


Comparison between Blood, Non-Blood Fluids and Tissue Specimens for the Analysis of Cannabinoid Metabolites in Cannabis-Related Post-Mortem Cases

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Case Study
2.2.1. Study Design
2.2.2. Specimens Collection
2.3. Sample Preparation
2.3.1. Non-Hydrolyzed Specimens
2.3.2. Solid Phase Extraction (SPE)
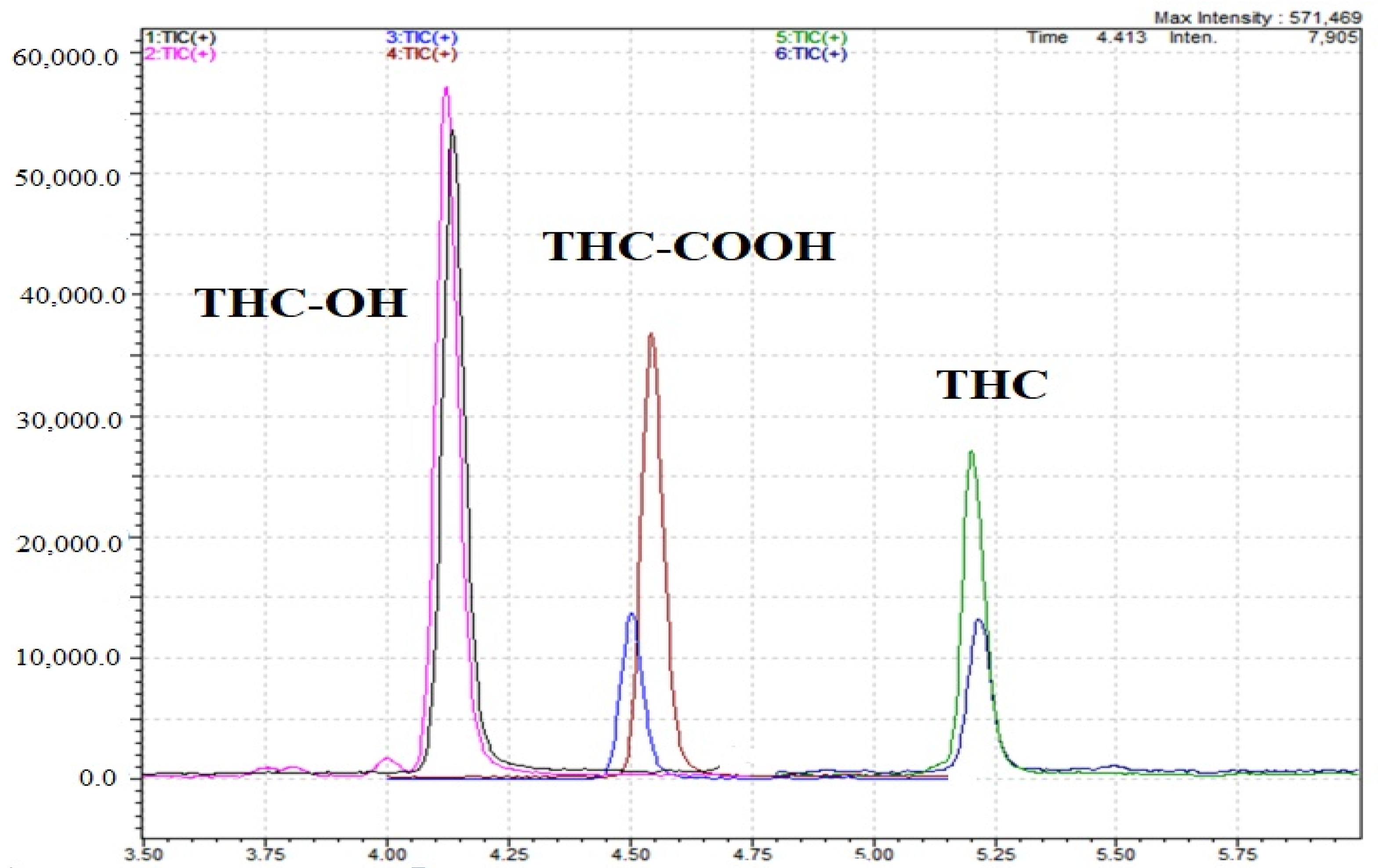
2.4. LC–MS/MS Conditions
2.5. Method Validation
3. Results
3.1. Demographic Profile (Table 2)
3.2. Multiple Specimens Analysis
3.3. THC in Different Specimens
3.4. THC-OOOH in Different Specimens
3.5. THC-OH in Different Specimens
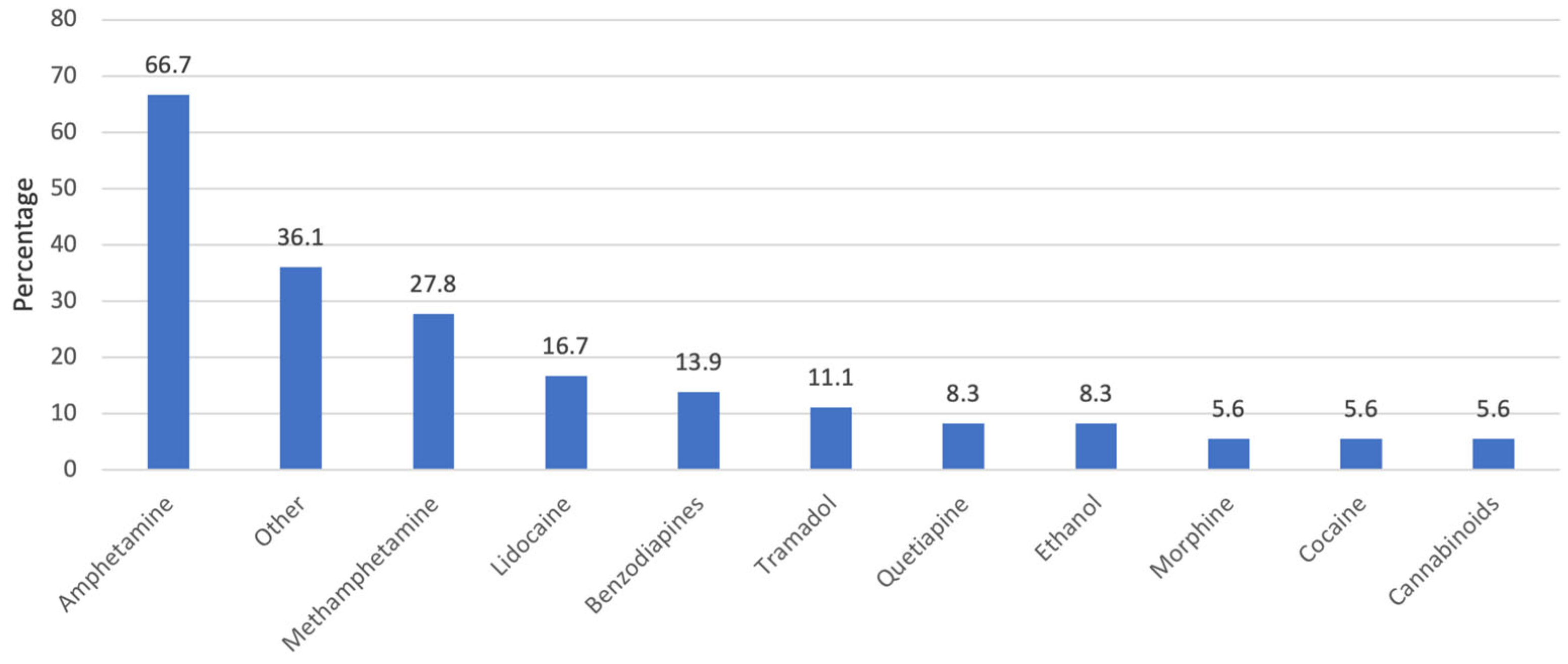
3.6. The Role of Other Drugs Detected
3.7. History of Drug Abuse
3.8. Body Mass Index and THC Metabolites
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nation Office on Drugs and Crime. World Drug Report 2022; United Nation Office on Drugs and Crime: Vienna, Austria, 2022. [Google Scholar]
- Cliburn, K.D.; Huestis, M.A.; Wagner, J.R.; Kemp, P.M. Cannabinoid Distribution in Fatally-Injured Pilots’ Postmortem Fluids and Tissues. Forensic Sci. Int. 2021, 329, 111075. [Google Scholar] [CrossRef]
- Lewis, B.; Fleeger, T.; Judge, B.; Riley, B.; Jones, J.S. Acute Toxicity Associated with Cannabis Edibles Following Decriminalization of Marijuana in Michigan. Am. J. Emerg. Med. 2021, 46, 732–735. [Google Scholar] [CrossRef]
- Shirah, B.H.; Ahmed, M.M. The Use of Cannabis for Medical Purposes in the Arab World. Med. Cannabis Cannabinoids 2021, 4, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Al-Asmari, A.I. Method for the Identification and Quantification of Sixty Drugs and Their Metabolites in Postmortem Whole Blood Using Liquid Chromatography Tandem Mass Spectrometry. Forensic Sci. Int. 2020, 309, 110193. [Google Scholar] [CrossRef] [PubMed]
- Drummer, O.H.; Gerostamoulos, D.; Woodford, N.W. Cannabis as a Cause of Death: A Review. Forensic Sci. Int. 2019, 298, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Hartung, B.; Kauferstein, S.; Ritz-Timme, S.; Daldrup, T. Sudden Unexpected Death under Acute Influence of Cannabis. Forensic Sci. Int. 2014, 237, e11–e13. [Google Scholar] [CrossRef]
- Cliburn, K.D.; Huestis, M.A.; Wagner, J.R.; Kemp, P.M. Identification and Quantification of Cannabinoids in Postmortem Fluids and Tissues by Liquid Chromatography-Tandem Mass Spectrometry. J. Chromatogr. A 2021, 1652, 462345. [Google Scholar] [CrossRef]
- Al-Asmari, A.I. Method for Postmortem Quantification of Δ9-Tetrahydrocannabinol and Metabolites Using LC-MS-MS. J. Anal. Toxicol. 2019, 43, 703–719. [Google Scholar] [CrossRef]
- Ashton, C.H. Pharmacology and Effects of Cannabis: A Brief Review. Br. J. Psychiatry 2001, 178, 101–106. [Google Scholar] [CrossRef]
- Saenz, S.R.; Lewis, R.J.; Angier, M.K.; Wagner, J.R. Postmortem Fluid and Tissue Concentrations of THC, 11-OH-THC and THC-COOH. J. Anal. Toxicol. 2017, 41, 508–516. [Google Scholar] [CrossRef]
- Lemos, N.P.; Ingle, E.A. Cannabinoids in Postmortem Toxicology. J. Anal. Toxicol. 2011, 35, 394–401. [Google Scholar] [CrossRef]
- Gronewold, A.; Skopp, G. A Preliminary Investigation on the Distribution of Cannabinoids in Man. Forensic Sci. Int. 2011, 210, e7–e11. [Google Scholar] [CrossRef]
- Al-Asmari, A.I. Method for Postmortem Tissue Quantification of Δ9-Tetrahydrocannabinol and Metabolites Using LC–MS-MS. J. Anal. Toxicol. 2020, 44, 718–733. [Google Scholar] [CrossRef] [PubMed]
- Kemp, P.M.; Cardona, P.S.; Chaturvedi, A.K.; Soper, J.W. Distribution of Δ9-Tetrahydrocannabinol and 11-Nor-9-Carboxy-Δ9-Tetrahydrocannabinol Acid in Postmortem Biological Fluids and Tissues From Pilots Fatally Injured in Aviation Accidents. J. Forensic Sci. 2015, 60, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Musshoff, F.; Madea, B. Review of Biologic Matrices (Urine, Blood, Hair) as Indicators of Recent or Ongoing Cannabis Use. Ther. Drug Monit. 2006, 28, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Singer, R. The Forensic Pharmacology of Drugs of Abuse. Int. J. Toxicol. 2002, 21, 436–437. [Google Scholar] [CrossRef]
- Maskell, P.D.; Wilson, N.E.; Seetohul, L.N.; Crichton, M.L.; Beer, L.J.; Drummond, G.; De Paoli, G. Postmortem Tissue Distribution of Morphine and Its Metabolites in a Series of Heroin-Related Deaths. Drug Test. Anal. 2019, 11, 292–304. [Google Scholar] [CrossRef]
- ANSI/ASB Standard 036; American Academy of Forensic Sciences Standards Board 2019. Method Validation in Forensic Toxicology. American Academy Forensic Sciences (AAFS): Colorado Springs, CO, USA, 2019.
- Peters, F.T.; Drummer, O.H.; Musshoff, F. Validation of New Methods. Forensic Sci. Int. 2007, 165, 216–224. [Google Scholar] [CrossRef]
- Antunes, M.; Barroso, M.; Gallardo, E. Analysis of Cannabinoids in Biological Specimens: An Update. Int. J. Environ. Res. Public Health 2023, 20, 2312. [Google Scholar] [CrossRef]
- Kemp, P.M.; Abukhalaf, I.K.; Manno, J.E.; Manno, B.R.; Alford, D.D.; Mc Williams, M.E.; Nixon, F.E.; Fitzgerald, M.J.; Reeves, R.R.; Wood, M.J. Cannabinoids in Humans. Ii. the Influence of Three Methods of Hydrolysis on the Conentration of Thc and Two Metabolites in Urine. J. Anal. Toxicol. 1995, 19, 292–298. [Google Scholar] [CrossRef]
- Pettersen, S.; Øiestad, Å.M.L.; Rogde, S.; Brochmann, G.W.; Øiestad, E.L.; Vindenes, V. Distribution of Tetrahydrocannabinol and Cannabidiol in Several Different Postmortem Matrices. Forensic Sci. Int. 2021, 329, 111082. [Google Scholar] [CrossRef] [PubMed]
- Kudo, K.; Nagata, T.; Kimura, K.; Imamura, T.; Jitsufuchi, N. Sensitive Determination of ∆9-Tetrahydrocannabinol in Human Tissues by Gc-Ms. J. Anal. Toxicol. 1995, 19, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Duflou, J.; Darke, S.; Easson, J. Morphine Concentrations in Stomach Contents of Intravenous Opioid Overdose Deaths. J. Forensic Sci. 2009, 54, 1181–1184. [Google Scholar] [CrossRef] [PubMed]
- Moriya, F.; Hashimoto, Y. Distribution of Free and Conjugated Morphine in Body Fluids and Tissues in a Fatal Heroin Overdose: Is Conjugated Morphine Stable in Postmortem Specimens? J. Forensic Sci. 1997, 42, 736–740. [Google Scholar] [CrossRef]
- Mura, P.; Kintz, P.; Dumestre, V.; Raul, S.; Hauet, T. THC Can Be Detected in Brain While Absent in Blood. J. Anal. Toxicol. 2005, 29, 842–843. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameters | Δ9—Tetrahydrocannabinol (THC) | 11-nor-Δ9-THC-9-Carboxy Acid | 11-Hydroxy-Δ9-THC | |
|---|---|---|---|---|
| Analytes | Precursor Ion (m/z) | 315 | 345 | 331 |
| Product Ion(s) (m/z) | 193, 123, 93 | 193, 299, 119 | 193, 201, 123 | |
| Quantifier Ion (m/z) | 315.0→123 | 345→193 | 331→193 | |
| Qualifier Ion (m/z) | 315→193 | 345→123 | 331→201 | |
| Reference ion ratios | 63 | 70 | 69 | |
| Retention time (Min) | 5.7 | 5.0 | 4.8 | |
| Internal standards | Internal Standard (IS) | THC-d3 | THC-COOH-d9 | THC-OH-d3 |
| IS Precursor Ion(s) (m/z) | 318 | 354 | 334 | |
| Product Ion (m/z) | 198, 123, 107 | 197, 123, 308 | 196, 201, 105 | |
| Quantifier Ion (m/z) | 318→123 | 354→197 | 334→196 | |
| Analytes and their internal standards | Dwell time (msec) | 10 | 10 | 10 |
| Q1 Bias (V) | −15 | −15 | −15 | |
| Collision energy (%) | −35 | −35 | −35 | |
| Q3 Bias (V) | −15 | −15 | −15 | |
| Nebulizing Gas Flow (L/Min) | 3 | 3 | 3 | |
| Interface Temperature °C | 300 | 300 | 300 | |
| Heater Block Temperature °C | 400 | 400 | 400 |
| Study Data | N (%) |
|---|---|
| Age in years (mean ± SD) | 32.1 ± 11.9 |
| Gender | |
| Male | 40 (93.0%) |
| Female | 03 (07.0%) |
| BMI level | |
| Normal (18.5–24.9 kg/m2) | 20 (46.5%) |
| Overweight (25–29.9 kg/m2) | 16 (37.2%) |
| Obese (≥30 kg/m2) | 07 (16.3%) |
| Previous history of drug abuse | |
| Yes | 08 (18.6%) |
| No | 35 (81.4%) |
| Use of other drugs | |
| Yes | 36 (83.7%) |
| No | 07 (16.3%) |
| Variables | Δ9—Tetrahydrocannabinol (ng/mL)/(ng/g) Mean (95% CI) | 11-nor—Δ9-THC-9-Carboxy Acid (ng/mL)/(ng/g) Mean (95% CI) | 11-Hydroxy-Δ9-THC (ng/mL)/(ng/g) Mean (95% CI) |
|---|---|---|---|
| Blood | 13.1 (−9.2–33.8) a | 17.1 (6.48–29.5) | 1.61 (−0.07–1.43) |
| Urine | 4.39 (−2.5–19.6) a | 383.6 (27.7–765) a | 0.62 (0.02–1.11) |
| Liver | 1.71 (0.88–2.47) | 80.6 (−24.7–199) a | 0.79 (0.04–1.27) |
| VH | 0.98 (−0.02–2.04) | 0.89 (−0.02–2.04) | 0.46 (−0.05–1.16) |
| Kidney | 3.39 (−2.66–13.7) | 118.8 (−2.66–13.7) | 0.63 (0.22–1.32) |
| Bile | 106.1 (−14.3–226) a | 8808.6 (1684 15932) a | 9.47 (4.97–13.9) |
| Gastric Contents | 80.9 (−41.7–121) | 68.3 (−41.7–121) | 3.51 (−1.06–4.96) |
| Brain | 2.02 (0.21–3.83) | 1.15 (−0.65–1.66) | 0.72 (−0.02–1.46) a |
| Specimens | Blood | Urine | Liver | VH |
|---|---|---|---|---|
| Blood | 1 | |||
| Urine | 0.444 ** | 1 | ||
| Liver | 0.709 * | 0.562 | 1 | |
| VH | 0.401 * | 0.461 * | 0.683 * | 1 |
| Kidney | 0.510 | 0.765 * | 0.828 ** | 0.500 |
| Bile | 0.243 | 0.053 | 0.203 | −0.147 |
| Gastric contents | 0.320 | 0.053 | −0.012 | −0.165 |
| Brain | −0.500 | -- | −0.500 | -- |
| Specimens | Blood | Urine | Liver | VH |
|---|---|---|---|---|
| Blood | 1 | |||
| Urine | 0.641 ** | 1 | ||
| Liver | 0.882 ** | 0.761 ** | 1 | |
| VH | 0.182 | −0.014 | 0.517 | 1 |
| Kidney | 0.817 ** | 0.460 | 0.895 ** | 0.214 |
| Bile | 0.404 | 0.216 | 0.735 ** | 0.273 |
| Gastric contents | 0.353 | 0.300 | 0.571 | −0.341 |
| Brain | -- | -- | 0.500 | -- |
| Specimens | Blood | Urine | Liver | VH |
|---|---|---|---|---|
| Blood | 1 | |||
| Urine | 0.715 ** | 1 | ||
| Liver | 0.561 | 0.908 ** | 1 | |
| VH | 0.716 ** | 0.790 ** | 0.673 * | 1 |
| Kidney | 0.357 | 0.678 * | 0.873 ** | 0.565 |
| Bile | 0.423 | 0.424 | 0.014 | 0.509 |
| Gastric contents | 0.388 | 0.519 * | 0.171 | 0.588 * |
| Brain | -- | -- | 0.500 | -- |
| Use of Other Drugs | t-Test | p-Value | ||
|---|---|---|---|---|
| Metabolites | ||||
| Specimens | Yes Mean ± SD | No Mean ± SD | ||
| Δ9—Tetrahydrocannabinol | ||||
| Blood a | 14.6 ± 49.4 | 4.94 ± 2.01 | 0.473 | 0.091 |
| Urine a | 4.29 ± 8.99 | 5.22 ± 3.77 | −0.201 | 0.222 |
| Liver b | 2.11 ± 0.61 | −0.621 | 0.545 | |
| VH b | 1.61 ± 1.34 | 0.79 ± 0.89 | 0.557 | 0.582 |
| Kidney b | 1.81 ± 2.17 | 12.1 ± 5.63 | −5.014 | <0.001 ** |
| Bile a | 94.4 ± 236.7 | 293.3 ± 0 | −0.815 | 0.235 |
| Gastric Contents b | 68.6 ± 96.8 | 185.9 ± 45.9 | −1.660 | 0.115 |
| 11-nor—Δ9-Tetrahydrocannabinol-9-Carboxy acid | ||||
| Blood b | 15.4 ± 16.1 | 26.9 ± 16.8 | −1.599 | 0.118 |
| Urine a | 379.9 ± 686.3 | 416.6 ± 435.7 | −0.095 | 0.620 |
| Liver a | 69.6 ± 148.2 | 124.7 ± 75.4 | −0.612 | 0.136 |
| VH b | 0.92 ± 0.56 | 0.75 ± 0.55 | 0.622 | 0.539 |
| Kidney b | 54.8 ± 148.7 | 471.3 ± 565.3 | −2.444 | 0.033 ** |
| Bile a | 8723.4 ± 14305.9 | 10,172.9 ± 0 | −0.098 | 0.588 |
| Gastric Contents b | 72.4 ± 237.9 | 31.6 ± 2.21 | 0.237 | 0.816 |
| 11-Hydroxy-Δ9-Tetrahydrocannabinol | ||||
| Blood b | 1.77 ± 5.67 | 0.71 ± 0.73 | 0.452 | 0.654 |
| Urine b | 0.63 ± 0.61 | 0.53 ± 0.62 | 0.308 | 0.760 |
| Liver b | 0.68 ± 0.51 | 1.28 ± 1.12 | −1.475 | 0.164 |
| VH b | 0.48 ± 0.46 | 0.39 ± 0.44 | 0.416 | 0.680 |
| Kidney b | 0.65 ± 0.43 | 0.49 ± 0.70 | 0.433 | 0.674 |
| Gastric contents b | 3.09 ± 8.09 | 7.24 ± 10.2 | −0.676 | 0.507 |
| Specimens | History of Drug Abuse | t-Test | p-Value |
|---|---|---|---|
| Metabolites | |||
| Yes Mean ± SD | No Mean ± SD | ||
| Δ9—Tetrahydrocannabinol | |||
| Blood a | 5.53 ± 4.88 | 14.7 ± 50.1 | −0.481 |
| Urine a | 4.22 ± 4.43 | 4.44 ± 9.32 | −0.059 |
| Liver b | 1.65 ± 1.16 | 1.72 ± 1.26 | −0.081 |
| VH b | 0.97 ± 0.84 | 0.98 ± 0.80 | −0.019 |
| Kidney b | 1.44 ± 1.00 | 3.76 ± 4.99 | −0.632 |
| Bile a | 83.3 ± 111.1 | 113.1 ± 264.3 | −0.216 |
| Gastric contents b | 30.9 ± 37.6 | 98.8 ± 108.8 | −1.345 |
| 11-nor—Δ9-Tetrahydrocannabinol-9-Carboxy acid | |||
| Blood b | 22.2 ± 19.4 | 16.0 ± 15.9 | 0.900 |
| Urine a | 705.3 ± 1325.0 | 308.5 ± 381.4 | 1.456 |
| Liver a | 145.8 ± 125.2 | 64.3 ± 139.1 | 0.922 |
| VH b | 1.06 ± 0.48 | 0.85 ± 0.57 | 0.811 |
| Kidney b | 250.8 ± 352.4 | 94.9 ± 258.6 | 0.756 |
| Bile a | 16,320.2 ± 17,012.6 | 6497.4 ± 12,610.9 | 1.263 |
| Gastric contents b | 235.6 ± 438.5 | 12.6 ± 26.7 | 2.076 |
| 11-Hydroxy-Δ9-Tetrahydrocannabinol | |||
| Blood b | 0.89 ± 0.71 | 1.76 ± 0.76 | −0.393 |
| Urine b | 0.77 ± 0.85 | 0.59 ± 0.54 | 0.710 |
| Liver b | 1.10 ± 0.88 | 0.72 ± 0.63 | 0.877 |
| VH b | 0.59 ± 0.46 | 0.43 ± 0.45 | 0.801 |
| Kidney b | 0.47 ± 0.62 | 10.2 ± 8.79 | −0.518 |
| Gastric contents b | 0.67 ± 1.08 | 4.45 ± 9.23 | −0.585 |
| Specimens | Level of BMI | F-Test | p-Value | ||
|---|---|---|---|---|---|
| Metabolites | |||||
| Normal Mean ± SD | Overweight Mean ± SD | Obese Mean ± SD | |||
| Δ9—Tetrahydrocannabinol | |||||
| Blood a | 17.0 ± 62.0 | 12.3 ± 26.3 | 3.97 ± 1.85 | 0.205 | 0.463 |
| Urine a | 2.36 ± 2.74 | 8.41 ± 14.1 | 2.75 ± 2.66 | 2.081 | 0.248 |
| Liver b | 0.88 ± 0.66 | 2.18 ± 1.16 | 1.87 ± 2.19 | 1.994 | 0.179 |
| VH b | 0.67 ± 0.74 | 1.14 ± 0.84 | 1.22 ± 0.74 | 1.516 | 0.237 |
| Kidney b | 0.95 ± 0.98 | 5.19 ± 5.99 | 4.14 ± 5.03 | 0.587 | 0.569 |
| Bile a | 81.4 ± 100.0 | 88.5 ± 105.2 | 1.95 ± 0 | 0.322 | 0.175 |
| 11-nor—Δ9-Tetrahydrocannabinol-9-Carboxy acid | |||||
| Blood b | 18.2 ± 16.7 | 20.3 ± 18.9 | 8.48 ± 7.63 | 1.253 | 0.298 |
| Urine a | 285.3 ± 313.8 | 673.8 ± 1052.2 | 138.9 ± 177.7 | 1.941 | 0.219 |
| Liver a | 64.5 ± 96.2 | 110.5 ± 169.9 | 1.04 ± 1.27 | 0.530 | 0.389 |
| VH b | 0.74 ± 0.66 | 0.96 ± 0.51 | 1.03 ± 0.44 | 0.755 | 0.479 |
| Kidney b | 115.9 ± 216.0 | 160.3 ± 349.3 | 2.03 ± 2.85 | 0.236 | 0.794 |
| Bile a | 134.2 ± 357.1 | 28.9 ± 39.9 | 2.09 ± 1.09 | 0.554 | 0.113 |
| 11-Hydroxy-Δ9-Tetrahydrocannabinol | |||||
| Blood b | 2.24 ± 7.48 | 1.12 ± 0.96 | 0.81 ± 0.57 | 0.269 | 0.766 |
| Urine b | 0.33 ± 0.43 | 0.94 ± 0.72 | 0.82 ± 0.44 | 5.087 | 0.012 ** |
| Liver b | 0.48 ± 0.36 | 1.04 ± 0.75 | 0.63 ± 0.88 | 1.186 | 0.339 |
| VH b | 0.24 ± 0.39 | 0.58 ± 0.45 | 0.63 ± 0.42 | 2.778 | 0.079 |
| Kidney b | 0.55 ± 0.47 | 0.71 ± 0.40 | 0.56 ± 0.78 | 0.172 | 0.844 |
| Gastric contents b | 5.62 ± 12.0 | 2.42 ± 4.33 | 0.46 ± 0.65 | 0.475 | 0.630 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zughaibi, T.A.; Al-Qumsani, L.; Mirza, A.A.; Almostady, A.; Basrawi, J.; Tabrez, S.; Alsolami, F.; Al-Makki, R.; Al-Ghamdi, S.; Al-Ghamdi, A.; et al. Comparison between Blood, Non-Blood Fluids and Tissue Specimens for the Analysis of Cannabinoid Metabolites in Cannabis-Related Post-Mortem Cases. Forensic Sci. 2023, 3, 330-344. https://doi.org/10.3390/forensicsci3020025
Zughaibi TA, Al-Qumsani L, Mirza AA, Almostady A, Basrawi J, Tabrez S, Alsolami F, Al-Makki R, Al-Ghamdi S, Al-Ghamdi A, et al. Comparison between Blood, Non-Blood Fluids and Tissue Specimens for the Analysis of Cannabinoid Metabolites in Cannabis-Related Post-Mortem Cases. Forensic Sciences. 2023; 3(2):330-344. https://doi.org/10.3390/forensicsci3020025
Chicago/Turabian StyleZughaibi, Torki A., Latifa Al-Qumsani, Ahmed A. Mirza, Amal Almostady, Jude Basrawi, Shams Tabrez, Faiz Alsolami, Rami Al-Makki, Sami Al-Ghamdi, Abdullah Al-Ghamdi, and et al. 2023. "Comparison between Blood, Non-Blood Fluids and Tissue Specimens for the Analysis of Cannabinoid Metabolites in Cannabis-Related Post-Mortem Cases" Forensic Sciences 3, no. 2: 330-344. https://doi.org/10.3390/forensicsci3020025
APA StyleZughaibi, T. A., Al-Qumsani, L., Mirza, A. A., Almostady, A., Basrawi, J., Tabrez, S., Alsolami, F., Al-Makki, R., Al-Ghamdi, S., Al-Ghamdi, A., Alzahrani, A. E., Altowairqi, M., Alharbi, H., Peace, M. R., Halwani, M. A., & Al-Asmari, A. I. (2023). Comparison between Blood, Non-Blood Fluids and Tissue Specimens for the Analysis of Cannabinoid Metabolites in Cannabis-Related Post-Mortem Cases. Forensic Sciences, 3(2), 330-344. https://doi.org/10.3390/forensicsci3020025