development of a protocol for use in Australia as successfully demonstrated in the UK.
4.6. Criteria for Referral of Paediatric Patients with IBD to Tertiary Centres
For invasive dental procedures that are associated with significant bleeding risk in high-risk patients, four therapeutic management options are available for use to increase factor levels:
4.6.1. Coagulation Factor Replacement Therapy
Coagulation factor replacement therapy is the mainstay of treatment for patients with moderate and severe Haemophilia. Factor replacement therapy may be administered on a prophylactic basis or prescribed as required for episodes of bleeding. Factor concentrates were historically plasma-derived and therefore were associated with the potential for transfusion-transmitted infections such as Hepatitis B. The development of recombinant factor replacement therapy over the past several decades has significantly decreased the risk of blood borne viral infections [
14]. One of the major complications following the administration of factor concentrate involves the development of inhibitors that negate the effect of the factor infusion [
10].
Factor concentrate is administered via IV infusion, either at an HTC or by the individual/their caregiver. The timing of factor administration is important due to the levels of factor declining over time; therefore a patients dental treatment should be performed ideally within 30 to 60 min of factor administration [
10]. Factor concentrates are costly, and it is important that the amount of treatment conducted is maximised on any one occasion following factor administration.
A recent publication by de Azevedo Kinalski and colleagues involved a scoping review on the prophylactic and therapeutic protocols for oral procedures in patients with IBD. They identified that factor replacement continues to be the most indicated approach when providing invasive dental treatment for patients with IBD, along with the adjunctive use of systemic or local anti-fibrinolytic agents. They identified that further research is needed in order to explore the safety of using antifibrinolytic agents alone as a prophylactic measure, without the addition of factor replacement therapy [
44].
4.6.2. Desmopressin (DDAVP)
Desmopressin is a synthetic derivative of vasopressin that stimulates the release of endogenous factor VIII and vWF. DDAVP is typically used in individuals with mild haemophilia A and vWD. It is important to note that patients with haemophilia B, however, do not respond to DDAVP treatment. Eligible patients often undergo a trial of DDAVP to evaluate their responsiveness to treatment. Repeated treatment with DDAVP may cause a diminished response. It is postulated that this decreased response to treatment over time is likely due to exhaustion of endothelial stores, hyponatremia and fluid retention [
45]. DDAVP can be administered subcutaneously 60 min prior to the procedure; intravenously 60 min prior with a 20–30-min infusion time; or intranasally. Treatment with DDAVP is contraindicated in children under 2 years of age, and should be avoided in very young children due to risks of hyponatraemia [
10].
4.6.3. Antifibrinolytic Agents
Antifibrinolytic agents prevent degradation of the fibrin clot which supports blood clotting; they can be administered topically or systemically. The most commonly used antifibrinolytic agents for the management of bleeding during invasive dental procedures such as extractions, are tranexamic acid (TXA) and epsilon aminocaproic acid (EACA). The TXA agent is more potent than EACA [
46]. TXA inhibits the activation of plasminogen to plasmin, thereby inhibiting the lysis of fibrin. It is available via intravenous preparation, oral preparation, and mouthwash form. TXA is given at an oral dose of 15–25 mg/kg, approximating to 1 g for adults every 6–8 h [
10]. The British Committee for Standards in Haematology recommend the use of TXA for use in the control of oral bleeding in acquired coagulation disorders, however this recommendation does not detail the preferred route of administrations [
47]. TXA (10 mL of 5% solution) may be commenced just prior the dental procedure, and then continued 6 hourly for 7–10 days post operatively [
10]. The use of a prescribed mouthwash in the paediatric population however poses practical challenges, as the recommended dose may be exceeded if inadvertently swallowed.
4.6.4. Local Haemostatic Measures
Suturing
In adults, suturing is a useful adjunctive local haemostatic measure. In the paediatric population however, opinion and preference vary. In some clinics, sutures are avoided due to concern regarding the increased number of puncture holes due to suturing, from a viewpoint that suturing is not as essential in smaller sockets from primary tooth extractions [
10]. Despite this, many centres advocate for the use of sutures, particularly when treatment is conducted under general anaesthesia, to prevent the potential need to return for a second general anaesthetic to control bleeding should post-operative haemorrhage occur.
Other Local Haemostatic Adjuncts
Collagen containing resorbable gelatine sponge, such as Gelfoam
® (Pharmacia and Upjohn Company, Kalamazoo, USA) is an absorbable gelatine sponge of bovine origin that provides a scaffold for clot formation. The sheet material is rolled into a cone shape and then placed inside the tooth socket, where it is absorbed and is associated with minimal to no scarring. It is important that Gelfoam
® is not used under flaps or epithelial incisions however, as it has been documented to inhibit the healing of epithelial edges [
50].
Surgicel
® (Johnson and Johnson, New Brunswick, NJ, USA) is an oxidised cellulose gauze of synthetic origin. It is a knitted material, prepared from polyanhydroglucuronic acid and alpha cellulose. It can conform readily to any contour; clings to bleeding tissues, can be applied as single layer or as a cavity pack and is able to retain its uniform structure when folded. When exposed to blood, it swells and is converted to a gelatinous mass forming an artificial clot-like structure. It is tolerated by the tissues and enclosed within the wound and does not impair healing within dental sockets. Other novel local haemostatic measures have also been documented in the literature, such as Lyostpt
® Ankaferd Blood Stopper [
10] for management of oral bleeding.
Fibrin glue is a topical biological adhesive. Its primary effective is by mimicking the final pathway of the coagulation cascade, whereby fibrinogen is converted to fibrin in the presence of thrombi, factor XIII, fibronectin, and ionised calcium. The resultant clot formed aids with haemostasis and is totally absorbed during wound healing, without any foreign body reactions nor significant fibrosis [
51]. The evidence for the use of fibrin glue use on gingiva and mucosa within the oral cavity remains limited [
10].
Bone wax is a management option for controlling bleeding within cancellous bone. It is comprised of, paraffin, beeswax, and a softening agent. To use bone wax, the origin of the bleed must be confirmed before the wax is packed into the space within the bone. The pressure provided by the wax aids in achieving haemostasis. A major disadvantage of bone wax is that it is not resorbable, and therefore a foreign body reaction may potentially be mounted. Consequently, it is preferrable that bone wax is removed once haemostasis has occurred; although in reality, it often remains in situ as total removal is challenging [
52].
4.7. Anaesthesia Considerations
For patients with IBD undergoing treatment under general anesthesia, factor replacement therapy is indicated in order to cover the potential bleeding risk associated with intubation. Nasal intubation is avoided as traumatic bleeding and submucosal haemorrhage [
35]. Care must be taken in patient positioning to ensure pressure points and extremities have appropriate padding to avoid intramuscular haematoma or haemarthrosis [
35].
Use of local anaesthesia (LA) poses various degrees of risk in patients with IBD and therefore may require discussion with their specialist haematologist. Infiltrations can be typically be safely provided without the provision of haemostatic cover, particularly with the development of single-use needles [
14]. Local anaesthesia should be injected slowly minimize the risk of haematoma formation and to allow sufficient time for the solution to slowly diffuse through the tissues. Local anaesthesia with vasoconstrictor should be used where appropriate to offer additional haemostasis [
53]. Use of nitrous oxide sedation and anxiolytics may also be considered to provide additional analgesia.
In individuals with severe IBD, regional nerve blocks and lingual infiltrations should be avoided. Historically there have been reported cases of airway obstruction due to haematoma formation in the retromolar and pterygoid spaces following the use of deep nerve block injections with local anaesthesia [
14]. The risk of a potneitally life-threatening haematoma is considered to be low with the advent of fine-gauge and single-use needles. Despite this, extreme care must still be taken when giving LA to high bleeding risk patients. In cases where anesthesia of the IAN distribution is required, the use of the Gow-Gates technique has been suggested for use as a relatively safer alternative [
14]. The Gow-Gates technique is otherwise known as a true manidbular nerve block; it requires the patients mouth to be wide open and the clinician aims to administer the LA just anterior to the neck of the condyle, in proximity to the manidbular branch of the trigeminal nerve after its exit from the foramen ovale [
54]. However where possible, intraligamentous or intrapapillary injections should be utilised instead, particularly with paediatric patients [
53].
The use of long acting LA such as bupivacaine hydrochloride may be a suitable option for not only haemostasis but also post operative analgesia, giving up to 8–10 h of pain control following the dental procedure. This may not be suitable for all paediatric patients however, and it is important that if used, parents and caregivers are aware of the risk of inadvertant self-trauma, such as lip, cheek and tongue biting while anesthetised.
4.8. Analgesia and Antibiotic Considerations
Post procedural dental pain can typically be managed with simple analgesia, with paracetamol being the mainstay medication to manage dental pain in paediatric patients with IBD [
4]. NSAIDs such as aspirin should not be used due to the risk of adverse affects on platelet aggregation. Should the use of additional NSAIDs be required, their use must be discussed with the patients haematologist [
14].
Baed on the current literature, there is insufficient evidence to support the use of prophylactic antibiotics prior to dental extractions in IBD patients [
14]. There are no contraindications to any type of antibiotics used for patients with IBD. If a significant risk of infection is considered, the provision of prophylactic antibiotics should be discussed with the patients haematologist on a case by case basis.
4.9. Emergency and Elective Dental Treatment
4.9.1. Emergency Dental Management
Traumatic dental injuries such as uncomplicated crown fractures (without pulpal exposure) can be treated without additional factor cover [
43]; however any soft tissue injuries or injuries involving significant oral haemorrhage secondary to orofacial trauma must be managed in conjunction with the patients haematologist.
Dentists managing patients with IBD in both the hospital and community settings should be competent in the emergency management of oral haemorrhage. Patients may present complaining of a slow ooze, or significant and sudden haemorrhage may result from oral trauma or dental procedures. Post extraction haemorrhage may be categorised in relation to timing:
- -
Primary haemorrhage: Describes bleeding immediately post operatively.
- -
Reactionary haemorrhage: Describes bleeding 2–3 h post procedure. This is due to cessation of vasoconstriction.
- -
Secondary haemorrhage: Can occur up to 2 weeks post procedure. The typical cause of secondary haemorrhage is post-operative infection.
Initial management of oral haemorrhage should always start with careful examination to determine the origin of the bleed, followed by control of the bleeding, and then prevention of further episodes of bleeding. A comprehensive history from the patient’s caregiver is important, as oral haemorrhage may result in patients with IBD with normal physiological processes such as erupting or exfoliating teeth.
Patients who present to emergency clinics complaining of odontogenic pain may be treated with analgesia. Those who present with mild facial swellings secondary to odontogenic infection may be managed initially with oral antibiotics. Those with moderate or severe facial swellings secondary to odontogenic infection may require hospital admission for the provision of intravenous antibiotics prior to definitive invasive dental treatment, upon discussion with the patients haematologist [
43].
4.9.2. General Principles of Elective Oral Health Care
When undertaking any procedure within the oral cavity of a patient with an IBD, it is important that potential trauma to the oral mucosa is limited. The risk of causing localised trauma may be reduced peri-operatively by careful placement of the saliva ejector and high speed suction, taking care when placing intraoral radiographs particularly in the sublingual region of the mouth and exercising careful techniques when taking intraoral impressions [
25].
4.9.3. Preventive Dental Treatment
Bleeding following invasive dental treatment in patients with IBD may result in severe or potentially life threatening bleeding events, therefore this patient group must be a priority for preventive oral health care [
55]. Early preventive dental care helps reduce the need for future invasive dental treatment, which carries with it a high financial and treatment burden. Taking a holistic and patient centred care approach, patients with IBD should be stratified as high caries risk due to the complex treatment considerations for comprehensive caries management in this patient group [
10].
The World Federation of Hemophilia recommend that children with haemophilia are seen by a dental professional at the time of their first tooth erupting, or by their first birthday to reduce the financial, health and psychosocial burden associated with oral health diseases in individuals with IBD [
4]. The World Federation of Hemophilia guidelines also detail that all children should be brushing twice daily (<7 years of age with 1000-ppm fluoride toothpaste; >7 years of age with 1400-ppm fluoride toothpaste), along with 6-monthly dental visits and restriction of high sugar foods [
14].
4.9.4. Restorative Treatment
Routine restorative dental treatment can be safely carried out in general dental practice outside of a hospital setting, provided that local anaesthesia is used appropriately and carefully [
25]. The modern use of minimally invasive dental techniques are highly relevant in patients with IBD, in minimising potential soft tissue trauma and morbidity associated with the restorative life cycle of teeth [
56].
4.9.5. Endodontic Treatment
Similar to restorative treatment, standard endodontic treatment is also considered a low-risk dental procedure in individuals with IBD [
14]. Pulpectomy and pulpotomy treatments can be performed in patients with bleeding disorders and generally represent a preferrable management option over extractions where appropriate. Endodontic treatment should be carefully carried out within the working length of the canal, to ensure that there is no extrusion of instruments beyond the root apex that may elicit bleeding. Teeth with open apices present a higher risk of intracanal bleeding than teeth with closed apices. Pulpotomies in primary teeth can be safely carried out within their accepted indications.
4.9.6. Periodontal Treatment
For patients with IBD who have periodontal disease and poor oral hygiene, it is important that a comprehensive periodontal treatment plan be devised in order to prevent progressive destruction of the periodontal tissues [
25]. For individuals with mild periodontitis, routine probing and supragingival debridement is unlikely to result in prolonged bleeding; meaning that no specific haemostatic interventions are typically required [
57]. For patients with moderate or severe bleeding risk, or moderate periodontal disease, a TXA mouthwash is useful to aid in haemostasis following supragingival scaling [
25]. In IBD patients with severe periodontal disease, liaising with the patient’s haematologist prior to commencing any treatment is imperative. Chlorhexidine mouthwash and gross supragingival debridement in these cases is suggested to decrease tissue inflammation prior to commencing subgingival scaling [
53]. Periodontal treatment often needs to be planned over a several appointments to avoid unnecessary bleeding [
14]. Periodontal surgery for individuals with IBD is considered a high bleeding risk procedure, and should only be contemplated where conservative treatment options have been exhausted [
25]. It is important that all periodontal surgery must be planned carefully in communication with the patients haematologist/HTC to allow for the provision of systemic haemostatic cover [
14].
4.9.7. Oral Surgical Treatment & Exodontia
Minor oral surgical treatment, including routine exodontia, should be carefully planned to minimise the risk of bleeding and haematoma formation in individuals with IBD. Treatment must planned be in discussion with the patients haematologist/HTC. Surgical techniques should be adapted to decrease the risk of intra-operative and post-operative haemorrhage. This may include planned sectioning of multi-rooted teeth, limiting the number of dental extractions in one session, minimally invasive flap design, opting for closure patterns that allow access for packing and suturing, endeavouring to obtain primary wound closure at surgical sites, and debridement of granulation tissue in regions of chronic inflammation [
58]. Persistent post-operative haemorrhage following exodontia or minor oral surgery should be managed initially with local measures. Should haemostasis still not be achieved, the patients HTC should be consulted to consider whether hospital admission for additional systemic haemostatic therapy may be indication [
25].
4.9.8. Orthodontic Treatment
It is deemed safe to deliver both fixed and removable orthodontic appliances to patients with IBD, alongside regular preventive care and hygiene therapy [
14]. Care must be taken to ensure that sharp edges or extruded wires that have the potential to cause intraoral trauma are trimmed and polished. The importance of good preventive care and oral hygiene during this period is essential [
57].
Limitations of this narrative review include the addition of a selection of publications relating to the oral health care of adults with IBD due to a scarcity of paediatric specific literature on protocols for management of this patient cohort.
5. Conclusions
Although excess bleeding is a significant risk for patients with IBD undergoing invasive dental procedures, non-invasive procedures can typically be safely undertaken in the general dental setting. Patients who access routine dental care are more likely to experience better oral health and less likely to require invasive treatment such as extractions. Despite it being safe, families of children with IBD face several barriers in accessing routine primary oral health care. The results of this narrative review showed a paucity of published literature investigating barriers and enabling factors for seeking and providing primary oral health care for this patient cohort and has highlighted the need for further exploration into both patient and clinician related factors. The results of this narrative review have informed the development of a survey for general dental practitioners in Australia and New Zealand to explore their attitudes, knowledge, and experience of treating paediatric patients with IBD. The results of this survey will be used to aid the development of a shared care protocol for management of paediatric patients with IBD in both the community and hospital dental setting, according to their risk stratification.
Author Contributions
Conceptualization, A.F.V.R. and N.P.; methodology, A.F.V.R.; formal analysis, A.F.V.R.; investigation, A.F.V.R.; resources, A.F.V.R. and N.P.; data curation, A.F.V.R. and N.P.; writing—original draft preparation, A.F.V.R.; writing—review and editing, N.P.; visualisation, A.F.V.R. and N.P.; supervision, N.P.; project administration, A.F.V.R. and N.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mannucci, P.M.; Duga, S.; Peyvandi, F. Recessiely inherited coagulation disorders. Blood 2004, 104, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- Rodeghiero, F.; Castaman, G.; Dini, E. Epidemiological investigation of the prevalence of von Willebrand’s disease. Blood 1987, 69, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, T.S.; Ruggeri, Z.M. Pathologic Basis of Disease. In Von Willebrand’s Disease, 4th ed.; Cotran, R.S.K.V., Robbins, S.L., Eds.; WB Saunders: Philadelphia, PA, USA, 1989; pp. 696–698. [Google Scholar]
- Srivastava, A.; Santagostino, E.; Dougall, A. WFH Guidelines for the Management of Hemophilia, 3rd edition. Haemophilia 2020, 26, 1–158. [Google Scholar] [CrossRef] [PubMed]
- White, G.C.; Rosendaal, F.; Aledort, L.M.; Lusher, J.M.; Rothschild, C.; Ingerslev, J.; Factor VIII and Factor IX Subcommittee. Definitions in hemophilia. Recommendation of the scientific subcommittee on factor VIII and factor IX of the scientific and standardization committee of the International Society on Thrombosis and Haemostasis. Thromb. Haemost. 2001, 85, 560. [Google Scholar] [PubMed]
- Dougall, A.; O’Mahoney, B. Evaluation of a collaborative model of shared care designed to increase access to preventive and restorative dentistry for patients with haemophilia. Haemophilia 2010, 16, 50. [Google Scholar]
- Adewumi, A.; Sakhalkar, V. Dental Management of a Patient with Factor X Deficiency. J. Can. Dent. Assoc. 2009, 75, 461–464. [Google Scholar]
- Albayrak, H.; Alpkilic, E.; Ak, G.; Pinar, A.; Sepet, E. Evaluation of oral and dental health in children with hemophilia. Hemophilia 2006, 12, 34–36. [Google Scholar]
- Alpkilic Baskirt, E.; Ak, G.; Zulfikar, B. Oral and general health-related quality of life among young patients with haemophilia. Haemophilia 2009, 15, 193–198. [Google Scholar] [CrossRef]
- Anderson, J.A.M.; Brewer, A.; Creagh, D.; Hook, S.; Mainwaring, J.; McKernan, A.; Yee, T.T.; Yeung, C.A. Guidance on the dental management of patients with haemophilia and congenital bleeding disorders. Br. Dent. J. 2013, 215, 497–504. [Google Scholar] [CrossRef]
- Basir, L.; Zarouni, F.; Sarikhani, P. Knowledge, Attitude and Performance of General Dentists in Relation to Children with Hemophilia and Related Therapies in Ahwaz. Indian J. Forensic Med. Toxicol. 2019, 13, 473. [Google Scholar] [CrossRef]
- Berlocher, W.C.; King, D.L. Considerations in the dental management of the factor VIII-deficient child with inhibitors. Pediatr. Dent. 1979, 1, 188–191. [Google Scholar]
- Boyd, D.; Kinirons, M. Dental caries experience of children with haemophilia in Northern Ireland. Int. J. Paediatr. Dent. 1997, 7, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Brewer, A.; Correa, M.E. Guidelines for dental treatment of patients with inherited bleeding disorders. Haemophilia 2005, 11, 504–509. [Google Scholar]
- Brown, M.C.; Hastie, E.; Shumake, C.; Waters, B.; Sidonio, R.F., Jr. Dental habits and oral health in children and adolescents with bleeding disorders: A single-institution cross-sectional study. Haemophilia 2022, 28, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Camm, J.H.; Murata, S.M. Emergency dental management of a patient with von Willebrand’s disease. Endod. Dent. Traumatol. 1992, 8, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Colin, W.; Needleman, H.L. Medical/dental management of a patient with congenital Factor XIII. Pediatr. Dent. 1985, 7, 227–230. [Google Scholar]
- Dellinger, T.M.; Livingston, M.; Holder, R.; Streckfus, C.F. Glycogen storage disease and von Willebrand’s disease implications for dental treatment: Dental management of a pediatric patient. SCD Spec. Care Dent. 1998, 18, 143–246. [Google Scholar]
- Durham, T.M.; Hodges, E.D.; Harper, J.; Green, J.; Tennant, F. Management of traumatic oral-facial injury in the hemophiliac patient with inhibitor: Case report. Pediatr. Dent. 1993, 15, 282–287. [Google Scholar]
- El Batawi, H.Y. Minimizing the Risk of Perioperative Bleeding in a Child with Hemophilia A during Dental Rehabilitation under General Anesthesia: A Case Report. Int. J. Clin. Paediatr. Dent. 2013, 6, 217–222. [Google Scholar] [CrossRef]
- Fong, F.; Davies, J.; Fearne, J.; Pasi, J. A dental care pathway for children with inherited bleeding disorders. J. Haemoph. Pract. 2014, 1, 3–6. [Google Scholar] [CrossRef]
- Gaddam, K.R.; Nuvvula, S.; Nirmala, S.; Kamatham, R. Oral health status among 6-to 12-year-old haemophilic children—An educational intervention study. Haemophilia 2014, 20, e338–e341. [Google Scholar] [CrossRef] [PubMed]
- George, A.M.; Mayya, A.; Mayya, A.; Iszham, A.B.; Rafi, N.H.B.M.; Marius, R.; Mayya, S.S. Knowledge and Awareness regarding Dental Management of Hemophilic Patients among Students of a Malaysian University: A Cross-Sectional Study. Open Dent. J. 2022, 16, E187421062205260. [Google Scholar] [CrossRef]
- Hall, R.K. Dental management of the chronically ill child. Aust. Dent. J. 1979, 24, 334–341. [Google Scholar] [CrossRef]
- Hewson, I.D.; Daly, J.; Hallett, K.B. Consensus statement by hospital based dentists providing dental treatment for patients with inherited bleeding disorders. Aust. Dent. J. 2011, 56, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Kabil, N.; El Alfy, M.; Metwalli, N. Evaluation of the oral health situation of a group of Egyptian haemophilic children and their re-evaluation following an oral hygiene and diet education programme. Haemophilia 2007, 13, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Kalsi, H.; Nanayakkara, L.; Pasi, K.J.; Bowles, L.; Hart, D.P. Access to primary dental care for patients with inherited bleeding disorders. Haemophilia 2012, 18, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Pai, K.M.; Kurien, A.; Vineetha, R. Oral hygiene and dentition status in children and adults with hemophilia: A case-control study. Spec. Care Dent. 2018, 38, 391–394. [Google Scholar] [CrossRef]
- Mielnick-Blaszcak, M. Evaluation of dentition status and oral hygiene in Polish children and adolescents with congenital haemorrhagic diatheses. Int. J. Pediatr. Dent. 1999, 9, 99–103. [Google Scholar] [CrossRef]
- Othman, N.A.; Sockalingam, S.N.; Mahyuddin, A. Oral health status in children and adolescents with haemophilia. Haemophilia 2015, 21, 605–611. [Google Scholar] [CrossRef]
- Parry, J.A.; Khan, F.A. Provision of dental care for medically compromised children in the UK by general dental practitioners. Int. J. Paediatr. Dent. 2000, 10, 322–327. [Google Scholar] [CrossRef]
- Poornima, P.; Shashibhushan, K.; Bharath, K.; Subba Reddy, V. Factor XIII deficiency: Report of two cases. J. Clin. Pediatr. Dent. 2010, 35, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Raso, S.; Napolitano, M.; Sirocchi, D.; Siragusa, S.; Hermans, C. The important impact of dental care on haemostatic treatment burden in patients with mild haemophilia. Haemophilia 2022, 28, 996–999. [Google Scholar] [CrossRef] [PubMed]
- Rasaratnam, L.; Chowdary, P.; Pollard, D.; Subel, B.; Harrington, C.; Darbar, U.R. Risk-based management of dental procedures in patients with inherited bleeding disorders: Development of a Dental Bleeding Risk Assessment and Treatment Tool (DeBRATT). Haemoph. Off. J. World Fed. Hemoph. 2017, 23, 247–254. [Google Scholar] [CrossRef]
- Rayen, R.; Hariharan, V.S.; Elzvazhagan, N.; Kamalendran, N.; Varadarajan, R. Dental management of hemophiliac child under general anesthesia. J. Indian Soc. Pedod. Prev. Dent. 2011, 29, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Salem, K.; Eshghi, P. Dental health and oral health-related quality of life in children with congenital bleeding disorders. Haemophilia 2013, 19, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Salem, K.; Seyyedkhamesi, S.; Aminian, M. Evaluation of oral and dental health status in hemophilic children and adolescents in the city of Rasht. J. Pediatr. Res. 2018, 5, 182–186. [Google Scholar] [CrossRef]
- Shivakumar, V.H.; Garg, R.; Tegginamani, A.S.; Gupta, V.V. Dental Considerations of Hereditary Bleeding Disorders in Children: An Overview. Oral Maxillofac. Pathol. J. 2022, 13, 36–43. [Google Scholar]
- Sonbol, H.; Pelargidou, M.; Lucas, V.S. Dental health indices and caries related microflora in children with severe hemophilia. Hemophilia 2001, 7, 468–474. [Google Scholar] [CrossRef]
- Stubbs, M.; Lloyd, J. A protocol for the dental management of von Willebrand’s disease, haemophilia A and haemophilia B. Aust. Dent. J. 2001, 46, 37–40. [Google Scholar] [CrossRef]
- Tamagond, S.B.; Hugar, S.I.; Patil, A.; Huddar, S. Christmas disease: Diagnosis and management of a haemorrhagic diathesis following dentofacial trauma. Case Rep. 2015, bcr2014203790. [Google Scholar] [CrossRef]
- Vierrou, A.M.; de la Fuente, B.; Poole, A.E.; Hoyer, L.W. DDAVP (desmopressin) in the dental management of patients with mild or moderate hemophilia and von Willebrand’s disease. Pediatr. Dent. 1985, 7, 297–301. [Google Scholar]
- Yee, R.; Duggal, M.S.; Wong, V.Y.Y.; Lam, J.C.M. An Update on the Dental Management of Children with Haemophilia. Prim. Dent. J. 2021, 10, 45–51. [Google Scholar] [CrossRef] [PubMed]
- de Azevedo Kinalski, M.; Sarkis-Onofre, R.; Dos Santos, M.B.F. Inherited bleeding disorders in oral procedures. Assessment of prophylactic and therapeutic protocols: A scoping review. Aust. Dent. J. 2021, 66, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Mannucci, P.M. Desmopressin (DDAVP) in the treatment of bleeding disorders: The first twenty years. Haemophilia 2000, 6, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Pell, G. Tranexamic acid—Its use in controlling dental post-operative bleeding in patients with defective clotting mechanisms. Br. J. Oral Surg. 1973, 11, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Perry, D.J.; Noakes, T.J.; Helliwell, P.S. Guidelines for the management of patients on oral anticoagulants requiring dental surgery. Br. Dent. J. 2007, 203, 389–393. [Google Scholar] [CrossRef]
- Adornato, M.C.; Penna, K.J. Hemostatic technique using a splint in oral bleeding. N. Y. State Dent. J. 2001, 67, 24. [Google Scholar]
- Lockhart, P.B.; Gibson, J.; Pond, S.H.; Leitch, J. Dental management considerations for the patient with an acquired coagulopathy. Part 1: Coagulopathies from systemic disease. Br. Dent. J. 2003, 195, 439–445. [Google Scholar] [CrossRef]
- Seichshnaydre, M.A.; Sismanis, A.; Hughes, G.B. Update of Reparative Granuloma: Survey of the American Otological Society and the American Neurotology Society. Am. J. Otolaryngol. 1994, 15, 155–160. [Google Scholar]
- Brennan, M. Fibrin glue. Blood Rev. 1991, 5, 240–244. [Google Scholar] [CrossRef]
- McCormick, N.J.; Moore, U.J.; Meechan, J.G. Haemostasis part 1: The management of post-extraction haemorrhage. Dent. Update 2014, 41, 290–296. [Google Scholar] [CrossRef]
- Gupta, A.; Epstein, J.B.; Cabay, R.J. Bleeding disorders of importance in dental care and related patient management. J. Can. Dent. Assoc. 2007, 73, 77–83. [Google Scholar] [PubMed]
- Gow-Gates, G.A.E. Mandibular conduction anesthesia: A new technique using extraoral landmarks. Oral Surg. Oral Med. Oral Pathol. 1973, 36, 321–330. [Google Scholar] [CrossRef]
- Scully, C.; Dios, P.D.; Giangrande, P.; Lee, C. Oral care for people with hemophilia or a hereditary bleeding tendency. Treat. Hemoph. Monogr. Ser. World Fed. Hemoph. Montr. 2008, 1, 10–11. [Google Scholar]
- Leal, S.C. Minimum intervention in dentistry: Applicability for dental care of patients with inherited bleeding disorders. Haemophilia 2010, 16, 50. [Google Scholar]
- Brewer, A.K.; Roebuck, E.M.; Donachie, M. The dental management of adult patients with haemophilia and other congenital bleeding disorders. Haemophilia 2003, 9, 673–677. [Google Scholar] [CrossRef] [PubMed]
- Israels, S.; Schwetz, N.; Boyar, R.; McNicol, A. Bleeding disorders: Characterization, dental considerations and management. J. Can. Dent. Assoc. 2006, 72, 827. [Google Scholar]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).





{kind=link}