

Quantification of Cycling Smoothness in Children with Cerebral Palsy




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
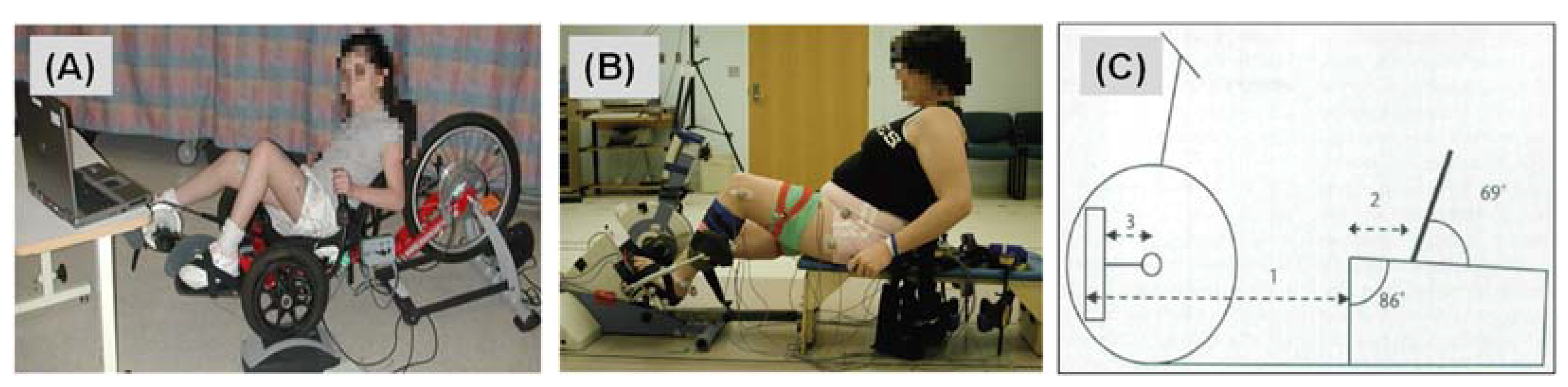
2.2. Data Collection
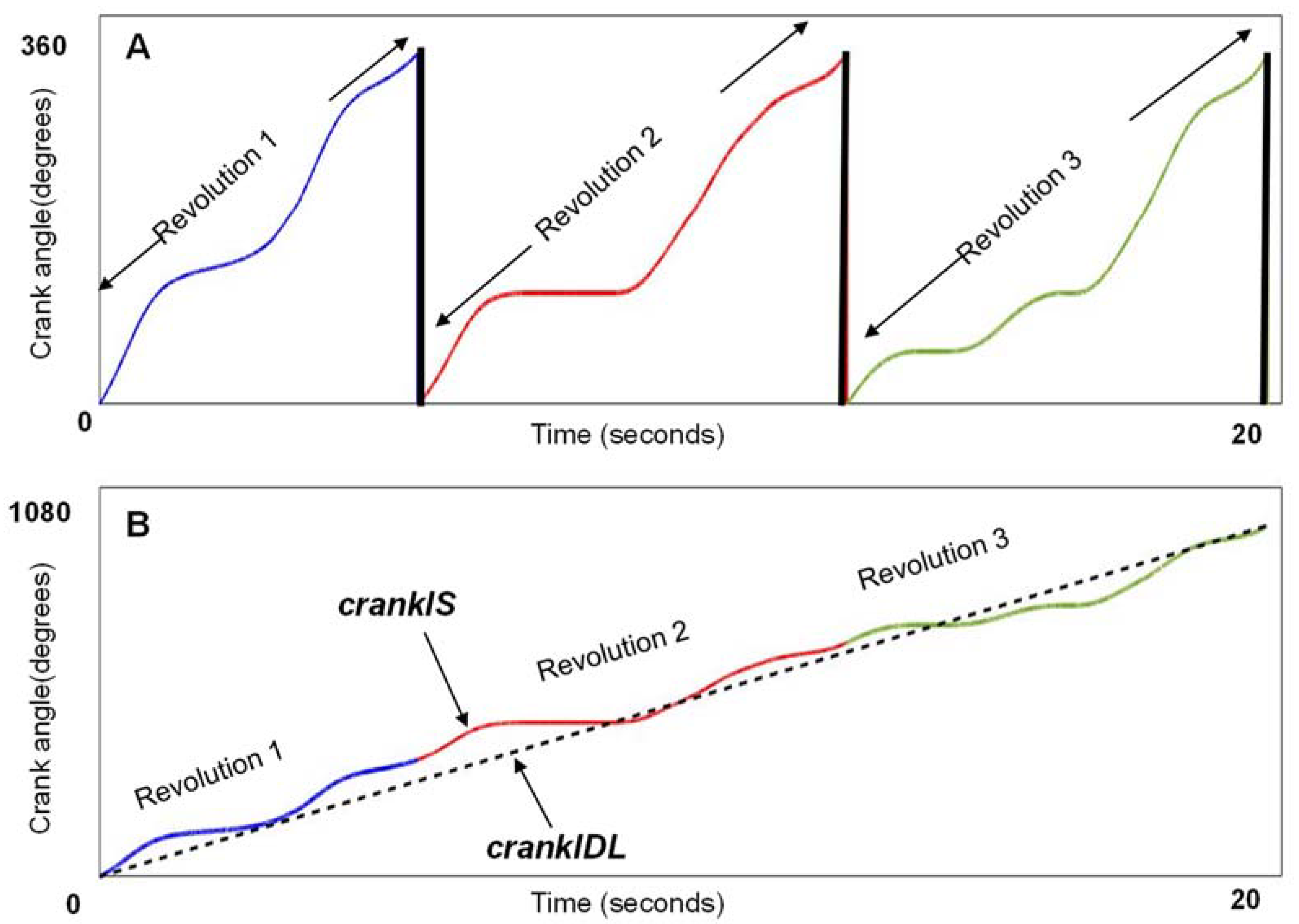
2.3. Data Analysis
2.4. Smoothness Metrics
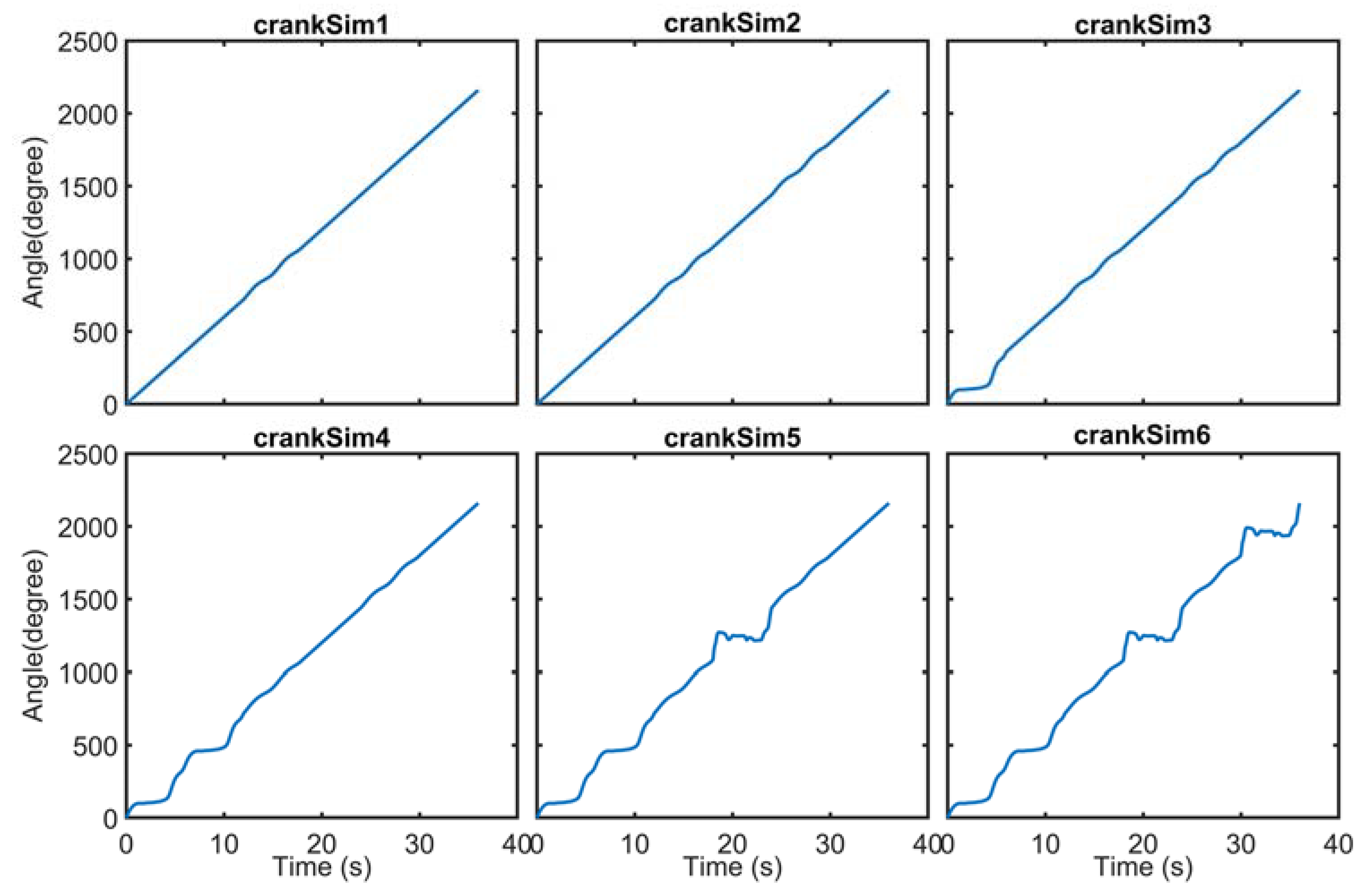
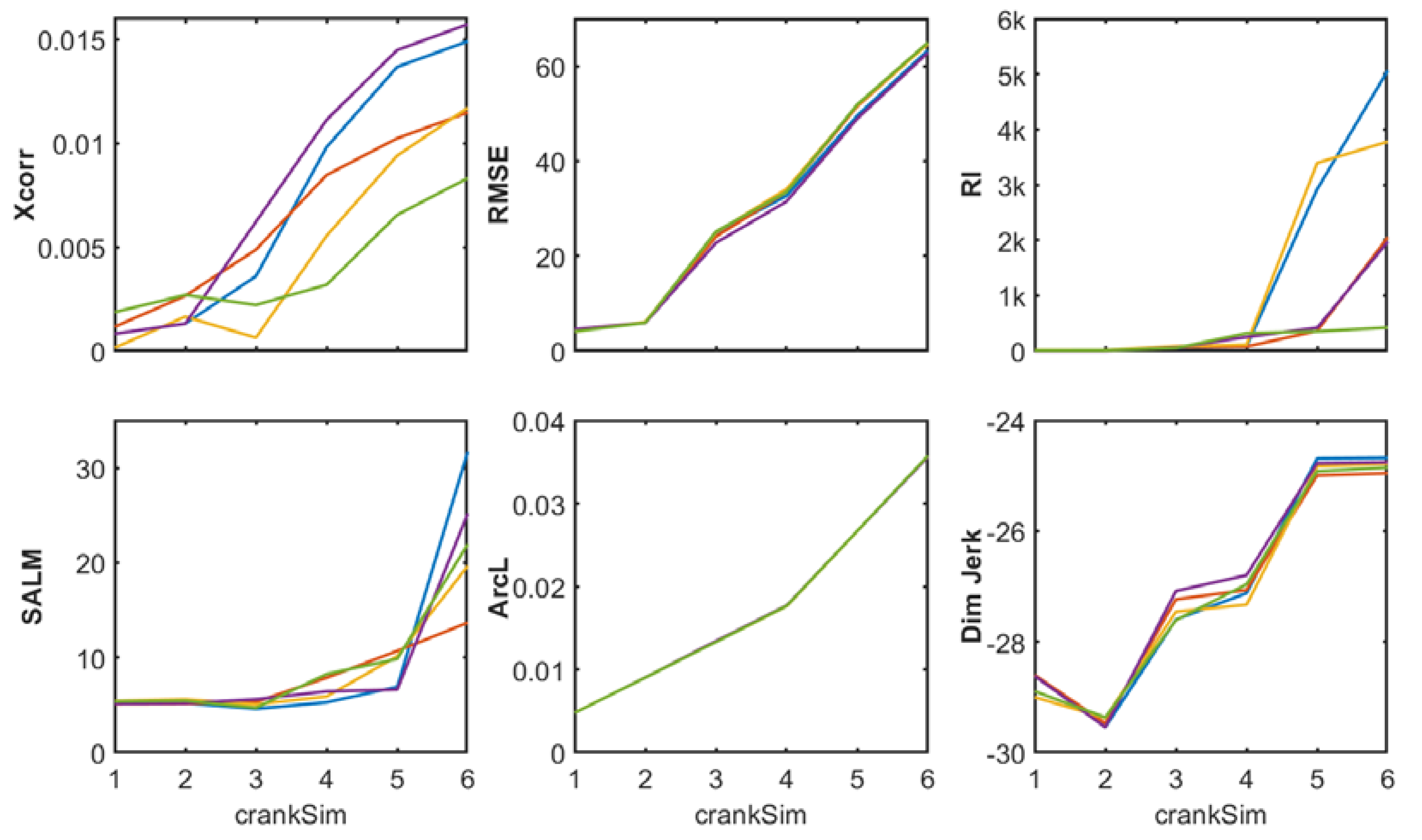
2.5. Simulated Signals Using Real Aberrant Cycles
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bax, M.; Goldstein, M.; Rosenbaun, P.; Leviton, A.; Paneth, N.; Dan, B.; Jacobsson, B.; Damiano, D. Proposed definition and classification of cerebral palsy, April 2005. Dev. Med. Child Neurol. 2005, 47, 571. [Google Scholar] [CrossRef] [PubMed]
- Wiley, M.E.; Damiano, D.L. Lower-extremity strength profiles in spastic cerebral palsy. Dev. Med. Child Neurol. 1998, 40, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Damiano, D.L.; Martellotta, T.L.; Sullivan, D.J.; Granata, K.P.; Abel, M.F. Muscle force production and functional performance in spastic cerebral palsy: Relationship of cocontraction. Arch. Phys. Med. Rehabil. 2000, 81, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Stackhouse, S.K.; Binder-Macleod, S.A.; Stackhouse, C.A.; McCarthy, J.J.; Prosser, L.A.; Lee, S.C. Neuromuscular electrical stimulation versus volitional isometric strength training in children with spastic diplegic cerebral palsy: A preliminary study. Neurorehabil. Neural Repair 2007, 21, 475–485. [Google Scholar] [CrossRef] [PubMed]
- Stackhouse, S.K.; Binder-Macleod, S.A.; Lee, S.C.K. Voluntary muscle activation, contractile properties, and fatigability in children with and without cerebral palsy. Muscle Nerve 2005, 31, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Thelen, D.D.; Riewald, S.A.; Asakawa, D.S.; Sanger, T.D.; Delp, S.L. Abnormal coupling of knee and hip moments during maximal exertions in persons with cerebral palsy. Muscle Nerve 2003, 27, 486–493. [Google Scholar] [CrossRef]
- Fujiwara, T.; Liu, M.; Chino, N. Effect of pedaling exercise on the hemiplegic lower limb. Am. J. Phys. Med. Rehabil. 2003, 82, 357–363. Available online: https://journals.lww.com/ (accessed on 10 January 2020). [CrossRef] [PubMed]
- Brown, D.A.; Nagpal, S.; Chi, S. Limb-loaded cycling program for locomotor intervention following stroke. Phys. Ther. 2005, 85, 159–168. [Google Scholar] [CrossRef]
- Williams, H.; Pountney, T. Effects of a static bicycling programme on the functional ability of young people with cerebral palsy who are non-ambulant. Dev. Med. Child Neurol. 2007, 49, 522–527. [Google Scholar] [CrossRef]
- Sejnowski, T.J. Making smooth moves. Nature 1998, 394, 725–726. [Google Scholar] [CrossRef]
- Bosecker, C.; Dipietro, L.; Volpe, B.; Krebs, H.I. Kinematic Robot-Based Evaluation Scales and Clinical Counterparts to Measure Upper Limb Motor Performance in Patients With Chronic Stroke. Neurorehabilit. Neural Repair 2010, 24, 62–69. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Melendez-Calderon, A.; Burdet, E. A robust and sensitive metric for quantifying movement smoothness. IEEE Trans. Biomed. Eng. 2012, 59, 2126–2136. [Google Scholar] [CrossRef] [PubMed]
- Hogan, N.; Sternad, D. Sensitivity of Smoothness Measures to Movement Duration, Amplitude, and Arrests. J. Mot. Behav. 2009, 41, 529–534. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Melendez-Calderon, A.; Roby-Brami, A.; Burdet, E. On the analysis of movement smoothness. J. Neuroeng. Rehabil. 2015, 12, 112. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.Y.; Chen, S.C.; Chen, J.J.J.; Fu, L.L.; Wang, Y.L. Kinesiological and kinematical analysis for stroke subjects with asymmetrical cycling movement patterns. J. Electromyogr. Kinesiol. 2005, 15, 587–595. [Google Scholar] [CrossRef]
- Sansare, A.; Behboodi, A.; Johnston, T.E.; Bodt, B.; Lee, S.C.K. Characterizing Cycling Smoothness and Rhythm in Children With and Without Cerebral Palsy. Front. Rehabil. Sci. 2021, 2, 12. [Google Scholar] [CrossRef] [PubMed]
- Ketcham, C.J.; Seidler, R.D.; Van Gemmert, A.W.A.; Stelmach, G.E. Age-related kinematic differences as influenced by task difficulty, target size, and movement amplitude. J. Gerontol. Ser. B 2002, 57, 54–64. [Google Scholar] [CrossRef]
- Teulings, H.L.; Contreras-Vidal, J.L.; Stelmach, G.E.; Adler, C.H. Parkinsonism reduces coordination of fingers, wrist, and arm in fine motor control. Exp. Neurol. 1997, 146, 159–170. [Google Scholar] [CrossRef]
- Smith, M.A.; Brandt, J.; Shadmehr, R. Motor disorder in Huntington’s disease begins as a dysfunction in error feedback control. Nature 2000, 403, 544–549. [Google Scholar] [CrossRef]
- Platz, T.; Denzler, P.; Kaden, B.; Mauritz, K.H. Motor learning after recovery from hemiparesis. Neuropsychologia 1994, 32, 1209–1223. [Google Scholar] [CrossRef]
- Montes, V.R.; Quijano, Y.; Chong Quero, J.E.; Ayala, D.V.; Perez Moreno, J.C. Comparison of 4 different smoothness metrics for the quantitative assessment of movement’s quality in the upper limb of subjects with cerebral palsy. In Proceedings of the Pan American Health Care Exchanges (PAHCE), IEEE Computer Society, Brasilia, Brazil, 7–12 April 2014. [Google Scholar]
- Quijano-Gonzalez, Y.; Melendez-Calderon, A.; Burdet, E.; Chong-Quero, J.E.; Villanueva-Ayala, D.; Pérez-Moreno, J.C. Upper limb functional assessment of children with cerebral palsy using a sorting box. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBC 2014, Chicago, IL, USA, 26–30 August 2014; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2014; pp. 2330–2333. [Google Scholar]
- Anaya, L.; Quinones, I.; Quijano, Y.; Bueyes, V.; Chong, E.; Ponce, V. Clustering of Data that Quantify the Degree of Impairment of the Upper Limb in Patients with Alterations of the Central Nervous System. In Proceedings of the 2020 17th International Conference on Electrical Engineering, Computing Science and Automatic Control, CCE 2020, Mexico City, Mexico, 11–13 November 2020. [Google Scholar]
- Chen, J.-J.J.; Chen, H.-Y.; Chen, S.-C.; Chen, C.-C. Clinical applications of FES-cycling to SCI and stroke subjects for smoother and symmetrical movement patterns. In Proceedings of the 11th Annual Conference of the International FES Society, Miyangi-Zao, Japan, 12–15 September 2006. [Google Scholar]
- Lin, S.I.; Lo, C.C.; Lin, P.Y.; Chen, J.J.J. Biomechanical assessments of the effect of visual feedback on cycling for patients with stroke. J. Electromyogr. Kinesiol. 2012, 22, 582–588. [Google Scholar] [CrossRef]
- Linder, S.M.; Rosenfeldt, A.B.; Bazyk, A.S.; Koop, M.M.; Ozinga, S.; Alberts, J.L. Improved lower extremity pedaling mechanics in individuals with stroke under maximal workloads. Top. Stroke Rehabil. 2018, 25, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Quian Quiroga, R.; Kraskov, A.; Kreuz, T.; Grassberger, P. Performance of different synchronization measures in real data: A case study on electroencephalographic signals. Phys. Rev. E 2002, 65, 14. [Google Scholar] [CrossRef] [PubMed]
- Penney, G.P.; Weese, J.; Little, J.A.; Desmedt, P.; Hill, D.L. A comparison of similarity measures for use in 2-D-3-D medical image registration. IEEE Trans. Med. Imaging 1998, 17, 586–595. Available online: https://ieeexplore.ieee.org/ (accessed on 10 January 2020). [CrossRef] [PubMed]
- Palisano, R.; Rosenbaum, P.L.; Russell, D.; Galuppi, B.E. Development and reliability of a system to classify gross motor function in children with Cerebral Palsy ICF into Practice View project Development and initial validation of an assessment of visual ability for children with cerebral palsy View project. Artic. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef]
- Sansare, A.; Harrington, A.T.; Wright, H.; Alesi, J.; Behboodi, A.; Verma, K.; Lee, S.C.K. Aerobic Responses to FES-Assisted and Volitional Cycling in Children with Cerebral Palsy. Sensors 2021, 21, 7590. [Google Scholar] [CrossRef] [PubMed]
- Johnston, T.E.; Prosser, L.A.; Lee, S.C. Differences in pedal forces during recumbent cycling in adolescents with and without cerebral palsy. Clin. Biomech. 2008, 23, 248–251. Available online: https://www.ncbi.nlm.nih.gov/ (accessed on 10 January 2020). [CrossRef]
- Harrington, A.T.; McRae, C.G.A.; Lee, S.C.K. Evaluation of Functional Electrical Stimulation to Assist Cycling in Four Adolescents with Spastic Cerebral Palsy. Int. J. Pediatr. 2012, 2012, 1–11. [Google Scholar] [CrossRef]
- Comrey, A.; Lee, H. A First Course in Factor Analysis, 2nd ed.; Psychology Press: New York, NY, USA, 1992. [Google Scholar]
- Lachenbruch, P.A. An almost unbiased method of obtaining confidence intervals for the probability of misclassification in discriminant analysis. Biometrics 1967, 23, 639–645. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 7th ed.; Allyn & Bacon/Pearson Education: Boston, MA, USA, 2019; ISBN 978-0-13-479054-1. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Ages 10–18. Diagnosis of spastic CP. | Lower-extremity orthopedic surgery or traumatic fracture within the past 6 months. |
| GMFCS II, III, or IV. Adequate range of motion of the hips, knees, and ankles to allow pedaling. Visuoperceptual skills and cognitive/communication skills to follow multiple-step commands for attending to exercise and data collection. Ability to communicate pain or discomfort with testing and training procedures. | Lower-extremity joint pain during cycling. Spinal fusion extending to the pelvis. Hip, knee, or ankle joint instability or dislocation. Lower-limb stress fractures in the past year. Symptomatic or current diagnosis of cardiac disease as assessed by the American Heart Association guidelines for cardiac history. Current pulmonary disease or asthma and taking oral steroids or hospitalized for an acute episode in the past 6 months. Severe spasticity in legs (score of 4 on the Modified Ashworth Scale). Severely limited joint range of motion or irreversible muscle contractures that prevented safe positioning on the cycle. Diagnosis of athetoid or ataxic CP. Less than six months following Botox injections to the leg muscles. |
| crankIS | A line form by concatenating the angle data of each revolution in series |
| carnkRPM | The instantaneous RPM of crankIS |
| crankIDL | That connected the beginning to the end of angle-in-series data points |
| crankSim | The simulated crankIS using the aberrant revolutions of CP subjects |
| CP | TD | |||
|---|---|---|---|---|
| Cycling Smoothness | M | SD | M | SD |
| DJ | 0.031 | 0.119 | 0.007 | 0.010 |
| SALM | −2.871 | 0.428 | −11.900 | 0.374 |
| RI | 5523.579 | 14,136.316 | 2.281 | 1.156 |
| ArcL | −0.008 | 0.006 | −0.997 | 0.001 |
| XCorr | 0.039 | 0.058 | 0.006 | 0.003 |
| RMSE | 120.165 | 155.602 | 4.298 | 1.804 |
| Variable | Within-Group Correlation |
|---|---|
| ArcL | 0.576 |
| DJ | 0.545 |
| RMSE | 0.086 |
| SALM | 0.064 |
| Xcorr | 0.061 |
| RI | 0.045 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Behboodi, A.; Sansare, A.; Lee, S.C.K. Quantification of Cycling Smoothness in Children with Cerebral Palsy. Biomechanics 2023, 3, 79-92. https://doi.org/10.3390/biomechanics3010008
Behboodi A, Sansare A, Lee SCK. Quantification of Cycling Smoothness in Children with Cerebral Palsy. Biomechanics. 2023; 3(1):79-92. https://doi.org/10.3390/biomechanics3010008
Chicago/Turabian StyleBehboodi, Ahad, Ashwini Sansare, and Samuel C. K. Lee. 2023. "Quantification of Cycling Smoothness in Children with Cerebral Palsy" Biomechanics 3, no. 1: 79-92. https://doi.org/10.3390/biomechanics3010008
APA StyleBehboodi, A., Sansare, A., & Lee, S. C. K. (2023). Quantification of Cycling Smoothness in Children with Cerebral Palsy. Biomechanics, 3(1), 79-92. https://doi.org/10.3390/biomechanics3010008