
D-Dimer Assessment to Predict Pulmonary Embolism in ICU Patients with COVID-19 Pneumonia


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion

{kind=link}
{kind=link}
| Study | Number of ICU Patients | Study Design | Type of Thrombo-Prophylaxis | Incidence of PE in ICU | D-Dimers of Patients without PE (μg/L) | D-Dimers of Patients with PE (μg/L) | Cut-Off for PE Diagnosis (μg/L) | Sensitivity of D-Dimer (%) | Specificity of D-Dimer (%) | AUC of D-Dimer |
|---|---|---|---|---|---|---|---|---|---|---|
| Faqihi [12] | 160 | Cohort | Enoxiparin: <50 kg, 20 mg od; 50–100 kg, 40 mg od; 100–150 kg, 40 mg bd; >150 kg, 60 mg bd | 34.4 | 2800 (1200–5500) | 5100 (2200–9100) | 3000 | 74.5 | 95.1 | ns |
| Taccone [13] | 40 | Cohort | Enoxiparin: 4000 IU od; later 4000 IU bd | 32.5 | 2302 (1327–5750) | 8280 (5976–11,483) | 3647 | 75 | 92 | 0.90 |
| van den Berg [2] | 76 | Cohort | Dalteparin: <100 kg, 5000 IU od; >100 kg, 5000 IU bd | 34.2 | 2785 (973–3298) | 3190 (1600–11,545) | 8460 | 74 | 86 | 0.82 |
| Present study | 100 | Case–control | Nadroparin: 5700 IU od | 34.7 | 850 (492–1570) | 6060 (1105–16,600) | 9000 | 28.6 | 100 | 0.78 |
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scudiero, F.; Silverio, A.; Di Maio, M.; Russo, V.; Citro, R.; Personeni, D.; Cafro, A.; D’Andrea, A.; Attena, E.; Pezzullo, S.; et al. Pulmonary embolism in COVID-19 patients: Prevalence, predictors and clinical outcome. Thromb. Res. 2021, 198, 34–39. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, M.J.W.; Waanders, D.; Kooistra, E.J.; Kox, M.; Pickkers, P. The value of D-dimer to predict pulmonary embolism in critically ill COVID-19 patients. J. Crit. Care 2021, 64, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Mansory, E.M.; Srigunapalan, S.; Lazo-Langner, A. Venous Thromboembolism in Hospitalized Critical and Noncritical COVID-19 Patients: A Systematic Review and Meta-analysis. TH Open 2021, 5, e286–e294. [Google Scholar] [CrossRef] [PubMed]
- Suh, Y.J.; Hong, H.; Ohana, M.; Bompard, F.; Revel, M.; Valle, C.; Gervaise, A.; Poissy, J.; Susen, S.; Hékimian, G.; et al. Pulmonary Embolism and Deep Vein Thrombosis in COVID-19: A Systematic Review and Meta-Analysis. Radiology 2021, 298, E70–E80. [Google Scholar] [CrossRef] [PubMed]
- Crawford, F.; Andras, A.; Welch, K.; Sheares, K.; Keeling, D.; Chappell, F.M.; Crawford, F. D-dimer test for excluding the diagnosis of pulmonary embolism. Cochrane Libr. 2016, 2016, CD010864. [Google Scholar] [CrossRef]
- Zhang, L.; Yan, X.; Fan, Q.; Liu, H.; Liu, X.; Liu, Z.; Zhang, Z. D-dimer levels on admission to predict in-hospital mortality in patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1324. [Google Scholar] [CrossRef]
- Xie, W.; Zhu, S.; Liu, Y.; Bai, Y.; Fu, W.; Chen, H.; Chen, Z.; Zhang, J. Clinical features of severe or critical ill patients with COVID-19. Nan Fang Yi Ke Da Xue Xue Bao 2020, 40, 1112–1118. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Zhan, H.; Chen, H.; Liu, C.; Cheng, L.; Yan, S.; Li, H.; Li, Y. Diagnostic Value of D-Dimer in COVID-19: A Meta-Analysis and Meta-Regression. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211010976. [Google Scholar] [CrossRef]
- Kwee, R.M.; Adams, H.J.A.; Kwee, T.C. Pulmonary embolism in patients with COVID-19 and value of D-dimer assessment: A meta-analysis. Eur. Radiol. 2021, 31, 8168–8186. [Google Scholar] [CrossRef] [PubMed]
- Ventura-Diaz, S.; Quintana-Perez, J.V.; Gil-Boronat, A.; Herrero-Huertas, M.; Gorospe-Sarasua, L.; Montilla, J.; Acosta-Batlle, J.; Blazquez-Sanchez, J.; Vicente-Bartulos, A. A higher D-dimer threshold for predicting pulmonary embolism in patients with COVID-19: A retrospective study. Emerg. Radiol. 2020, 27, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Faqihi, F.; Alharthy, A.; Balhamar, A.; Nasim, N.; Alanezi, K.; Alaklobi, F.; Memish, Z.A.; Blaivas, M.; Alqahtani, S.A.; Karakitsos, D. A Retrospective Analysis of Thromboembolic Phenomena in Mechanically Ventilated Patients with COVID-19. Crit. Care. Res. Pract. 2021, 2021, 8737580. [Google Scholar] [CrossRef] [PubMed]
- Taccone, F.S.; Gevenois, P.A.; Peluso, L.; Pletchette, Z.; Lheureux, O.; Brasseur, A.; Garufi, A.; Talamonti, M.; Motte, S.; Nobile, L.; et al. Higher Intensity Thromboprophylaxis Regimens and Pulmonary Embolism in Critically Ill Coronavirus Disease 2019 Patients. Crit. Care Med. 2020, 48, e1087–e1090. [Google Scholar] [CrossRef] [PubMed]
- Rutjes, A.W.S.; Reitsma, J.B.; Vandenbroucke, J.P.; Glas, A.S.; Bossuyt, P.M.M. Case-control and two-gate designs in diagnostic accuracy studies. Clin. Chem. 2005, 51, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Kline, J.A. Diagnosis and Exclusion of Pulmonary Embolism. Thromb. Res. 2018, 163, 207–220. [Google Scholar] [CrossRef] [PubMed]
- Whyte, M.B.; Kelly, P.A.; Gonzalez, E.; Arya, R.; Roberts, L.N. Pulmonary embolism in hospitalised patients with COVID-19. Thromb. Res. 2020, 195, 95–99. [Google Scholar] [CrossRef]
- Rindi, L.V.; Al Moghazi, S.; Donno, D.R.; Cataldo, M.A.; Petrosillo, N. Predictive scores for the diagnosis of Pulmonary Embolism in COVID-19: A systematic review. Int. J. Infect. Dis. 2022, 115, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Ortega, A.; Oscullo, G.; Calvillo, P.; Lopez-Reyes, R.; Mendez, R.; Gomez-Olivas, J.D.; Bekki, A.; Fonfria, C.; Trilles-Olaso, L.; Zaldivar, E.; et al. Incidence, risk factors, and thrombotic load of pulmonary embolism in patients hospitalized for COVID-19 infection. J. Infect. 2021, 82, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Schouten, H.J.; Geersing, G.J.; Koek, H.L.; Zuithoff, N.P.A.; Janssen, K.J.M.; Douma, R.A.; van Delden, J.J.M.; Moons, K.G.M.; Reitsma, J.B. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: Systematic review and meta-analysis. BMJ 2013, 346, f2492. [Google Scholar] [CrossRef]
- Patel, B.V.; Arachchillage, D.J.; Ridge, C.A.; Bianchi, P.; Doyle, J.F.; Garfield, B.; Ledot, S.; Morgan, C.; Passariello, M.; Price, S.; et al. Pulmonary Angiopathy in Severe COVID-19: Physiologic, Imaging, and Hematologic Observations. Am. J. Respir. Crit. Care Med. 2020, 202, 690. [Google Scholar] [CrossRef]


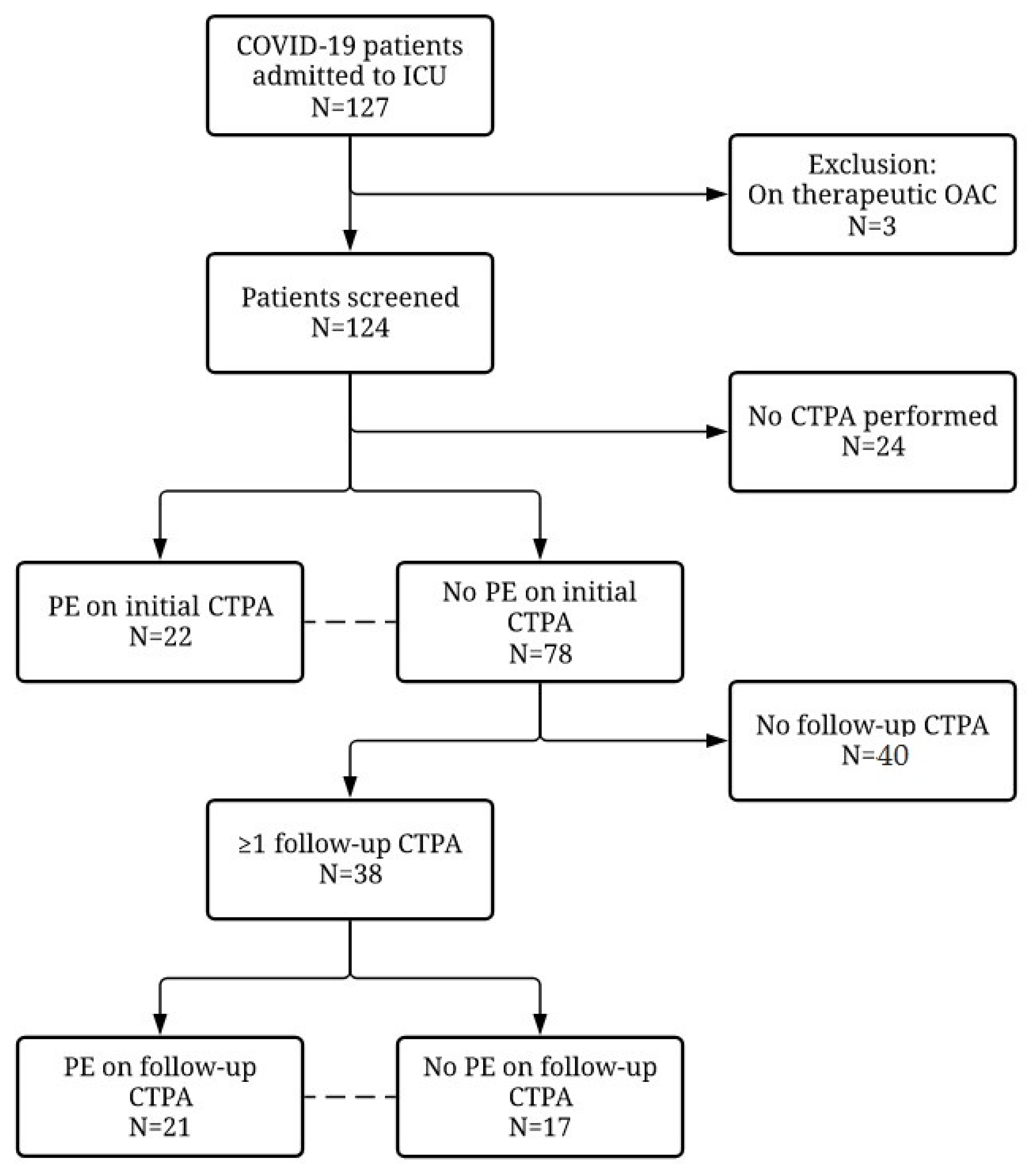
| All Patients (N = 124) | No CTPA Performed (N = 24) | No PE on Initial CTPA (N = 78) | PE on Initial CTPA (N = 22) | p-Value | |
|---|---|---|---|---|---|
| Sex (male) | 84 (67.7) | 15 (62.5) | 52 (66.7) | 17 (77.3) | 0.347 |
| Age (years) | 66 (57–72) | 62 (57–72) | 66 (58–71) | 66 (56–72) | 0.913 |
| Mechanical ventilation | 84 (67.7) | 13 (54.2) | 56 (71.8) | 15 (68.2) | 0.745 |
| Mortality | 21 (16.9) | 1 (4.2) | 14 (17.9) | 6 (27.3) | 0.339 |
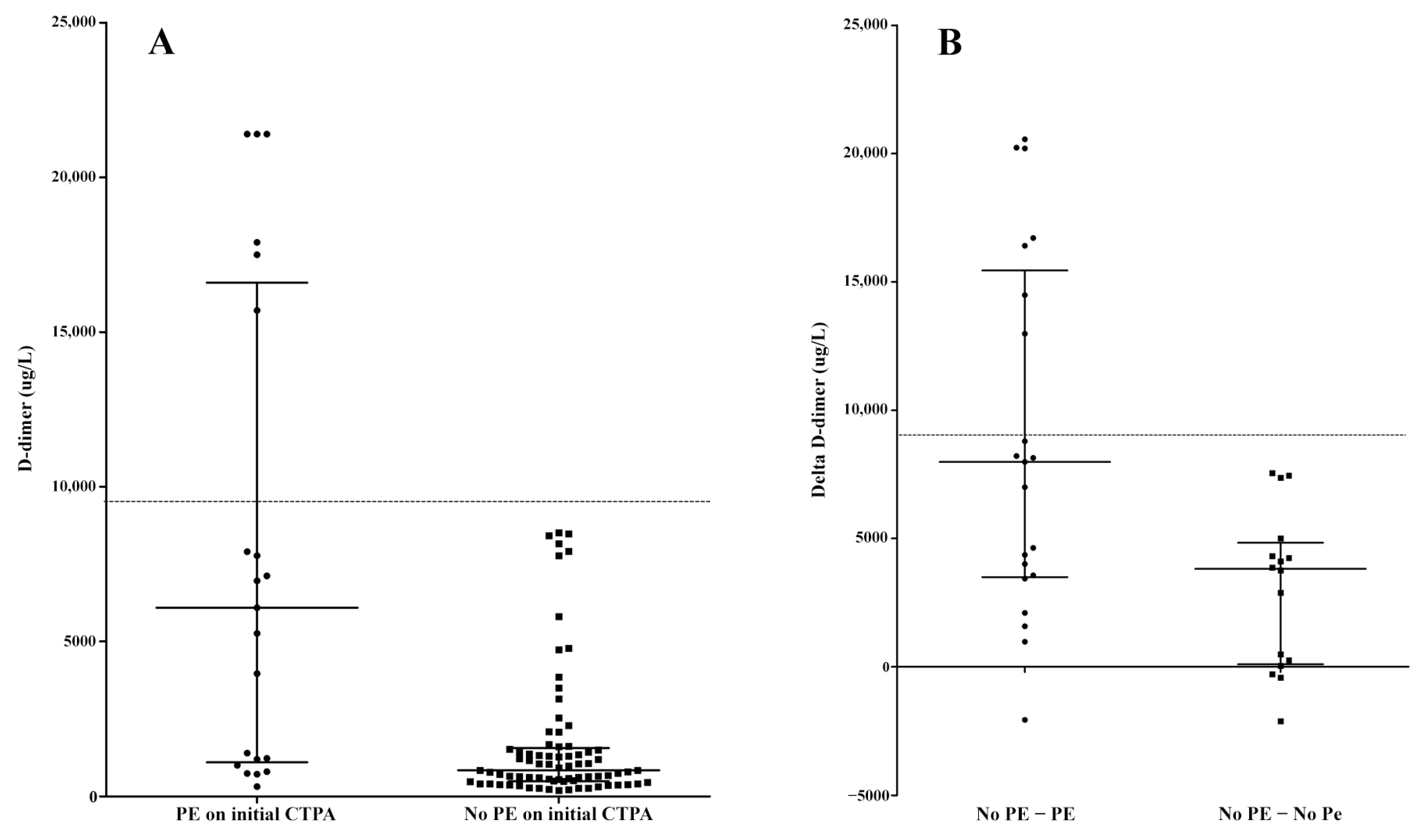
| D-dimers on admission (μg/L) | 850 (492–1570) | 6060 (1105–16,600) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Louwsma, J.; Langeveld, B.; Luyendijk, J.M.; van den Oever, H.L.A. D-Dimer Assessment to Predict Pulmonary Embolism in ICU Patients with COVID-19 Pneumonia. COVID 2023, 3, 1380-1388. https://doi.org/10.3390/covid3090095
Louwsma J, Langeveld B, Luyendijk JM, van den Oever HLA. D-Dimer Assessment to Predict Pulmonary Embolism in ICU Patients with COVID-19 Pneumonia. COVID. 2023; 3(9):1380-1388. https://doi.org/10.3390/covid3090095
Chicago/Turabian StyleLouwsma, Jelger, Bas Langeveld, Jacqueline M. Luyendijk, and Huub L. A. van den Oever. 2023. "D-Dimer Assessment to Predict Pulmonary Embolism in ICU Patients with COVID-19 Pneumonia" COVID 3, no. 9: 1380-1388. https://doi.org/10.3390/covid3090095
APA StyleLouwsma, J., Langeveld, B., Luyendijk, J. M., & van den Oever, H. L. A. (2023). D-Dimer Assessment to Predict Pulmonary Embolism in ICU Patients with COVID-19 Pneumonia. COVID, 3(9), 1380-1388. https://doi.org/10.3390/covid3090095