
The Chart Diagnostic System Improves the Diagnostic Accuracy of Cervical Lymph Node Metastasis in Oral Squamous Cell Carcinoma

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Image Analysis
2.2.1. Protocol for Contrast-Enhanced CT and US
2.2.2. Protocol for 18F FDG-PET/CT
2.3. Diagnosis of Clinical Nodal Status
2.4. Pathological Examination
2.5. Definite Diagnosis of Cervical Lymph Nodal Status
2.6. Statistical Analysis
3. Results
4. Discussion
4.1. Imaging Analysis
4.2. Pathological Factor
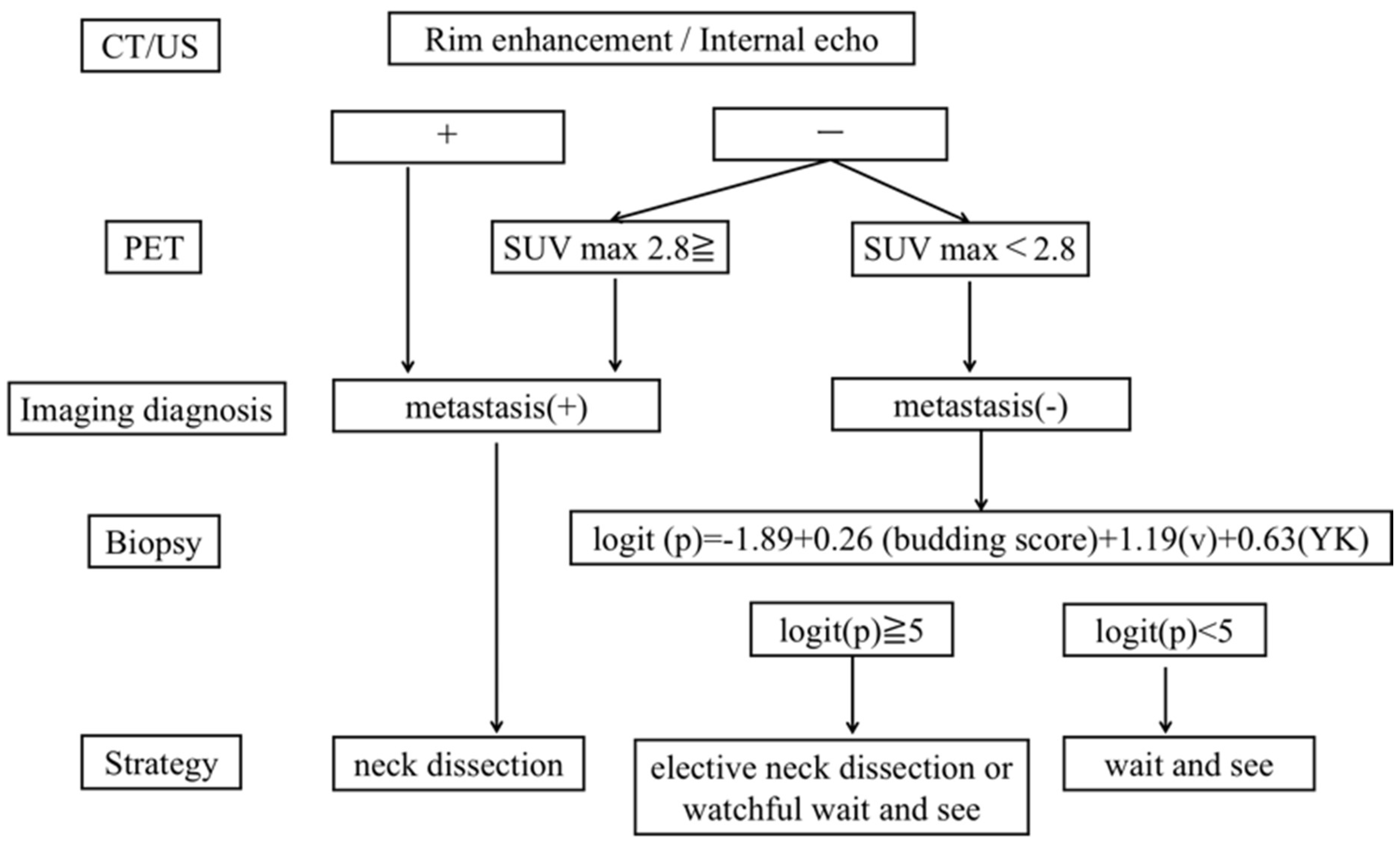
4.3. New Established Diagnostic Chart System
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beenken, S.W.; Krontiras, H.; Maddox, W.A.; Peters, G.E.; Soong, S.; Urist, M. T1 and T2 squamous cell carcinoma of the oral tongue: Prognostic factors and the role of elective lymph node dissection. Head Neck 1999, 21, 124–130. [Google Scholar] [CrossRef]
- Okamoto, M.; Nishimine, M.; Kishi, M.; Kirita, T.; Sugimura, M.; Nakamura, M.; Konishi, N. Prediction of delayed neck metastasis in patients with stage I/II squamous cell carcinoma of the tongue. J. Oral Pathol. Med. 2002, 31, 227–233. [Google Scholar] [CrossRef] [PubMed]
- El-Naaj, I.A.; Leiser, Y.; Shveis, M.; Sabo, E.; Peled, M. Incidence of Oral Cancer Occult Metastasis and Survival of T1-T2N0 OralCancer Patients. J. Oral Maxillofac. Surg. 2011, 69, 2674–2679. [Google Scholar] [CrossRef]
- Tânia, A.; Addah, F.; André, C.; Clóvis, P.; Luiz, K. Predictive factors of occult metastasis and prognosis of clinical stages I and II squamous cell carcinoma of the tongue and floor of the mouth. Oral Oncol. 2004, 40, 780–786. [Google Scholar] [CrossRef]
- Fernando, L.D.; Roberto, A.L.; Jacob, K.; Terence, P.F.; Jose, N.S.; Gabriel, M.; Geraldo, M.S. Relevance of Skip Metastases for Squamous Cell Carcinoma of the Oral Tongue and the Floor of the Mouth. Otolaryngol. Head Neck Surg. 2006, 134, 460–465. [Google Scholar] [CrossRef]
- Ishida, T.; Hijioka, H.; Kume, K.; Yoshimura, T.; Miyawaki, A.; Nozoe, E.; Suenaga, S.; Indo, H.; Majima, H.; Nakamura, N. A diagnosis system for detecting cervical lymph node metastasis in oral squamous cell carcinoma: Collective consideration of the results of multiple imaging modalities. J. Oral. Maxillofac. Surg. Med. Pathol. 2017, 29, 210–216. [Google Scholar] [CrossRef]
- Barnier, J.; Domenge, C.; Ozahin, M.; Matuszewska, K.; Lefèbvre, J.L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; et al. Postoperative Irradiation with or without Concomitant Chemotherapy for Locally Advanced Head and Neck Cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef]
- Wang, C.; Huang, H.; Huang, Z.; Wang, A.; Chen, X.; Huang, L.; Zhou, X.; Liu, X. Tumor budding correlates with poor prognosis and epithelial-mesenchymal transition in tongue squamous cell carcinoma. J. Oral Pathol. Med. 2011, 40, 545–551. [Google Scholar] [CrossRef]
- Xie, N.; Wang, C.; Liu, X.; Li, R.; Hou, J.; Chen, X.; Hung, H. Tumor budding correlates with occult cervical lymph node metastasis and poor prognosis in clinical early-stage tongue squamous cell carcinoma. J. Oral Pathol. Med. 2014, 44, 266–272. [Google Scholar] [CrossRef]
- Sakata, J.; Yamana, K.; Yoshida, R.; Matsuoka, Y.; Kawahara, K.; Arita, H.; Nakashima, H.; Nagata, M.; Hirosue, A.; Kawaguchi, S.; et al. Tumor budding as a novel predictor of occult metastasis in cT2N0 tongue squamous cell carcinoma. Hum. Pathol. 2018, 76, 1–8. [Google Scholar] [CrossRef]
- Steinkamp, H.; Cornehl, M.; Hosten, N.; Pegios, W.; Vogl, T.; Felix, R. Cervical lymphadenopathy: Ratio of long-to short-axis diameter as a predictor of malignancy. Br. J. Radiol. 1995, 68, 266–270. [Google Scholar] [CrossRef]
- Yuasa, K.; Kawazu, T.; Nagata, T.; Kanda, S.; Ohishi, M.; Shirasuna, K. Computed tomography and ultrasonography of metastatic cervical lymph nodes in oral squamous cell carcinoma. Dentomaxillofac. Radiol. 2000, 29, 238–244. [Google Scholar] [CrossRef]
- Norling, R.; Buron, B.; Therkilden, M.H.; Henriksen, B.M.; Buchwald, C.; Nielsen, M.B. Staging of Cervical Lymph Nodes in Oral Squamous Cell Carcinoma: Adding Ultrasound in Clinically Lymph Node Negative Patients May Improve Diagnostic Work-Up. PLoS ONE 2014, 20, e90360. [Google Scholar] [CrossRef]
- Ceylan, Y.; Omur, O.; Hatipoglu, F. Contribution of (18)F-FDG PET/CT to staging of head and neck malignancies. Mol. Imaging Radionucl. Ther. 2018, 27, 19–24. [Google Scholar] [CrossRef]
- Ng, H.; Yen, C.; Liao, T.; Chang, T.; Chan, C.; Ko, F.; Wang, M.; Wong, F. 18F-FDG PET and CT/MRI in oral cavity squamous cell carcinoma: A prospective study of 124 patients with histologic correlation. J. Nucl. Med. 2005, 46, 1136–1143. [Google Scholar]
- Roh, J.L.; Yeo, N.K.; Kim, J.S.; Lee, J.H.; Cho, K.J.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Utility of 2-[18F] fluoro-2-deoxy-d-glucose positron emission tomography and positron emission tomography/computed tomography imaging in the preoperative staging of head and neck squamous cell carcinoma. Oral Oncol. 2007, 43, 887–893. [Google Scholar] [CrossRef]
- Laimer, J.; Lauinger, A.; Steinmassl, O.; Offermanns, V.; Grams, A.; Zwlger, B.; Bruckmoser, E. Cervical lymph node metastasis in oral squamous cell carcinoma-How much imaging do we need? Diagnostics 2020, 10, 199. [Google Scholar] [CrossRef]
- Bae, M.R.; Roh, J.L.; Kim, J.S.; Lee, J.H.; Cho, K.J.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. 18F-FDG PET/CT versus CT/MR imaging for detection of neck lymph node metastasis in palpably node-negative oral cavity cancer. J. Cancer Res. Clin. Oncol. 2020, 46, 237–244. [Google Scholar] [CrossRef]
- Linz, C.; Brands, C.R.; Herterich, T.; Hartmann, S.; Richter, M.U.; Kubler, C.A.; Hang, L.; Kertels, O.; Bley, A.T.; Dierks, A.; et al. Accuracy of 18-F Fluorodeoxyglucose Positron Emission Tomographic/Computed Tomographic Imaging in Primary Staging of Squamous Cell Carcinoma of the Oral Cavity. JAMA Open 2021, 4, e217083. [Google Scholar] [CrossRef]
- Caylakli, F.; Yilmaz, S.; Ozer, C.; Reyhan, M. The Role of PET-CT in Evaluation of Cervical Lymph Node Metastases in Oral Cavity Squamous Cell Carcinomas. Turk. Arch. Otorhinolaryngol. 2015, 53, 67–72. [Google Scholar] [CrossRef]
- Cheng, G.; Huang, H. Prognostic value of 18F-fluorodeoxyglucose PET/computed tomography in non–small-cell lung Cancer. PET Clin. 2018, 13, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Bosio, G.; Bianchetti NPagani, C.; Re, A.; Tucci, A.; Giubbini, R.; Bertagna, F. Prognosticroleofbaseline18F-FDG PET/CT metabolic parameters in mantle cell lymphoma. Ann. Nucl. Med. 2019, 33, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Lai, W.; David, K.; Hugh, M.; Jacintha, O.; David, F.; John, H.; Diarmuid, O.; Kieran, S. Tumor budding is a strong and reproducible prognostic marker in T3N0 colorectal cancer. Am. J. Surg. Pathol. 2009, 33, 134–141. [Google Scholar] [CrossRef]
- Helvécio, J.; Priscila, L.R.L.; Victória, M.; Ângela, C.; Paulo, S.; Maria, A.; Martinho, H. Cell proliferation is associated with intensity of tumor budding in oral squamous cell carcinoma. J. Oral Pathol. Med. 2018, 47, 128–135. [Google Scholar] [CrossRef]
- Yamada, S.; Otsuru, M.; Yanamoto, S.; Hasegawa, T.; Aizawa, H.; Kamata, T.; Yamakawa, N.; Kohgom, T.; Ito, A.; Noda, Y.; et al. Progression level of extracapsular spread and tumor budding for cervical lymph node metastasis of OSCC. Clin. Oral Investig. 2018, 22, 1311–1318. [Google Scholar] [CrossRef]
- Yamakawa, N.; Kirita, T.; Umeda, M.; Yanamoto, S.; Ota, Y.; Otsuru, M.; Okura, M.; Kurita, H.; Yamada, S.; Hasegawa, T.; et al. Tumor budding and adjacent tissue at the invasive front correlate with delayed neck metastasis in clinical early-stage tongue squamous cell carcinoma. J. Surg. Oncol. 2019, 119, 370–378. [Google Scholar] [CrossRef]
- Mscitti, M.; Tongi, L.; Caponio, V.; Zhurakivska, L.; Muzio, L.; Rubini, C.; Santnrelli, A.; Triano, G. Prognostic significance of tumor budding thresholds in oral tongue squamous cell carcinoma. Oral Dis. 2022. [Google Scholar] [CrossRef]
- Matthias, T.; Selgai, H.; Sophie, B.; Markus, T.; Florian PMichael, E.; Sven, O. What Factors Are Associated with Regional Recurrence After Operative Treatment of Oral Squamous Cell Carcinoma? J. Oral Maxillofac. Surg. 2018, 76, 2650–2659. [Google Scholar] [CrossRef]
- Barnes, L.; Eveson, J.; Reichart, P.; Sidransky, D. World Health Organization Classification of Timours, Pathology & Genetics, Head and Neck Tumors, 4th ed.; IARC Press: London, UK, 2005; pp. 168–175. [Google Scholar]
- Yamamoto, E.; Miyakawa, A.; Kohama, G. Mode of invasion and lymph node metastasis in squamous cell carcinoma of the oral cavity. Head Neck Surg. 1984, 6, 938–947. [Google Scholar] [CrossRef]
- Coper, J.S.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.J.; Campbell, B.H.; Saxman, S.B.; Kish, J.K.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2004, 350, 1937–1944. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| pN(+) Group | pN(−) Group | p Value | |
|---|---|---|---|
| Number | 22 | 51 | |
| age | 64.7 ± 14.0 | 67.1 ± 12.1 | 0.462 |
| sex | |||
| male | 14 | 30 | 0.699 |
| female | 8 | 21 | |
| cT clssification | |||
| T1 | 3 | 10 | 0.629 |
| T2 | 14 | 27 | |
| T3 | 4 | 8 | |
| T4 | 1 | 6 | |
| Primary tumor | |||
| Tongue | 11 | 22 | 0.419 |
| Floor of mouth | 2 | 6 | |
| Mandibular | 32 | 12 | |
| Maxilla | 4 | 8 | |
| Buccal mucosa | 2 | 3 | |
| cN0 | 7 | 31 | 0.018 * |
| cN1/2 | 15 | 20 | |
| late metastasis | 5 | 0 | - |
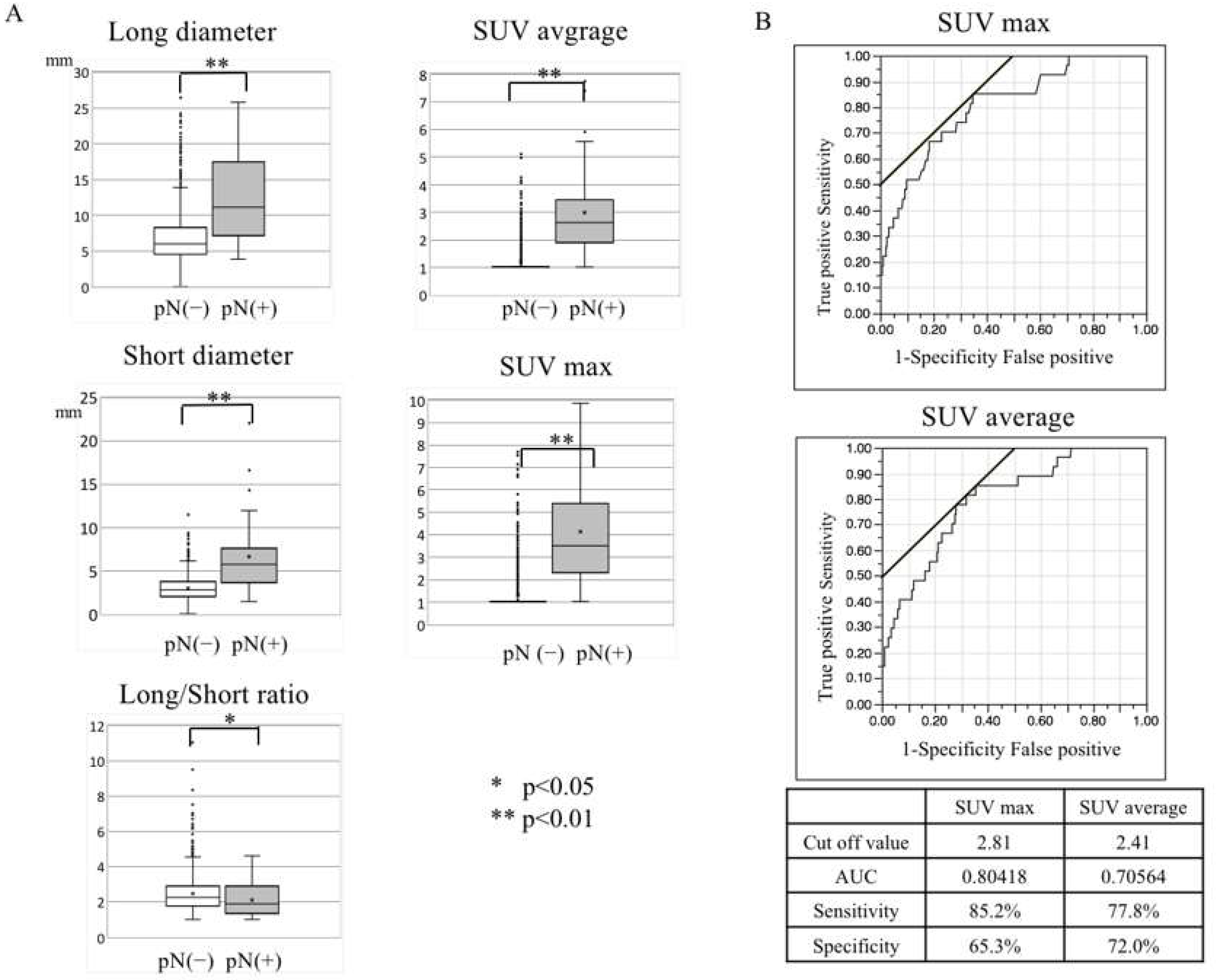
| Imaging Feature | χ2 Test | Result of Logistic Regression Analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|
| pN(+) LNs | pN(−) LNs | p Value | Univariate Analysis | Multivariable Analysis | |||||
| n = 33 | n = 1554 | OR | 95% Cl | p Value | OR | 95% Cl | p Value | ||
| Long diameter | 11.1 (7.1–17.4) | 6.0 (4.6–8.2) | <0.001 ** | 1.23 | 1.16–1.31 | <0.001 ** | - | - | - |
| Short diameter | 4.6 (3.6–5.9) | 2.7 (2.0–3.6) | <0.001 ** | 1.98 | 1.67–2.36 | <0.001 ** | - | - | - |
| Long/Short ratio | 1.9 (1.3–2.9) | 2.2 (1.8–2.9) | 0.042 * | 0.60 | 0.36–0.94 | 0.038 * | - | - | - |
| US observation | |||||||||
| Hilum | |||||||||
| Clear/unclear | 21/6 | 687/569 | 0.886 | 0.94 | 0.89–2.14 | 0.885 | - | - | - |
| disappearance | 6 | 298 | |||||||
| Internal echo | |||||||||
| None/unclear | 14/4 | 1452/87 | <0.001 ** | 109.0 | 47.1–260.9 | <0.001 ** | 16.37 | 4.00–57.78 | <0.001 ** |
| Appearance | 17 | 15 | |||||||
| CT contrast effect | |||||||||
| None/heterogeneity | 14/5 | 1506/43 | <0.001 ** | 228.3 | 79.1–767.5 | <0.001 ** | 5.58 | 1.08–31.64 | 0.045 * |
| Rim enhancement | 14 | 5 | |||||||
| SUV max | 3.5 (2.3–5.4) | 1.0 (1.0–1.0) | <0.001 ** | 2.51 | 2.07–3.10 | <0.001 ** | 2.11 | 1.66–2.68 | <0.001 ** |
| SUV average | 2.6 (1.9–3.4) | 1.0 (1.0–1.0) | <0.001 ** | 4.51 | 3.26–6.45 | <0.001 ** | - | - | - |
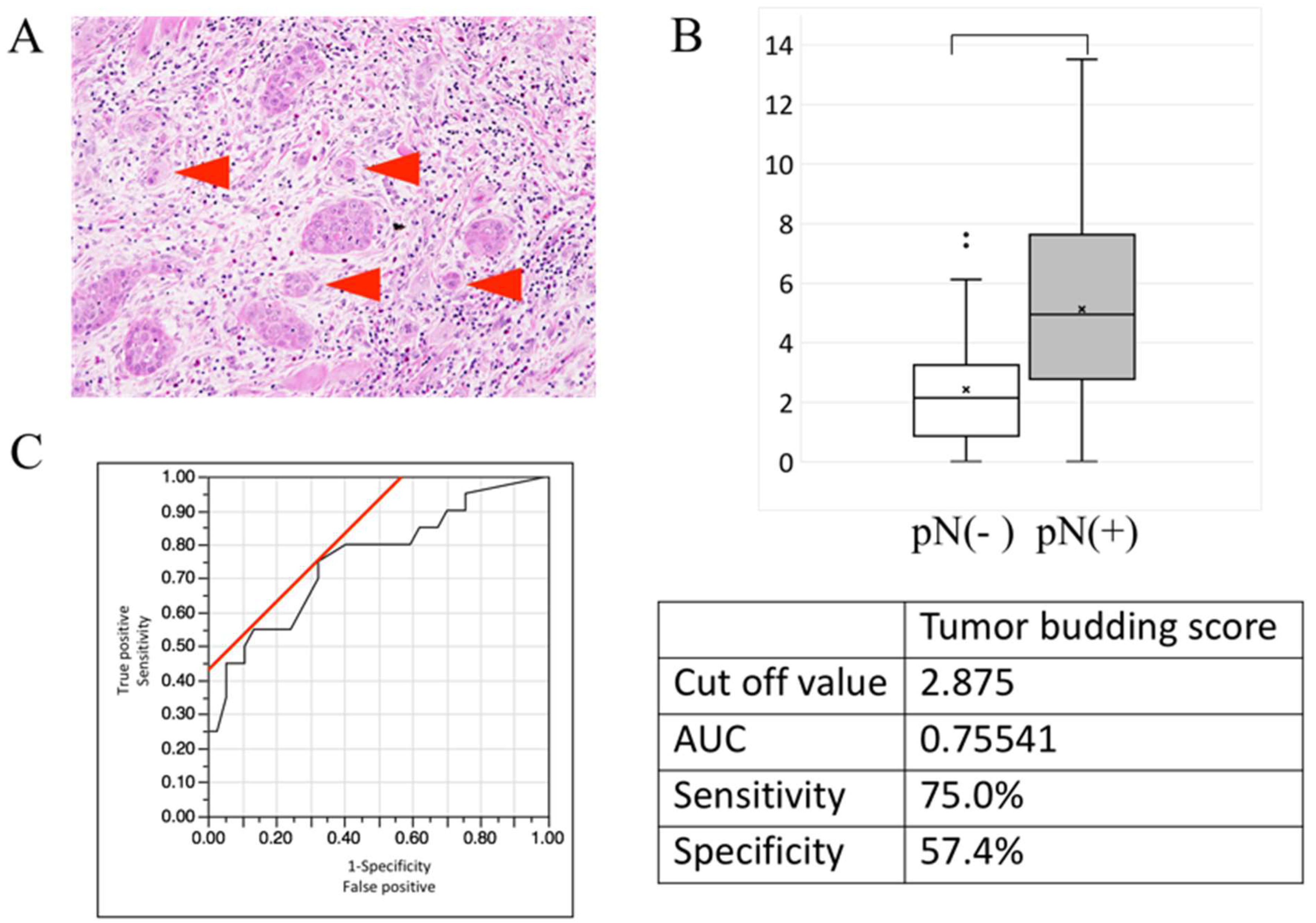
| Pathological Factor | χ2 Test | Result of Logistic Regression Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| pN(+) Group | pN(−) Group | p Value | Univariate Analysis | Multivariable Analysis | ||||||
| n = 20 | n = 37 | OR | 95% Cl | p Value | OR | 95% Cl | p Value | |||
| Budding score | 5.12 ± 3.57 | 2.24 ± 2.12 | <0.001 ** | 1.44 | 1.17–1.87 | <0.001 ** | 1.30 | 0.99–1.73 | 0.043 * | |
| ly | none | 20 | 37 | - | - | - | - | - | - | - |
| positive | 0 | 0 | ||||||||
| v | none | 12 | 34 | 0.004 * | 7.56 | 0.85–39.1 | 0.042 * | 3.31 | 0.17–20.6 | 0.172 |
| positive | 8 | 3 | ||||||||
| pn | none | 20 | 35 | 0.290 | - | - | - | - | - | - |
| positive | 0 | 2 | ||||||||
| YK classification | ||||||||||
| 2/3 | 0/13 | 6/27 | 0.069 | 3.54 | 0.88–15.7 | 0.075 | 1.87 | 0.33–10.3 | 0.467 | |
| 4C/4D | 4/2 | 3/1 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nomura, A.; Ishida, T.; Hijioka, H.; Yoshimura, T.; Suzuki, H.; Nozoe, E.; Nakamura, N. The Chart Diagnostic System Improves the Diagnostic Accuracy of Cervical Lymph Node Metastasis in Oral Squamous Cell Carcinoma. Onco 2023, 3, 53-64. https://doi.org/10.3390/onco3010005
Nomura A, Ishida T, Hijioka H, Yoshimura T, Suzuki H, Nozoe E, Nakamura N. The Chart Diagnostic System Improves the Diagnostic Accuracy of Cervical Lymph Node Metastasis in Oral Squamous Cell Carcinoma. Onco. 2023; 3(1):53-64. https://doi.org/10.3390/onco3010005
Chicago/Turabian StyleNomura, Ayako, Takayuki Ishida, Hiroshi Hijioka, Takuya Yoshimura, Hajime Suzuki, Eturo Nozoe, and Norifumi Nakamura. 2023. "The Chart Diagnostic System Improves the Diagnostic Accuracy of Cervical Lymph Node Metastasis in Oral Squamous Cell Carcinoma" Onco 3, no. 1: 53-64. https://doi.org/10.3390/onco3010005
APA StyleNomura, A., Ishida, T., Hijioka, H., Yoshimura, T., Suzuki, H., Nozoe, E., & Nakamura, N. (2023). The Chart Diagnostic System Improves the Diagnostic Accuracy of Cervical Lymph Node Metastasis in Oral Squamous Cell Carcinoma. Onco, 3(1), 53-64. https://doi.org/10.3390/onco3010005