

Age-at-Death Estimation: Accuracy and Reliability of Common Age-Reporting Strategies in Forensic Anthropology

Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Age-Estimation Methods
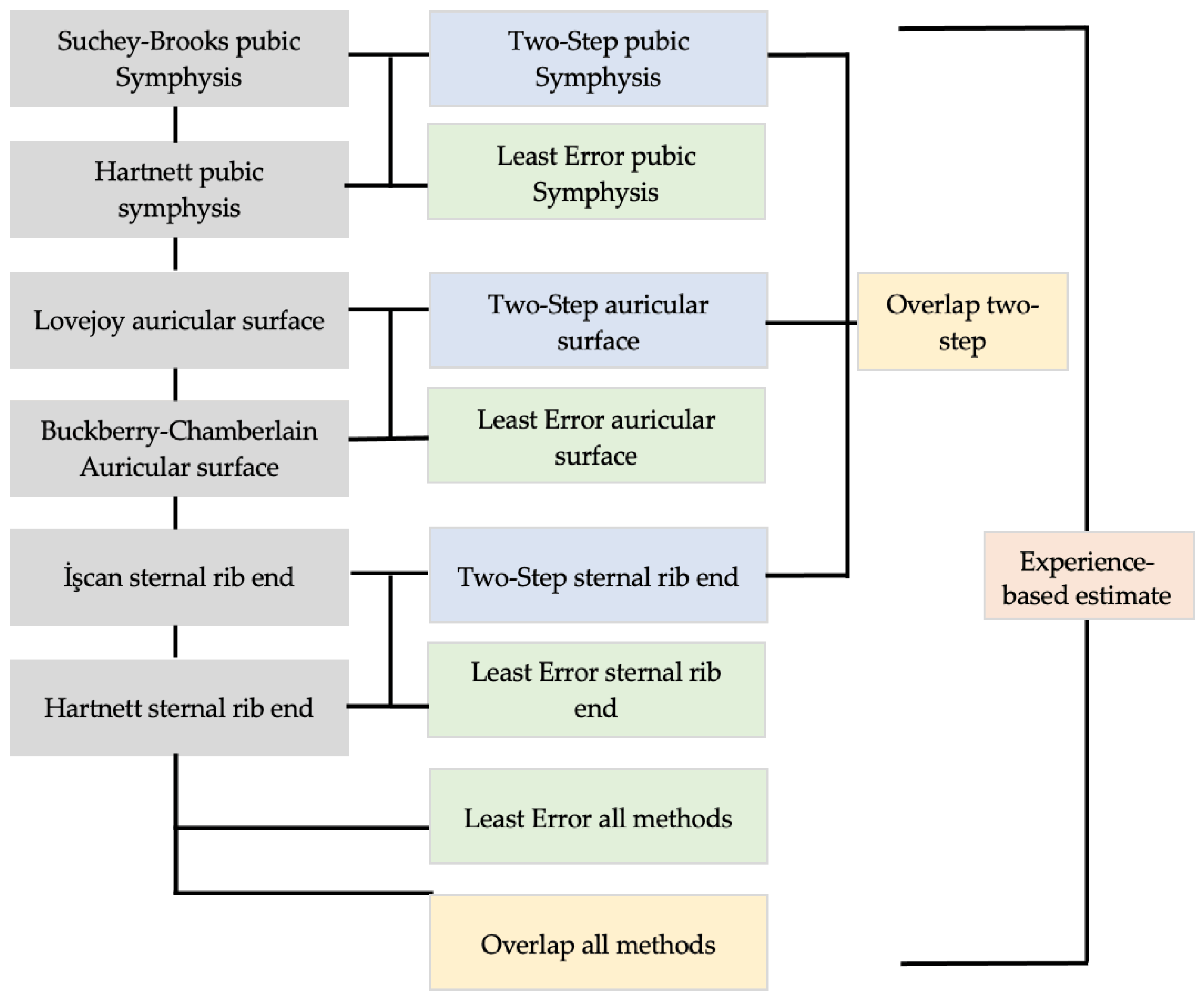
2.3. Age-Reporting Strategies
2.4. Statistical Methodologies
3. Results
3.1. T-Test Results Comparing Actual Age and Estimated Age
3.2. Accuracy and Reliability Results
3.3. Results by Age Cohort
3.4. Results by Sex
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Daubert v. Merrell Dow Pharmaceuticals. 1993. Available online: https://supreme.justia.com/cases/federal/us/509/579/ (accessed on 13 March 2023).
- Garvin, H.M.; Passalacqua, N.V. Current Practices by Forensic Anthropologists in Adult Skeletal Age Estimation. J. Forensic Sci. 2011, 57, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Martrille, L.; Ubelaker, D.H.; Cattaneo, C.; Seguret, F.; Tremblay, M.; Baccino, E. Comparison of Four Skeletal Methods for the Estimation of Age at Death on White and Black Adults. J. Forensic Sci. 2007, 52, 302–307. [Google Scholar] [CrossRef]
- Merritt, C.E. Testing the Accuracy of Adult Skeletal Age Estimation Methods: Original Methods versus Revised and Newer Methods. Explor. Anthropol. 2013, 12, 102–119. [Google Scholar]
- Miranker, M. A Comparison of Different Age Estimation Methods of the Adult Pelvis. J. Forensic Sci. 2016, 61, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Saunders, S.; Fitzgerald, C.; Rogers, T.; Dudar, C.; McKillop, H. A Test of Several Methods of Skeletal Age Estimation using a Documented Archaeological Sample. Can. Soc. Forensic Sci. J. 1992, 25, 97–118. [Google Scholar] [CrossRef]
- Baccino, E.; Ubelaker, D.H.; Hayek, L.-A.C.; Zerilli, A. Evaluation of Seven Methods of Estimating Age at Death from Mature Human Skeletal Remains. J. Forensic Sci. 1999, 44, 12019J. [Google Scholar] [CrossRef]
- Baccino, E.; Sinfield, L.; Colomb, S.; Baum, T.P.; Martrille, L. Technical note: The two step procedure (TSP) for the determination of age at death of adult human remains in forensic cases. Forensic Sci. Int. 2014, 244, 247–251. [Google Scholar] [CrossRef]
- Lovejoy, C.O.; Meindl, R.S.; Mensforth, R.P.; Barton, T.J. Multifactorial determination of skeletal age at death: A method and blind tests of its accuracy. Am. J. Phys. Anthr. 1985, 68, 1–14. [Google Scholar] [CrossRef]
- Nawrocki, S.P. The Nature and Sources of Error in the Estimation of Age at Death from the Skeleton. In Age Estimation of the Human Skeleton; Latham, K.E., Finnegan, M., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2010; pp. 79–101. [Google Scholar]
- Brooks, S.; Suchey, J.M. Skeletal Age Determination Base on the Os Pubis: A Comparison of the Acsádi-Nemeskéri and Suchey-Brooks Methods; Springer: Berlin/Heidelberg, Germany, 1990; pp. 227–238. [Google Scholar]
- Lovejoy, C.O.; Meindl, R.S.; Pryzbeck, T.R.; Mensforth, R.P. Chronological metamorphosis of the auricular surface of the ilium: A new method for the determination of adult skeletal age at death. Am. J. Phys. Anthr. 1985, 68, 15–28. [Google Scholar] [CrossRef]
- İşcan, M.Y.; Loth, S.R.; Wright, R.K. Age Estimation from the Rib by Phase Analysis: White Males. J. Forensic Sci. 1984, 29, 11776J. [Google Scholar] [CrossRef]
- İşcan, M.Y.; Loth, S.R.; Wright, R.K. Metamorphosis at the sternal rib end: A new method to estimate age at death in white males. Am. J. Phys. Anthr. 1984, 65, 147–156. [Google Scholar] [CrossRef] [PubMed]
- İşcan, M.Y.; Loth, S.R.; Wright, R.K. Age Estimation from the Rib by Phase Analysis: White Females. J. Forensic Sci. 1985, 30, 11018J. [Google Scholar] [CrossRef]
- Hartnett, K.M. Analysis of Age-at-Death Estimation Using Data from a New, Modern Autopsy Sample-Part I: Pubic Bone. J. Forensic Sci. 2010, 55, 1145–1151. [Google Scholar] [CrossRef] [PubMed]
- Buckberry, J.; Chamberlain, A. Age estimation from the auricular surface of the ilium: A revised method. Am. J. Phys. Anthr. 2002, 119, 231–239. [Google Scholar] [CrossRef]
- Hartnett, K.M. Analysis of Age-at-Death Estimation Using Data from a New, Modern Autopsy Sample-Part II: Sternal End of the Fourth Rib. J. Forensic Sci. 2010, 55, 1152–1156. [Google Scholar] [CrossRef] [PubMed]
- Yule, G.U. On the Theory of Correlation. J. R. Stat. Soc. 1897, 60, 812. [Google Scholar] [CrossRef]
- IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0; IBM Corp: Armonk, NY, USA, 2016. [Google Scholar]
- Meindl, R.S.; Lovejoy, C.O.; Mensforth, R.P.; Walker, R.A. A revised method of age determination using the os pubis, with a review and tests of accuracy of other current methods of pubic symphyseal aging. Am. J. Phys. Anthr. 1985, 68, 29–45. [Google Scholar] [CrossRef]
- Milner, G.R.; Boldsen, J.L. Transition analysis: A validation study with known-age modern American skeletons. Am. J. Phys. Anthr. 2012, 148, 98–110. [Google Scholar] [CrossRef]
- Parsons, H.R. The Accuracy of the Biological Profile in Casework: An Analysis of Forensic Anthropology Reports in Three Medical Examiner Offices; University of Tennessee: Knoxville, TN, USA, 2017. [Google Scholar]
- Lamendin, H.; Baccino, E.; Humbert, J.F.; Tavernier, J.C.; Nossintchouk, R.M.; Zerilli, A. A Simple Technique for Age Estimation in Adult Corpses: The Two Criteria Dental Method. J. Forensic Sci. 1992, 37, 13327J. [Google Scholar] [CrossRef]
- San-Millán, M.; Rissech, C.; Turbón, D. New approach to age estimation of male and female adult skeletons based on the morphological characteristics of the acetabulum. Int. J. Leg. Med. 2016, 131, 501–525. [Google Scholar] [CrossRef]
- Passalacqua, N.V. Forensic Age-at-Death Estimation from the Human Sacrum. J. Forensic Sci. 2009, 54, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Langley, N.R.; Jantz, L.M.; Ousley, S.D.; Jantz, R.L.; Milner, G. Data Collection Procedures for Forensic Skeletal Material 2.0. 2016. Available online: https://fac.utk.edu/wp-content/uploads/2016/03/DCP20_webversion.pdf (accessed on 13 March 2023).


{kind=link}
| Age Group | Females | Males | Total |
|---|---|---|---|
| 20–30 | 2 | 6 | 8 |
| 31–39 | 5 | 5 | 10 |
| 40–49 | 5 | 6 | 10 |
| 50–59 | 5 | 6 | 10 |
| 60–69 | 5 | 6 | 10 |
| 70–79 | 5 | 6 | 10 |
| Total | 27 | 31 | 58 |
| Skeletal Indicator | Method | % of Sample Over Age 60 * | Phase/Component |
|---|---|---|---|
| Pubic Symphysis | Suchey–Brooks [11] | 15% | Phase |
| Pubic Symphysis | Hartnett [16] | 40% | Phase |
| Auricular Surface | Lovejoy [12] | 13% | Phase |
| Auricular Surface | Buckberry–Chamberlain [17] | 48% | Component |
| Sternal Rib End | İşcan [13,14] | 19% | Phase |
| Sternal Rib End | Hartnett [18] | 40% | Phase |
| Phase | SBPS Males | SBPS Females | HNPS Males | HNPS Female | LJAS | BCAS |
|---|---|---|---|---|---|---|
| 1 | 0.02 | 0.38 | 0.52 | 0.59 | - | 0.88 |
| 2 | 0.42 | 0.71 | 0.50 | 1.06 | - | 2.74 |
| 3 | 0.91 | 1.22 | 1.11 | 1.02 | - | 2.79 |
| 4 | 0.72 | 1.75 | 1.01 | 1.03 | - | 2.56 |
| 5 | 0.90 | 2.20 | 0.89 | 0.70 | - | 1.62 |
| 6 | 0.87 | 1.74 | 1.38 | 1.24 | - | 1.86 |
| 7 | - | - | 0.95 | 0.99 | - | 3.67 |
| 8 | - | - | - | - | - | - |
| Phase | ISR Males | ISR Females | HNR Males | HNR Females | ||
| 1 | 0.25 | - | 0.32 | 0.63 | ||
| 2 | 0.59 | 0.68 | 0.38 | 0.44 | ||
| 3 | 0.85 | 0.74 | 0.71 | 0.68 | ||
| 4 | 1.11 | 1.46 | 0.43 | 0.67 | ||
| 5 | 1.93 | 2.96 | 0.40 | 0.59 | ||
| 6 | 2.71 | 3.52 | 0.45 | 0.80 | ||
| 7 | 2.31 | 2.81 | 0.76 | 0.82 | ||
| 8 | 2.97 | 2.66 | - | - |
| Paired Samples Test | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Paired Differences | t | df | Sig. (2-Tailed) | ||||||
| Mean | Std. Deviation | Std. Error Mean | 95% Confidence Interval of the Difference | ||||||
| Lower | Upper | ||||||||
| Pair 1 | Age—ISR | 1.2500 | 11.6590 | 1.5309 | −1.8156 | 4.3156 | 0.817 | 57 | 0.418 |
| Pair 2 | Age—HNR | −2.7328 | 12.4405 | 1.6335 | −6.0038 | 0.5383 | −1.673 | 57 | 0.100 |
| Pair 3 | Age—SBPS | 2.0000 | 15.4056 | 2.0229 | −2.0507 | 6.0507 | 0.989 | 57 | 0.327 |
| Pair 4 | Age—LJAS | 7.6810 | 14.2425 | 1.8701 | 3.9362 | 11.4259 | 4.107 | 57 | 0.000 |
| Pair 5 | Age—BCAS | −6.4397 | 14.0728 | 1.8479 | −10.1399 | −2.7394 | −3.485 | 57 | 0.001 |
| Pair 6 | Age—LEall | −1.1810 | 11.1145 | 1.4594 | −4.1034 | 1.7414 | −0.809 | 57 | 0.422 |
| Pair 7 | Age—LER | −2.7672 | 12.8838 | 1.6917 | −6.1549 | .6204 | −1.636 | 57 | 0.107 |
| Pair 8 | Age—LEPS | −0.6552 | 13.7883 | 1.8105 | −4.2806 | 2.9703 | −0.362 | 57 | 0.719 |
| Pair 9 | Age—LEAS | −6.4397 | 14.0728 | 1.8479 | −10.1399 | −2.7394 | −3.485 | 57 | 0.001 |
| Pair 10 | Age—TSR | −0.4138 | 12.5164 | 1.6435 | −3.7048 | 2.8772 | −0.252 | 57 | 0.802 |
| Pair 11 | Age—TSPS | −1.2586 | 14.3812 | 1.8883 | −5.0400 | 2.5227 | −0.667 | 57 | 0.508 |
| Pair 12 | Age—TSAS | −2.6638 | 14.9556 | 1.9638 | −6.5962 | 1.2686 | −1.356 | 57 | 0.180 |
| Pair 13 | Age—TSOL | −0.0086 | 10.1914 | 1.3382 | −2.6883 | 2.6711 | −0.006 | 57 | 0.995 |
| Pair 14 | Age—overlap | 0.1552 | 10.4748 | 1.3754 | −2.5990 | 2.9094 | 0.113 | 57 | 0.911 |
| Pair 15 | Age—experience | 0.6293 | 8.2921 | 1.0888 | −1.5510 | 2.8096 | 0.578 | 57 | 0.566 |
| Pair 16 | Age—HNPS | −2.0690 | 12.3702 | 1.6243 | −5.3215 | 1.1836 | −1.274 | 57 | 0.208 |
| Sample Group | Suchey–Brooks Pubic Symphysis | Hartnett Pubic Symphysis | İşcan Ribs | Hartnett Ribs | Lovejoy Auricular Surface | Buckberry–Chamberlain Auricular Surface |
|---|---|---|---|---|---|---|
| 20–39 | ||||||
| n = 18 | ||||||
| Accuracy | 89% | 67% | 78% | 39% | 22% | 78% |
| Inaccuracy | 8.81 | 9.53 | 7.00 | 8.92 | 8.89 | 19.00 |
| Bias | 0.47 | 8.36 | 2.06 | 6.53 | 5.33 | 16.06 |
| 40–59 | ||||||
| n = 20 | ||||||
| Accuracy | 95% | 80% | 70% | 35% | 25% | 85% |
| Inaccuracy | 14.10 | 11.25 | 10.08 | 10.78 | 7.95 | 12.07 |
| Bias | 7.35 | 4.60 | 1.68 | 2.73 | −6.15 | 9.48 |
| 60–79 | ||||||
| n = 20 | ||||||
| Accuracy | 70% | 85% | 90% | 50% | 15% | 100% |
| Inaccuracy | 15.58 | 9.28 | 10.00 | 9.18 | 20.93 | 7.85 |
| Bias | 10.68 | −6.13 | −7.15 | −0.68 | −20.93 | −5.25 |
| Males | ||||||
| n = 31 | ||||||
| Accuracy | 74% | 81% | 77% | 42% | 29% | 84% |
| Inaccuracy | 12.50 | 10.58 | 8.10 | 9.18 | 12.58 | 13.18 |
| Bias | 4.02 | −1.03 | −4.97 | 4.08 | −5.54 | 9.24 |
| Females | ||||||
| n = 27 | ||||||
| Accuracy | 96% | 74% | 82% | 41% | 11% | 93% |
| Inaccuracy | 13.50 | 9.41 | 10.24 | 9.44 | 12.87 | 12.30 |
| Bias | 9.06 | 5.63 | 3.02 | 1.19 | −10.13 | 3.30 |
| Total | ||||||
| n = 58 | ||||||
| Accuracy | 84% | 78% | 79% | 41% | 21% | 88% |
| Inaccuracy | 12.97 | 10.03 | 9.10 | 9.65 | 13.75 | 12.77 |
| Bias | 6.36 | 2.07 | −1.25 | 2.73 | −8.72 | 6.44 |
| Sample Group | Lowest Error All | Lowest Error Ribs | Lowest Error Pubic Symphysis | Lowest Error Auricular Surface | Two-Step Ribs | Two-Step Pubic Symphysis | Two-Step Auricular Surface | Overlap | Overlap Two-Step | Experience |
|---|---|---|---|---|---|---|---|---|---|---|
| 20–39 | ||||||||||
| n = 18 | ||||||||||
| Accuracy | 44% | 39% | 83% | 78% | 67% | 78% | 56% | 83% | 72% | 78% |
| Inaccuracy | 7.36 | 9.83 | 8.44 | 19.00 | 6.61 | 10.19 | 14.56 | 5.72 | 6.64 | 5.42 |
| Bias | 4.92 | 7.56 | 8.22 | 16.06 | 0.33 | 9.36 | 11.00 | 4.00 | 4.03 | 4.58 |
| 40–59 | ||||||||||
| n = 20 | ||||||||||
| Accuracy | 35% | 30% | 80% | 85% | 30% | 75% | 60% | 65% | 85% | 85% |
| Inaccuracy | 8.70 | 10.20 | 10.68 | 12.08 | 10.53 | 12.20 | 14.43 | 8.05 | 6.28 | 5.63 |
| Bias | 1.80 | 3.30 | 3.98 | 9.48 | 2.98 | 3.55 | 4.48 | 0.05 | 1.78 | −0.08 |
| 60–79 | ||||||||||
| n = 20 | ||||||||||
| Accuracy | 40% | 45% | 80% | 100% | 45% | 80% | 95% | 50% | 65% | 75% |
| Inaccuracy | 10.70 | 9.98 | 12.08 | 7.85 | 9.98 | 11.48 | 8.95 | 10.45 | 9.68 | 7.28 |
| Bias | −2.80 | −2.08 | −9.48 | −5.25 | −2.08 | −8.33 | −6.65 | −4.10 | −5.38 | −5.88 |
| Males | ||||||||||
| n = 31 | ||||||||||
| Accuracy | 42% | 42% | 87% | 88% | 48% | 77% | 61% | 61% | 71% | 71% |
| Inaccuracy | 8.58 | 10.02 | 10.82 | 13.18 | 9.45 | 12.68 | 13.50 | 8.86 | 8.42 | 7.19 |
| Bias | 1.84 | 3.37 | −3.47 | 9.24 | 0.58 | −2.87 | 4.82 | −4.68 | −0.61 | −0.84 |
| Females | ||||||||||
| n = 27 | ||||||||||
| Accuracy | 37% | 33% | 74% | 93% | 44% | 78% | 82% | 71% | 78% | 89% |
| Inaccuracy | 9.43 | 10.00 | 10.06 | 12.30 | 8.74 | 9.78 | 11.52 | 7.35 | 6.57 | 4.91 |
| Bias | 0.43 | 2.07 | 5.39 | 3.30 | 0.22 | 6.00 | 0.19 | 0.20 | 0.72 | −0.39 |
| Total | ||||||||||
| n = 58 | ||||||||||
| Accuracy | 40% | 38% | 81% | 88% | 47% | 78% | 71% | 66% | 74% | 80% |
| Inaccuracy | 8.97 | 10.01 | 10.47 | 12.77 | 9.12 | 11.33 | 12.58 | 8.16 | 7.56 | 6.13 |
| Bias | 1.18 | 2.77 | 0.66 | 6.44 | 0.41 | 1.26 | 2.66 | −0.16 | 0.01 | −0.63 |
| Sample Group | Accuracy | Inaccuracy | Bias | Accuracy, Inaccuracy, and Bias |
|---|---|---|---|---|
| 20–39 n = 18 | Suchey–Brooks Pubic Symphysis (89%) | Experience (5.42) | Two-Step Ribs (0.33) | Suchey–Brooks Pubic Symphysis (89%, 8.81, 0.47) |
| 40–59 n = 20 | Suchey–Brooks Pubic Symphysis (95%) | Experience (5.63) | İşcan Ribs (1.68) | Experience (85%, 5.63, −0.08) |
| 60–79 n = 20 | Buckberry–Chamberlain (100%) | Experience (7.28) | Hartnett Ribs (−0.33) | None |
| Males n = 31 | Buckberry–Chamberlain (88%) | Experience (7.19) | Two-Step Ribs (0.58) | None |
| Females n = 27 | Suchey–Brooks Pubic Symphysis (96%) | Experience (4.91) | Two-Step Auricular Surface (0.19) | Experience (89%, 4.91, −0.39) |
| Total n = 58 | Buckberry–Chamberlain (88%) | Experience (6.13) | Overlap Two-Step (0.01) | Experience (80%, 6.13, −0.63) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bailey, C.; Vidoli, G. Age-at-Death Estimation: Accuracy and Reliability of Common Age-Reporting Strategies in Forensic Anthropology. Forensic Sci. 2023, 3, 179-191. https://doi.org/10.3390/forensicsci3010014
Bailey C, Vidoli G. Age-at-Death Estimation: Accuracy and Reliability of Common Age-Reporting Strategies in Forensic Anthropology. Forensic Sciences. 2023; 3(1):179-191. https://doi.org/10.3390/forensicsci3010014
Chicago/Turabian StyleBailey, Christine, and Giovanna Vidoli. 2023. "Age-at-Death Estimation: Accuracy and Reliability of Common Age-Reporting Strategies in Forensic Anthropology" Forensic Sciences 3, no. 1: 179-191. https://doi.org/10.3390/forensicsci3010014
APA StyleBailey, C., & Vidoli, G. (2023). Age-at-Death Estimation: Accuracy and Reliability of Common Age-Reporting Strategies in Forensic Anthropology. Forensic Sciences, 3(1), 179-191. https://doi.org/10.3390/forensicsci3010014