
Abdominal Breathing Effect on Postural Stability and the Respiratory Muscles’ Activation during Body Stances Used in Fitness Modalities


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Abdominal Breathing Visual and Experimental Verification
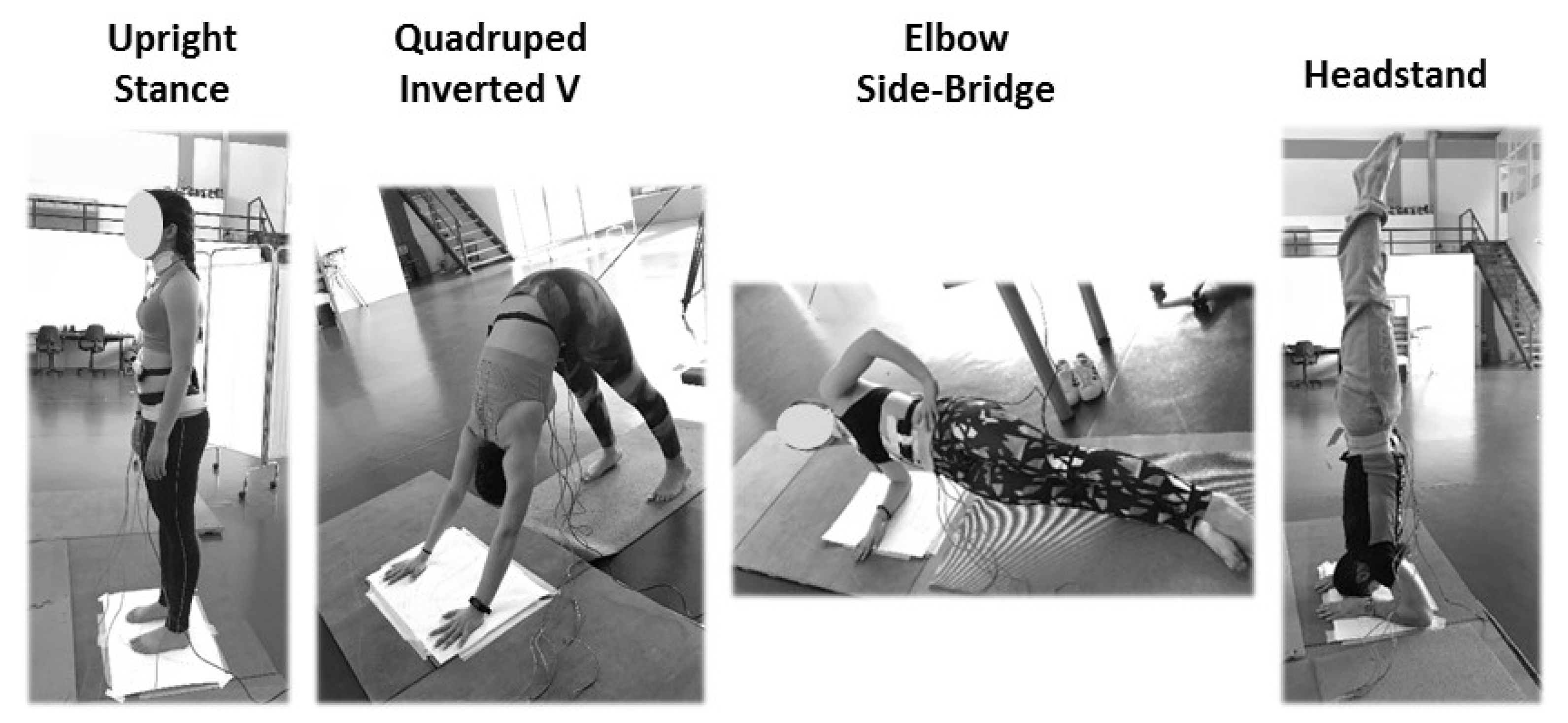
2.3. Experimental Procedure
2.4. Postural Stability: Data Collection and Data Procession
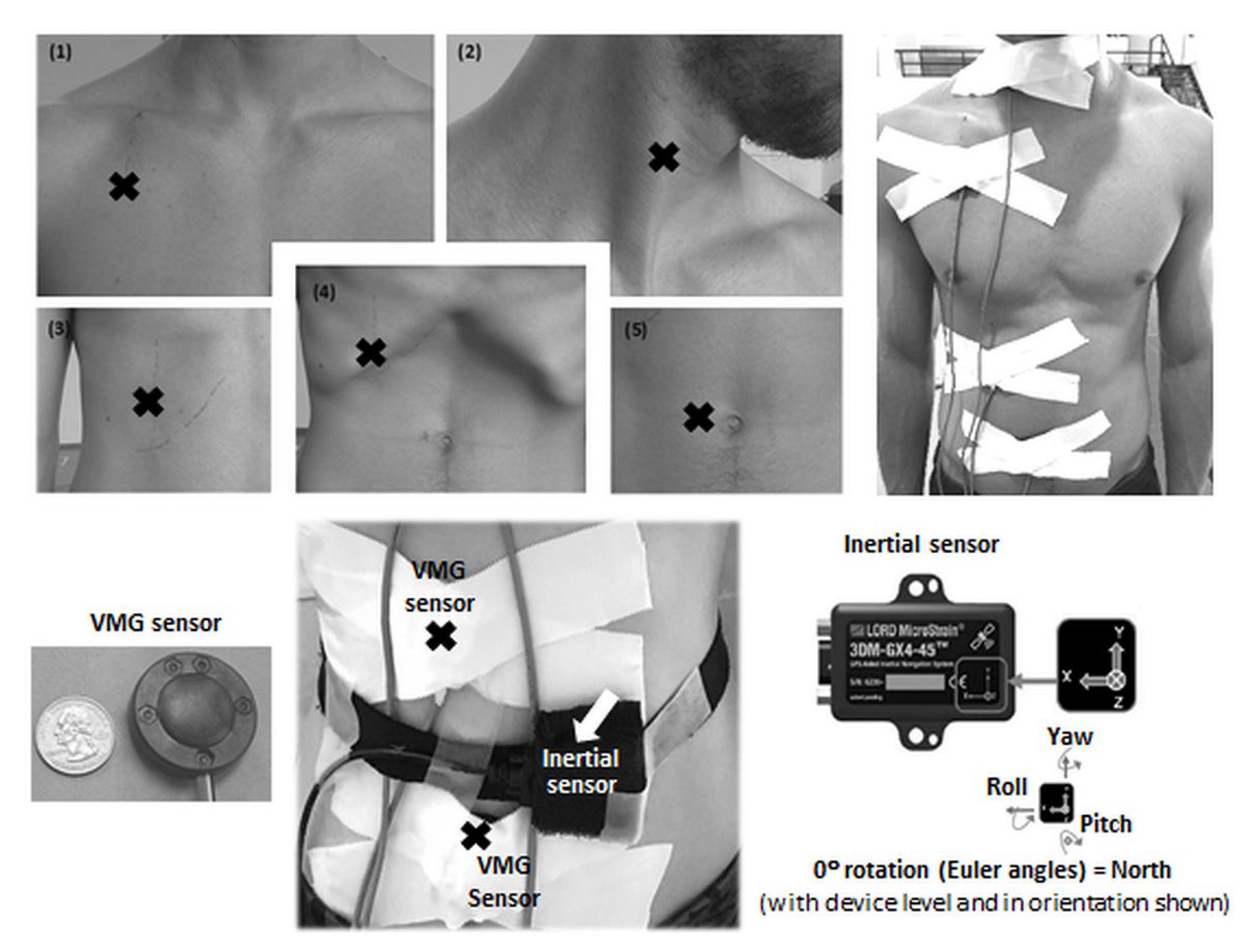
2.5. Respiratory Muscles’ Activation: Data Collection and Data Procession
2.6. Data Reliability
2.7. Statistical Analysis
3. Results
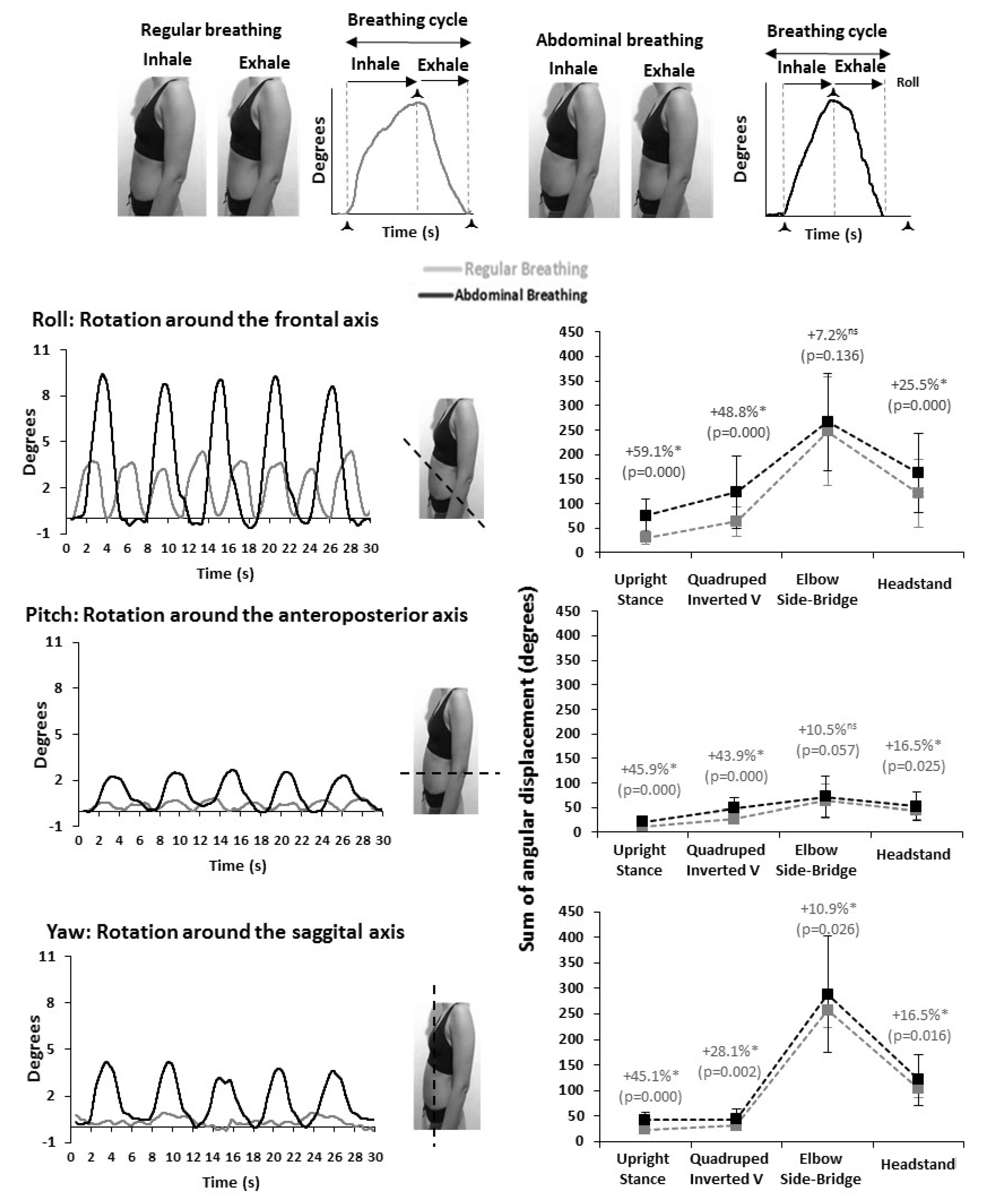
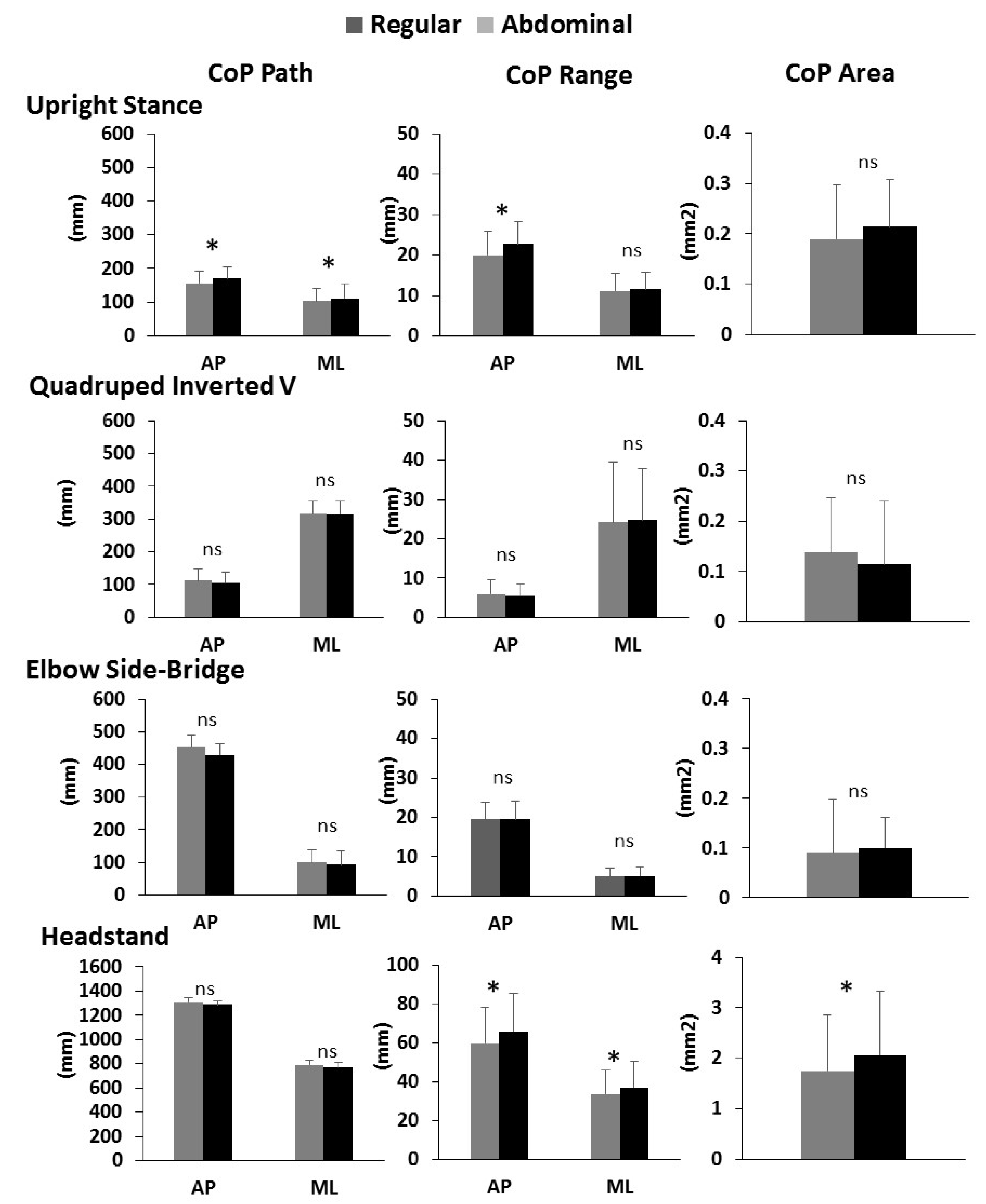
3.1. Abdominal Breathing Effect on Postural Stability
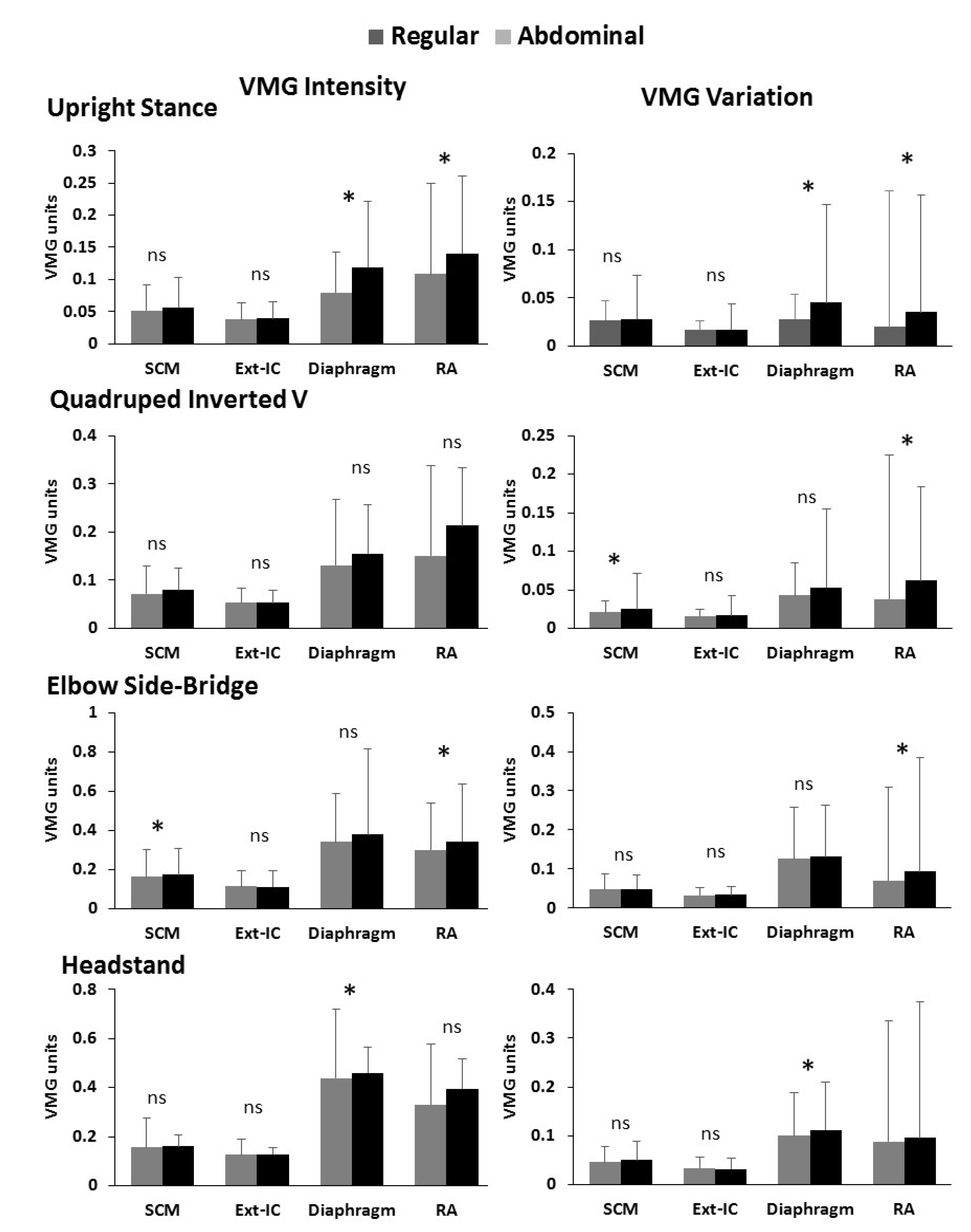
3.2. Abdominal Breathing Effect on the Respiratory Muscle’s Activation
4. Discussion
4.1. Postural Stability
4.2. Respiratory Muscles’ Activation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Martarelli, D.; Cocchioni, M.; Scuri, S.; Pompei, P. Diaphragmatic breathing reduces exercise-induced oxidative stress. Evid. Based. Complement. Altern. Med. 2011, 2011, 932430. [Google Scholar] [CrossRef] [PubMed]
- Steurer-Stey, C.; Russi, E.W.; Steurer, J. Complementary and Alternative Medicine in Asthma: Do They Work? Swiss Med. Wkly. 2002, 132, 338–344. [Google Scholar] [PubMed]
- Dhruva, A.; Miaskowski, C.; Abrams, D.; Acree, M.; Cooper, B.; Goodman, S.; Hecht, F.M. Yoga Breathing for Cancer Chemotherapy-Associated Symptoms and Quality of Life: Results of a Pilot Randomized Controlled Trial. J. Altern. Complement. Med. 2012, 18, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Yue, Z.-Q.; Gong, Z.-Q.; Zhang, H.; Duan, N.-Y.; Shi, Y.-T.; Wei, G.-X.; Li, Y.-F. The Effect of Diaphragmatic Breathing on Attention, Negative Affect and Stress in Healthy Adults. Front. Psychol. 2017, 8, 1–12. [Google Scholar] [CrossRef]
- Wahbeh, H.; Elsas, S.-M.; Oken, B.S. Mind-Body Interventions: Applications in Neurology. Neurology 2008, 70, 2321–2328. [Google Scholar] [CrossRef]
- Perry, S.F.; Similowski, T.; Klein, W.; Codd, J.R. The Evolutionary Origin of the Mammalian Diaphragm. Respir. Physiol. Neurobiol. 2010, 171, 1–16. [Google Scholar] [CrossRef]
- Hamaoui, A.; Hudson, A.L.; Laviolette, L.; Nierat, M.C.; Do, M.C.; Similowski, T. Postural Disturbances Resulting from Unilateral and Bilateral Diaphragm Contractions: A Phrenic Nerve Stimulation Study. J. Appl. Physiol. 2014, 117, 825–832. [Google Scholar] [CrossRef]
- Kim, S.-H.; Shin, H.-J.; Cho, H.-Y. Impact of Types of Breathing on Static Balance Ability in Healthy Adults. Int. J. Environ. Res. Public Health 2022, 19, 1205. [Google Scholar] [CrossRef]
- Bordoni, B.; Zanier. Anatomic Connections of the Diaphragm Influence of Respiration on the Body System. J. Multidiscip. Healthc. 2013, 6, 281. [Google Scholar] [CrossRef]
- Hodges, P.W.; Butler, J.E.; McKenzie, D.K.; Gandevia, S.C. Contraction of the Human Diaphragm during Rapid Postural Adjustments. J. Physiol. 1997, 505, 539–548. [Google Scholar] [CrossRef]
- Hodges, P.W.; Gandevia, S.C. Changes in Intra-Abdominal Pressure during Postural and Respiratory Activation of the Human Diaphragm. J. Appl. Physiol. 2000, 89, 967–976. [Google Scholar] [CrossRef]
- Kocjan, J.; Adamek, M.; Gzik-Zroska, B.; Czyżewski, D.; Rydel, M. Network of Breathing. Multifunctional Role of the Diaphragm: A Review. Adv. Respir. Med. 2017, 85, 224–232. [Google Scholar] [CrossRef]
- Kim, E.; Lee, H. The Effects of Deep Abdominal Muscle Strengthening Exercises on Respiratory Function and Lumbar Stability. J. Phys. Ther. Sci. 2013, 25, 663–665. [Google Scholar] [CrossRef]
- De Troyer, A.; Boriek, A. Mechanics of the Respiratory Muscles. Compr. Physiol. 2011, 1, 1273–1300. [Google Scholar] [CrossRef]
- Kolář, P.; Šafářová, M. Dynamic Neuromuscular Stabilization. In Clinical Rehabilitation, 1st ed.; Kolář, P., Kobesová, A., Eds.; K. Vápence 16: Praha, Czech Republic, 2013; pp. 257–258. [Google Scholar]
- Sieck, G.C.; Ferreira, L.F.; Reid, M.B.; Mantilla, C.B. Mechanical Properties of Respiratory Muscles. In Comprehensive Physiology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013; Volume 3, pp. 1533–1567. [Google Scholar] [CrossRef]
- Bouisset, S.; Duchêne, J.L. Is Body Balance More Perturbed by Respiration in Seating than in Standing Posture? Neuroreport 1994, 5, 957–960. [Google Scholar] [CrossRef]
- Gurfinkel, V.S.; Kots, Y.M.; Paltsev, E.I.F.A. The Compensation of Respiratory Disturbances of the Erect Posture of Man as an Example of the Organisation of Interarticular Action. In Systems; Gurfinkel, V.S., Fomin, T.M.L.S., Eds.; MIT Press: Cambridge, MA, USA, 1971. [Google Scholar]
- Hamaoui, A.; Gonneau, E.; Le Bozec, S. Respiratory Disturbance to Posture Varies According to the Respiratory Mode. Neurosci. Lett. 2010, 475, 141–144. [Google Scholar] [CrossRef]
- Hunter, I.W.; Kearney, R.E. Respiratory Components of Human Postural Sway. Neurosci. Lett. 1981, 25, 155–159. [Google Scholar] [CrossRef]
- Stephens, R.J.; Haas, M.; Moore, W.L.; Emmil, J.R.; Sipress, J.A.; Williams, A. Effects of Diaphragmatic Breathing Patterns on Balance: A Preliminary Clinical Trial. J. Manip. Physiol. Ther. 2017, 40, 169–175. [Google Scholar] [CrossRef]
- Vera-Garcia, F.J.; Moreside, J.M.; McGill, S.M. MVC Techniques to Normalize Trunk Muscle EMG in Healthy Women. J. Electromyogr. Kinesiol. 2010, 20, 10–16. [Google Scholar] [CrossRef]
- Vera-Garcia, F.J.; Irles-Vidal, B.; Prat-Luri, A.; García-Vaquero, M.P.; Barbado, D.; Juan-Recio, C. Progressions of Core Stabilization Exercises Based on Postural Control Challenge Assessment. Eur. J. Appl. Physiol. 2020, 120, 567–577. [Google Scholar] [CrossRef]
- Lehman, G.J.; Hoda, W.; Oliver, S. Trunk Muscle Activity during Bridging Exercises on and off a Swiss Ball. Chiropr. Osteopat. 2005, 13, 14. [Google Scholar] [CrossRef]
- García-Vaquero, M.P.; Moreside, J.M.; Brontons-Gil, E.; Peco-González, N.; Vera-Garcia, F.J. Trunk Muscle Activation during Stabilization Exercises with Single and Double Leg Support. J. Electromyogr. Kinesiol. 2012, 22, 398–406. [Google Scholar] [CrossRef]
- Campos, M.H.; Giraldi, N.M.; Gentil, P.; de Lira, C.A.B.; Vieira, C.A.; de Paula, M.C. The Geometric Curvature of the Spine during the Sirshasana, the Yoga’s Headstand. J. Sports Sci. 2017, 35, 1134–1141. [Google Scholar] [CrossRef]
- Clément, G.; Rézette, D. Motor Behavior Underlying the Control of an upside-down Vertical Posture. Exp. Brain Res. 1985, 59, 478–484. [Google Scholar] [CrossRef]
- Hector, R.; Jensen, J.L. Sirsasana (Headstand) Technique Alters Head/Neck Loading: Considerations for Safety. J. Bodyw. Mov. Ther. 2015, 19, 434–441. [Google Scholar] [CrossRef]
- Hedbávný, P.; Sklena, J.; Hupka, D.; Kalichová, M. Balancing in Handstand on the Floor. Sci. Gymnast. J. 2013, 5, 69–80. [Google Scholar]
- Gautier, G.; Thouvarecq, R.; Chollet, D. Visual and Postural Control of an Arbitrary Posture: The Handstand. J. Sports Sci. 2007, 25, 1271–1278. [Google Scholar] [CrossRef]
- Omorczyk, J.; Bujas, P.; Puszcza\lowska-Lizis, E.; Biskup, L. Balance in Handstand and Postural Stability in Standing Position in Athletes Practicing Gymnastics. Acta. Bioeng. Biomech. 2018, 20, 139–147. [Google Scholar] [CrossRef]
- Slobounov, S.M.; Newell, K.M. Postural Dynamics in Upright and Inverted Stances. J. Appl. Biomech. 1996, 12, 185–196. [Google Scholar] [CrossRef]
- Sobera, M.; Siedlecka, B.; Piestrak, P.; Sojka-Krawiec, K.; Graczykowska, B. Maintaning Body Balance in Extreme Positions. Biol. Sport. 2007, 24, 81–88. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, L.; Manning, J.; Zhang, S. Voluntary Control of Breathing Affects Center of Pressure Complexity during Static Standing in Healthy Older Adults. Gait Posture 2019, 68, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-Y.; Cheon, S.-H.; Yong, M.-S. Effect of Diaphragm Breathing Exercise Applied on the Basis of Overload Principle. J. Phys. Ther. Sci. 2017, 29, 1054–1056. [Google Scholar] [CrossRef] [PubMed]
- Bates, A.; Ling, M.J.; Mann, J.; Arvind, D.K. Respiratory Rate and Flow Waveform Estimation from Tri-Axial Accelerometer Data. In Proceedings of 2010 International Conference on Body Sensor Networks, IEEE, Singapore, 7–9 June 2010. [Google Scholar] [CrossRef]
- Haescher, M.; Matthies, D.J.C.; Trimpop, J.; Urban, B. A Study on Measuring Heart- and Respiration-Rate via Wrist-Worn Accelerometer-Based Seismocardiography (SCG) in Comparison to Commonly Applied Technologies. In Proceedings of the iWOAR 2015—2nd International Workshop on Sensor-Based Activity Recognition and Interaction, Rostock Warnemade, Germany, 25–26 June 2015. [Google Scholar] [CrossRef]
- Phan, D.H.; Bonnet, S.; Guillemaud, R.; Castelli, E.; Pham Thi, N.Y. Estimation of Respiratory Waveform and Heart Rate Using an Accelerometer. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 14 October 2018. [Google Scholar] [CrossRef]
- Schubert, P.; Kirchner, M. Ellipse Area Calculations and Their Applicability in Posturography. Gait Posture 2014, 39, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Chien, M.-Y.; Wu, Y.-T.; Chang, Y.-J. Assessment of Diaphragm and External Intercostals Fatigue from Surface EMG Using Cervical Magnetic Stimulation. Sensors 2008, 8, 2174–2187. [Google Scholar] [CrossRef] [PubMed]
- De Mayo, T.; Miralles, R.; Barrero, D.; Bulboa, A.; Carvajal, D.; Valenzuela, S.; Ormeño, G. Breathing Type and Body Position Effects on Sternocleidomastoid and Suprahyoid EMG Activity. J. Oral. Rehabil. 2005, 32, 487–494. [Google Scholar] [CrossRef]
- Druz, W.S.; Sharp, J.T. Activity of Respiratory Muscles in Upright and Recumbent Humans. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1981, 51, 1552–1561. [Google Scholar] [CrossRef]
- Santos, T.V.; Ruas, G.; Sande de Souza, L.A.P.; Volpe, M.S. Influence of Forward Leaning and Incentive Spirometry on Inspired Volumes and Inspiratory Electromyographic Activity during Breathing Exercises in Healthy Subjects. J. Electromyogr. Kinesiol. 2012, 22, 961–967. [Google Scholar] [CrossRef]
- Segizbaeva, M.O.; Pogodin, M.A.; Aleksandrova, N.P. Effects of Body Positions on Respiratory Muscle Activation during Maximal Inspiratory Maneuvers. In Advances in Experimental Medicine and Biology; Pokorski, M., Ed.; Springer: Dordrecht, The Netherlands, 2013; Volume 756, pp. 355–363. [Google Scholar] [CrossRef]
- Valenzuela, S.; Miralles, R.; Santander, H.; Bull, R.; Cordova, R.; Celhay, I.; Cavada, G.; Gutiérrez, M.F. Effects of Breathing Type on Electromyographic Activity of Respiratory Muscles at Different Body Positions. Cranio 2017, 35, 110–115. [Google Scholar] [CrossRef]
- Druz, W.S.; Sharp, J.T. Electrical and Mechanical Activity of the Diaphragm Accompanying Body Position in Severe Chronic Obstructive Pulmonary Disease. Am. Rev. Respir. Dis. 1982, 125, 275–280. [Google Scholar] [CrossRef]
- Hudson, A.L.; Joulia, F.; Butler, A.A.; Fitzpatrick, R.C.; Gandevia, S.C.; Butler, J.E. Activation of Human Inspiratory Muscles in an upside-down Posture. Respir. Physiol. Neurobiol. 2016, 226, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Takazakura, R.; Takahashi, M.; Nitta, N.; Murata, K. Diaphragmatic Motion in the Sitting and Supine Positions: Healthy Subject Study Using a Vertically Open Magnetic Resonance System. J. Magn. Reson. Imaging 2004, 19, 605–609. [Google Scholar] [CrossRef] [PubMed]
- Kera, T.; Maruyama, H. The Effect of Posture on Respiratory Activity of the Abdominal Muscles. J. Physiol. Anthropol. Appl. Hum. Sci. 2005, 24, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Maarsingh, E.J.; van Eykern, L.A.; Sprikkelman, A.B.; Hoekstra, M.O.; van Aalderen, W.M. Respiratory Muscle Activity Measured with a Noninvasive EMG Technique: Technical Aspects and Reproducibility. J. Appl. Physiol. 2000, 88, 1955–1961. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Pinsault, N.; Vuillerme, N. Test-Retest Reliability of Centre of Foot Pressure Measures to Assess Postural Control during Unperturbed Stance. Med. Eng. Phys. 2009, 31, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Fleiss, J.L. Reliability of Measurement. In The Design and Analysis of Clinical Experiments; Fleis, J.L., Ed.; Wiley: New York, NY, USA, 1986; pp. 1–32. [Google Scholar]
- Rodrigues, G.D.; Gurgel, J.L.; Gonçalves, T.R.; Porto, F.; Paulo, P. Influence of Breathing Patterns and Orthostatic Stress on Postural Control in Older Adults. Geriatr. Gerontol. Int. 2018, 18, 692–697. [Google Scholar] [CrossRef] [PubMed]
- Kuznetsov, N.A.; Riley, M.A. Effects of Breathing on Multijoint Control of Center of Mass Position during Upright Stance. J. Mot. Behav. 2012, 44, 241–253. [Google Scholar] [CrossRef]
- Schmid, M.; Conforto, S.; Bibbo, D.; D’Alessio, T. Respiration and Postural Sway: Detection of Phase Synchronizations and Interactions. Hum. Mov. Sci. 2004, 23, 105–119. [Google Scholar] [CrossRef]
- Nelson, N. Diaphragmatic Breathing: The Foundation of Core Stability. Strength Cond. J. 2012, 34, 34–40. [Google Scholar] [CrossRef]
- Ishida, H.; Watanabe, S. Maximum Expiration Activates the Abdominal Muscles during Side Bridge Exercise. J. Back Musculoskelet. Rehabil. 2014, 27, 481–484. [Google Scholar] [CrossRef] [PubMed]
- Celhay, I.; Cordova, R.; Miralles, R.; Meza, F.; Erices, P.; Barrientos, C.; Valenzuela, S. Effect of upper Costal and Costo-Diaphragmatic Breathing Types on Electromyographic Activity of Respiratory Muscles. Cranio 2015, 33, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Cordova, R.; Miralles, R.; Bull, R.; Gamboa, N.A.; Santander, H.; Valenzuela, S.; Fuentes, A.D.; Morales, N.S.; Gutierrez, M.F. Respiratory EMG Activity between Subjects with Costo-Diaphragmatic, Upper Costal or Mixed Breathing Type. J. Sleep. Disord. Ther. 2019, 8, 2167-0277. [Google Scholar] [CrossRef]
- Miralles, R.; Gamboa, N.A.; Gutiérrez, M.F.; Valenzuela, S.; Bull, R.; Fuentes, A.D. Effect of Breathing Type on Electromyographic Activity of Respiratory Muscles during Tooth Clenching at Different Decubitus Positions. Cranio 2019, 9634, 28–34. [Google Scholar] [CrossRef]
- Cahalin, L.P.; Braga, M.; Matsuo, Y.; Hernandez, E.D. Efficacy of Diaphragmatic Breathing in Persons with Chronic Obstructive Pulmonary Disease: A Review of the Literature. J. Cardiopulm. Rehabil. 2002, 22, 7–21. [Google Scholar] [CrossRef]
- Pollock, A.S.; Durward, B.R.; Rowe, P.J.; Paul, J.P. What Is Balance? Clin. Rehabil. 2000, 14, 402–406. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| F | Sig. (p Value) | Observed Power | Cohen’s f Effect Size | |
|---|---|---|---|---|
| Upright Stance | ||||
| Cop Path | ||||
| AP | 6.8 | 0.014 * | 0.71 | 0.49 |
| ML | 5.97 | 0.021 * | 0.66 | 0.46 |
| CoP Range | ||||
| AP | 9.59 | 0.004 * | 0.85 | 0.59 |
| ML | 1.54 | 0.225 ns | 0.22 | 0.23 |
| CoP Area | 2.98 | 0.095 ns | 0.39 | 0.33 |
| Quadruped Inverted V | ||||
| Cop Path | ||||
| AP | 1.33 | 0.259 ns | 0.20 | 0.22 |
| ML | 0.19 | 0.669 ns | 0.07 | 0.08 |
| CoP Range | ||||
| AP | 0.75 | 0.395 ns | 0.13 | 0.16 |
| ML | 0.16 | 0.696 ns | 0.07 | 0.07 |
| CoP Area | 0.48 | 0.495 ns | 0.10 | 0.13 |
| Elbow Side-Bridge | ||||
| Cop Path | ||||
| AP | 3.9 | 0.058 ns | 0.48 | 0.37 |
| ML | 0.98 | 0.330 ns | 0.16 | 0.19 |
| CoP Range | ||||
| AP | 0.04 | 0.850 ns | 0.05 | 0.00 |
| ML | 0.29 | 0.596 ns | 0.08 | 0.04 |
| CoP Area | 0.81 | 0.375 ns | 0.14 | 0.10 |
| Headstand | ||||
| Cop Path | ||||
| AP | 0.22 | 0.643 ns | 0.07 | 0.09 |
| ML | 0.64 | 0.431 ns | 0.12 | 0.15 |
| CoP Range | ||||
| AP | 9.24 | 0.005 * | 0.84 | 0.57 |
| ML | 4.61 | 0.041 * | 0.55 | 0.41 |
| CoP Area | 4.27 | 0.048 * | 0.51 | 0.39 |
| F | Sig. (p Value) | Observed Power | Cohen’s f Effect Size | |
|---|---|---|---|---|
| Upright Stance | ||||
| SCM | 1.88 | 0.182 ns | 0.26 | 0.26 |
| Ext-IC | 0.27 | 0.606 ns | 0.08 | 0.10 |
| Diaphragm | 12.46 | 0.001 * | 0.93 | 0.67 |
| RA | 9.97 | 0.004 * | 0.86 | 0.60 |
| Quadruped Inverted V | ||||
| SCM | 2.08 | 0.160 ns | 0.29 | 0.27 |
| Ext-IC | 0.09 | 0.767 ns | 0.06 | 0.06 |
| Diaphragm | 1.85 | 0.184 | 0.26 | 0.26 |
| RA | 3.03 | 0.093 ns | 0.39 | 0.33 |
| Elbow Side-Bridge | ||||
| SCM | 5.02 | 0.033 * | 0.58 | 0.42 |
| Ext-IC | 0.09 | 0.773 ns | 0.06 | 0.05 |
| Diaphragm | 2.61 | 0.117 ns | 0.35 | 0.31 |
| RA | 10.05 | 0.004 * | 0.86 | 0.60 |
| Headstand | ||||
| SCM | 1.31 | 0.263 ns | 0.20 | 0.22 |
| Ext-IC | 0.02 | 0.889 ns | 0.05 | 0.03 |
| Diaphragm | 10.66 | 0.003 * | 0.88 | 0.62 |
| RA | 0.93 | 0.343 ns | 0.15 | 0.18 |
| F | Sig. (p Value) | Observed Power | Cohen’s f Effect Size | |
|---|---|---|---|---|
| Upright Stance | ||||
| SCM | 0.31 | 0.580 ns | 0.08 | 0.11 |
| Ext-IC | 0.44 | 0.514 ns | 0.10 | 0.12 |
| Diaphragm | 20.22 | 0.000 * | 0.99 | 0.85 |
| RA | 39.83 | 0.000 * | 1.00 | 1.19 |
| Quadruped Inverted V | ||||
| SCM | 6.96 | 0.013 * | 0.72 | 0.50 |
| Ext-IC | 0.97 | 0.333 ns | 0.16 | 0.19 |
| Diaphragm | 22.47 | 0.000 * | 1.00 | 0.90 |
| RA | 13.82 | 0.001 * | 0.95 | 0.70 |
| Elbow Side-Bridge | ||||
| SCM | 0.28 | 0.604 ns | 0.08 | 0.10 |
| Ext-IC | 0.17 | 0.688 ns | 0.07 | 0.08 |
| Diaphragm | 0.14 | 0.714 ns | 0.07 | 0.07 |
| RA | 9.08 | 0.005 * | 0.83 | 0.57 |
| Headstand | ||||
| SCM | 1.65 | 0.210 ns | 0.24 | 0.24 |
| Ext-IC | 0.42 | 0.525 ns | 0.10 | 0.12 |
| Diaphragm | 4.41 | 0.045 * | 0.53 | 0.40 |
| RA | 1.15 | 0.293 ns | 0.18 | 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foskolou, A.; Emmanouil, A.; Boudolos, K.; Rousanoglou, E. Abdominal Breathing Effect on Postural Stability and the Respiratory Muscles’ Activation during Body Stances Used in Fitness Modalities. Biomechanics 2022, 2, 478-493. https://doi.org/10.3390/biomechanics2030037
Foskolou A, Emmanouil A, Boudolos K, Rousanoglou E. Abdominal Breathing Effect on Postural Stability and the Respiratory Muscles’ Activation during Body Stances Used in Fitness Modalities. Biomechanics. 2022; 2(3):478-493. https://doi.org/10.3390/biomechanics2030037
Chicago/Turabian StyleFoskolou, Apostolina, Analina Emmanouil, Konstantinos Boudolos, and Elissavet Rousanoglou. 2022. "Abdominal Breathing Effect on Postural Stability and the Respiratory Muscles’ Activation during Body Stances Used in Fitness Modalities" Biomechanics 2, no. 3: 478-493. https://doi.org/10.3390/biomechanics2030037
APA StyleFoskolou, A., Emmanouil, A., Boudolos, K., & Rousanoglou, E. (2022). Abdominal Breathing Effect on Postural Stability and the Respiratory Muscles’ Activation during Body Stances Used in Fitness Modalities. Biomechanics, 2(3), 478-493. https://doi.org/10.3390/biomechanics2030037