
Association between Menstrual Hygiene Management and School Performance among the School-Going Girls in Rural Bangladesh

 ,
, 
 ,
,
Abstract
:1. Background
2. Materials and Methods
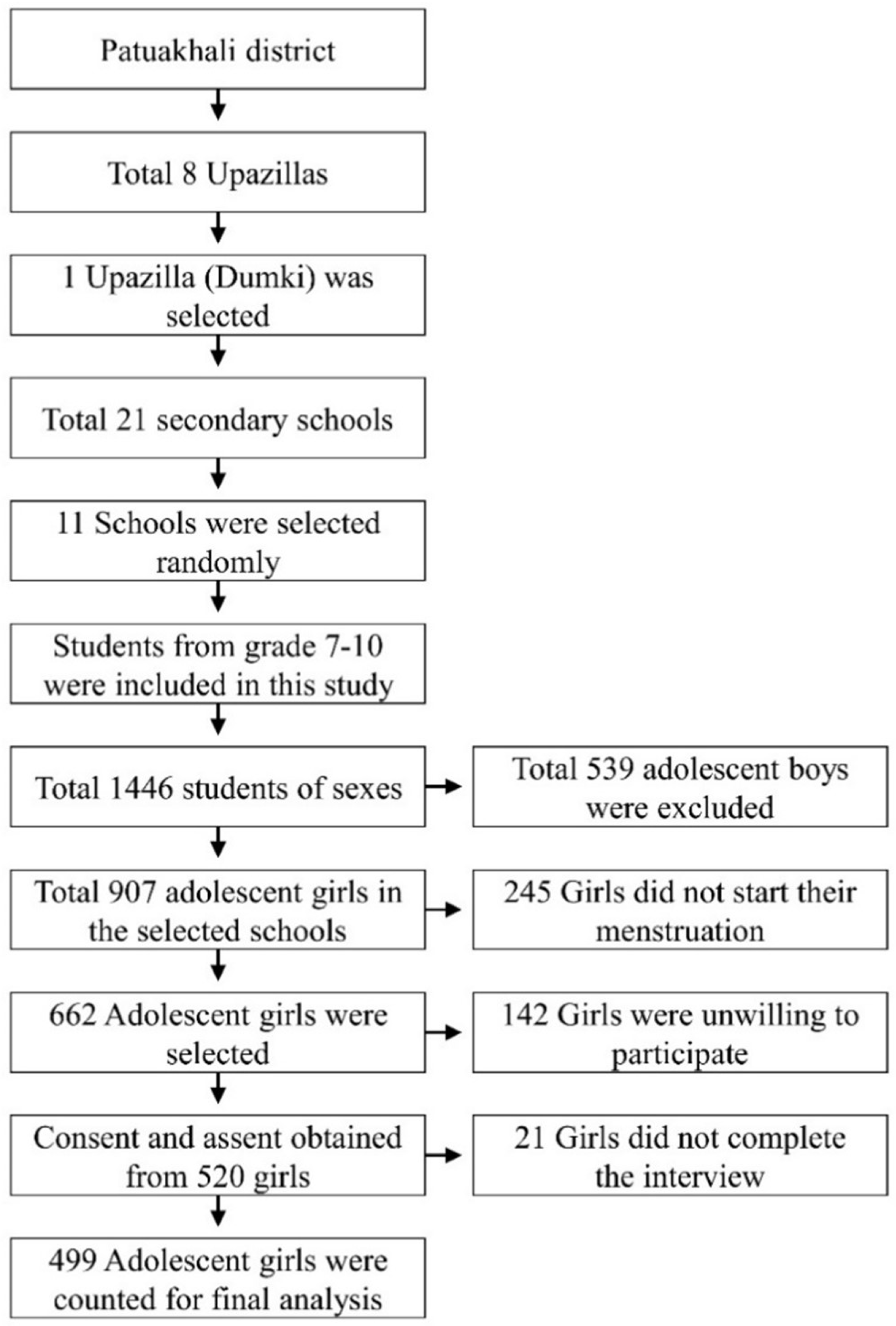
2.1. Study Design and Participants
2.2. Sample Size and Sampling
2.3. Data Collection Tools and Technique
2.4. Outcome Measurement
2.5. Explanatory Variables
2.6. Statistical Analysis
2.7. Ethical Consideration
3. Results
3.1. Background Characteristics and the Girls Based on the School Performance
3.2. Menstrual Information of the Adolescent Girls and Association with MHM
3.3. Association of Menstruation Hygiene Management and School Performance
3.4. Association between Socio-Demographic Variables and School Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hennegan, J.; Shannon, A.K.; Rubli, J.; Schwab, K.J.; Melendez-Torres, G.J. Women’s and girls’ experiences of menstruation in low- and middle-income countries: A systematic review and qualitative metasynthesis. PLoS Med. 2019, 16, e1002803. [Google Scholar] [CrossRef] [Green Version]
- McMahon, S.A.; Winch, P.J.; Caruso, B.A.; Obure, A.F.; Ogutu, E.A.; Ochari, I.S.; Rheingans, R.D. ‘The girl with her period is the one to hang her head’ Reflections on menstrual management among schoolgirls in rural Kenya. BMC Int. Health Hum. Rights 2011, 11, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, M.S. Impact Assessment of Adolescent Peer Organised Network on Attitudes and Behaviour Change of Adolescents in Rural Bangladesh. Ph.D. Thesis, University of Western Australia, Perth, Australia, 2015. [Google Scholar]
- Tegegne, T.K.; Sisay, M.M. Menstrual hygiene management and school absenteeism among female adolescent students in Northeast Ethiopia. BMC Public Health 2014, 14, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Dambhare, D.G.; Wagh, S.V.; Dudhe, J.Y. Age at Menarche and Menstrual Cycle Pattern among School Adolescent Girls in Central India. Glob. J. Health Sci. 2011, 4, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Ibitoye, M.; Choi, C.; Tai, H.; Lee, G.; Sommer, M. Early menarche: A systematic review of its effect on sexual and reproductive health in low- and middle-income countries. PLoS ONE 2017, 12, e0178884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, J.; MacIntyre, A.; Odagiri, M.; Suriastini, W.; Cordova, A.; Huggett, C.; Agius, P.A.; Faiqoh; Budiyani, A.E.; Quillet, C.; et al. Menstrual hygiene management and school absenteeism among adolescent students in Indonesia: Evidence from a cross-sectional school-based survey. Trop. Med. Int. Health 2018, 23, 1350–1363. [Google Scholar] [CrossRef] [PubMed]
- Korir, E.; Okwara, F.N.; Okumbe, G. Menstrual hygiene management practices among primary school girls from a pastoralist community in Kenya: A cross sectional survey. Pan Afr. Med. J. 2018, 31, 222. [Google Scholar] [CrossRef]
- Mumtaz, Z.; Sivananthajothy, P.; Bhatti, A.; Sommer, M. “How can we leave the traditions of our Baab Daada” socio-cultural structures and values driving menstrual hygiene management challenges in schools in Pakistan. J. Adolesc. 2019, 76, 152–161. [Google Scholar] [CrossRef]
- Oster, E.; Thornton, R. Menstruation, Sanitary Products, and School Attendance: Evidence from a Randomized Evaluation. Am. Econ. J. Appl. Econ. 2011, 3, 91–100. [Google Scholar] [CrossRef] [Green Version]
- Adams, J.; Bartram, J.; Chartier, Y.; Sims, J. Water, Sanitation and Hygiene Standards for Schools in Low-Cost Settings; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Vashisht, A.; Pathak, R.; Agarwalla, R.; Patavegar, B.N.; Panda, M. School absenteeism during menstruation amongst adolescent girls in Delhi, India. J. Fam. Community Med. 2018, 25, 163–168. [Google Scholar] [CrossRef]
- Alexander, K.T.; Oduor, C.; Nyothach, E.; Laserson, K.F.; Amek, N.; Eleveld, A.; Mason, L.; Rheingans, R.; Beynon, C.; Mohammed, A.; et al. Water, Sanitation and Hygiene Conditions in Kenyan Rural Schools: Are Schools Meeting the Needs of Menstruating Girls? Water 2014, 6, 1453–1466. [Google Scholar] [CrossRef]
- Miiro, G.; Rutakumwa, R.; Nakiyingi-Miiro, J.; Nakuya, K.; Musoke, S.; Namakula, J.; Francis, S.; Torondel, B.; Gibson, L.J.; Ross, D.A.; et al. Menstrual health and school absenteeism among adolescent girls in Uganda (MENISCUS): A feasibility study. BMC Womens Health 2018, 18, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Jewitt, S.; Ryley, H. It’s a girl thing: Menstruation, school attendance, spatial mobility and wider gender inequalities in Kenya. Geoforum 2014, 56, 137–147. [Google Scholar] [CrossRef]
- Hutton, G.; Chase, C. The Knowledge Base for Achieving the Sustainable Development Goal Targets on Water Supply, Sanitation and Hygiene. Int. J. Environ. Res. Public Health 2016, 13, 536. [Google Scholar] [CrossRef] [Green Version]
- WEDC. Menstruation Hygiene Management for Schoolgirls, Guide 18; Water, Engineering and Development Centre (WEDC), Loughborough University: Leicestershire, UK, 2014. [Google Scholar]
- McCammon, E.; Bansal, S.; Hebert, L.E.; Yan, S.; Menendez, A.; Gilliam, M. Exploring young women’s menstruation-related challenges in Uttar Pradesh, India, using the socio-ecological framework. Sex. Reprod. Health Matters 2020, 28, 1749342. [Google Scholar] [CrossRef] [PubMed]
- UN. Sustainable Development Goals; UN: New York, NY, USA, 2015.
- Sumpter, C.; Torondel, B. A Systematic Review of the Health and Social Effects of Menstrual Hygiene Management. PLoS ONE 2013, 8, e62004. [Google Scholar] [CrossRef] [Green Version]
- Mahon, T.; Fernandes, M. Menstrual hygiene in South Asia: A neglected issue for WASH (water, sanitation and hygiene) programmes. Gend. Dev. 2010, 18, 99–113. [Google Scholar] [CrossRef]
- Hennegan, J.; Montgomery, P. Do Menstrual Hygiene Management Interventions Improve Education and Psychosocial Outcomes for Women and Girls in Low and Middle Income Countries? A Systematic Review. PLoS ONE 2016, 11, e0146985. [Google Scholar] [CrossRef] [Green Version]
- Kansiime, C.; Hytti, L.; Nalugya, R.; Nakuya, K.; Namirembe, P.; Nakalema, S.; Neema, S.; Tanton, C.; Alezuyo, C.; Musoke, S.N.; et al. Menstrual health intervention and school attendance in Uganda (MENISCUS-2): A pilot intervention study. BMJ Open 2020, 10, e031182. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.-U.; Luby, S.P.; Halder, A.K.; Islam, K.; Opel, A.; Shoab, A.K.; Ghosh, P.K.; Rahman, M.; Mahon, T.; Unicomb, L. Menstrual hygiene management among Bangladeshi adolescent schoolgirls and risk factors affecting school absence: Results from a cross-sectional survey. BMJ Open 2017, 7, e015508. [Google Scholar] [CrossRef] [PubMed]
- Haque, S.E.; Rahman, M.; Itsuko, K.; Mutahara, M.; Sakisaka, K. The effect of a school-based educational intervention on menstrual health: An intervention study among adolescent girls in Bangladesh. BMJ Open 2014, 4, e004607. [Google Scholar] [CrossRef] [Green Version]
- Cite This: MICS. Designing and Selecting the Sample. Multiple Indicator Cluster Survey, United Nations Chi dren’s Emergency Fund. Available online: https://mics.unicef.org/files?job=W1siZiIsIjIwMTvMDQvMDIvMDgvMDAvMTkvODEwL01JQ1MzX0NoYXB0ZXJfNF9fX0Rlc2lnbmluZ19hbmRfU2VsZWN0aW5nX3RoZV9TYW1wbGVfMDYwMjE5LnBkZiJdXQ&sha=3d97a05358bb0e37 (accessed on 7 August 2021).
- Tang, S.-F.; Wang, X.; Zhang, Y.; Hou, J.; Ji, L.; Wang, M.-L.; Huang, R. Analysis of high alert medication knowledge of medical staff in Tianjin: A convenient sampling survey in China. Acta Acad. Med. Wuhan 2015, 35, 176–182. [Google Scholar] [CrossRef] [PubMed]
- WHO/UNICEF. Consultation on Draft Long List of Goal, Target and Indicator Options for Future Global Monitoring of Water, Sanitation and Hygiene. 2012. Available online: https://washdata.org/sites/default/files/documents/%0Areports/2017-06/JMP-2012-post2015-consultation.pdf (accessed on 15 January 2021).
- Johnson, R.; Wichern, D. Applied Multivariate Analysis, 6th ed.; Pearson Education Inc.: Hoboken, NJ, USA, 2007. [Google Scholar]
- House, S.; Mahon, T.; Cavill, S. Menstrual hygiene matters: A resource for improving menstrual hygiene around the world. Reprod. Health Matters 2013, 21, 257–259. [Google Scholar]
- Rutstein, S.O. Steps to Constructing the New DHS Wealth Index; ICF International: Rockville, MD, USA, 2015. [Google Scholar]
- Bobhate, P.; Shrivastava, S. A cross sectional study of knowledge and practices about reproductive health among female adolescents in an urban slum of Mumbai. J. Fam. Reprod. Health 2011, 5, 117–124. [Google Scholar]
- Mishra, S.K.; Dasgupta, D.; Ray, S. A study on the relationship of sociocultural characteristics, menstrual hygiene practices and gynaecological problems among adolescent girls in Eastern India. Int. J. Adolesc. Med. Health 2016, 29. [Google Scholar] [CrossRef]
- Kerubo, E.; Laserson, K.F.; Otecko, N.; Odhiambo, C.; Mason, L.; Nyothach, E.; Oruko, K.O.; Bauman, A.; Vulule, J.; Zeh, C.; et al. Prevalence of reproductive tract infections and the predictive value of girls’ symptom-based reporting: Findings from a cross-sectional survey in rural western Kenya. Sex. Transm. Infect. 2016, 92, 251–256. [Google Scholar] [CrossRef] [Green Version]
- Winkler, I.; Roaf, V. Bringing the Dirty Bloody Linen Out of the Closet–Menstrual Hygiene as a Priority for Achieving Gender Equality. Cardozo J. Law Gend. 2015. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2575250 (accessed on 15 January 2021).
- Mohammed, S.; Larsen-Reindorf, R.E.; Awal, I. Menstrual Hygiene Management and School Absenteeism among Adolescents in Ghana: Results from a School-Based Cross-Sectional Study in a Rural Community. Int. J. Reprod. Med. 2020, 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sivakami, M.; Van Eijk, A.M.; Thakur, H.; Kakade, N.; Patil, C.; Shinde, S.; Surani, N.; Bauman, A.; Zulaika, G.; Kabir, Y.; et al. Effect of menstruation on girls and their schooling, and facilitators of menstrual hygiene management in schools: Surveys in government schools in three states in India, 2015. J. Glob. Health 2018, 9, 010408. [Google Scholar] [CrossRef] [PubMed]
- Sudeshna, R.; Aparajita, D. Determinants of menstrual hygiene among adolescent girls: A multivariate analysis. Natl. J. Community Med. 2012, 3, 294–301. [Google Scholar]
- Hennegan, J.; Dolan, C.; Steinfield, L.; Montgomery, P. A qualitative understanding of the effects of reusable sanitary pads and puberty education: Implications for future research and practice. Reprod. Health 2017, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sommer, M. Where the education system and women’s bodies collide: The social and health impact of girls’ experiences of menstruation and schooling in Tanzania. J. Adolesc. 2010, 33, 521–529. [Google Scholar] [CrossRef]
- Montgomery, P.; Hennegan, J.; Dolan, C.; Wu, M.; Steinfield, L.; Scott, L. Menstruation and the Cycle of Poverty: A Cluster Quasi-Randomised Control Trial of Sanitary Pad and Puberty Education Provision in Uganda. PLoS ONE 2016, 11, e0166122. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.; Kaur, K.; Kaur, R. Menstrual hygiene, management, and waste disposal: Practices and challenges faced by girls/women of developing countries. J. Environ. Public Health 2018, 2018, 1730964. [Google Scholar] [CrossRef] [PubMed]
- Crofts, T.; Fisher, J. Menstrual hygiene in Ugandan schools: An investigation of low-cost sanitary pads. J. Water Sanit. Hyg. Dev. 2012, 2, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Kuhlmann, A.S.; Henry, K.; Wall, L.L. Menstrual Hygiene Management in Resource-Poor Countries. Obstet. Gynecol. Surv. 2017, 72, 356–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | n (%) | School Performance (%) | χ2 (df) | p | |
|---|---|---|---|---|---|
| Poor | Good | ||||
| Age (Years) | |||||
| 11–14 | 312 (62.5) | 72.4 | 27.5 | 2.80 (1) | 0.094 |
| 15–17 | 187 (37.5) | 79.1 | 20.9 | ||
| Current level of education | |||||
| Grade 7 | 82 (16.4) | 85.4 | 14.6 | 9.98 (3) | 0.019 * |
| Grade 8 | 151 (30.3) | 70.2 | 29.8 | ||
| Grade 9 | 131 (26.3) | 69.5 | 30.5 | ||
| Grade 10 | 135 (27.1) | 79.3 | 20.7 | ||
| Father’s education | |||||
| 0–4 | 260 (52.1) | 73.5 | 26.5 | 6.05 (2) | 0.048 * |
| 5–9 | 182 (36.5) | 80.2 | 19.8 | ||
| 10+ | 57 (11.4) | 64.9 | 35.1 | ||
| Father’s occupation | |||||
| Agriculture based | 86 (17.2) | 86.0 | 14.0 | 10.29 (4) | 0.036 * |
| Labor | 90 (18.0) | 76.7 | 23.3 | ||
| Business | 107 (21.4) | 72.0 | 28.0 | ||
| Job | 115 (23.1) | 67.0 | 33.0 | ||
| Others | 101 (20.2) | 76.2 | 23.8 | ||
| Mother’s education | |||||
| 0–4 | 244 (48.9) | 75.0 | 25.0 | 10.38 (2) | 0.006 * |
| 5–9 | 227 (45.5) | 78.0 | 22.0 | ||
| 10+ | 28 (5.6) | 50.0 | 50.0 | ||
| Mother’s occupation | |||||
| Homemaker | 473 (94.8) | 75.3 | 24.7 | 0.478 (1) | 0.489 |
| Working outside | 26 (5.2) | 69.2 | 30.8 | ||
| Household wealth status | |||||
| Low | 193 (38.7) | 81.3 | 18.7 | 7.88 (2) | 0.019 * |
| Middle | 161 (32.3) | 73.3 | 26.7 | ||
| High | 145 (29.1) | 68.3 | 31.7 | ||
| Family size | |||||
| ≤4 | 161 (32.3) | 76.4 | 23.6 | 0.26 (1) | 0.607 |
| >4 | 338 (67.7) | 74.3 | 25.7 | ||
| Knowledge level of menstruation | |||||
| Low | 263 (52.70) | 80.6 | 19.4 | 9.64 (2) | 0.008 * |
| Middle | 135 (27.1) | 69.6 | 30.4 | ||
| High | 101 (20.2) | 67.3 | 32.7 | ||
| Menstrual Hygiene Management | |||||
| Poor | 142 (28.5) | 87.3 | 12.7 | 19.64 (2) | <0.001 * |
| Average | 278 (55.7) | 72.3 | 27.7 | ||
| Good | 79 (15.8) | 62.0 | 38.0 | ||
| Characteristics | Frequency (%) | Menstrual Hygiene Management (%) | χ2 (df) | p | ||
|---|---|---|---|---|---|---|
| Poor | Average | Good | ||||
| Age at menarche (years) (mean ± SD) | 12.03 ± 0.95 | |||||
| Menstrual status | ||||||
| Regular | 414 (83.0) | 27.3 | 56.0 | 16.7 | 2.27 (2) | 0.321 |
| Irregular | 85 (17.0) | 34.1 | 54.1 | 11.8 | ||
| Main source of knowledge about menstruation | ||||||
| Newspapers/TV/Radio | 9 (1.8) | 33.3 | 44.4 | 22.2 | 13.30 (14) | 0.503 |
| School teachers | 57 (11.4) | 19.3 | 61.4 | 19.3 | ||
| Mother | 229 (45.9) | 28.4 | 57.6 | 14.0 | ||
| Relatives | 37 (7.4) | 37.8 | 51.4 | 10.8 | ||
| Elder sister | 93 (18.6) | 36.6 | 45.2 | 18.3 | ||
| Friends | 31 (6.2) | 19.4 | 58.1 | 22.6 | ||
| Books | 15 (3.0) | 20.0 | 66.7 | 13.3 | ||
| Others | 28 (5.6) | 21.4 | 64.3 | 14.3 | ||
| Have knowledge before menarche | ||||||
| Yes | 212 (42.5) | 23.6 | 56.6 | 19.8 | 6.81 (2) | 0.033 * |
| No | 287 (57.5) | 32.1 | 55.1 | 12.9 | ||
| Feelings at first menstruation | ||||||
| Feared | 283 (56.7) | 25.4 | 58.7 | 15.9 | 17.86 (10) | 0.057 |
| Worried | 81 (16.2) | 39.5 | 46.9 | 13.6 | ||
| Anxiety | 22 (4.4) | 27.3 | 45.5 | 27.3 | ||
| Felt shy | 63 (12.6) | 27.0 | 65.1 | 7.9 | ||
| No feelings | 47 (9.4) | 27.7 | 48.9 | 23.4 | ||
| Excited | 3 (0.6) | 66.7 | 0.0 | 33.3 | ||
| Miss school in last menstruation | ||||||
| Yes | 114 (22.7) | 33.6 | 48.7 | 17.7 | 8.39 (4) | 0.078 |
| No | 385 (77.3) | 27.0 | 57.9 | 15.1 | ||
| Usual feelings about menstruation | ||||||
| Fear | 17 (3.4) | 41.2 | 47.1 | 11.8 | 15.91 (12) | 0.195 |
| Worry | 19 (3.8) | 47.4 | 52.6 | 0.0 | ||
| Anxiety | 12 (2.4) | 16.7 | 58.3 | 25.0 | ||
| Shy | 21 (4.2) | 23.8 | 66.7 | 9.5 | ||
| Pain | 128 (25.7) | 25.0 | 53.1 | 21.9 | ||
| Normal | 301 (60.5) | 28.7 | 57.0 | 14.3 | ||
| Materials used during menstruation | ||||||
| Sanitary napkin | 259 (51.9) | 31.7 | 68.0 | 0.4 | 116.92 (4) | <0.001 * |
| Piece of new cloths (one-time use) | 23 (4.6) | 30.4 | 69.6 | 0.0 | ||
| Piece of reusable cloths per occasions (multiple use) | 216 (43.3) | 24.5 | 39.8 | 35.6 | ||
| Number of pads use per day during menstruation (N = 259) (mean ± SD) | 2.66 ± 0.829 | |||||
| Feel shy to buy pads (N = 259) | ||||||
| Yes | 38 (14.6) | 36.1 | 63.9 | 0.0 | 2.22 (2) | 0.328 |
| No | 26 (10.1) | 42.3 | 57.7 | 0.0 | ||
| Never bought | 195 (75.3) | 29.2 | 70.8 | 0.0 | ||
| Who usually buy pads (N = 259) | ||||||
| Mother | 174 (67.2) | 29.3 | 70.7 | 0.0 | 4.89 (3) | 0.180 |
| Father | 16 (6.2) | 18.8 | 81.3 | 0.0 | ||
| By own | 25 (9.6) | 48.0 | 52.0 | 0.0 | ||
| Elder sister | 44 (17.0) | 34.1 | 65.9 | 0.0 | ||
| Mode of disposal of the used pads (N = 259) | ||||||
| Burn | 7 (2.7) | 57.1 | 42.9 | 0.0 | 5.50 (5) | 0.357 |
| Bin | 67 (25.8) | 28.4 | 71.6 | 0.0 | ||
| Latrine | 58 (22.4) | 31.0 | 69.0 | 0.0 | ||
| Buried | 85 (32.8) | 28.2 | 71.8 | 0.0 | ||
| Anywhere nearby (back door of the house) | 26 (10.1) | 46.2 | 53.8 | 0.0 | ||
| Other | 16 (6.2) | 28.6 | 71.4 | 0.0 | ||
| Storage place of pads (N = 259) | ||||||
| With regular cloths | 63 (24.3) | 27.0 | 73.0 | 0.0 | 1.97 (2) | 0.373 |
| Special cup board | 137 (52.9) | 30.7 | 69.3 | 0.0 | ||
| Keep it to my mother | 59 (22.8) | 38.6 | 61.4 | 0.0 | ||
| Advantage of sanitary pads (N = 259) | ||||||
| Comfortable | 143 (55.2) | 32.6 | 67.4 | 0.0 | 12.71 (4) | 0.013 * |
| Adequate absorption | 36 (13.9) | 13.9 | 86.1 | 0.0 | ||
| Easy to use | 55 (21.2) | 32.7 | 67.3 | 0.0 | ||
| Do not soil cloths | 22 (8.5) | 40.9 | 59.1 | 0.0 | ||
| No itching | 3 (1.2) | 100.0 | 0.0 | 0.0 | ||
| Disadvantage of sanitary pads (N = 259) | ||||||
| Expensive | 131 (50.6) | 30.5 | 69.5 | 0.0 | 2.19 (3) | 0.534 |
| Not easily available | 35 (13.5) | 37.1 | 62.9 | 0.0 | ||
| Feel disgusted | 17 (6.6) | 17.6 | 82.4 | 0.0 | ||
| No disadvantage | 76 (29.3) | 33.3 | 66.7 | 0.0 | ||
| Method of drying reusable cloths (N = 216) | ||||||
| Under direct sunlight | 109 (50.5) | 3.7 | 23.9 | 72.5 | 132 (4) | <0.001 * |
| Hiding under other cloths | 90 (41.7) | 42.6 | 57.4 | 0.0 | ||
| Bathroom | 17 (7.8) | 52.9 | 47.1 | 0.0 | ||
| Storage place of washed reusable cloths (N = 216) | ||||||
| Plastic bag | 132 (61.1) | 21.2 | 39.4 | 39.4 | 8.59 (8) | 0.378 |
| Bathroom | 5 (2.3) | 60.0 | 20.0 | 20.0 | ||
| Under mattress | 16 (7.4) | 31.3 | 25.0 | 43.8 | ||
| In a dark, damp place | 8 (3.7) | 12.5 | 50.0 | 37.5 | ||
| Hidden from other family member | 55 (25.5) | 27.1 | 45.8 | 27.1 | ||
| Cleaning agent used during cleaning of cloths (N = 216) | ||||||
| Detergent | 208 (96.3) | 25.0 | 38.2 | 36.8 | 8.34 (4) | 0.080 |
| Liquid antiseptic | 5 (2.3) | 0.0 | 80.0 | 20.0 | ||
| Plain water | 3 (1.4) | 0.0 | 100.0 | 0.0 | ||
| Change pad/cloths at school | ||||||
| Yes | 87 (17.4) | 19.5 | 64.4 | 16.1 | 4.24 (2) | 0.120 |
| No | 412 (82.6) | 30.2 | 54.0 | 15.8 | ||
| Change pad/cloth every 6 hr. | ||||||
| Yes | 360 (72.1) | 5.8 | 72.2 | 21.9 | 326.18 (2) | <0.001 * |
| No | 139 (27.9) | 87.1 | 12.9 | 0.0 | ||
| Wash hands with soap before and after changing pads/cloths | ||||||
| Yes | 453 (90.8) | 23.2 | 59.4 | 17.4 | 68.01 (2) | <0.001 * |
| No | 46 (9.2) | 80.4 | 19.6 | 0.0 | ||
| Wash genitalia at least once per day | ||||||
| Yes | 459 (92.0) | 27.5 | 55.6 | 17.0 | 6.94 (2) | 0.031 * |
| No | 40 (8.0) | 40.0 | 57.5 | 2.5 | ||
| Reusable cloths with proper washing and drying (N = 216) | ||||||
| Yes | 110 (50.6) | 3.6 | 24.5 | 71.8 | 132.29 (2) | <0.001 * |
| No | 106 (49.4) | 45.5 | 54.5 | 0.0 | ||
| Characteristics | Crude 1 | Adjusted 2 | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| Menstruation Hygiene Management | ||||||
| Poor | 1.00 | 1.00 | ||||
| Average | 2.72 | 1.57–4.70 | <0.001 * | 2.71 | 1.49–4.90 | 0.001 * |
| Good | 4.38 | 2.25–8.51 | <0.001 | 5.08 | 2.46–10.46 | <0.001 * |
| Current level of education | ||||||
| Grade 7 | 1.00 | 1.00 | ||||
| Grade 8 | 2.31 | 1.16–4.58 | 0.016 * | 2.72 | 1.31–5.65 | 0.007 * |
| Grade 9 | 2.61 | 1.30–5.26 | 0.007 * | 1.99 | 0.94–4.23 | 0.071 |
| Grade 10 | 1.48 | 0.72–3.06 | 0.284 | 1.36 | 0.62–2.95 | 0.434 |
| Father’s education | ||||||
| 0–4 | 1.00 | 1.00 | ||||
| 5–9 | 0.72 | 0.46–1.12 | 0.151 | 0.76 | 0.45–1.26 | 0.294 |
| 10+ | 1.76 | 0.96–3.20 | 0.063 | 0.85 | 0.41–1.76 | 0.677 |
| Father’s occupation | ||||||
| Agriculture based | 1.00 | 1.00 | ||||
| Labor | 2.12 | 0.97–4.61 | 0.057 | 2.16 | 0.96–4.82 | 0.060 |
| Business | 2.85 | 1.34–6.03 | 0.006 * | 2.14 | 0.98–4.65 | 0.053 |
| Job | 3.64 | 1.75–7.58 | 0.001 * | 2.33 | 1.09–4.97 | 0.028 * |
| Others | 2.04 | 0.95–4.38 | 0.065 | 1.85 | 0.84–4.06 | 0.122 |
| Mother’s education | ||||||
| 0–4 | 1.00 | 1.00 | ||||
| 5–9 | 0.84 | 0.55–1.27 | 0.426 | 0.84 | 0.54–1.31 | 0.460 |
| 10+ | 2.74 | 1.24–6.02 | 0.012 * | 2.54 | 1.08–5.94 | 0.031 * |
| Mother’s occupation | ||||||
| Homemaker | 1.00 | 1.00 | ||||
| Working outside | 1.35 | 0.58–3.12 | 0.477 | 1.08 | 0.42–2.75 | 0.864 |
| Household wealth status | ||||||
| Low | 1.00 | 1.00 | ||||
| Middle | 1.60 | 0.98–2.62 | 0.058 | 1.35 | 0.80–2.30 | 0.256 |
| High | 2.26 | 1.38–3.70 | 0.001 * | 1.41 | 0.81–2.46 | 0.215 |
| Knowledge level of menstruation | ||||||
| Low | 1.00 | 1.00 | ||||
| Middle | 1.94 | 1.20–3.11 | 0.006 * | 1.82 | 1.09–3.03 | 0.021 * |
| High | 2.11 | 1.26–3.54 | 0.004 * | 1.94 | 1.10–3.41 | 0.021 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, M.S.; Yunus, F.M.; Hossain, M.B.; Sarker, K.K.; Khan, S. Association between Menstrual Hygiene Management and School Performance among the School-Going Girls in Rural Bangladesh. Adolescents 2021, 1, 335-347. https://doi.org/10.3390/adolescents1030025
Ahmed MS, Yunus FM, Hossain MB, Sarker KK, Khan S. Association between Menstrual Hygiene Management and School Performance among the School-Going Girls in Rural Bangladesh. Adolescents. 2021; 1(3):335-347. https://doi.org/10.3390/adolescents1030025
Chicago/Turabian StyleAhmed, Md. Sabbir, Fakir Md Yunus, Md. Belal Hossain, Kinsuk Kalyan Sarker, and Safayet Khan. 2021. "Association between Menstrual Hygiene Management and School Performance among the School-Going Girls in Rural Bangladesh" Adolescents 1, no. 3: 335-347. https://doi.org/10.3390/adolescents1030025
APA StyleAhmed, M. S., Yunus, F. M., Hossain, M. B., Sarker, K. K., & Khan, S. (2021). Association between Menstrual Hygiene Management and School Performance among the School-Going Girls in Rural Bangladesh. Adolescents, 1(3), 335-347. https://doi.org/10.3390/adolescents1030025