
Effectiveness of COVID-19 Vaccination on Transmission: A Systematic Review

 ,
,
Abstract
:1. Introduction
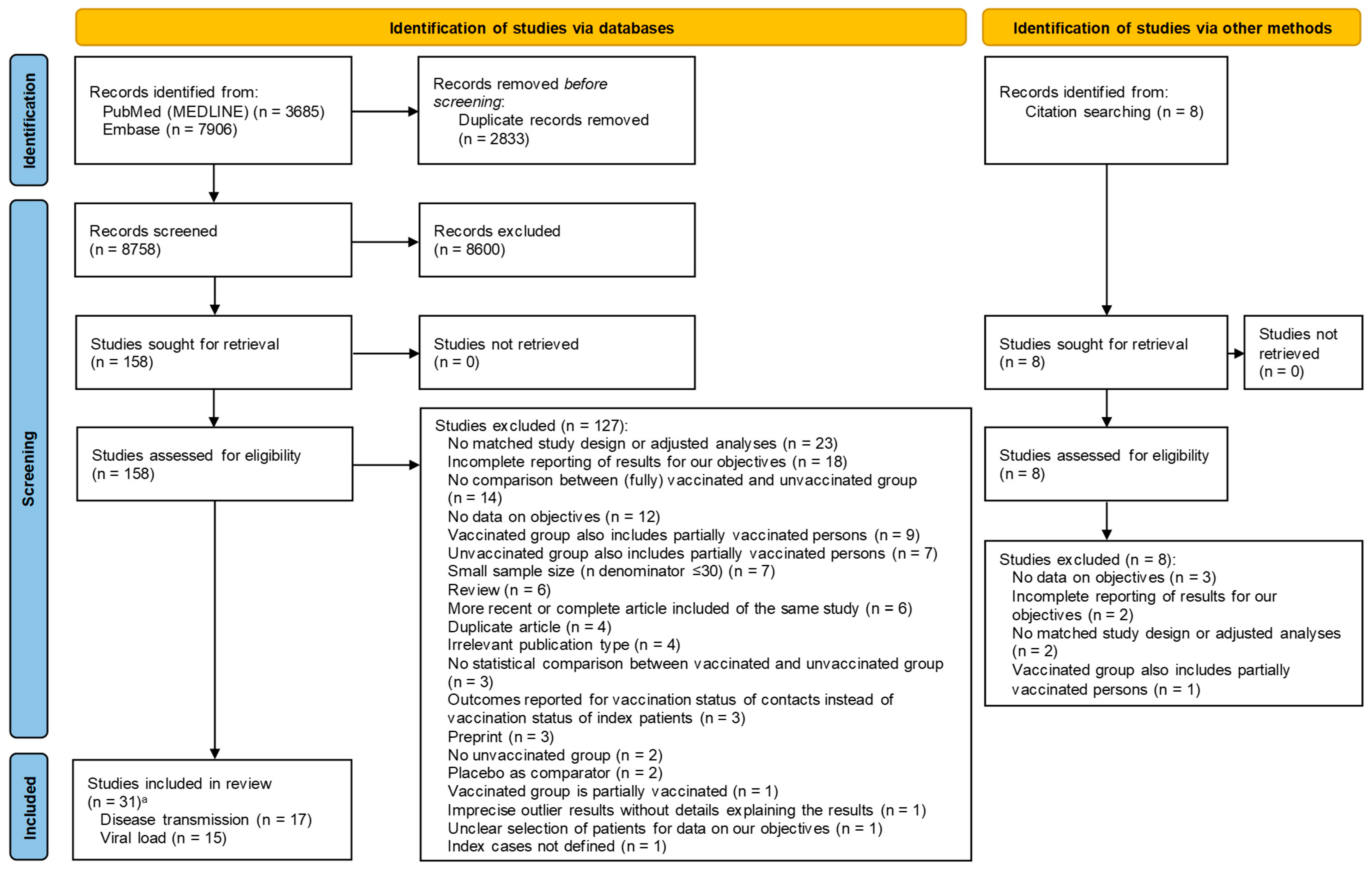
2. Materials and Methods
3. Results
3.1. Study Characteristics
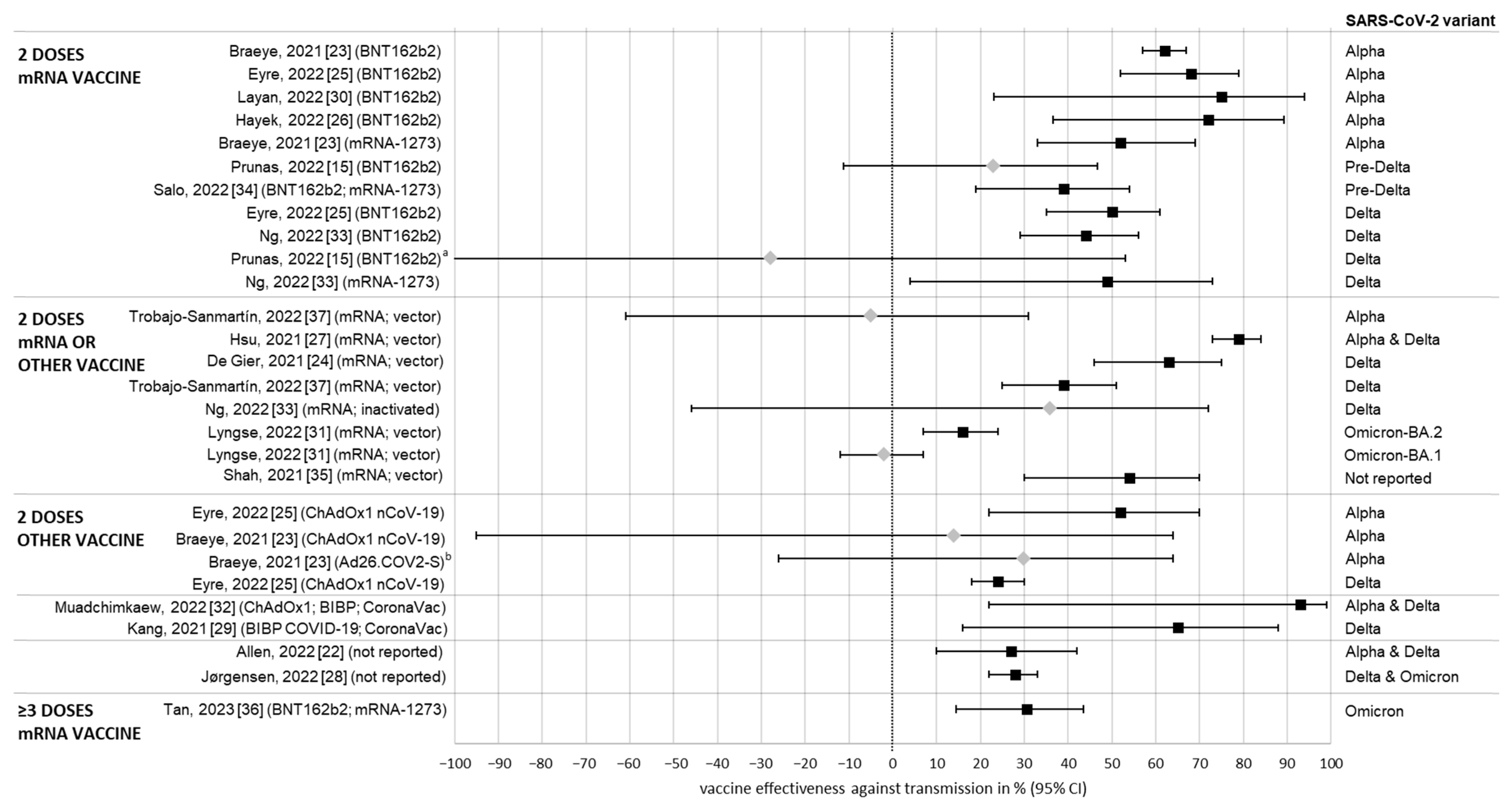
3.2. Vaccine Effects on Transmission
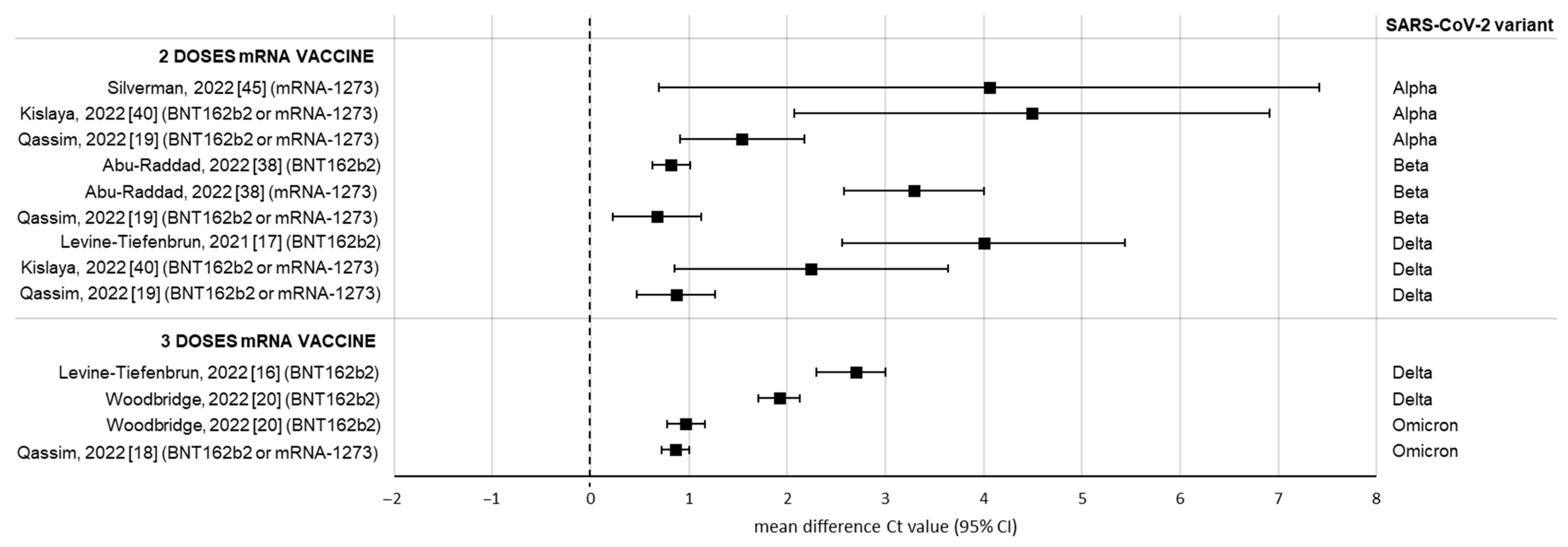
3.3. Vaccine Effects on Viral Load
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Timeline: WHO’s COVID-19 Response. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline# (accessed on 31 March 2023).
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 18 September 2023).
- Zhou, F.; Hu, T.-J.; Zhang, X.-Y.; Lai, K.; Chen, J.-H.; Zhou, X.-H. The Association of Intensity and Duration of Non-Pharmacological Interventions and Implementation of Vaccination with COVID-19 Infection, Death, and Excess Mortality: Natural Experiment in 22 European Countries. J. Infect. Public Health 2022, 15, 499–507. [Google Scholar] [CrossRef]
- Lison, A.; Banholzer, N.; Sharma, M.; Mindermann, S.; Unwin, H.J.T.; Mishra, S.; Stadler, T.; Bhatt, S.; Ferguson, N.M.; Brauner, J. Effectiveness Assessment of Non-Pharmaceutical Interventions: Lessons Learned from the COVID-19 Pandemic. Lancet Public Health 2023, 8, e311–e317. [Google Scholar] [CrossRef]
- Iezadi, S.; Gholipour, K.; Azami-Aghdash, S.; Ghiasi, A.; Rezapour, A.; Pourasghari, H.; Pashazadeh, F. Effectiveness of Non-Pharmaceutical Public Health Interventions against COVID-19: A Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0260371. [Google Scholar] [CrossRef]
- Talic, S.; Shah, S.; Wild, H.; Gasevic, D.; Maharaj, A.; Ademi, Z.; Li, X.; Xu, W.; Mesa-Eguiagaray, I.; Rostron, J. Effectiveness of Public Health Measures in Reducing the Incidence of COVID-19, SARS-CoV-2 Transmission, and COVID-19 Mortality: Systematic Review and Meta-Analysis. BMJ 2021, 375, e068302. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, S.H.; Mansatta, K.; Mallett, G.; Harris, V.; Emary, K.R.W.; Pollard, A.J. What Defines an Efficacious COVID-19 Vaccine? A Review of the Challenges Assessing the Clinical Efficacy of Vaccines against SARS-CoV-2. Lancet Infect. Dis. 2021, 21, e26–e35. [Google Scholar] [CrossRef]
- Young, M.; Crook, H.; Scott, J.; Edison, P. COVID-19: Virology, Variants, and Vaccines. BMJ Med. 2022, 1, e000040. [Google Scholar] [CrossRef] [PubMed]
- Pollard, A.J.; Bijker, E.M. A Guide to Vaccinology: From Basic Principles to New Developments. Nat. Rev. Immunol. 2021, 21, 83–100. [Google Scholar] [CrossRef]
- Richterman, A.; Meyerowitz, E.A.; Cevik, M. Indirect Protection by Reducing Transmission: Ending the Pandemic with Severe Acute Respiratory Syndrome Coronavirus 2 Vaccination. Open Forum Infect. Dis. 2022, 9, ofab259. [Google Scholar] [CrossRef] [PubMed]
- Binnicker, M.J. Can Testing Predict SARS-CoV-2 Infectivity? The Potential for Certain Methods to Be Surrogates for Replication-Competent Virus. J. Clin. Microbiol. 2021, 59, e00469-21. [Google Scholar] [CrossRef]
- Cochrane Emergency Critical Care Group. Efficacy and Safety of COVID-19 Vaccines. Cochrane Database Syst. Rev. 2023, 12, CD015477. [Google Scholar]
- Rahmani, K.; Shavaleh, R.; Forouhi, M.; Disfani, H.F.; Kamandi, M.; Oskooi, R.K.; Foogerdi, M.; Soltani, M.; Rahchamani, M.; Mohaddespour, M. The Effectiveness of COVID-19 Vaccines in Reducing the Incidence, Hospitalization, and Mortality from COVID-19: A Systematic Review and Meta-Analysis. Front. Public Health 2022, 10, 2738. [Google Scholar] [CrossRef]
- Zeng, B.; Gao, L.; Zhou, Q.; Yu, K.; Sun, F. Effectiveness of COVID-19 Vaccines against SARS-CoV-2 Variants of Concern: A Systematic Review and Meta-Analysis. BMC Med. 2022, 20, 200. [Google Scholar] [CrossRef] [PubMed]
- Prunas, O.; Warren, J.L.; Crawford, F.W.; Gazit, S.; Patalon, T.; Weinberger, D.M.; Pitzer, V.E. Vaccination with Bnt162b2 Reduces Transmission of SARS-CoV-2 to Household Contacts in Israel. Science 2022, 375, 1151–1154. [Google Scholar] [CrossRef] [PubMed]
- Levine-Tiefenbrun, M.; Yelin, I.; Alapi, H.; Herzel, E.; Kuint, J.; Chodick, G.; Gazit, S.; Patalon, T.; Kishony, R. Waning of SARS-CoV-2 Booster Viral-Load Reduction Effectiveness. Nat. Commun. 2022, 13, 1237. [Google Scholar] [CrossRef]
- Levine-Tiefenbrun, M.; Yelin, I.; Alapi, H.; Katz, R.; Herzel, E.; Kuint, J.; Chodick, G.; Gazit, S.; Patalon, T.; Kishony, R. Viral Loads of Delta-Variant SARS-CoV-2 Breakthrough Infections after Vaccination and Booster with Bnt162b2. Nat. Med. 2021, 27, 2108–2110. [Google Scholar] [CrossRef]
- Qassim, S.H.; Chemaitelly, H.; Ayoub, H.H.; AlMukdad, S.; Tang, P.; Hasan, M.R.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Abdul-Rahim, H.F.; et al. Effects of Ba.1/Ba.2 Subvariant, Vaccination and Prior Infection on Infectiousness of SARS-CoV-2 Omicron Infections. J. Travel Med. 2022, 29, taac068. [Google Scholar] [CrossRef]
- Qassim, S.H.; Hasan, M.R.; Tang, P.; Chemaitelly, H.; Ayoub, H.H.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Abdul-Rahim, H.F.; Nasrallah, G.K.; et al. Effects of SARS-CoV-2 Alpha, Beta, and Delta Variants, Age, Vaccination, and Prior Infection on Infectiousness of SARS-COV-2 Infections. Front. Immunol. 2022, 13, 984784. [Google Scholar] [CrossRef]
- Woodbridge, Y.; Amit, S.; Huppert, A.; Kopelman, N.M. Viral Load Dynamics of SARS-CoV-2 Delta and Omicron Variants Following Multiple Vaccine Doses and Previous Infection. Nat. Commun. 2022, 13, 6706. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 9 January 2023).
- Allen, H.; Vusirikala, A.; Flannagan, J.; Twohig, K.A.; Zaidi, A.; Chudasama, D.; Lamagni, T.; Groves, N.; Turner, C.; Rawlinson, C.; et al. Household Transmission of COVID-19 Cases Associated with SARS-CoV-2 Delta Variant (B.1.617.2): National Case-Control Study. Lancet Reg. Health Eur. 2022, 12, 100252. [Google Scholar] [CrossRef] [PubMed]
- Braeye, T.; Cornelissen, L.; Catteau, L.; Haarhuis, F.; Proesmans, K.; De Ridder, K.; Djiena, A.; Mahieu, R.; De Leeuw, F.; Dreuw, A.; et al. Vaccine Effectiveness against Infection and Onwards Transmission of COVID-19: Analysis of Belgian Contact Tracing Data, January-June 2021. Vaccine 2021, 39, 5456–5460. [Google Scholar] [CrossRef]
- De Gier, B.; Andeweg, S.; Backer, J.A.; Hahné, S.J.M.; van den Hof, S.; de Melker, H.E.; Knol, M.J. Vaccine Effectiveness against SARS-CoV-2 Transmission to Household Contacts During Dominance of Delta Variant (B.1.617.2), the Netherlands, August to September 2021. Eurosurveillance 2021, 26, 2100977. [Google Scholar] [CrossRef]
- Eyre, D.W.; Taylor, D.; Purver, M.; Chapman, D.; Fowler, T.; Pouwels, K.B.; Walker, A.S.; Peto, T.E.A. Effect of COVID-19 Vaccination on Transmission of Alpha and Delta Variants. N. Engl. J. Med. 2022, 386, 744–756. [Google Scholar] [CrossRef] [PubMed]
- Hayek, S.; Shaham, G.; Ben-Shlomo, Y.; Kepten, E.; Dagan, N.; Nevo, D.; Lipsitch, M.; Reis, B.Y.; Balicer, R.D.; Barda, N. Indirect Protection of Children from SARS-CoV-2 Infection through Parental Vaccination. Science 2022, 375, 1155–1159. [Google Scholar] [CrossRef]
- Hsu, L.; Grüne, B.; Buess, M.; Joisten, C.; Klobucnik, J.; Nießen, J.; Patten, D.; Wolff, A.; Wiesmüller, G.A.; Kossow, A.; et al. COVID-19 Breakthrough Infections and Transmission Risk: Real-World Data Analyses from Germany’s Largest Public Health Department (Cologne). Vaccines 2021, 9, 1267. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, S.B.; Nygård, K.; Kacelnik, O.; Telle, K. Secondary Attack Rates for Omicron and Delta Variants of SARS-CoV-2 in Norwegian Households. JAMA—J. Am. Med. Assoc. 2022, 327, 1610–1611. [Google Scholar] [CrossRef]
- Kang, M.; Xin, H.; Yuan, J.; Ali, S.T.; Liang, Z.; Zhang, J.; Hu, T.; Lau, E.H.; Zhang, Y.; Zhang, M.; et al. Transmission Dynamics and Epidemiological Characteristics of SARS-CoV-2 Delta Variant Infections in Guangdong, China, May to June 2021. Eurosurveillance 2022, 27, 2100815. [Google Scholar] [CrossRef] [PubMed]
- Layan, M.; Gilboa, M.; Gonen, T.; Goldenfeld, M.; Meltzer, L.; Andronico, A.; Hozé, N.; Cauchemez, S.; Regev-Yochay, G. Impact of Bnt162b2 Vaccination and Isolation on SARS-CoV-2 Transmission in Israeli Households: An Observational Study. Am. J. Epidemiol. 2022, 191, 1224–1234. [Google Scholar] [CrossRef]
- Lyngse, F.P.; Kirkeby, C.T.; Denwood, M.; Christiansen, L.E.; Mølbak, K.; Møller, C.H.; Skov, R.L.; Krause, T.G.; Rasmussen, M.; Sieber, R.N.; et al. Household Transmission of SARS-CoV-2 Omicron Variant of Concern Subvariants Ba.1 and Ba.2 in Denmark. Nat. Commun. 2022, 13, 5760. [Google Scholar] [CrossRef]
- Muadchimkaew, M.; Siripongboonsitti, T.; Wongpatcharawarakul, S.; Boonsankaew, C.; Tawinprai, K.; Soonklang, K.; Mahanonda, N. Effect of Inactivated SARS-CoV-2 Vaccines and Chadox1 Ncov-19 Vaccination to Prevent COVID-19 in Thai Households (Vacprevent Trial). Int. J. Infect. Dis. 2022, 124, 190–198. [Google Scholar] [CrossRef]
- Ng, O.T.; Koh, V.; Chiew, C.J.; Marimuthu, K.; Thevasagayam, N.M.; Mak, T.M.; Chua, J.K.; Ong, S.S.H.; Lim, Y.K.; Ferdous, Z.; et al. Impact of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccination and Pediatric Age on Delta Variant Household Transmission. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2022, 75, e35–e43. [Google Scholar] [CrossRef]
- Salo, J.; Hägg, M.; Kortelainen, M.; Leino, T.; Saxell, T.; Siikanen, M.; Sääksvuori, L. The Indirect Effect of Mrna-Based COVID-19 Vaccination on Healthcare Workers’ Unvaccinated Household Members. Nat. Commun. 2022, 13, 1162. [Google Scholar] [CrossRef]
- Shah, A.S.V.; Gribben, C.; Bishop, J.; Hanlon, P.; Caldwell, D.; Wood, R.; Reid, M.; McMenamin, J.; Goldberg, D.; Stockton, D.; et al. Effect of Vaccination on Transmission of SARS-CoV-2. N. Engl. J. Med. 2021, 385, 1718–1720. [Google Scholar] [CrossRef]
- Tan, S.T.; Kwan, A.T.; Rodríguez-Barraquer, I.; Singer, B.J.; Park, H.J.; Lewnard, J.A.; Sears, D.; Lo, N.C. Infectiousness of SARS-CoV-2 Breakthrough Infections and Reinfections During the Omicron Wave. Nat. Med. 2023, 29, 358–365. [Google Scholar] [CrossRef]
- Trobajo-Sanmartín, C.; Martínez-Baz, I.; Miqueleiz, A.; Fernández-Huerta, M.; Burgui, C.; Casado, I.; Baigorría, F.; Navascués, A.; Castilla, J.; Ezpeleta, C. Differences in Transmission between SARS-CoV-2 Alpha (B.1.1.7) and Delta (B.1.617.2) Variants. Microbiol. Spectr. 2022, 10, e00008-22. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; Tang, P.; Coyle, P.; Hasan, M.R.; Yassine, H.M.; Benslimane, F.M.; Al-Khatib, H.A.; Al-Kanaani, Z.; et al. Relative Infectiousness of SARS-CoV-2 Vaccine Breakthrough Infections, Reinfections, and Primary Infections. Nat. Commun. 2022, 13, 532. [Google Scholar] [CrossRef] [PubMed]
- Bramante, C.T.; Proper, J.L.; Boulware, D.R.; Karger, A.B.; Murray, T.; Rao, V.; Hagen, A.; Tignanelli, C.J.; Puskarich, M.; Cohen, K.; et al. Vaccination against SARS-CoV-2 Is Associated with a Lower Viral Load and Likelihood of Systemic Symptoms. Open Forum Infect. Dis. 2022, 9, ofac066. [Google Scholar] [CrossRef]
- Kislaya, I.; Rodrigues, E.F.; Borges, V.; Gomes, J.P.; Sousa, C.; Almeida, J.P.; Peralta-Santos, A.; Nunes, B. Comparative Effectiveness of Coronavirus Vaccine in Preventing Breakthrough Infections among Vaccinated Persons Infected with Delta and Alpha Variants. Emerg. Infect. Dis. 2022, 28, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Pouwels, K.B.; Pritchard, E.; Matthews, P.C.; Stoesser, N.; Eyre, D.W.; Vihta, K.D.; House, T.; Hay, J.; Bell, J.I.; Newton, J.N.; et al. Effect of Delta Variant on Viral Burden and Vaccine Effectiveness against New SARS-CoV-2 Infections in the Uk. Nat. Med. 2021, 27, 2127–2135. [Google Scholar] [CrossRef] [PubMed]
- Puhach, O.; Adea, K.; Hulo, N.; Sattonnet, P.; Genecand, C.; Iten, A.; Jacquérioz, F.; Kaiser, L.; Vetter, P.; Eckerle, I.; et al. Infectious Viral Load in Unvaccinated and Vaccinated Individuals Infected with Ancestral, Delta or Omicron SARS-CoV-2. Nat. Med. 2022, 28, 1491–1500. [Google Scholar] [CrossRef]
- Riemersma, K.K.; Haddock, L.A., III; Wilson, N.A.; Minor, N.; Eickhoff, J.; Grogan, B.E.; Kita-Yarbro, A.; Halfmann, P.J.; Segaloff, H.E.; Kocharian, A. Shedding of Infectious SARS-CoV-2 Despite Vaccination. PLoS Pathog. 2022, 18, e1010876. [Google Scholar] [CrossRef]
- Rife Magalis, B.; Rich, S.; Tagliamonte, M.S.; Mavian, C.; Cash, M.N.; Riva, A.; Marini, S.; Amador, D.M.; Zhang, Y.; Shapiro, J.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 Delta Vaccine Breakthrough Transmissibility in Alachua County, Florida. Clin. Infect. Dis. 2022, 75, 1618–1627. [Google Scholar] [CrossRef]
- Silverman, R.A.; Ceci, A.; Cohen, A.; Helmick, M.; Short, E.; Bordwine, P.; Friedlander, M.J.; Finkielstein, C.V. Vaccine Effectiveness During Outbreak of COVID-19 Alpha (B.1.1.7) Variant in Men’s Correctional Facility, United States. Emerg. Infect. Dis. 2022, 28, 1321–1326. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.G.; Yoon, S.K.; Naleway, A.L.; Meece, J.; Fabrizio, T.P.; Caban-Martinez, A.J.; Burgess, J.L.; Gaglani, M.; Olsho, L.E.W.; Bateman, A.; et al. Association of Mrna Vaccination with Clinical and Virologic Features of COVID-19 among Us Essential and Frontline Workers. JAMA 2022, 328, 1523–1533. [Google Scholar] [PubMed]
- Stephens, D.S. Protecting the Herd: The Remarkable Effectiveness of the Bacterial Meningitis Polysaccharide-Protein Conjugate Vaccines in Altering Transmission Dynamics. Trans. Am. Clin. Climatol. Assoc. 2011, 122, 115. [Google Scholar]
- Yin, J.K.; Heywood, A.E.; Georgousakis, M.; King, C.; Chiu, C.; Isaacs, D.; Macartney, K.K. Systematic Review and Meta-Analysis of Indirect Protection Afforded by Vaccinating Children against Seasonal Influenza: Implications for Policy. Clin. Infect. Dis. 2017, 65, 719–728. [Google Scholar] [CrossRef]
- Pather, S.; Madhi, S.A.; Cowling, B.J.; Moss, P.; Kamil, J.P.; Ciesek, S.; Muik, A.; Türeci, Ö. SARS-CoV-2 Omicron Variants: Burden of Disease, Impact on Vaccine Effectiveness and Need for Variant-Adapted Vaccines. Front. Immunol. 2023, 14, 1130539. [Google Scholar] [CrossRef] [PubMed]
- Kinross, P.; Suetens, C.; Dias, J.G.; Alexakis, L.; Wijermans, A.; Colzani, E.; Monnet, D.L. Rapidly Increasing Cumulative Incidence of Coronavirus Disease (COVID-19) in the European Union/European Economic Area and the United Kingdom, 1 January to 15 March 2020. Eurosurveillance 2020, 25, 2000285. [Google Scholar] [CrossRef]
- Kronfeld-Schor, N.; Stevenson, T.J.; Nickbakhsh, S.; Schernhammer, E.S.; Dopico, X.C.; Dayan, T.; Martinez, M.; Helm, B. Drivers of Infectious Disease Seasonality: Potential Implications for COVID-19. J. Biol. Rhythm. 2021, 36, 35–54. [Google Scholar] [CrossRef]
- Neumann, G.; Kawaoka, Y. Seasonality of Influenza and Other Respiratory Viruses. EMBO Mol. Med. 2022, 14, e15352. [Google Scholar] [CrossRef]
- Li, Y.; Reeves, R.M.; Wang, X.; Bassat, Q.; Brooks, W.A.; Cohen, C.; Moore, D.P.; Nunes, M.; Rath, B.; Campbell, H. Global Patterns in Monthly Activity of Influenza Virus, Respiratory Syncytial Virus, Parainfluenza Virus, and Metapneumovirus: A Systematic Analysis. Lancet Glob. Health 2019, 7, e1031–e1045. [Google Scholar] [CrossRef]
- Juneau, C.-E.; Pueyo, T.; Bell, M.; Gee, G.; Collazzo, P.; Potvin, L. Lessons from Past Pandemics: A Systematic Review of Evidence-Based, Cost-Effective Interventions to Suppress COVID-19. Syst. Rev. 2022, 11, 90. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Masum, M.H.U.; Wajed, S.; Talukder, A. A Comprehensive Review on COVID-19 Vaccines: Development, Effectiveness, Adverse Effects, Distribution and Challenges. Virusdisease 2022, 33, 1–22. [Google Scholar] [CrossRef] [PubMed]
- She, J.; Hou, D.; Chen, C.; Bi, J.; Song, Y. Challenges of Vaccination and Herd Immunity in COVID-19 and Management Strategies. Clin. Respir. J. 2022, 16, 708–716. [Google Scholar] [CrossRef] [PubMed]
- Sonabend, R.; Whittles, L.K.; Imai, N.; Perez-Guzman, P.N.; Knock, E.S.; Rawson, T.; Gaythorpe, K.A.M.; Djaafara, B.A.; Hinsley, W.; FitzJohn, R.G. Non-Pharmaceutical Interventions, Vaccination, and the SARS-CoV-2 Delta Variant in England: A Mathematical Modelling Study. Lancet 2021, 398, 1825–1835. [Google Scholar] [CrossRef] [PubMed]

 Significant effect.
Significant effect.  Non-significant effect.
Significant effect. Non-significant effect.
Non-significant effect.
Significant effect. Non-significant effect. Significant effect.
Significant effect.
Significant effect.
Significant effect.

{kind=link}
{kind=link}
{kind=link}
| Transmission Studies | Viral Load Studies | |
|---|---|---|
| Population | Contacts of symptomatic or asymptomatic SARS-CoV-2-infected index cases | Symptomatic or asymptomatic SARS-CoV-2-infected persons |
| Exposure | Full vaccination of the index case with COVID-19 vaccine | Full vaccination with COVID-19 vaccine |
| Comparison | Unvaccinated index cases | Unvaccinated |
| Outcome | Vaccine effectiveness against transmission of infection or relative risk reduction Odds ratio, relative risk or hazard ratio of onward transmission of disease from SARS-CoV-2-infected vaccinated index cases versus SARS-CoV-2-infected unvaccinated index cases Secondary attack rates | Viral load Cycle threshold (Ct) values as a surrogate measure for viral load |
| Study Characteristics | Total Studies n (%) | Transmission Studies n (%) | Viral Load Studies n (%) |
|---|---|---|---|
| Number of studies | 31 a | 17 a | 15 a |
| Study design | |||
| Retrospective cohort study | 21 (68%) | 12 (71%) | 9 (60%) |
| Prospective cohort study | 4 (13%) | 2 (12%) | 2 (13%) |
| Matched cohort study | 3 (10%) | 2 (12%) | 2 (13%) |
| Case–control study | 1 (3%) | 1 (6%) | 0 |
| Case–case study | 1 (3%) | 0 | 1 (7%) |
| Cross-sectional study | 1 (3%) | 0 | 1 (7%) |
| Region | |||
| Northern America | 6 (19%) | 1 (6%) | 5 (33%) |
| Europe | 13 (42%) | 10 (59%) | 4 (27%) |
| Middle East | 9 (29%) | 3 (18%) | 6 (40%) |
| Asia | 3 (10%) | 3 (18%) | 0 |
| Setting/population | |||
| Households | 11 (35%) | 11 (68%) | 0 |
| Households and non-households | 3 (10%) | 3 (18%) | 0 |
| Community | 2 (6%) | 1 (6%) | 2 (13%) |
| High-risk contacts | 1 (3%) | 1 (6%) | 0 |
| Essential and frontline workers | 1 (3%) | 0 | 1 (7%) |
| Outpatients | 1 (3%) | 0 | 1 (7%) |
| Prison | 2 (6%) | 1 (6%) | 1 (7%) |
| Positive RT-PCR samples from laboratory | 6 (19%) | 0 | 6 (40%) |
| National SARS-CoV-2 database | 4 (13%) | 0 | 4 (27%) |
| SARS-CoV-2 variant of concern b | |||
| Alpha | 12 | 8 | 5 |
| Beta | 2 | 0 | 2 |
| Pre-delta | 3 | 2 | 1 |
| Delta | 21 | 10 | 12 |
| Omicron | 6 | 3 | 3 |
| Not reported | 1 | 1 | 0 |
| COVID-19 vaccine | |||
| mRNA vaccine | 14 (45%) | 4 (24%) c | 10 (67%) d |
| mRNA or vector vaccine | 12 (39%) | 8 (47%) | 5 (33%) |
| mRNA or inactivated vaccine | 1 (3%) | 1 (6%) | 0 |
| Vector or inactivated vaccine | 1 (3%) | 1 (6%) | 0 |
| Inactivated vaccine | 1 (3%) | 1 (6%) | 0 |
| Not reported | 2 (6%) | 2 (12%) | 0 |
| Risk of bias assessment | |||
| Low risk of bias | 19 (61%) | 9 (53%) | 11 (73%) |
| Moderate risk of bias | 12 (39%) | 8 (47%) | 4 (27%) |
| High risk of bias | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oordt-Speets, A.; Spinardi, J.; Mendoza, C.; Yang, J.; Morales, G.; McLaughlin, J.M.; Kyaw, M.H. Effectiveness of COVID-19 Vaccination on Transmission: A Systematic Review. COVID 2023, 3, 1516-1527. https://doi.org/10.3390/covid3100103
Oordt-Speets A, Spinardi J, Mendoza C, Yang J, Morales G, McLaughlin JM, Kyaw MH. Effectiveness of COVID-19 Vaccination on Transmission: A Systematic Review. COVID. 2023; 3(10):1516-1527. https://doi.org/10.3390/covid3100103
Chicago/Turabian StyleOordt-Speets, Anouk, Julia Spinardi, Carlos Mendoza, Jingyan Yang, Graciela Morales, John M. McLaughlin, and Moe H. Kyaw. 2023. "Effectiveness of COVID-19 Vaccination on Transmission: A Systematic Review" COVID 3, no. 10: 1516-1527. https://doi.org/10.3390/covid3100103
APA StyleOordt-Speets, A., Spinardi, J., Mendoza, C., Yang, J., Morales, G., McLaughlin, J. M., & Kyaw, M. H. (2023). Effectiveness of COVID-19 Vaccination on Transmission: A Systematic Review. COVID, 3(10), 1516-1527. https://doi.org/10.3390/covid3100103